You might also like
- Alinhador Fixturlaser DirigoDocument2 pagesAlinhador Fixturlaser DirigoJossesmsNo ratings yet
- Melissa Gomroki CVDocument2 pagesMelissa Gomroki CVapi-618835422No ratings yet
- Palliative Sedation Therapy in The Last Weeks of Life: A Literature Review and Recommendations For StandardsDocument19 pagesPalliative Sedation Therapy in The Last Weeks of Life: A Literature Review and Recommendations For StandardsMárcia MatosNo ratings yet
- Inbound 2197063521713227868Document11 pagesInbound 2197063521713227868NylNo ratings yet
- Construction Site PremisesDocument78 pagesConstruction Site PremisesDrew B Mrtnz67% (6)
- 11 - FORAGERS by Sam BoyerDocument106 pages11 - FORAGERS by Sam BoyerMurtaza HussainNo ratings yet
- Galactic Handbook and Synchronized MeditationsDocument91 pagesGalactic Handbook and Synchronized Meditationslapiton100% (10)
- NOTES - Freedom and ResponsibilityDocument7 pagesNOTES - Freedom and ResponsibilitySonnel CalmaNo ratings yet
- Arizona Independent Republic Nov 30 1938 P 42Document1 pageArizona Independent Republic Nov 30 1938 P 42Hailey LongNo ratings yet
- Expert System Assessing Threat Level of Attacks On A Hybrid SSH HoneynetDocument19 pagesExpert System Assessing Threat Level of Attacks On A Hybrid SSH HoneynetCoder CoderNo ratings yet
- Fs 4-2Document6 pagesFs 4-2api-598987483No ratings yet
- OHS-PR-09-03-F07 JOB SAFE PROCEDURE (02) Access Road and Structure PadDocument14 pagesOHS-PR-09-03-F07 JOB SAFE PROCEDURE (02) Access Road and Structure Padmohammed tofiqNo ratings yet
- Gan & Romano-8 Modern MathematiciansDocument2 pagesGan & Romano-8 Modern MathematiciansJerica GanNo ratings yet
- Practice of Washing of Hand Using Liquid Detergent Among Pupils in Owerri Municipal A Tool For Health Promotion and Health SecurityDocument5 pagesPractice of Washing of Hand Using Liquid Detergent Among Pupils in Owerri Municipal A Tool For Health Promotion and Health SecurityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ball and Beam WorkbookDocument31 pagesBall and Beam WorkbookCicero MelloNo ratings yet
- Handwriting Differences in Individuals With Presence and Absence of Antisocial BehaviourDocument37 pagesHandwriting Differences in Individuals With Presence and Absence of Antisocial BehaviourEditor IJTSRDNo ratings yet
- VJpSdQX3edKaXNEa 289Document40 pagesVJpSdQX3edKaXNEa 289Jesslyn AmbrocioNo ratings yet
- Cell MetabDocument21 pagesCell MetabgassemNo ratings yet
- EErcDocument108 pagesEErcRohit Ramesh KaleNo ratings yet
- Sexual abuse of females in organizations and its impact on job satisfactionDocument24 pagesSexual abuse of females in organizations and its impact on job satisfactionNatasha kumariNo ratings yet
- Medically Unexplained Symptoms Assessment and ManagementDocument6 pagesMedically Unexplained Symptoms Assessment and ManagementMatheus AzevedoNo ratings yet
- BECE Past Questions RME Objectives 2013-WPS OfficeDocument11 pagesBECE Past Questions RME Objectives 2013-WPS OfficeBENNo ratings yet
- Barron's - 2022.09.26Document63 pagesBarron's - 2022.09.26EDGAR BAUTISTA LEONNo ratings yet
- Bioterrorism An IntroductionDocument6 pagesBioterrorism An IntroductionEditor IJTSRD100% (1)
