You might also like
- Jurnal Studi Karakteristik Mekanik Beton Dengan Menggunakan Agregat Halus Tailing Dengan Variasi Serat BajaDocument13 pagesJurnal Studi Karakteristik Mekanik Beton Dengan Menggunakan Agregat Halus Tailing Dengan Variasi Serat BajaIrsas InsanilNo ratings yet
- Draft Justek V.O 07 Partial Taking OverDocument14 pagesDraft Justek V.O 07 Partial Taking OverFahmi PratamaNo ratings yet
- Honor TukangDocument13 pagesHonor TukangimasNo ratings yet
- PDF RMPK CompressDocument47 pagesPDF RMPK CompressYoan SulistiyoNo ratings yet
- Lampiran RabDocument27 pagesLampiran RabDENTISA GARININo ratings yet
- Ustek PjuDocument8 pagesUstek PjuBoetjah ChihuahuaaNo ratings yet
- Tech Companies Rethink Inventory ManagementDocument12 pagesTech Companies Rethink Inventory Managementankitmiddha1No ratings yet
- Evaluasi Tingkat Kerusakan JalanDocument13 pagesEvaluasi Tingkat Kerusakan JalanMuammar MuisNo ratings yet
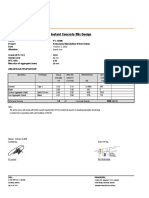
- Instant Concrete Mix DesignDocument1 pageInstant Concrete Mix DesignJoel Alfonso ManurungNo ratings yet
- Billing Rate InkindoDocument3 pagesBilling Rate InkindoJames HammondNo ratings yet
- PT. KARTIKA ASRI PRIMA 1 M3 SLOOF PAGAR PRICE ANALYSISDocument2 pagesPT. KARTIKA ASRI PRIMA 1 M3 SLOOF PAGAR PRICE ANALYSISAang HerieNo ratings yet
- RAB PipaDocument8 pagesRAB PipaMucin Mocn100% (1)
- Cover EeDocument3 pagesCover EeFanny Namakule LewierNo ratings yet
- Printronix P5000 Line Matrix Printers Maintenance ManualDocument410 pagesPrintronix P5000 Line Matrix Printers Maintenance ManualLee113880% (5)
- Boarding PassDocument1 pageBoarding PassNorhanisah HanNo ratings yet
- Pemberi Tugas Kepolisian Negara Republik IndonesiaDocument1 pagePemberi Tugas Kepolisian Negara Republik IndonesiaArsitek Iskandar Ilyas SemendawaiNo ratings yet
- Sms AdcircDocument19 pagesSms AdcircHeb RuNo ratings yet
- 1.lampiran SONDIR Tasik Malaya PDFDocument31 pages1.lampiran SONDIR Tasik Malaya PDFDhie NydhaMonichNo ratings yet
- Standar Kode Internasional Tek - SipilDocument2 pagesStandar Kode Internasional Tek - SipilAgunXwidodoNo ratings yet
- BaskomDocument8 pagesBaskomKrisnandha RahardianNo ratings yet
- Formulir TKDN Gabungan Barang dan JasaDocument15 pagesFormulir TKDN Gabungan Barang dan JasaAhmad JazuliNo ratings yet
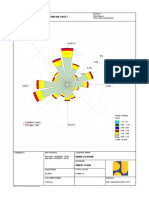
- Windrose - Dry Season (Apr-Oct)Document1 pageWindrose - Dry Season (Apr-Oct)Edi AriyantoNo ratings yet
- RAB APLIKASI GALANGAN KAPAL BAGAN SIAPI-APIDocument9 pagesRAB APLIKASI GALANGAN KAPAL BAGAN SIAPI-APIBagusPrambudiNo ratings yet
- Rencana Anggaran Biaya Dock To Dock: Pekerjaan Pemasangan Central & Instalasi Gas LPGDocument1 pageRencana Anggaran Biaya Dock To Dock: Pekerjaan Pemasangan Central & Instalasi Gas LPGShasa HarihandiniNo ratings yet
- Tutorial Manual Plaxis V7.2Document118 pagesTutorial Manual Plaxis V7.2Muhammad Rizal PahlevyNo ratings yet
