You might also like
- Denecke EurJPediatr 03Document21 pagesDenecke EurJPediatr 03Thorsten MarquardtNo ratings yet
- Koepsell - GlucoseTransportersInBrainInHeDocument45 pagesKoepsell - GlucoseTransportersInBrainInHeManuelNo ratings yet
- Carbohydrate DisorderDocument74 pagesCarbohydrate DisorderEric YewNo ratings yet
- Huntington Disease FinalDocument4 pagesHuntington Disease Finalicrs_aamirNo ratings yet
- IgD VladutiuDocument32 pagesIgD VladutiuValentina MusatNo ratings yet
- The Genetic Aspect and Morphological Appearance of AchondrogenesisDocument10 pagesThe Genetic Aspect and Morphological Appearance of AchondrogenesisRizka RamadaniNo ratings yet
- NIH Public Access: Isocitrate Dehydrogenase Mutations in Gliomas: Mechanisms, Biomarkers and Therapeutic TargetDocument9 pagesNIH Public Access: Isocitrate Dehydrogenase Mutations in Gliomas: Mechanisms, Biomarkers and Therapeutic TargetZaharah YunosNo ratings yet
- Autoimmune Liver Disease Systemic Lupus.201Document91 pagesAutoimmune Liver Disease Systemic Lupus.201A Rezki ChairamsyahNo ratings yet
- J Nucl Med-2004-Avril-930-2Document4 pagesJ Nucl Med-2004-Avril-930-2Thắng Nguyễn quốcNo ratings yet
- Gaucher 3 CDocument10 pagesGaucher 3 CSergio ZambranoNo ratings yet
- DiGeorge SyndromeDocument18 pagesDiGeorge SyndromeRupesh MohandasNo ratings yet
- Metabolism of Acylglycerols and Sphingolipids: DR - Qasim AL-DaamiDocument23 pagesMetabolism of Acylglycerols and Sphingolipids: DR - Qasim AL-Daamiraafat mohammedNo ratings yet
- Diabetes Mellitus: Type 1 DM Type 2 DM Gestational DM Other TypesDocument20 pagesDiabetes Mellitus: Type 1 DM Type 2 DM Gestational DM Other Typesmohamed mowafeyNo ratings yet
- Genetic Etiologies of Leukocyte Adhesion DefectsDocument6 pagesGenetic Etiologies of Leukocyte Adhesion DefectsCosmin BarbosNo ratings yet
- Diabetes Mellitus: Etiology:-Signaling Defects: - LeprechaunismDocument4 pagesDiabetes Mellitus: Etiology:-Signaling Defects: - LeprechaunismmehboobNo ratings yet
- Diabetes: Activity Levels As Countries Become More Industrialized, and The Aging of The PopulationDocument9 pagesDiabetes: Activity Levels As Countries Become More Industrialized, and The Aging of The PopulationLouije MombzNo ratings yet
- ACase Report of Familial Glucocorticoid DeficiencyDocument2 pagesACase Report of Familial Glucocorticoid DeficiencyIOSRjournalNo ratings yet
- Globo SeriesDocument7 pagesGlobo SeriesConcepcion R. AquinoNo ratings yet
- بحث immunodeficiency disorder2Document25 pagesبحث immunodeficiency disorder2suqylNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptJosephine D CarandangNo ratings yet
- Gly 1 PDFDocument37 pagesGly 1 PDFGirum SolomonNo ratings yet
- Articulo 1Document16 pagesArticulo 1Juliana CorreaNo ratings yet
- Activation of Nrf2 Signaling by Natural Products-Can It Alleviate DiabetesDocument30 pagesActivation of Nrf2 Signaling by Natural Products-Can It Alleviate DiabetesDra. Ianna CarmoNo ratings yet
- Digeorge Syndrome: Rupesh Mohandas GR3Document18 pagesDigeorge Syndrome: Rupesh Mohandas GR3Rupesh MohandasNo ratings yet
- Membrane 37-Kda Islet Beta Cell Antigen: Pancreatic Autoimmune Disorders: EdtDocument2 pagesMembrane 37-Kda Islet Beta Cell Antigen: Pancreatic Autoimmune Disorders: EdtDaena TimtimanNo ratings yet