- PEER: Issue Brief: Mississippi Department of Corrections Accountability Program InventoryDocument49 pagesPEER: Issue Brief: Mississippi Department of Corrections Accountability Program InventoryRuss LatinoNo ratings yet
- Assessment and Feedback in Higher EducatDocument67 pagesAssessment and Feedback in Higher EducatSonja AndjelkovNo ratings yet
- Z-TV Guide 2022Document9 pagesZ-TV Guide 2022Cooperation and Conflict LabNo ratings yet
- SNCO COVID-19 Community Indicator Report 12-9-2021Document4 pagesSNCO COVID-19 Community Indicator Report 12-9-2021Michael K. DakotaNo ratings yet
- Barren Island Ph1 Safety FactsheetDocument2 pagesBarren Island Ph1 Safety FactsheetKevin ParkerNo ratings yet
- Ricci Psichiatriabun - It.enDocument122 pagesRicci Psichiatriabun - It.enCosmin DeaconuNo ratings yet
- 1 s2.0 S2590116822000030 MainDocument19 pages1 s2.0 S2590116822000030 MainJIANG LYUNo ratings yet
- Structure-Mapping: A Theoretical Framework For Analogy : Bolt Beranek and Newman IncDocument16 pagesStructure-Mapping: A Theoretical Framework For Analogy : Bolt Beranek and Newman IncVioleta PrietoNo ratings yet
- EMERALD TrialDocument13 pagesEMERALD TrialCristian MuñozNo ratings yet
- Univ317 Final 5Document3 pagesUniv317 Final 5Bagas KaraNo ratings yet
- Commonwealth V Malone May 1946Document44 pagesCommonwealth V Malone May 1946MindSpaceApocalypseNo ratings yet
- Alkaloids: DR N AhmedDocument23 pagesAlkaloids: DR N AhmedMohammad SamirNo ratings yet
- Birdflu 666Document406 pagesBirdflu 666sligomcNo ratings yet
- Mid TernDocument13 pagesMid TernRevy CumahigNo ratings yet
- Test Series: April, 2021 Mock Test Paper 2 Final (Old) Course Paper 1: Financial ReportingDocument16 pagesTest Series: April, 2021 Mock Test Paper 2 Final (Old) Course Paper 1: Financial ReportingPraveen Reddy DevanapalleNo ratings yet
- Essential guide to implementing newborn screening nationwideDocument300 pagesEssential guide to implementing newborn screening nationwideJosanne Wadwadan De CastroNo ratings yet
- Lanka Arrests 12 Fishermen Stalin Asks PM To Intervene: U'khand, Goa Go To Booths TodayDocument12 pagesLanka Arrests 12 Fishermen Stalin Asks PM To Intervene: U'khand, Goa Go To Booths TodayS AkashNo ratings yet
- AccountingDocument15 pagesAccountingRahul agarwalNo ratings yet
- Own Own Body Own Final ComprimidoDocument20 pagesOwn Own Body Own Final Comprimidoapi-609236458100% (1)
- Typical goals of malware and their implementationsDocument47 pagesTypical goals of malware and their implementationsSaluu TvTNo ratings yet
- Grizzly Industrial, 15" Planer Instruction ManualDocument45 pagesGrizzly Industrial, 15" Planer Instruction ManualkatfishisgreatNo ratings yet
- ChargesDocument62 pagesChargessudhirNo ratings yet
- Clinical Assessment of Antibiotic Use in CKD PatientsDocument8 pagesClinical Assessment of Antibiotic Use in CKD PatientsMITA RESTINIA UINJKTNo ratings yet
- CGL 2020 GST Inspector, Po & Examiner State Wise VacancyDocument8 pagesCGL 2020 GST Inspector, Po & Examiner State Wise VacancyAmlan DuttaNo ratings yet
- Enduro World Series 2022 - #3 Val Di Fassa - Day 1Document30 pagesEnduro World Series 2022 - #3 Val Di Fassa - Day 1MTB-VCONo ratings yet