- Hotel Reliability Assessment After 20 YearsDocument8 pagesHotel Reliability Assessment After 20 YearsSyukri IndrawansyahNo ratings yet
- Fair RPLDocument61 pagesFair RPLAliphi Yudhistira AstineNo ratings yet
- 12,000 DWT Barge Specs and DetailsDocument2 pages12,000 DWT Barge Specs and DetailsIqbal AbidinNo ratings yet
- Dinas Perhubungan, Komunikasi Dan Informatika: NO. Uraian Pekerjaan Volume Satuan Harga Satuan (RP.)Document11 pagesDinas Perhubungan, Komunikasi Dan Informatika: NO. Uraian Pekerjaan Volume Satuan Harga Satuan (RP.)Rah Panji DamarsidhiNo ratings yet
- Materi Kuliah Crash ProgramDocument14 pagesMateri Kuliah Crash ProgramImam Syafi'iNo ratings yet
- A4 - REV Simple Design & MagnelDocument35 pagesA4 - REV Simple Design & MagnelVicky Faras Barunson PanggabeanNo ratings yet
- 2016 Catalogue of Lighting Products and SolutionsDocument110 pages2016 Catalogue of Lighting Products and SolutionsDani HambalinaNo ratings yet
- Soal Tes TOEFL Dan Pembahasan Jawaban Structure (Model Test 2) - Pusat TOEFL 2Document1 pageSoal Tes TOEFL Dan Pembahasan Jawaban Structure (Model Test 2) - Pusat TOEFL 2Gustavo Aulawy121No ratings yet
- Compro TrirekonDocument14 pagesCompro Trirekonhadipurnomoputra100% (1)
- Contoh CV ProgrammerDocument1 pageContoh CV ProgrammerFaris Al FaruqNo ratings yet
- Analisa Sumur BorDocument5 pagesAnalisa Sumur BortambunanNo ratings yet
- Rencana Pembangunan Bendungan Cibeet Kabupaten Bogor: NorthDocument1 pageRencana Pembangunan Bendungan Cibeet Kabupaten Bogor: NorthEdi AriyantoNo ratings yet
- CamScanner Scans PDFs from PhotosDocument5 pagesCamScanner Scans PDFs from PhotosIdham DaniarsyahNo ratings yet
- Slide Pemaparan - Pembangunan Tower TelekomunkasiDocument26 pagesSlide Pemaparan - Pembangunan Tower TelekomunkasiRully Firmansyah100% (1)
- BQ Perencanaan GedungDocument6 pagesBQ Perencanaan GedungnurchozinazaNo ratings yet
- Taufik Hidayat, S.T.: Curriculum VitaeDocument3 pagesTaufik Hidayat, S.T.: Curriculum VitaeRCAriestaNo ratings yet
- Module 8 Benefit Cost RatioDocument13 pagesModule 8 Benefit Cost RatioRhonita Dea AndariniNo ratings yet
- 3.1-Study On Temperature For Modeling of PV Array Using TEST DATA PDFDocument4 pages3.1-Study On Temperature For Modeling of PV Array Using TEST DATA PDFRUBIONo ratings yet
- Industrial building design calculationsDocument79 pagesIndustrial building design calculationsMayNo ratings yet
- 15200-Article Text-48581-2-10-20210505Document8 pages15200-Article Text-48581-2-10-20210505NadyaNo ratings yet
- Nays2D Solver Manual: iRIC SoftwareDocument53 pagesNays2D Solver Manual: iRIC SoftwarePiere Christofer Salas HerreraNo ratings yet
- Cover DPTDocument16 pagesCover DPTArfan MufadaNo ratings yet
- 16.163.173.eka MinartiDocument11 pages16.163.173.eka MinartiLinda AisyahNo ratings yet
- Detail Kuda Kuda Kayu Autocad DWGDocument1 pageDetail Kuda Kuda Kayu Autocad DWGAlhufi SusenoNo ratings yet
