You might also like
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationFrom EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationNo ratings yet
- Neurosurgery in PregnancyDocument12 pagesNeurosurgery in PregnancyhkdawnwongNo ratings yet
- Optimal Management of Hypotension During Cesarean Delivery Under Spinal AnesthesiaDocument22 pagesOptimal Management of Hypotension During Cesarean Delivery Under Spinal AnesthesiaJosé Alberto LozanoNo ratings yet
- Postdural Puncture Headache: Kyung-Hwa KwakDocument8 pagesPostdural Puncture Headache: Kyung-Hwa KwakRakha FahrezaNo ratings yet
- Current Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsDocument6 pagesCurrent Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsManju KumariNo ratings yet
- Uterine and Fetal Placental Doppler Indices Are Associated With Maternal Cardiovascular FunctionDocument8 pagesUterine and Fetal Placental Doppler Indices Are Associated With Maternal Cardiovascular FunctionMuhammad Pebri Nilhakim ZavbmNo ratings yet
- C - RCT Jurding FixDocument7 pagesC - RCT Jurding FixDr. MuslimNo ratings yet
- Pregnancy and Glomerular Disease: A Systematic Review of The Literature With Management GuidelinesDocument11 pagesPregnancy and Glomerular Disease: A Systematic Review of The Literature With Management GuidelinesmeliabudiNo ratings yet
- HBPM+aspirina prevencion de preeclampsiaDocument14 pagesHBPM+aspirina prevencion de preeclampsiaGaudy Francheska Alvarado GutierrezNo ratings yet
- Atent Ductus Arteriosus in Preterm InfantsDocument8 pagesAtent Ductus Arteriosus in Preterm InfantsLissaberti AmaliahNo ratings yet
- Predicting Spinal Hypotension During Caesarean Section: South Afr J Anaesth AnalgDocument4 pagesPredicting Spinal Hypotension During Caesarean Section: South Afr J Anaesth AnalgPalwasha MalikNo ratings yet
- Guideline HipertensiDocument7 pagesGuideline HipertensiAgus RiyantoNo ratings yet
- Piis0007091217315908 PDFDocument13 pagesPiis0007091217315908 PDFJothy DeepakNo ratings yet
- MJMU Volume 50 Issue 4 Pages 155-163-1Document9 pagesMJMU Volume 50 Issue 4 Pages 155-163-1Fred OkelloNo ratings yet
- 1 s2.0 S2666668521001324 MainDocument5 pages1 s2.0 S2666668521001324 Mainmchojnacki81No ratings yet
- Cenkowski 2019Document7 pagesCenkowski 2019Rafael BagusNo ratings yet
- Ductus ArteriosoDocument17 pagesDuctus ArteriosoJohn Romero CevallosNo ratings yet
- Jurnal Berpikir KritisDocument9 pagesJurnal Berpikir KritisNindita IllahiNo ratings yet
- Review Ductus ArteriousDocument8 pagesReview Ductus ArteriousWiwit ClimberNo ratings yet
- Preeclampsia management obstetric anaesthesiaDocument21 pagesPreeclampsia management obstetric anaesthesiaIndra WijayaNo ratings yet
- Preventing and Treating Hypotension During Spinal Anaesthesia For Caesarean SectionDocument2 pagesPreventing and Treating Hypotension During Spinal Anaesthesia For Caesarean Sectionvictor rodriguezNo ratings yet
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyDocument6 pagesStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganNo ratings yet
- A Study On The Prevalence of Fundus Changes in Pregnancy Induced Hypertension Among Antenatal Care Patients Attending Gmers Hospital, ValsadDocument10 pagesA Study On The Prevalence of Fundus Changes in Pregnancy Induced Hypertension Among Antenatal Care Patients Attending Gmers Hospital, ValsadIJAR JOURNALNo ratings yet
- Obesidad en El Paciente CriticoDocument11 pagesObesidad en El Paciente CriticocastillojessNo ratings yet
- SJMPS 69 616-621 C x9IOCOHDocument6 pagesSJMPS 69 616-621 C x9IOCOHRezky amalia basirNo ratings yet
- Managing Hypotension Induced by Spinal Anesthesia For Caesarean SectionDocument6 pagesManaging Hypotension Induced by Spinal Anesthesia For Caesarean SectionPalwasha MalikNo ratings yet
- Aderoba 2016Document8 pagesAderoba 2016DONNYNo ratings yet
- AMJ_Volume 45_Issue 4_Pages 833-846Document13 pagesAMJ_Volume 45_Issue 4_Pages 833-846atikaNo ratings yet