- Financial Analysis of Indian Oil CorporationDocument29 pagesFinancial Analysis of Indian Oil CorporationNikshith HegdeNo ratings yet
- Manual Therapy: Critical Assessment Profession of Physical Therapy Role TheDocument10 pagesManual Therapy: Critical Assessment Profession of Physical Therapy Role TheManuel Silva HérnandezNo ratings yet
- A1 Speaking Book FINALDocument60 pagesA1 Speaking Book FINALVũ Quốc ĐạiNo ratings yet
- TiC CMS RecsDocument4 pagesTiC CMS RecsJakob EmersonNo ratings yet
- Colorado Health Foundation 2022 Pulse PollDocument97 pagesColorado Health Foundation 2022 Pulse PollMichael_Roberts2019No ratings yet
- Bài tập tự động hóa sản xuất - 0001-0001Document1 pageBài tập tự động hóa sản xuất - 0001-0001Minh NhậtNo ratings yet
- 10 1021@acs Iecr 0c00181Document42 pages10 1021@acs Iecr 0c00181JUAN EDUARDO LEON HUAMANINo ratings yet
- Harris SX-1 Operators ManualDocument46 pagesHarris SX-1 Operators ManualLuis AhmedNo ratings yet
- Business License Revocation Letter. Naomi I. Halter.1Document3 pagesBusiness License Revocation Letter. Naomi I. Halter.1T RNo ratings yet
- Guide to Writing Effective Essays for English Proficiency TestsDocument25 pagesGuide to Writing Effective Essays for English Proficiency Testslê myNo ratings yet
- Representations and Implications of Papers Written by E.T. Whittaker in 1903 and 1904 (Latex PDFDocument6 pagesRepresentations and Implications of Papers Written by E.T. Whittaker in 1903 and 1904 (Latex PDFMark TitlemanNo ratings yet
- Chapter 8Document57 pagesChapter 8بو تركيNo ratings yet
- 723 FullDocument11 pages723 Fullclaudia velaNo ratings yet
- cVEMP y oVEMP en ESCLEROSIS MULTIPLEDocument8 pagescVEMP y oVEMP en ESCLEROSIS MULTIPLEJaneth GuzmanNo ratings yet
- Ni602201-1217753 032257Document10 pagesNi602201-1217753 032257Vinay GNo ratings yet
- WdweDocument7 pagesWdweVinay GNo ratings yet
- CP Angle SOLDocument8 pagesCP Angle SOLVinay GNo ratings yet
- 55 Year Old Male With Back Pain and RadiculopathyDocument7 pages55 Year Old Male With Back Pain and RadiculopathyVinay GNo ratings yet
- Bhagavad Gita - With Sri Shankaracharya CommentaryDocument508 pagesBhagavad Gita - With Sri Shankaracharya CommentaryEstudante da Vedanta100% (24)
- CerebellumDocument10 pagesCerebellumVinay GNo ratings yet
- Comparing The Efficacy of Short Segment Pedicle.43Document5 pagesComparing The Efficacy of Short Segment Pedicle.43Vinay GNo ratings yet
- My File TDocument1 pageMy File TVinay GNo ratings yet
- My File To DownloadsDocument1 pageMy File To DownloadsVinay GNo ratings yet
- My File TDocument1 pageMy File TVinay GNo ratings yet
- My File To DownloadsDocument1 pageMy File To DownloadsVinay GNo ratings yet
- Gane SanDocument7 pagesGane SanVinay GNo ratings yet
- My File To DownloaDocument1 pageMy File To DownloaVinay GNo ratings yet
- My File To DownloadDocument1 pageMy File To DownloadVinay GNo ratings yet
- My FileDocument1 pageMy FileVinay GNo ratings yet
- My FileDocument1 pageMy FileVinay GNo ratings yet
- 0610 m16 QP 62Document12 pages0610 m16 QP 62faryal khanNo ratings yet
- Chapter 14 Chemical EquilibriumDocument29 pagesChapter 14 Chemical EquilibriumlynloeNo ratings yet
