You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Physiology of Amniotic Fluid Volume RegulationDocument8 pagesPhysiology of Amniotic Fluid Volume RegulationYosep SutandarNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Musa 2015Document15 pagesMusa 2015Jose Luis Morales BautistaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- IETADocument10 pagesIETAJose Luis Morales BautistaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Meta-Analysis of Second-Trimester Markers For Trisomy 21. 2013Document15 pagesMeta-Analysis of Second-Trimester Markers For Trisomy 21. 2013risos7No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- PIIS000293781502102XDocument1 pagePIIS000293781502102XYosep SutandarNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Routine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolDocument15 pagesRoutine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolYosep SutandarNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Uog 10054Document22 pagesUog 10054Aswin ChristantoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Maxillary Gap at 11-13 WeeksDocument5 pagesMaxillary Gap at 11-13 Weekscarlos cobeloNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Diagnosis of Fetal Non-Chromosomal Abnormalities On Routine Ultrasound Examination at 11-13 Weeks' GestationDocument10 pagesDiagnosis of Fetal Non-Chromosomal Abnormalities On Routine Ultrasound Examination at 11-13 Weeks' GestationYosep SutandarNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Ferra RettiDocument51 pagesFerra RettiYosep SutandarNo ratings yet
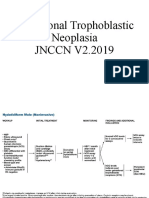
- Gestational Trophoblastic NeoplasiaDocument14 pagesGestational Trophoblastic NeoplasiaYosep SutandarNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- PIIS0015028207001161Document8 pagesPIIS0015028207001161Yosep SutandarNo ratings yet
- Clostridium Perfringens Sepsis Following A Molar Pregnancy: ASE EportDocument2 pagesClostridium Perfringens Sepsis Following A Molar Pregnancy: ASE EportYosep SutandarNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Mao2014 Article ImagingOfPelvicLymphNodesDocument13 pagesMao2014 Article ImagingOfPelvicLymphNodesYosep SutandarNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Ovarian Reserve Testing: A User's Guide: Expert ReviewsDocument12 pagesOvarian Reserve Testing: A User's Guide: Expert ReviewsYosep SutandarNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- PDFDocument9 pagesPDFYosep SutandarNo ratings yet
- Changes in The Sexual Function During Pregnancy: Aim. MethodsDocument10 pagesChanges in The Sexual Function During Pregnancy: Aim. MethodsYosep SutandarNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Murtagh 2010Document9 pagesMurtagh 2010Yosep SutandarNo ratings yet
- Practice Bullet In: Emergency ContraceptionDocument11 pagesPractice Bullet In: Emergency ContraceptionYosep SutandarNo ratings yet
- ISUOG - Fetal Heart ExaminationDocument12 pagesISUOG - Fetal Heart ExaminationAzucenaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Effect of Pregnancy On Sexual Function of Couples: AbstractDocument8 pagesEffect of Pregnancy On Sexual Function of Couples: AbstractYosep SutandarNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Eng - PDF JsessionidDocument34 pagesEng - PDF JsessionidYosep SutandarNo ratings yet
- Acog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentDocument10 pagesAcog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentYosep SutandarNo ratings yet
- Pi Is 0884217517304100Document3 pagesPi Is 0884217517304100Yosep SutandarNo ratings yet
- NSAMR Systematic ReviewDocument8 pagesNSAMR Systematic ReviewYosep SutandarNo ratings yet
- FSFI Questionnaire2000Document5 pagesFSFI Questionnaire2000Dewi AsmalindaNo ratings yet
- Systematic Reviews To Support Evidence-Based Medicine (2nd Edition)Document216 pagesSystematic Reviews To Support Evidence-Based Medicine (2nd Edition)Yosep Sutandar100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Emergency Contraception: Sogc Clinical Practice GuidelineDocument9 pagesEmergency Contraception: Sogc Clinical Practice GuidelineYosep SutandarNo ratings yet