- LAMPIRAN BERITA ACARA TAMBAH KURANG KEGIATAN PENINGKATAN DISTRIBUSI PENYEDIAAN AIR BAKUDocument10 pagesLAMPIRAN BERITA ACARA TAMBAH KURANG KEGIATAN PENINGKATAN DISTRIBUSI PENYEDIAAN AIR BAKUAdi ArchNo ratings yet
- CIV-PY-002 - Occupational Health & Safety Policy Rev 1Document1 pageCIV-PY-002 - Occupational Health & Safety Policy Rev 1Gabriel CeluqueNo ratings yet
- WINRIP - DOC - MPR - CTC MPR No.48 2016 12 - 2016 12 30 - 00442 PDFDocument173 pagesWINRIP - DOC - MPR - CTC MPR No.48 2016 12 - 2016 12 30 - 00442 PDFazizNo ratings yet
- ThesisDocument19 pagesThesisSofyan SuriNo ratings yet
- CT Contrast Injection and ProtocolsDocument35 pagesCT Contrast Injection and ProtocolskeziasNo ratings yet
- Radiological Anatomy of AbdomenDocument38 pagesRadiological Anatomy of AbdomenMr. Hrisab DebNo ratings yet
- Clinical Aspects of Abdominal Dynamic CTDocument42 pagesClinical Aspects of Abdominal Dynamic CTfauziNo ratings yet
- Abdomen & Pelvis CT ImagingDocument34 pagesAbdomen & Pelvis CT Imagingfalhazmi0069No ratings yet
- CT LiverDocument12 pagesCT LiverWaiz ChNo ratings yet
- Triphasic CT ScanDocument44 pagesTriphasic CT ScanPari Pengda BaliNo ratings yet
- 02 - Gastroenterology Intermediate NEDocument35 pages02 - Gastroenterology Intermediate NEArvind PrabhakarNo ratings yet
- Robin SmithuisDocument17 pagesRobin SmithuisVENDINo ratings yet
- Information About Intravenous and Oral Contrast Used in CTDocument3 pagesInformation About Intravenous and Oral Contrast Used in CTVENDINo ratings yet
- UM Mantematic K20S v01 enDocument29 pagesUM Mantematic K20S v01 enVENDINo ratings yet
- Instruction Manual STR 155 RL-1Document24 pagesInstruction Manual STR 155 RL-1VENDI100% (3)
- Stainless Steel Gas Griddle: Free StandingDocument1 pageStainless Steel Gas Griddle: Free StandingVENDINo ratings yet
- TL-330 Micro Computor Thermostat For Freezer (User Instructions)Document3 pagesTL-330 Micro Computor Thermostat For Freezer (User Instructions)VENDINo ratings yet
- TL-330 Micro Computor Thermostat For Freezer (User Instructions)Document3 pagesTL-330 Micro Computor Thermostat For Freezer (User Instructions)VENDINo ratings yet
- PositioningDocument97 pagesPositioningzixdiddy100% (1)
- Venous Thromboembolic DiseaseDocument262 pagesVenous Thromboembolic DiseasesamNo ratings yet
- Pulmonary EmbolismDocument27 pagesPulmonary EmbolismEfren Ezekiel AlbiosNo ratings yet
- Thrombosis and EmbolismDocument39 pagesThrombosis and Embolismilva100% (1)
- Obstetrics V13 Obstetric Emergencies Chapter Pulmonary Embolism During Pregnancy 1632545155Document8 pagesObstetrics V13 Obstetric Emergencies Chapter Pulmonary Embolism During Pregnancy 1632545155Miriam Sanchez RamosNo ratings yet
- Manage and Diagnose Acute and Chronic Cor PulmonaleDocument42 pagesManage and Diagnose Acute and Chronic Cor PulmonaleNym Angga SantosaNo ratings yet
