You might also like
- Art-Previene El Ejercicio Regular Incluido MSP La Iu e Ia en El EmbarazoDocument11 pagesArt-Previene El Ejercicio Regular Incluido MSP La Iu e Ia en El EmbarazoPaula RangelNo ratings yet
- A Comparison of Two PFMT Programs in Females With Stress Urinary IncontineneceDocument11 pagesA Comparison of Two PFMT Programs in Females With Stress Urinary Incontinenecemenna lNo ratings yet
- Futbol y Vo2Document5 pagesFutbol y Vo2Sandra R A MedinaNo ratings yet
- Phys TherDocument16 pagesPhys TherNovie AstiniNo ratings yet
- Pelvic Floor Muscle Training Protocol For Stress Urinary Incontinence in Women: A Systematic ReviewDocument9 pagesPelvic Floor Muscle Training Protocol For Stress Urinary Incontinence in Women: A Systematic ReviewKarem FernandezNo ratings yet
- Jurnal Propriosepsi GeriatriDocument9 pagesJurnal Propriosepsi GeriatriIra AdventiaNo ratings yet
- Hypo PF functionDocument17 pagesHypo PF functionIvan Garcia OsorioNo ratings yet
- Jpts 25 1087 PDFDocument5 pagesJpts 25 1087 PDFArry FirmansyahNo ratings yet
- Kegel Exercise PDFDocument5 pagesKegel Exercise PDFDisaKNNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchariniNo ratings yet
- Effect of A Physiotherapy Program in Women With Primary DysmenorrheaDocument6 pagesEffect of A Physiotherapy Program in Women With Primary DysmenorrheaPaula RangelNo ratings yet
- Bibliography (Critical Care Nursing)Document2 pagesBibliography (Critical Care Nursing)bijoiiNo ratings yet
- Does Regular Exercise in Pregnancy Influence Duration of Labor? A Secondary Analysis of A Randomized Controlled TrialDocument7 pagesDoes Regular Exercise in Pregnancy Influence Duration of Labor? A Secondary Analysis of A Randomized Controlled Trialana pintoNo ratings yet
- Impact of Applying Different Physical Activity GuidelinesDocument9 pagesImpact of Applying Different Physical Activity GuidelinesnirchennNo ratings yet
- Ansai Et Al. (2016) PDFDocument8 pagesAnsai Et Al. (2016) PDFvabrandaoNo ratings yet
- Experiences of Exercise During pregnancyDocument9 pagesExperiences of Exercise During pregnancyNuno RobertoNo ratings yet
- Postnatal Exercises Improve Quality of LifeDocument4 pagesPostnatal Exercises Improve Quality of LiferohiniNo ratings yet
- Women's Health Reports Knowledge and Practice of Pelvic Floor ExercisesDocument7 pagesWomen's Health Reports Knowledge and Practice of Pelvic Floor ExercisesQORI KARUNIA WANTINo ratings yet
- Inter Fan ZhangDocument9 pagesInter Fan ZhangrizkaNo ratings yet
- Complementary Therapies in Clinical Practice: Semiha Ayd In Özkan, Gülay Rath FischDocument6 pagesComplementary Therapies in Clinical Practice: Semiha Ayd In Özkan, Gülay Rath FischAlek OkeNo ratings yet
- Muscle Strength Training Program in Nonagenarians - A Randomized Controlled TrialDocument6 pagesMuscle Strength Training Program in Nonagenarians - A Randomized Controlled TrialGabriel ArcenioNo ratings yet
- Metode de Reeducare PosturalaDocument4 pagesMetode de Reeducare PosturalaMaria RamonaNo ratings yet
- Effect of A Postpartum Training Program On Prevale PDFDocument9 pagesEffect of A Postpartum Training Program On Prevale PDFHardik SinghNo ratings yet
- 2002 PDFDocument6 pages2002 PDFIMaa Wati AlbiizzahNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument6 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive Biologyana pintoNo ratings yet
- Perineal Massage and Training Reduce TraumaDocument7 pagesPerineal Massage and Training Reduce TraumaGum GulNo ratings yet
- Oliveira 2007Document8 pagesOliveira 2007Carlos VieiraNo ratings yet
- Effects of Prenatal Perineal Massage and Kegel Exercise On The Episiotomy RateDocument10 pagesEffects of Prenatal Perineal Massage and Kegel Exercise On The Episiotomy RateIOSRjournalNo ratings yet
- Pelvic Floor Rehabilitation in The Treatment of Women With Dyspareunia: A Randomized Controlled Clinical TrialDocument7 pagesPelvic Floor Rehabilitation in The Treatment of Women With Dyspareunia: A Randomized Controlled Clinical TrialFERNANDA SILVEIRANo ratings yet
- Kidney Paper 2018Document5 pagesKidney Paper 2018samah hossnyNo ratings yet
- Does Exercise Training During Pregnancy Affect Gestational Age? A Randomised Controlled TrialDocument6 pagesDoes Exercise Training During Pregnancy Affect Gestational Age? A Randomised Controlled TrialTrnidad Moder GarvizoNo ratings yet
- Jurnal Obgyn GueDocument4 pagesJurnal Obgyn Gueamel_ariefNo ratings yet
- Regular Exercise During Pregnancy To Prevent Gestational DiabetesDocument8 pagesRegular Exercise During Pregnancy To Prevent Gestational DiabetesEgie Nugraha Fitriyan ApriyadiNo ratings yet
- Oral Presentation David Oktavianus Tambunan TerbaruDocument34 pagesOral Presentation David Oktavianus Tambunan TerbaruMunifah YusriyahNo ratings yet