- S2 Papers FinalizedDocument149 pagesS2 Papers FinalizedRaffles HolmesNo ratings yet
- A Review: HPLC Method Development and Validation: November 2015Document7 pagesA Review: HPLC Method Development and Validation: November 2015R Abdillah AkbarNo ratings yet
- Common Mistakes in Dimensional Calibration MethodsDocument16 pagesCommon Mistakes in Dimensional Calibration MethodssujudNo ratings yet
- Textile Internship Report AlokDocument39 pagesTextile Internship Report AlokRahul TelangNo ratings yet
- Tejas: Practice Sheet JEE PhysicsDocument3 pagesTejas: Practice Sheet JEE PhysicsAshree KesarwaniNo ratings yet
- Essay - DnaDocument2 pagesEssay - Dnaapi-243852896No ratings yet
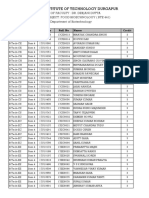
- List of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFDocument26 pagesList of Students Allotted in Open Elective Subjects (B. Tech and M. Tech (Dual Degree) Integrated MSc. - 4th Semester - Regular - 2018 - 19) - 2 PDFArpan JaiswalNo ratings yet
- MidtermDocument3 pagesMidtermTrisha MondonedoNo ratings yet
- Philips HF C-Arm BrochureDocument2 pagesPhilips HF C-Arm Brochuregarysov50% (2)
- BAlochistanDocument14 pagesBAlochistanzee100% (1)
- Musical Siren Project Report Under 40 CharactersDocument10 pagesMusical Siren Project Report Under 40 Charactersvinod kapateNo ratings yet
- GLOBAL GAME AFK IN THE ZOMBIE APOCALYPSE GAME Chapter 201-250Document201 pagesGLOBAL GAME AFK IN THE ZOMBIE APOCALYPSE GAME Chapter 201-250ganesh sarikondaNo ratings yet
- MD R2 Nastran Release GuideDocument276 pagesMD R2 Nastran Release GuideMSC Nastran BeginnerNo ratings yet
- Detecting Oil Spills from Remote SensorsDocument7 pagesDetecting Oil Spills from Remote SensorsFikri Adji Wiranto100% (1)
- Chemistry of Food Changes During Storage: Group 7Document22 pagesChemistry of Food Changes During Storage: Group 7Sonny MichaelNo ratings yet
- Managed Pressure Drilling MPD BrochureDocument5 pagesManaged Pressure Drilling MPD Brochureswaala4realNo ratings yet
- Understanding of AVO and Its Use in InterpretationDocument35 pagesUnderstanding of AVO and Its Use in Interpretationbrian_schulte_esp803100% (1)
- Well Rounded.: 360 CassetteDocument12 pagesWell Rounded.: 360 CassetteMonty Va Al MarNo ratings yet
- Rajagiri Public School Unit Test PhysicsDocument3 pagesRajagiri Public School Unit Test PhysicsNITHINKJOSEPHNo ratings yet
- PMR205 DR Shawn BakerDocument31 pagesPMR205 DR Shawn Bakerspiridon_andrei2011No ratings yet
- Barney's Great Adventure - Barney Wiki - WikiaDocument2 pagesBarney's Great Adventure - Barney Wiki - WikiachefchadsmithNo ratings yet
- Week 7: Nurses Role in Disaster: Home Mitigation and PreparednessDocument10 pagesWeek 7: Nurses Role in Disaster: Home Mitigation and PreparednessRose Ann LacuarinNo ratings yet
- Bosch EBike Product Catalogue MY2021 enDocument92 pagesBosch EBike Product Catalogue MY2021 enIvanNo ratings yet
- State of The Art in Roller Compacted Concrete (RCC) PDFDocument226 pagesState of The Art in Roller Compacted Concrete (RCC) PDFEduardoDavilaOrtegaNo ratings yet
- EE 102 Cabric Final Spring08 o Id15Document10 pagesEE 102 Cabric Final Spring08 o Id15Anonymous TbHpFLKNo ratings yet