- clampeamento tardio cordão 2021 benefícios e sem efeito fototerapiaDocument7 pagesclampeamento tardio cordão 2021 benefícios e sem efeito fototerapiaenfasconteudoproNo ratings yet
- Manejo de La Sepsis 2Document5 pagesManejo de La Sepsis 2Rachmi Pratiwi Febrita PartiNo ratings yet
- 2017 Manejo Perioperatorio de La Hiperglicemia INGLÉSDocument14 pages2017 Manejo Perioperatorio de La Hiperglicemia INGLÉSKarla Ivonne Hernandez AguilarNo ratings yet
- Hellp Syndrome PDFDocument11 pagesHellp Syndrome PDFLisya AnggraeniNo ratings yet
- Pengaruh Anestesi Regional Dan General Pada Sectio Cesaria Pada Ibu Dengan Pre Eklampsia Berat Terhadap Apgar ScoreDocument12 pagesPengaruh Anestesi Regional Dan General Pada Sectio Cesaria Pada Ibu Dengan Pre Eklampsia Berat Terhadap Apgar ScoreMuhamad Ongky NRahardiNo ratings yet
- Joacp 32 153Document7 pagesJoacp 32 153thresh mainNo ratings yet
- Hypertensive Disorders of Pregnancy and Longterm Risk of Maternal StrokeDocument21 pagesHypertensive Disorders of Pregnancy and Longterm Risk of Maternal StrokenskhldNo ratings yet
- Abarientos Con 2a Assignment 3 PDFDocument3 pagesAbarientos Con 2a Assignment 3 PDFjennielunay00No ratings yet
- PIIS2210778916303701Document2 pagesPIIS2210778916303701Fatimah AssagafNo ratings yet
- Bahan Bacaan PreeklampsiaDocument11 pagesBahan Bacaan PreeklampsiaMegan LewisNo ratings yet
- WOS - Neurodevelopmental outcomes of premature infants born at ≤ 32 weeks of gestational age with post-hemorrhagic hydrocephalus treated with ventriculoperitoneal shuntDocument11 pagesWOS - Neurodevelopmental outcomes of premature infants born at ≤ 32 weeks of gestational age with post-hemorrhagic hydrocephalus treated with ventriculoperitoneal shuntanto.fernandez0107No ratings yet
- Hiperlazie Adrenala CongenitalaDocument11 pagesHiperlazie Adrenala CongenitalaClaudia IrimieNo ratings yet
- Spinal Anesthesia-Inducided HypotensionDocument3 pagesSpinal Anesthesia-Inducided HypotensionManolin KinNo ratings yet
- Tran 2020Document8 pagesTran 2020whyme becauseNo ratings yet
- Jurnal Berpikir KritisDocument9 pagesJurnal Berpikir KritisNindita IllahiNo ratings yet
- PDA An Overview 2007Document9 pagesPDA An Overview 2007HelenaFalconeNo ratings yet
- Pregnant Patient With Eclampsia For Emergency Cesarean Section Case FileDocument2 pagesPregnant Patient With Eclampsia For Emergency Cesarean Section Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Management of Neonatal Hypotension and ShockDocument7 pagesManagement of Neonatal Hypotension and ShockntnquynhproNo ratings yet
- Management of Neonatal Hypotension and ShockDocument7 pagesManagement of Neonatal Hypotension and ShockntnquynhproNo ratings yet
- Anestesia Embarazo y Mujer EmbarazadaDocument19 pagesAnestesia Embarazo y Mujer Embarazadanata0916No ratings yet
- 17 Analysis of Maternal Outcome of General Versus Spinal Anaesthesia For Caesarean Delivery in Severe Pre EclampsiaDocument7 pages17 Analysis of Maternal Outcome of General Versus Spinal Anaesthesia For Caesarean Delivery in Severe Pre EclampsiaUlfa PuspitaNo ratings yet
- Cerebral Perfusion Pressure and Autoregulation inDocument9 pagesCerebral Perfusion Pressure and Autoregulation inayu permata dewiNo ratings yet
- Estado Hemodinamico La Primera Semana de Vida en VLBWDocument7 pagesEstado Hemodinamico La Primera Semana de Vida en VLBWMaluNo ratings yet
- 2019 Jurnal 2Document9 pages2019 Jurnal 2noviyantieliskaNo ratings yet
- Safety of Umbilical Cord Milking in Very Preterm Neonates: A Randomized Controlled StudyDocument8 pagesSafety of Umbilical Cord Milking in Very Preterm Neonates: A Randomized Controlled StudyFatma ElzaytNo ratings yet
- The Ductus Arteriosus A Refined ApproachDocument9 pagesThe Ductus Arteriosus A Refined ApproachHelenaFalconeNo ratings yet
- Jurnal AdeDocument5 pagesJurnal AdeSuryanti SultanNo ratings yet
