You might also like
- Tau Opa ThiesDocument22 pagesTau Opa ThiesIrina OdajiuNo ratings yet
- Senate Alzheimers Letter To CMS and HHS - 02-17-23Document5 pagesSenate Alzheimers Letter To CMS and HHS - 02-17-23WCNC DigitalNo ratings yet
- Imaging Tau Pathology in Alzheimer's Disease With Positron Emission Tomography: Lessons Learned From Imaging-Neuropathology Validation StudiesDocument5 pagesImaging Tau Pathology in Alzheimer's Disease With Positron Emission Tomography: Lessons Learned From Imaging-Neuropathology Validation StudiesBravo BNo ratings yet
- Alzheimer 'S Disease Profiled by Uid and Imaging Markers: Tau PET Best Predicts Cognitive DeclineDocument11 pagesAlzheimer 'S Disease Profiled by Uid and Imaging Markers: Tau PET Best Predicts Cognitive DeclineChouaib OujhainNo ratings yet
- UPDRS (Data Sheet)Document2 pagesUPDRS (Data Sheet)CNS WARDNo ratings yet
- The Amyloid-β Pathway in Alzheimer's Disease. Molecular PsychiatryDocument23 pagesThe Amyloid-β Pathway in Alzheimer's Disease. Molecular Psychiatryanggi abNo ratings yet
- Disease Signs and Symptoms Deficiency/Problem Notes AmyloidosisDocument14 pagesDisease Signs and Symptoms Deficiency/Problem Notes AmyloidosisSriKavya DevineniNo ratings yet
- Tau Protein and Neurodegeneration: Michel GoedertDocument5 pagesTau Protein and Neurodegeneration: Michel GoedertT Aliagita RojasNo ratings yet
- Imaging Alzheimer PDFDocument22 pagesImaging Alzheimer PDFSuman SharmaNo ratings yet
- Therapeutics of Alzheimer's DiseaseDocument24 pagesTherapeutics of Alzheimer's DiseaseArtemis LiNo ratings yet
- STEP 1 CluesDocument3 pagesSTEP 1 CluesRaji NaamaniNo ratings yet
- CarteDocument354 pagesCartepaslaru danNo ratings yet
- Recent Advances in Understanding & Management of DementiaDocument43 pagesRecent Advances in Understanding & Management of DementiaaartiNo ratings yet
- Pathological Mechanisms and Therapeutic Strategies For ADDocument24 pagesPathological Mechanisms and Therapeutic Strategies For ADShuaib AhmadNo ratings yet
- 01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFDocument26 pages01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFawinsyNo ratings yet
- New Molecular Targets For PET and SPECT Imaging in Neurodegenerative DiseasesDocument12 pagesNew Molecular Targets For PET and SPECT Imaging in Neurodegenerative DiseasesMihaela ToaderNo ratings yet
- Review To CNS Radiology Including SSDocument52 pagesReview To CNS Radiology Including SSBisher Al-halabiNo ratings yet
- Mapping Progressive Brain Structural Changes in Early Alzheimer's DiseaseDocument27 pagesMapping Progressive Brain Structural Changes in Early Alzheimer's Diseasetonylee24No ratings yet
- PDR 2020Document1 pagePDR 2020api-506024957No ratings yet
- CERADDocument14 pagesCERADMaría KristjánsdóttirNo ratings yet
- 03 TumoursDocument50 pages03 TumoursMalinda KarunaratneNo ratings yet
- MS Word 2010 All Keyboard Shortcut Keys OdiaPortal - in 746289Document4 pagesMS Word 2010 All Keyboard Shortcut Keys OdiaPortal - in 746289Ali Shaikh AbdulNo ratings yet