- MCP PDFDocument3 pagesMCP PDFValentina Barrera BerrioNo ratings yet
- Immunodeficiency Disease: Primary ImmunodeficienciesDocument8 pagesImmunodeficiency Disease: Primary ImmunodeficienciesAbo AmgadNo ratings yet
- Diabetes Mellitus 1Document5 pagesDiabetes Mellitus 1smurplerNo ratings yet
- Immunodeficiency: Syarifuddin WahidDocument52 pagesImmunodeficiency: Syarifuddin Wahidadzkia-hkNo ratings yet
- Pediatrics Storage DiseasesDocument2 pagesPediatrics Storage DiseasesuyesNo ratings yet
- Migdalska-Richards Et Al-2016-Journal of NeurochemistryDocument14 pagesMigdalska-Richards Et Al-2016-Journal of Neurochemistryjazz castañedaNo ratings yet
- Primary Immunodeficiencies Associated With or Secondary To Other DiseasesDocument2 pagesPrimary Immunodeficiencies Associated With or Secondary To Other Diseasesmike_helplineNo ratings yet
- The Endocrine Pancreas IIDocument134 pagesThe Endocrine Pancreas IIHoque Mohammed Newaz ShorifulNo ratings yet
- Redox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsDocument6 pagesRedox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsEdisher TsivtsivadzeNo ratings yet
- Genetic Disorders: Dr. Winny Natacia Leiwakabessy, Mkes, SppaDocument50 pagesGenetic Disorders: Dr. Winny Natacia Leiwakabessy, Mkes, Sppasyela trifenaNo ratings yet
- Differential Diagnosis of Cherry-Red Spot at MaculaDocument4 pagesDifferential Diagnosis of Cherry-Red Spot at MaculaVarun BoddulaNo ratings yet
- Lec D.M.Document39 pagesLec D.M.liathmahmood15No ratings yet
- 213 FullDocument4 pages213 FullMartina RivasNo ratings yet
- Diabetes Mellitus SeminarDocument35 pagesDiabetes Mellitus SeminarAnkush SinglaNo ratings yet
- 15-Deoxy - Prostaglandin J Induces IL-8 and GM-CSF in A Human Airway Epithelial Cell Line (NCI-H)Document7 pages15-Deoxy - Prostaglandin J Induces IL-8 and GM-CSF in A Human Airway Epithelial Cell Line (NCI-H)Roy GoldenNo ratings yet
- DM, DKA, and IDMDocument19 pagesDM, DKA, and IDMJennyu YuNo ratings yet
- Frontotemporal Dementia NeuropathologyDocument14 pagesFrontotemporal Dementia Neuropathologyppico1963No ratings yet
- Maccioni 2002Document8 pagesMaccioni 2002vsvsuresh2099No ratings yet
- Miglustat For Tangier DiseaseDocument4 pagesMiglustat For Tangier DiseaseIan RoarkNo ratings yet
- CURS HGDocument26 pagesCURS HGCodruta-Elena BadeaNo ratings yet
- Diagnosis of Hepatic Glycogenosis in Poorly Controlled Type 1 Diabetes MellitusDocument8 pagesDiagnosis of Hepatic Glycogenosis in Poorly Controlled Type 1 Diabetes MellituskhitasmoumeneNo ratings yet
- Genes For All DisordersDocument86 pagesGenes For All Disordersvenkyreddy97No ratings yet
- GSD MahmoudDocument19 pagesGSD MahmouddrmamodoNo ratings yet
- Glycogen Storage Disorders PDFDocument4 pagesGlycogen Storage Disorders PDFAHMEDNo ratings yet
- Jungtrakoon SLC19A2 PDFDocument11 pagesJungtrakoon SLC19A2 PDFChristantya VitaNo ratings yet
- Glycogen Storage Disease, Type II (Pompe Disease) : BackgroundDocument7 pagesGlycogen Storage Disease, Type II (Pompe Disease) : Background201111000No ratings yet
- BST 49 2561Document12 pagesBST 49 2561Nathur IdrisNo ratings yet
- Congenital Hyperinsulinism Current Trends in Diagnosis and TheraphyDocument14 pagesCongenital Hyperinsulinism Current Trends in Diagnosis and TheraphyJaka KurniawanNo ratings yet
