You might also like
- Creatine Phosphokinase TestDocument7 pagesCreatine Phosphokinase TestAhsan KhanNo ratings yet
- Patient Diagnosed With Myocardial Infarct M006Document11 pagesPatient Diagnosed With Myocardial Infarct M006Kefix WritersHubNo ratings yet
- PheoDocument4 pagesPheoantonijevicuNo ratings yet
- Nbme 5.1Document54 pagesNbme 5.1Hafsa SafdarNo ratings yet
- Cindy M. Minasalbas BSN-401 Immunodeficiency Disorders: How The Test Is PerformedDocument17 pagesCindy M. Minasalbas BSN-401 Immunodeficiency Disorders: How The Test Is PerformedAlvin Binoy LazarraNo ratings yet
- Medical Surgical ManagementDocument13 pagesMedical Surgical ManagementNikki BrodethNo ratings yet
- Case Study of Anterior Wall MI 48Document32 pagesCase Study of Anterior Wall MI 48سوما الشمريNo ratings yet
- Cardiac BiomarDocument34 pagesCardiac BiomarVaibhav KaroliyaNo ratings yet
- Purpose: Lymphoma Lupus Giant Cell Arteritis Rheumatoid Arthritis Inflammatory Bowel Disease OsteomyelitisDocument5 pagesPurpose: Lymphoma Lupus Giant Cell Arteritis Rheumatoid Arthritis Inflammatory Bowel Disease OsteomyelitisJenny Rose Lademora CorderoNo ratings yet
- Medical Management For Cerobvascular DiseaseDocument5 pagesMedical Management For Cerobvascular DiseaseCyrill Alexandria TolentinoNo ratings yet
- Current Clinical Strategies, Critical Care and Cardiac Medicine (2005) BM OCR 7.0-2Document79 pagesCurrent Clinical Strategies, Critical Care and Cardiac Medicine (2005) BM OCR 7.0-2api-3709022100% (2)
- PBL PgamboaDocument6 pagesPBL PgamboaLeanne Princess GamboaNo ratings yet
- Clinical Chemistry Activity 2Document9 pagesClinical Chemistry Activity 2loona oneNo ratings yet
- Junetta Cooper Vsim Prep 2Document5 pagesJunetta Cooper Vsim Prep 2Michelle Pinkhasova100% (2)
- CVADocument4 pagesCVACloyd Marvin Pajas SegundoNo ratings yet
- Usmle 2ck Practice Questions All 2015Document6 pagesUsmle 2ck Practice Questions All 2015Sharmela BrijmohanNo ratings yet
- Ischemic Stroke: Laboratory StudiesDocument21 pagesIschemic Stroke: Laboratory Studieskuchaibaru90No ratings yet
- Kayse White SNRN Case Study Leukemia With Bone Marrow TransplantDocument5 pagesKayse White SNRN Case Study Leukemia With Bone Marrow TransplantIssaiah Nicolle CeciliaNo ratings yet
- PracticeExam CCSDocument12 pagesPracticeExam CCSBehrouz Yari75% (4)
- (Osborn Chapter) 40: Learning Outcomes (Number and Title)Document23 pages(Osborn Chapter) 40: Learning Outcomes (Number and Title)KittiesNo ratings yet
- Cardiology Literature ReviewDocument8 pagesCardiology Literature Reviewaflsvwoeu100% (2)
- Bleeding DisorderDocument56 pagesBleeding DisorderPriya Singh100% (1)
- PBL Vii Fix BeetDocument33 pagesPBL Vii Fix BeetNUR AFRI NINGSIHNo ratings yet
- Prognostic Value of Increased Soluble Thrornbornodulin and Increased Soluble E-Selectin in Ischaernic Heart DiseaseDocument6 pagesPrognostic Value of Increased Soluble Thrornbornodulin and Increased Soluble E-Selectin in Ischaernic Heart DiseaseIoanna Bianca HNo ratings yet
- Clin Cardiology CasesDocument34 pagesClin Cardiology CasesSunny Singh0% (1)
- 3 NopalpamogasDocument5 pages3 NopalpamogasFeb NamiaNo ratings yet
- Cesar - Cardio & HemaDocument77 pagesCesar - Cardio & HemakdfhjfhfNo ratings yet
- Untitled Document - Edited - 2022-07-16T015625.553Document3 pagesUntitled Document - Edited - 2022-07-16T015625.553Moses WabunaNo ratings yet
- Health Assessment in Nursing (LEC) : Prepared By: Mark Joseph V. Liwanag, RN, MSNDocument43 pagesHealth Assessment in Nursing (LEC) : Prepared By: Mark Joseph V. Liwanag, RN, MSNCj MayoyoNo ratings yet