- Symptom Onset Arrival: Circle Yes, No or Not Known As AppropriateDocument2 pagesSymptom Onset Arrival: Circle Yes, No or Not Known As AppropriateB-win IrawanNo ratings yet
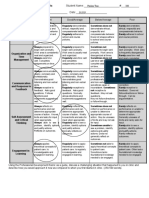
- EF5231 Assessment 001 Marking CriteriaDocument1 pageEF5231 Assessment 001 Marking CriteriaTú LêNo ratings yet
- Infections Diseases of The Central Nervous System: Chapter VI - J. RuscalledaDocument11 pagesInfections Diseases of The Central Nervous System: Chapter VI - J. RuscalledaArif BudimanNo ratings yet
- Stroke Inclusion Exclusion StrokeDocument1 pageStroke Inclusion Exclusion Strokecdeepak71No ratings yet
- Adult Brain Tumours: DR M.P. Okemwa PathologistDocument39 pagesAdult Brain Tumours: DR M.P. Okemwa PathologistSalman MajidNo ratings yet
- Seizure and EpilepsyDocument18 pagesSeizure and EpilepsyJamal JosephNo ratings yet
- Neurology: Timothy E. Welty, Pharm.D., FCCP, BCPSDocument68 pagesNeurology: Timothy E. Welty, Pharm.D., FCCP, BCPSAlmaha AlfakhriNo ratings yet
- Cheryl E. Ball CV (January 2011)Document17 pagesCheryl E. Ball CV (January 2011)s2ceballNo ratings yet
- Neuroimaging in DementiaDocument11 pagesNeuroimaging in DementiaAndika ResaNo ratings yet
- Faculty LetterDocument2 pagesFaculty LetterMarcus GilmerNo ratings yet
- CAHSS Guidelines For Tenure, Promotion, and Reappointment - Approved 12 June 2019 PDFDocument18 pagesCAHSS Guidelines For Tenure, Promotion, and Reappointment - Approved 12 June 2019 PDFmohrinerNo ratings yet
- نشاط ينايرDocument23 pagesنشاط ينايرDark AngelNo ratings yet
- ParkinsonDiseaseFarter2017Document103 pagesParkinsonDiseaseFarter2017DISKA YUNIAROHIMNo ratings yet
- Downbeat Nystagmus: Aetiology and Comorbidity in 117 PatientsDocument7 pagesDownbeat Nystagmus: Aetiology and Comorbidity in 117 PatientsVinay GNo ratings yet
- Palliative Care in AdvancedDocument24 pagesPalliative Care in AdvancedClaudio Silva FilhoNo ratings yet
- Cheryl E Ball - CV (Oct2012)Document23 pagesCheryl E Ball - CV (Oct2012)s2ceballNo ratings yet
- Chapter 3 (7!1!20 Edition)Document29 pagesChapter 3 (7!1!20 Edition)DePauliaNo ratings yet
- EMERALD TrialDocument13 pagesEMERALD TrialCristian MuñozNo ratings yet
- Gan & Romano-8 Modern MathematiciansDocument2 pagesGan & Romano-8 Modern MathematiciansJerica GanNo ratings yet
- Herbertz Letter (Allen)Document1 pageHerbertz Letter (Allen)Matt HerbertzNo ratings yet
- Early Detection Key for SMA TreatmentDocument55 pagesEarly Detection Key for SMA TreatmentSnezana MihajlovicNo ratings yet
- Cerebrovascular Diseases Risk Factors:: o o o o oDocument4 pagesCerebrovascular Diseases Risk Factors:: o o o o otrinaNo ratings yet
- DD Nyeri Kepala Skenario 1Document8 pagesDD Nyeri Kepala Skenario 1Ika Putri YulianiNo ratings yet
- Parkinson Disease Pharmacotherapy GuideDocument91 pagesParkinson Disease Pharmacotherapy GuideHsn Tuyết HàNo ratings yet
- 07 BMDocument9 pages07 BMMajid KhanNo ratings yet
- CNS Pathology Fall 2009Document106 pagesCNS Pathology Fall 2009EllagEszNo ratings yet
- 01 VascularDocument31 pages01 VascularMalinda KarunaratneNo ratings yet
- Neisseria Meningitidis Strep Pneumoniae E. ColiDocument3 pagesNeisseria Meningitidis Strep Pneumoniae E. ColiÐr SalmaNo ratings yet