- BiologyDocument26 pagesBiologyamhhospital0No ratings yet
- Maed 07 271Document6 pagesMaed 07 271MARDHIANo ratings yet
- g6pd - An Old Bottle With New WineDocument7 pagesg6pd - An Old Bottle With New Winecutegal88No ratings yet
- Euglycaemic Diabetic Ketoacidosis As A Complication of SGLT-2 Inhibitors. Epidemiology, Pathophysiology, and TreatmentDocument11 pagesEuglycaemic Diabetic Ketoacidosis As A Complication of SGLT-2 Inhibitors. Epidemiology, Pathophysiology, and Treatmentmaria arenas de itaNo ratings yet
- Golgi DiseasesDocument1 pageGolgi Diseasesninja-2001No ratings yet
- Glycoproteins: DR Amina Tariq BiochemistryDocument27 pagesGlycoproteins: DR Amina Tariq BiochemistryMadeline UdarbeNo ratings yet
- International Textbook of Diabetes MellitusFrom EverandInternational Textbook of Diabetes MellitusR. A. DeFronzoNo ratings yet
- Ta BookDocument128 pagesTa BookIon CimirinschiNo ratings yet
- A26badmintoninfomanual2007 PDFDocument24 pagesA26badmintoninfomanual2007 PDFAdy NgNo ratings yet
- Yt 1000R 20081Document2 pagesYt 1000R 20081Ion CimirinschiNo ratings yet
- Pressures Produced When Penguins PooDocument3 pagesPressures Produced When Penguins Poojamesyu100% (4)
- Badminton TutorialDocument19 pagesBadminton Tutorialtvr123100% (1)
- Exploring Psychedelic Trance and Electronic Dance Music in Modern CultureDocument39 pagesExploring Psychedelic Trance and Electronic Dance Music in Modern CultureIon CimirinschiNo ratings yet
- Badminton PDFDocument8 pagesBadminton PDFricardoNo ratings yet
- "All The Khan's Horses" by Morris RossabiDocument3 pages"All The Khan's Horses" by Morris RossabiAlperenler44No ratings yet
- "All The Khan's Horses" by Morris RossabiDocument3 pages"All The Khan's Horses" by Morris RossabiAlperenler44No ratings yet
- MN Mongolian Language Lessons PDFDocument12 pagesMN Mongolian Language Lessons PDFFranco Salvatore100% (1)
- Testimonials PDFDocument3 pagesTestimonials PDFIon CimirinschiNo ratings yet
- Sigal It 2012Document33 pagesSigal It 2012Ion CimirinschiNo ratings yet
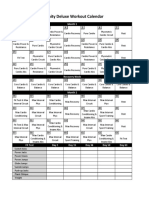
- Insanity Workout Deluxe Calendar SimpleDocument1 pageInsanity Workout Deluxe Calendar SimpleCristian Manuel GonzálezNo ratings yet
- InfoDocument1 pageInfoIon CimirinschiNo ratings yet
- Ind2601 Study NotesDocument63 pagesInd2601 Study NotesIon CimirinschiNo ratings yet
- PDF Ebooks - Org 02221503Sf2N8Document302 pagesPDF Ebooks - Org 02221503Sf2N8Anonymous 3Oprx0LbwNo ratings yet
- The Story of Medusa and Athena 2Document2 pagesThe Story of Medusa and Athena 2Ion Cimirinschi0% (1)
- Gene Therapy ReportDocument2 pagesGene Therapy ReportKaren Jane YapNo ratings yet
- AlkalinphosphatDocument16 pagesAlkalinphosphatSanthosh PNo ratings yet
- Biology Topic Questions (@IMAT - Hub)Document111 pagesBiology Topic Questions (@IMAT - Hub)pahlavandarinisotoodehNo ratings yet
- Rollno - 02 PDD GPCRDocument20 pagesRollno - 02 PDD GPCRJayesh KadamNo ratings yet
- General Biology 1: First Semester-Quarter 2Document21 pagesGeneral Biology 1: First Semester-Quarter 2Laelannie MagpayoNo ratings yet