- 5 - Clinical 1Document21 pages5 - Clinical 1levan guluaNo ratings yet
- Various Blood InvestigationsDocument59 pagesVarious Blood InvestigationsRiteka SinghNo ratings yet
- Group 8 - Case 5 - Hypothetical Case For AnalysisDocument39 pagesGroup 8 - Case 5 - Hypothetical Case For AnalysisHyun Jae WonNo ratings yet
- Amarenco, 2020Document11 pagesAmarenco, 2020luccafcms56No ratings yet
- Phphenylephrine Vs EphedrinerineDocument42 pagesPhphenylephrine Vs EphedrinerineDr.Deb Sanjay NagNo ratings yet
- Nursing Care Plan Sample For BeginnersDocument15 pagesNursing Care Plan Sample For BeginnersMoe KhanNo ratings yet
- Cardiac Diagnostic TestsDocument14 pagesCardiac Diagnostic TestsSimran Josan100% (5)
- 16464-Article Text-54657-1-10-20170124Document4 pages16464-Article Text-54657-1-10-20170124Aashish KalikaNo ratings yet
- Diagnostic Tool: Complete Blood CountDocument14 pagesDiagnostic Tool: Complete Blood Countjoanna gurtizaNo ratings yet
- Laboratory StudiesDocument4 pagesLaboratory StudiesNapelyn Pinero DisimulacionNo ratings yet
- Laboratory StudiesDocument4 pagesLaboratory StudiesNapelyn Pinero DisimulacionNo ratings yet
- Stress Testing and ECG.. (Poonam Soni)Document14 pagesStress Testing and ECG.. (Poonam Soni)Poonam soniNo ratings yet
- Disusun Untuk Memenuhi Tugas Bahasa Inggris Dosen Pembimbing: Widjijati, MNDocument4 pagesDisusun Untuk Memenuhi Tugas Bahasa Inggris Dosen Pembimbing: Widjijati, MNSalsabilla KimikoNo ratings yet
- Pathophysiology and Investigation of Coronary Artery DiseaseDocument4 pagesPathophysiology and Investigation of Coronary Artery DiseasekartikaparamitaNo ratings yet
- Nstemi and Stemi: Therapeutic Updates 2011: AuthorDocument9 pagesNstemi and Stemi: Therapeutic Updates 2011: AuthorAfdol Triatmojo SikumbangNo ratings yet
- Comparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsDocument54 pagesComparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsJagannadha Rao PeelaNo ratings yet
- Data Interpretation For Medical StudentDocument18 pagesData Interpretation For Medical StudentWee K WeiNo ratings yet
- UQU SLE CORRECTED FILE by DR Samina FidaDocument537 pagesUQU SLE CORRECTED FILE by DR Samina Fidaasma .sassi100% (1)
- Role of Biochemical Markers in Diagnosis of Myocardial InfarctionDocument3 pagesRole of Biochemical Markers in Diagnosis of Myocardial InfarctionAlexandra ApostoaeNo ratings yet
- UntitledDocument2 pagesUntitledOleOhhNo ratings yet
- BACKGROUND: Through Thrombolysis Is The Ideal Treatment For CardiacDocument2 pagesBACKGROUND: Through Thrombolysis Is The Ideal Treatment For CardiacOleOhhNo ratings yet
- Review Articles: Medical ProgressDocument10 pagesReview Articles: Medical ProgressMiko AkmarozaNo ratings yet
- Slides Congestive Heart FailureDocument113 pagesSlides Congestive Heart FailureRegina ZalukhuNo ratings yet
- Case StudyDocument6 pagesCase StudyMarie-Suzanne Tanyi100% (1)
- Haemodynamic Monitoring & Manipulation: an easy learning guideFrom EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNo ratings yet
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesFrom EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesRating: 5 out of 5 stars5/5 (1)
- Sports Cardiology: Care of the Athletic Heart from the Clinic to the SidelinesFrom EverandSports Cardiology: Care of the Athletic Heart from the Clinic to the SidelinesDavid J. EngelNo ratings yet
- CV 2023010319584829Document1 pageCV 2023010319584829Asniah Hadjiadatu AbdullahNo ratings yet