- Chapter 8Document57 pagesChapter 8بو تركيNo ratings yet
- Reinhard L. Friede M.D. (Auth.) - Developmental Neuropathology-Springer Vienna (1975) PDFDocument535 pagesReinhard L. Friede M.D. (Auth.) - Developmental Neuropathology-Springer Vienna (1975) PDFMuhammad HabiburrahmanNo ratings yet
- R&W Thematic UnitDocument28 pagesR&W Thematic Unitapi-275162743No ratings yet
- MSK Infection: Osteomyelitis and Septic Arthritis Diagnosis and TreatmentDocument5 pagesMSK Infection: Osteomyelitis and Septic Arthritis Diagnosis and TreatmentMajid Khan100% (1)
- Metabolic Bone DiseaseDocument41 pagesMetabolic Bone DiseaseVenerandaNo ratings yet
- Medical PG Quiz ResultsDocument654 pagesMedical PG Quiz ResultsTITAN IZZ HERENo ratings yet
- Stroke Cognitive Deficits PDFDocument19 pagesStroke Cognitive Deficits PDFBárbara Romero OlateNo ratings yet
- Colorado Health Foundation 2022 Pulse PollDocument97 pagesColorado Health Foundation 2022 Pulse PollMichael_Roberts2019No ratings yet
- Mitochondrial Encephalomyopathies (MEM)Document66 pagesMitochondrial Encephalomyopathies (MEM)Fatma KaledNo ratings yet
- Animal Model of EADocument13 pagesAnimal Model of EAzigurat00No ratings yet
- Electroconvulsive Therapy in Geriatric PsychiatryDocument15 pagesElectroconvulsive Therapy in Geriatric Psychiatryppico1963No ratings yet
- Cognitive Reserve From Theperspective of Preclinical Alzheimer DiseaseDocument17 pagesCognitive Reserve From Theperspective of Preclinical Alzheimer Diseaseppico1963No ratings yet
- Mec CronicaDocument29 pagesMec CronicaAlfredo Luis Arana MaqueraNo ratings yet
- Lewy Body Degenerations As Neuropsychiatric DisordersDocument21 pagesLewy Body Degenerations As Neuropsychiatric Disordersppico1963No ratings yet
- Tuberculosis of The Central Nervous SystemDocument17 pagesTuberculosis of The Central Nervous Systemnight.shadowNo ratings yet
- MOCADocument1 pageMOCAAna PimentelNo ratings yet
- Recomendacoes em Alzheimer PDFDocument108 pagesRecomendacoes em Alzheimer PDFreneverasNo ratings yet
- Hunt HessDocument1 pageHunt HessIqbal RahmansyahNo ratings yet
- Perda de Visao 2011Document11 pagesPerda de Visao 2011ppico1963No ratings yet
- Kleine-Levin Syndrome: A Systematic Review of 186 Cases in The LiteratureDocument14 pagesKleine-Levin Syndrome: A Systematic Review of 186 Cases in The Literatureppico1963No ratings yet
- Personal Development: Quarter 1 - Module 6Document28 pagesPersonal Development: Quarter 1 - Module 6JulieAnnLucasBagamaspad100% (1)
- A White Paper On The Future of Artificial IntelligenceDocument6 pagesA White Paper On The Future of Artificial IntelligenceGIRISHNo ratings yet
- Alzheimer'S Disease:: Pathophysiology and TreatmentDocument34 pagesAlzheimer'S Disease:: Pathophysiology and TreatmentKarthik KoneruNo ratings yet
- Solms - New ProjectDocument32 pagesSolms - New ProjectHugo Tannous Jorge100% (1)
- Hypnosis and Cingulate-Mediated Mechanisms of AnalgesiaDocument20 pagesHypnosis and Cingulate-Mediated Mechanisms of AnalgesiaCristian GondacNo ratings yet