- Neurological Outcome and Frequency of Overdrainage in Normal Pressure Hydrocephalus Directly Correlates With Implanted Ventriculo Peritoneal ShuntDocument6 pagesNeurological Outcome and Frequency of Overdrainage in Normal Pressure Hydrocephalus Directly Correlates With Implanted Ventriculo Peritoneal ShuntcNo ratings yet
- Prerenalacutekidneyinjury 2020Document9 pagesPrerenalacutekidneyinjury 2020diana ramirezNo ratings yet
- Is Massive Proteinuria Associated With Maternal An PDFDocument6 pagesIs Massive Proteinuria Associated With Maternal An PDFAmpry LoyraNo ratings yet
- Coagulation Management and Transfusion in Massive Postpartum HemorrhageDocument7 pagesCoagulation Management and Transfusion in Massive Postpartum HemorrhageAlberto LiraNo ratings yet
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaDocument5 pagesProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangNo ratings yet
- Parthasarathy2013 PDFDocument7 pagesParthasarathy2013 PDFAndi BintangNo ratings yet
- Anestesia General para Césarea PDFDocument7 pagesAnestesia General para Césarea PDFAgnese ValentiniNo ratings yet
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TDocument3 pagesMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangNo ratings yet
- Anestesia General para Césarea PDFDocument7 pagesAnestesia General para Césarea PDFAgnese ValentiniNo ratings yet
- Depresión e InmunidadDocument13 pagesDepresión e InmunidadgabisaenaNo ratings yet
- Cultural Sociology of Mental Illness n28Document5 pagesCultural Sociology of Mental Illness n28Andi BintangNo ratings yet
- Bar A Zanchi 2018Document17 pagesBar A Zanchi 2018Andi BintangNo ratings yet
- Overweight linked to increased risk of lower back painDocument8 pagesOverweight linked to increased risk of lower back painAndi BintangNo ratings yet
- 2013 Student Membership ApplicationDocument1 page2013 Student Membership ApplicationAndi BintangNo ratings yet
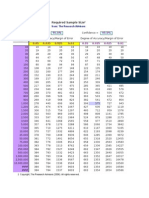
- Required Sample Size: From: The Research AdvisorsDocument3 pagesRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Instruction For Author ClimactericDocument9 pagesInstruction For Author ClimactericAndi BintangNo ratings yet
- 1 s2.0 S1052305714000561 MainDocument6 pages1 s2.0 S1052305714000561 MainAndi BintangNo ratings yet
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityDocument5 pagesSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangNo ratings yet
- 1 s2.0 S0002937803001388 MainDocument3 pages1 s2.0 S0002937803001388 MainAndi BintangNo ratings yet
- 1 s2.0 S0002937803001388 MainDocument3 pages1 s2.0 S0002937803001388 MainAndi BintangNo ratings yet
- 1 s2.0 S0002937800704534 Main PDFDocument1 page1 s2.0 S0002937800704534 Main PDFAndi BintangNo ratings yet
- Serviks DocjhjuDocument366 pagesServiks DocjhjuAndi BintangNo ratings yet
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesDocument10 pagesAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangNo ratings yet
- 1 s2.0 S0021755713002003 MainDocument6 pages1 s2.0 S0021755713002003 MainAndi BintangNo ratings yet
- Hepatitis C APASLfghDocument27 pagesHepatitis C APASLfghAndi BintangNo ratings yet
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDocument6 pagesPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangNo ratings yet
- Urologi PDFDocument237 pagesUrologi PDFAndi BintangNo ratings yet
- 1 s2.0 S0021755713002003 MainDocument6 pages1 s2.0 S0021755713002003 MainAndi BintangNo ratings yet
- MK Giz Slide Infant Feeding PracticeDocument1 pageMK Giz Slide Infant Feeding PracticeAndi BintangNo ratings yet
- Anthropometry: Ergonomics Additional ResourcesDocument5 pagesAnthropometry: Ergonomics Additional ResourcesAndi BintangNo ratings yet
- PCT CAP ABiuytoDocument10 pagesPCT CAP ABiuytoAndi BintangNo ratings yet
- ATS Guidelines CAP ManagementDocument25 pagesATS Guidelines CAP ManagementMae Matira AbeladorNo ratings yet