- Application Forms (Fillable)Document2 pagesApplication Forms (Fillable)Asniah Hadjiadatu AbdullahNo ratings yet
- Health Teaching Plan FinaleDocument4 pagesHealth Teaching Plan FinaleAsniah Hadjiadatu AbdullahNo ratings yet
- Nursing Notes Maternal and Child Nursing CareDocument70 pagesNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahNo ratings yet
- Pnle ReviewerDocument293 pagesPnle ReviewerAsniah Hadjiadatu Abdullah94% (18)
- Credential Verification Form Non-Clinical (Without Signature Page)Document1 pageCredential Verification Form Non-Clinical (Without Signature Page)Asniah Hadjiadatu AbdullahNo ratings yet
- Daniel Saladas ResumeDocument2 pagesDaniel Saladas ResumeAsniah Hadjiadatu AbdullahNo ratings yet
- To Fill-Up Id-Atm FormDocument7 pagesTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahNo ratings yet
- FNCP PoorsanitationmarwahDocument3 pagesFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahNo ratings yet
- Poor Compliance With Treatment As Health Threat CuesDocument11 pagesPoor Compliance With Treatment As Health Threat CuesAsniah Hadjiadatu AbdullahNo ratings yet
- Poor Environmetal Sanitation As Health Threat CuesDocument11 pagesPoor Environmetal Sanitation As Health Threat CuesAsniah Hadjiadatu AbdullahNo ratings yet
- Family Case Study On Pulmonary TuberculosisDocument4 pagesFamily Case Study On Pulmonary TuberculosisAsniah Hadjiadatu AbdullahNo ratings yet
- Family Case StudyDocument33 pagesFamily Case StudyAsniah Hadjiadatu AbdullahNo ratings yet
- Family Case Study PresentationDocument1 pageFamily Case Study PresentationAsniah Hadjiadatu AbdullahNo ratings yet
- Or/Dr/Nicu/Pacu Requirements: Open Wound TypesDocument6 pagesOr/Dr/Nicu/Pacu Requirements: Open Wound TypesAsniah Hadjiadatu AbdullahNo ratings yet
- Mock ResumeDocument3 pagesMock ResumeAsniah Hadjiadatu AbdullahNo ratings yet
- Water RescueDocument7 pagesWater RescueAsniah Hadjiadatu AbdullahNo ratings yet
- History: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentDocument4 pagesHistory: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentAsniah Hadjiadatu AbdullahNo ratings yet
- Proposed Budget For The 17th Striping and Pinning Investiture CeremonyDocument1 pageProposed Budget For The 17th Striping and Pinning Investiture CeremonyAsniah Hadjiadatu AbdullahNo ratings yet
- Health EDUC Teaching Demo RubricsDocument4 pagesHealth EDUC Teaching Demo RubricsAsniah Hadjiadatu Abdullah100% (1)
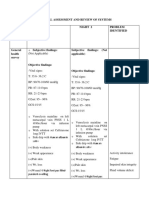
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDocument9 pagesPhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahNo ratings yet
- Concept Map AtekharlssDocument3 pagesConcept Map AtekharlssAsniah Hadjiadatu AbdullahNo ratings yet
- Assessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationDocument11 pagesAssessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationAsniah Hadjiadatu Abdullah100% (1)
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDocument12 pagesAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNo ratings yet
- Psychiatric-Mental Health NursingDocument6 pagesPsychiatric-Mental Health NursingAsniah Hadjiadatu AbdullahNo ratings yet
- Final Nursing CareplanDocument7 pagesFinal Nursing CareplanAsniah Hadjiadatu AbdullahNo ratings yet
- ECG Diagnosis: Right Ventricular Myocardial Infarction: Clinical MedicineDocument2 pagesECG Diagnosis: Right Ventricular Myocardial Infarction: Clinical MedicineNadyaindriati96No ratings yet
- AXA Non Death Claim FormDocument4 pagesAXA Non Death Claim FormKenji ChinNo ratings yet