- NCM 117 Maladaptive Patterns of Behavior: Rose Marla L. Fernando, RN, MANDocument64 pagesNCM 117 Maladaptive Patterns of Behavior: Rose Marla L. Fernando, RN, MANDhen Marc100% (1)
- Reading Paul PDFDocument10 pagesReading Paul PDFmega malikNo ratings yet
- The Clinical NeuropsychologistDocument13 pagesThe Clinical NeuropsychologistPriscila FreitasNo ratings yet
- How The Brain WorksDocument37 pagesHow The Brain WorksGerson Freire De Amorim FilhoNo ratings yet
- Lesson 3 He Neuromotor Basis For Motor ControlDocument46 pagesLesson 3 He Neuromotor Basis For Motor ControlDrift AlvinNo ratings yet
- 2 The BrainDocument21 pages2 The BrainLok YiuNo ratings yet
- CVS TreatmentDocument6 pagesCVS TreatmentNaguibYunosNo ratings yet
- Gongora2019 - Neurobiological Evidences Functional and Emotional Aspects Associated With The AmygdalaDocument18 pagesGongora2019 - Neurobiological Evidences Functional and Emotional Aspects Associated With The AmygdalaErick SolisNo ratings yet
- MRI Brain Anatomy Sections ExplainedDocument34 pagesMRI Brain Anatomy Sections Explainedsyafiqa abdullahNo ratings yet
- Francisco Aboitiz (Auth.) - A Brain For Speech - A View From Evolutionary Neuroanatomy-Palgrave Macmillan UK (2017)Document515 pagesFrancisco Aboitiz (Auth.) - A Brain For Speech - A View From Evolutionary Neuroanatomy-Palgrave Macmillan UK (2017)TecuitlatlNo ratings yet
- Untitled DocumentDocument2 pagesUntitled DocumentClaudia WinNo ratings yet
- Neuroanatomy & PhysiologyDocument44 pagesNeuroanatomy & PhysiologyKarina MawarnursaviraNo ratings yet
- How Children Develop Canadian 5th Edition Siegler Test BankDocument50 pagesHow Children Develop Canadian 5th Edition Siegler Test BankJasonMackjrwty100% (16)
- Gurdjieff - A Symbol of The Cosmos and Its Laws (K.a.buzzell)Document12 pagesGurdjieff - A Symbol of The Cosmos and Its Laws (K.a.buzzell)Txus666No ratings yet
- Solso, Robert L. - Cognitive Psychology-Pearson (2013) - KOGNITIF PDFDocument533 pagesSolso, Robert L. - Cognitive Psychology-Pearson (2013) - KOGNITIF PDFNabiela Rahmadiana P91% (11)
- Forensic Hair Analysis: Identifying Species, Race, Drugs & DNADocument21 pagesForensic Hair Analysis: Identifying Species, Race, Drugs & DNATJPlayzNo ratings yet
- Basal Ganglia (Edit)Document66 pagesBasal Ganglia (Edit)kkkaadashfisafNo ratings yet
- Pathophysiology of Migraine.5Document11 pagesPathophysiology of Migraine.5Bryan100% (1)
- 2015 Movement DisordersDocument567 pages2015 Movement DisordersAndreea Raluca CimpoiNo ratings yet
- NeurophysiologyDocument72 pagesNeurophysiologyRizki DaulayNo ratings yet
- Oasis-3: Imaging Methods and Data Dictionary: Version 1.6 April 2018Document32 pagesOasis-3: Imaging Methods and Data Dictionary: Version 1.6 April 2018murlak37No ratings yet
- NppcityDocument63 pagesNppcityMohammad JoharNo ratings yet
- Neuroanatomy Final Flashcards - QuizletDocument17 pagesNeuroanatomy Final Flashcards - QuizletFaten AklanNo ratings yet
- Chapter 33 Theory of Mind 3Document12 pagesChapter 33 Theory of Mind 3Costrut Laur100% (3)
- Motor Impairments Following StrokeDocument31 pagesMotor Impairments Following StrokeFrancess LeveauNo ratings yet