- (Developmental Neuroscience) Anthony T. Campagnoni-Brain Development With A Focus On The Cortex - Developmental Neuroscience Vol 25 Issue 2-4-S Karger Pub (2003) PDFDocument215 pages(Developmental Neuroscience) Anthony T. Campagnoni-Brain Development With A Focus On The Cortex - Developmental Neuroscience Vol 25 Issue 2-4-S Karger Pub (2003) PDFFrancisco DiezNo ratings yet
- Base DadosDocument86 pagesBase DadosGersonNo ratings yet
- Afns Initial Test Experiences 16 August 2k23Document5 pagesAfns Initial Test Experiences 16 August 2k23factfeast446No ratings yet
- Quiz 1 - MacromoleculesDocument2 pagesQuiz 1 - MacromoleculesEricha Palaypay EmpaynadoNo ratings yet
- Chapter 10 GeneticsDocument5 pagesChapter 10 Geneticspatrick cagueteNo ratings yet
- Immune Regulation by GlucocorticoidsDocument35 pagesImmune Regulation by GlucocorticoidsSyifa SariNo ratings yet
- A New Generation of Drugs: Synthetic Peptides Based On Natural Regulatory PeptidesDocument30 pagesA New Generation of Drugs: Synthetic Peptides Based On Natural Regulatory PeptidesDicky M SitanggangNo ratings yet
- CRISPR Cas9Document8 pagesCRISPR Cas9kashif WaseemNo ratings yet
- Plant Virus VectorsDocument30 pagesPlant Virus VectorsJason AlvarezNo ratings yet
- Eukaryotic Transposable ElementsDocument28 pagesEukaryotic Transposable Elementskerkour-abd1523No ratings yet
- Application of Data Mining in BioinformaticsDocument5 pagesApplication of Data Mining in BioinformaticsYuni ListianaNo ratings yet
- Article: Communication Between Viruses Guides Lysis-Lysogeny DecisionsDocument18 pagesArticle: Communication Between Viruses Guides Lysis-Lysogeny DecisionsianchinaNo ratings yet
- Mock 2 IRDocument3 pagesMock 2 IRWendell Kim LlanetaNo ratings yet
- Solutions Increasing Productivity of MabDocument50 pagesSolutions Increasing Productivity of MabAlex Danny Zapata CalleNo ratings yet
- Chapter 2.2. The Cell Cycle Meiosis and MitosisDocument23 pagesChapter 2.2. The Cell Cycle Meiosis and MitosisB. ThuậnNo ratings yet
- Zymography of Metalloproteinases: UNIT 21.15Document12 pagesZymography of Metalloproteinases: UNIT 21.15Dr-Gnaneshwar GoudNo ratings yet
- Presentation 4 Fe-S Protein, Cytochrome, NitrogenaseDocument18 pagesPresentation 4 Fe-S Protein, Cytochrome, NitrogenaseRuby AhmedNo ratings yet
- Research Article: Involvement of Prohibitin Upregulation in Abrin-Triggered ApoptosisDocument11 pagesResearch Article: Involvement of Prohibitin Upregulation in Abrin-Triggered ApoptosisAndri Praja SatriaNo ratings yet
- Genetics: Chromosomes and Cell DivisionDocument31 pagesGenetics: Chromosomes and Cell DivisionPaqui Miranda GualdaNo ratings yet
- DNA Damage by ROSDocument11 pagesDNA Damage by ROSapi-19762689No ratings yet
- Xantalgosil CDocument3 pagesXantalgosil CTais Amadio MenegatNo ratings yet
- 2021 Test 1 Cell BiologyDocument7 pages2021 Test 1 Cell BiologyIzz IrfanNo ratings yet
- (Advances in Parasitology 39) J.R. Baker, R. Muller and D. Rollinson (Eds.) - Academic Press (1997)Document316 pages(Advances in Parasitology 39) J.R. Baker, R. Muller and D. Rollinson (Eds.) - Academic Press (1997)Stoian GoranovNo ratings yet
- Cell Engineering 101Document20 pagesCell Engineering 101Vương HoàngNo ratings yet
- Membrane Transport Practice QuestionsDocument2 pagesMembrane Transport Practice QuestionsLogan ParkisonNo ratings yet