- PLE 2019 - Medicine Questions and Answer KeyDocument24 pagesPLE 2019 - Medicine Questions and Answer KeydicksonNo ratings yet
- Understanding Likelihood Ratios and Applying V/Q Scan Results to Diagnose Pulmonary EmbolismDocument46 pagesUnderstanding Likelihood Ratios and Applying V/Q Scan Results to Diagnose Pulmonary EmbolismwibowomustokoNo ratings yet
- 4 5997052321324860969 PDFDocument384 pages4 5997052321324860969 PDFMedicine Agency100% (1)
- CT For PE Breathing Technique PRESENTATIONDocument17 pagesCT For PE Breathing Technique PRESENTATIONEka JuliantaraNo ratings yet
- Maternity - Postnatal Care in The First Week - CG - 2015Document41 pagesMaternity - Postnatal Care in The First Week - CG - 2015Monica SurduNo ratings yet
- CT of The HeartDocument12 pagesCT of The HeartGil PerezNo ratings yet
- DX Imaging 1 MT and FinalDocument24 pagesDX Imaging 1 MT and FinalRaymondNo ratings yet
- Puerperal Venous Thrombosis and Pulmonary EmbolismDocument14 pagesPuerperal Venous Thrombosis and Pulmonary EmbolismSamhitha Ayurvedic ChennaiNo ratings yet
- Professional Strategies for Nursing ReviewDocument14 pagesProfessional Strategies for Nursing ReviewAJ DalawampuNo ratings yet
- NCM 118 - Lesson 3 (Pulmonary Embolism)Document4 pagesNCM 118 - Lesson 3 (Pulmonary Embolism)Bobby Christian DuronNo ratings yet
- EKGin PEDocument2 pagesEKGin PEพงศธร ปัตถาNo ratings yet
- Travel DVT Risk & PreventionDocument3 pagesTravel DVT Risk & PreventionandreaNo ratings yet
- The PERT Concept Q1 A Step-By-Step Approach To Managing Pulmonary EmbolismDocument9 pagesThe PERT Concept Q1 A Step-By-Step Approach To Managing Pulmonary EmbolismntnquynhproNo ratings yet
- Case Report ASMIHA 2022Document1 pageCase Report ASMIHA 2022Ghina NinditasariNo ratings yet
- Ultrasonido en El Paciente Crítico Daniel Lichtenstein PDFDocument33 pagesUltrasonido en El Paciente Crítico Daniel Lichtenstein PDFVallejo Romo Alberto CristianNo ratings yet
- Anki QuesetionsDocument220 pagesAnki QuesetionsMatthew SoNo ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisitdocNo ratings yet
- UPDATE MENEJEMEN DVTDocument9 pagesUPDATE MENEJEMEN DVTSupandy HasanNo ratings yet
- Algorithm 1. Use of PE Criteria Based On Patient Location at Time of EventDocument5 pagesAlgorithm 1. Use of PE Criteria Based On Patient Location at Time of EventKatherynSotoNo ratings yet
- Nursing Care Plan: Pulmonary EbolismDocument5 pagesNursing Care Plan: Pulmonary EbolismneuronurseNo ratings yet
- Venous Thromboembolism Prophylaxis in Orthopedic SurgeryDocument30 pagesVenous Thromboembolism Prophylaxis in Orthopedic SurgerymohNo ratings yet
- D Di2Document5 pagesD Di2ARIF AHAMMED P100% (1)
- StreptokinaseDocument4 pagesStreptokinaseAfiqah So Jasmi100% (1)
- Disturbances in OxygenationDocument10 pagesDisturbances in OxygenationjenrylNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)