- Enteral NutritionDocument73 pagesEnteral NutritionYosep SutandarNo ratings yet
- Invos System Improving Patient Outcomes Cerebral Somatic Oximetry BrochureDocument6 pagesInvos System Improving Patient Outcomes Cerebral Somatic Oximetry Brochuremihalcea alinNo ratings yet
- PATHOPHYSIOLOGY OF OSTEOSARCOMaDocument1 pagePATHOPHYSIOLOGY OF OSTEOSARCOMakyawNo ratings yet
- Nursing Care Plan SampleDocument1 pageNursing Care Plan SampleEds SyNo ratings yet
- AdamRouilly Healthcare Education Catalogue 2015-16Document326 pagesAdamRouilly Healthcare Education Catalogue 2015-16NGUYEN HUU TRUONG TruongNo ratings yet
- Pediatric Asthma Situation in Chengdu, China, During The COVID-19 Pandemic: An Observational StudyDocument10 pagesPediatric Asthma Situation in Chengdu, China, During The COVID-19 Pandemic: An Observational StudyzainabNo ratings yet
- What Kate Did at WorkDocument3 pagesWhat Kate Did at WorkSpeech & Language Therapy in PracticeNo ratings yet
- Forward IMRT Breast PDFDocument54 pagesForward IMRT Breast PDFmitza05100% (1)
- Reflection Paper Regulatory Guidance Use Health Related Quality Life HRQL Measures Evaluation - enDocument5 pagesReflection Paper Regulatory Guidance Use Health Related Quality Life HRQL Measures Evaluation - en813l1srgr1No ratings yet
- AHA Coding Clinic Guidance: Code Number in Lieu of A DiagnosisDocument2 pagesAHA Coding Clinic Guidance: Code Number in Lieu of A Diagnosissyaiful rinantoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elman Book FlyerDocument2 pagesElman Book FlyerCarolina CruzNo ratings yet
- Maternal and Child ReviewerDocument330 pagesMaternal and Child ReviewerMiles Brianne Lymer A. OlvidoNo ratings yet
- NCLEX Practice ExamDocument10 pagesNCLEX Practice ExamJune DumdumayaNo ratings yet
- Guideline Elaboración de AcDocument3 pagesGuideline Elaboración de AcsilviazulNo ratings yet
- Peripheral Vascular Diseases NCLEXDocument6 pagesPeripheral Vascular Diseases NCLEXPotchiee PfizerNo ratings yet
- Pre & Post Operative TracheostomyDocument2 pagesPre & Post Operative TracheostomyHantu Kak Limah100% (2)
- Stok Opname Nopember 2015-RevisiDocument146 pagesStok Opname Nopember 2015-RevisinooNo ratings yet
- CV DR Ari Sami Hussain NadhimDocument5 pagesCV DR Ari Sami Hussain NadhimAri SamiNo ratings yet
- Government of Andhra Pradesh Andhra Pradesh Medical Services Recruitment BoardDocument13 pagesGovernment of Andhra Pradesh Andhra Pradesh Medical Services Recruitment Boardchandu93152049No ratings yet
- Chapter 13 Injuries To The Thorax and AbdomenDocument4 pagesChapter 13 Injuries To The Thorax and Abdomenapi-287615830No ratings yet
- Malaria: Health Education HFT 201 By: Sophia Kol, MDDocument10 pagesMalaria: Health Education HFT 201 By: Sophia Kol, MDTith SeavmeyNo ratings yet
- Gabel 2013Document12 pagesGabel 2013rahulNo ratings yet
- Animal Incident Report Form 02 10 2021Document4 pagesAnimal Incident Report Form 02 10 2021WenaNo ratings yet
- Recommendations CardiovascularRenal 07.09.2022Document6 pagesRecommendations CardiovascularRenal 07.09.2022Harisankarthekkethil 26No ratings yet
- MANIFESTASI KLINIK Penyakit Jantung KoronerDocument4 pagesMANIFESTASI KLINIK Penyakit Jantung KoronerDwitya NoviariNo ratings yet
- BodyBallancer Lipo Brochure PDFDocument2 pagesBodyBallancer Lipo Brochure PDFRoss Gale100% (1)
- ESR Microsed PermaiDocument20 pagesESR Microsed PermaiHishamudin RaisNo ratings yet
- Carboplatin PaclitaxelDocument6 pagesCarboplatin PaclitaxelNida Auliya RahmahNo ratings yet
- Ao2022 0037Document22 pagesAo2022 0037Abigael VianaNo ratings yet
- The Cardiovascular SystemDocument43 pagesThe Cardiovascular Systemtravis efraimNo ratings yet
- Characterization of Successful Root Canal TreatmenDocument10 pagesCharacterization of Successful Root Canal TreatmenSitiRahmahAzharNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (26)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)