- Heart Disease: - T.Priyadharshini Ece-3 YearDocument14 pagesHeart Disease: - T.Priyadharshini Ece-3 Yearpriya ThennarasuNo ratings yet
- MS Compre 2015A Ans KeyDocument8 pagesMS Compre 2015A Ans KeyPaul Lexus Gomez LorenzoNo ratings yet
- HDFC Life Click 2 Protect Life - Product Brochure PDFDocument24 pagesHDFC Life Click 2 Protect Life - Product Brochure PDFvaibhav kumar KhokharNo ratings yet
- Interventional Endos PDFDocument559 pagesInterventional Endos PDFBrenda De Anda100% (1)
- Aircraft Accident ReportDocument9 pagesAircraft Accident ReportMuhammad AsyrafNo ratings yet
- Preventive Cardiology: Textbook of Cardiovascular Medicine-2nd EditionDocument4 pagesPreventive Cardiology: Textbook of Cardiovascular Medicine-2nd EditionBintun NahlNo ratings yet
- Case Studies Therapy 1Document9 pagesCase Studies Therapy 1WONDWOSSEN ALEMUNo ratings yet
- Fuck ShitDocument11 pagesFuck Shitkrull243100% (2)
- Cardiovascular Disease Nursing Diagnosis - Causes - FactsDocument3 pagesCardiovascular Disease Nursing Diagnosis - Causes - Factsfeirri0% (1)
- Prognosis and Outcomes Following Sudden Cardiac Arrest in AdultsDocument24 pagesPrognosis and Outcomes Following Sudden Cardiac Arrest in AdultsAnca StanNo ratings yet
- Mymaxicare Brochure 2022 1.5.22Document16 pagesMymaxicare Brochure 2022 1.5.22Charie GemaoNo ratings yet
- Family Medicine Textbook Notes PDFDocument174 pagesFamily Medicine Textbook Notes PDFJack GuccioneNo ratings yet
- Speaking Test Avcn 1: Unit 1: Hospital StaffDocument5 pagesSpeaking Test Avcn 1: Unit 1: Hospital StaffHoàng Huy NguyễnNo ratings yet
- The Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Document12 pagesThe Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Jonathan Ian ArinsolNo ratings yet
- RE Josefina D. Farrales, A.M. Nos. 06-3-196-RTC & A.M. No. 06-7-416-RTC PDFDocument31 pagesRE Josefina D. Farrales, A.M. Nos. 06-3-196-RTC & A.M. No. 06-7-416-RTC PDFJohzzyluck R. MaghuyopNo ratings yet
- Medical-Surgical Nursing Exam 16cardiovascular Nursing (60 Items)Document19 pagesMedical-Surgical Nursing Exam 16cardiovascular Nursing (60 Items)Heather ClemonsNo ratings yet
- Pharmacotherapeutics - PharmD II YearDocument5 pagesPharmacotherapeutics - PharmD II YearSuresh Thanneru100% (2)
- Pengetahuan Mengenai Faktor Risiko Dan Perilaku Pasien Sindrom Koroner Akut Jeki RefialdinataDocument10 pagesPengetahuan Mengenai Faktor Risiko Dan Perilaku Pasien Sindrom Koroner Akut Jeki RefialdinataFATIMAH WANDANo ratings yet
- Mpu3313 - V2 Health & Wellness 2 AssigmentDocument15 pagesMpu3313 - V2 Health & Wellness 2 Assigmentsentamilarsi arumugamNo ratings yet
- Radiology Semiotics of Diseases of Various SystemDocument7 pagesRadiology Semiotics of Diseases of Various Systemnikhil gendreNo ratings yet
- First Aid Q&A PDFDocument764 pagesFirst Aid Q&A PDFStephanie Williams100% (9)
- Lecture 12 Cardio Intensive CasesDocument32 pagesLecture 12 Cardio Intensive Casesraul0% (1)
- Angina Set #8Document26 pagesAngina Set #8Zaid Al-KadhimiNo ratings yet
- ASPREE Definición de Desenlace CompuestoDocument32 pagesASPREE Definición de Desenlace CompuestoYesica Villalba CerqueraNo ratings yet
- Biology - MYP 3 - 31st AugustDocument6 pagesBiology - MYP 3 - 31st Augustarchit.kulkarni7756No ratings yet
- Acute Chest Pain of Cardiac OriginDocument32 pagesAcute Chest Pain of Cardiac OriginKhurram NadeemNo ratings yet
- JCI International Library of MeasuresDocument261 pagesJCI International Library of MeasuresDedy Haris DeswandarNo ratings yet