- Cap Bts 2009 ComplitdgDocument139 pagesCap Bts 2009 ComplitdgAndi BintangNo ratings yet
- Management by Objective Approach in Nursing Performance Appraisal and Its Impact On Quality of Nursing CareDocument13 pagesManagement by Objective Approach in Nursing Performance Appraisal and Its Impact On Quality of Nursing CareGummie Akalal SugalaNo ratings yet
- Nursing Process, Fluids, Acid Base, IV CalcDocument24 pagesNursing Process, Fluids, Acid Base, IV CalcStephanieNo ratings yet
- BUPA - Staff PresentationDocument20 pagesBUPA - Staff PresentationMaurizio RosaNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyMariana González DíazNo ratings yet
- Isabela State University Nursing Final Exam ReviewDocument8 pagesIsabela State University Nursing Final Exam ReviewSteve EstebanNo ratings yet
- Grade 10 Health Career PlanningDocument12 pagesGrade 10 Health Career PlanningJenz Rey Justo50% (2)
- Module 5-Safety and Health at Work - MANUALDocument46 pagesModule 5-Safety and Health at Work - MANUALYhan Brotamonte BoneoNo ratings yet
- RehumaticDocument3 pagesRehumaticgopscharanNo ratings yet
- Electronic Medical RecordsDocument25 pagesElectronic Medical Recordslrrcenter100% (2)
- Nutrition Assessment of Mr. GrandDocument16 pagesNutrition Assessment of Mr. GrandSyahrulbariah AbdulhamidNo ratings yet
- DRUG ADDICTION: CAUSES AND EFFECTSDocument17 pagesDRUG ADDICTION: CAUSES AND EFFECTSgaurav nehraNo ratings yet
- Nasogastric Tube FeedingDocument2 pagesNasogastric Tube FeedingApple BelicanNo ratings yet
- Bahasa Inggris KeperawatanDocument7 pagesBahasa Inggris KeperawatanGeldine Raudina25No ratings yet
- Diveintopython3 r802Document25 pagesDiveintopython3 r802Ashwin VargheseNo ratings yet
- Intensive & Critical Care NursingDocument8 pagesIntensive & Critical Care Nursingdevi ana ariesta bellaNo ratings yet
- His 5Document167 pagesHis 5Anjum100% (5)
- Pelaez - Et - Al - 2014 - NandU - Pelvic Floor Muscle Training Included in A Pregnancy Exercise Program Is Effective in Primary Prevention of Urinary IncontinenceDocument5 pagesPelaez - Et - Al - 2014 - NandU - Pelvic Floor Muscle Training Included in A Pregnancy Exercise Program Is Effective in Primary Prevention of Urinary IncontinenceShannon DolanNo ratings yet
- Congenital Vertical TalusDocument24 pagesCongenital Vertical TalusKaizar EnnisNo ratings yet
- Assessment of The Neurological Patient Case Study: QuestionsDocument1 pageAssessment of The Neurological Patient Case Study: QuestionstildateoNo ratings yet
- Clinical Trial Protocol Iranian Registry of Clinical TrialsDocument10 pagesClinical Trial Protocol Iranian Registry of Clinical TrialsAnupNo ratings yet
- Gestational Diabetes Mellitus: Case PresentationDocument46 pagesGestational Diabetes Mellitus: Case PresentationATEHAN BORDSNo ratings yet
- Close Reading BittenDocument5 pagesClose Reading Bittenapi-405140390No ratings yet
- Pyoderma Gangrenosum A Review of Orthopedic Case ReportsDocument4 pagesPyoderma Gangrenosum A Review of Orthopedic Case ReportsIga Nurwani RidwanNo ratings yet
- Online CLOLAR Clofarabine Purchase With DiscountDocument4 pagesOnline CLOLAR Clofarabine Purchase With Discountcena heyNo ratings yet
- Infectious Diseases Lecture on Fever PathophysiologyDocument2 pagesInfectious Diseases Lecture on Fever PathophysiologyNonoy JoyaNo ratings yet
- Med Surg 2 MIDTERM REVIEWDocument6 pagesMed Surg 2 MIDTERM REVIEWHannah PerkinsNo ratings yet
- Smoking in Public Places Should Be BannedDocument2 pagesSmoking in Public Places Should Be BannedMark Landolf GoNo ratings yet
- Abdo History TakingDocument4 pagesAbdo History TakingJamie Rina KeeNo ratings yet
- Doctor, S DetailsDocument3 pagesDoctor, S DetailsSteven BryantNo ratings yet
- Andreas: Focused Assessment With Sonography in TraumaDocument13 pagesAndreas: Focused Assessment With Sonography in Traumarina paramitaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)