- Jurnal Post PartumDocument11 pagesJurnal Post PartumjayaNo ratings yet
- Role of Kegel's Exercise On Postpartum Perineal Fitness Randomised Control TrialDocument6 pagesRole of Kegel's Exercise On Postpartum Perineal Fitness Randomised Control TrialCatalina DincaNo ratings yet
- Effects of Leg Strength Exercise On Muscle Strength, Flexibility and Symptoms of Urinary Incontinence of Elderly WomenDocument9 pagesEffects of Leg Strength Exercise On Muscle Strength, Flexibility and Symptoms of Urinary Incontinence of Elderly Womenkang soon cheolNo ratings yet
- Vikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundDocument8 pagesVikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundSekar AyuNo ratings yet
- Efects of Inspiratory Muscle Training in Older AdultsDocument10 pagesEfects of Inspiratory Muscle Training in Older AdultsMaría Camila Zuluaga AriasNo ratings yet
- Physical Activity During Pregnancy and Its Influence On Delivery Time: A Randomized Clinical TrialDocument14 pagesPhysical Activity During Pregnancy and Its Influence On Delivery Time: A Randomized Clinical TrialZaray EspinosaNo ratings yet
- Environmental Research and Public Health: International Journal ofDocument10 pagesEnvironmental Research and Public Health: International Journal ofrestu pangestutiNo ratings yet
- Pilares Eficiente para El Suelo PelvicoDocument6 pagesPilares Eficiente para El Suelo PelvicoRitaNo ratings yet
- Effects of pelvic floor muscle training during pregnancyDocument8 pagesEffects of pelvic floor muscle training during pregnancyelfanizar yusandiNo ratings yet
- LP Post Partum SpontanDocument16 pagesLP Post Partum SpontanPutri PuspitaNo ratings yet
- Hipopresivos y Dolor Lumbar Cronico 2021Document9 pagesHipopresivos y Dolor Lumbar Cronico 2021klgarivasNo ratings yet
- Bo Et AlDocument6 pagesBo Et AlMaria Betania NunesNo ratings yet
- 1 Monteiro Etal 2021Document6 pages1 Monteiro Etal 2021Gabriel GursenNo ratings yet
- Papn MS Id 000156Document7 pagesPapn MS Id 000156niekoNo ratings yet
- Comparative Effect of Vision Deprived Balance Training Over Free Vision Balance Training Among Stroke SubjectsDocument8 pagesComparative Effect of Vision Deprived Balance Training Over Free Vision Balance Training Among Stroke SubjectsijphyNo ratings yet
- A Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder PatientsDocument4 pagesA Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder Patientsfi.afifah NurNo ratings yet
- Mobility Training After Hip FractureDocument7 pagesMobility Training After Hip FracturewirasenaNo ratings yet
- RCT Zumba ExerciseDocument5 pagesRCT Zumba ExerciseSukmarahayuNo ratings yet
- Pilates Reduces Postpartum FatigueDocument5 pagesPilates Reduces Postpartum FatigueHidroterapia lucenaNo ratings yet
- Mulligan Sustained Natural Apophyseal Glides Versus Thoracic Manipulation On Mechanical Neck Pain: A Randomized Controlled StudyDocument12 pagesMulligan Sustained Natural Apophyseal Glides Versus Thoracic Manipulation On Mechanical Neck Pain: A Randomized Controlled StudyAbdul Latiful KhabirNo ratings yet
- A Clinical Study of Programmed Labour and Its Maternal and Foetal OutcomeDocument4 pagesA Clinical Study of Programmed Labour and Its Maternal and Foetal OutcomeInternational Organization of Scientific Research (IOSR)No ratings yet
- Effects of Pelvic Floor Muscle Training Combined With Estriol On Pelvic Floor Dysfunction After Total Hysterectomy Applied in PerimenopauseDocument6 pagesEffects of Pelvic Floor Muscle Training Combined With Estriol On Pelvic Floor Dysfunction After Total Hysterectomy Applied in PerimenopauseChoirul AkbarNo ratings yet
- Effectiveness of StretchingDocument10 pagesEffectiveness of Stretchingاحمد العايديNo ratings yet
- Exercise in Pregnancy: Effect On Fitness and Obstetric Outcomes - A Randomized TrialDocument4 pagesExercise in Pregnancy: Effect On Fitness and Obstetric Outcomes - A Randomized TrialInes NozicaNo ratings yet
- Exercise and Sporting Activity During Pregnancy: Evidence-Based GuidelinesFrom EverandExercise and Sporting Activity During Pregnancy: Evidence-Based GuidelinesRita Santos-RochaNo ratings yet
- The Art of Healing Movement: Exploring Therapeutic Wu Shu Gymnastics.From EverandThe Art of Healing Movement: Exploring Therapeutic Wu Shu Gymnastics.No ratings yet
- Stages of Labor: Latent, Active, Transition & PlacentalDocument18 pagesStages of Labor: Latent, Active, Transition & Placentallushxene84No ratings yet
- Obstetrics and GynacologyDocument14 pagesObstetrics and GynacologykalkidanNo ratings yet
- Demographic Data: #2 RefusedDocument31 pagesDemographic Data: #2 Refusedjp102090No ratings yet
- Nfhs-5 India ReportDocument713 pagesNfhs-5 India ReportROHIT DASNo ratings yet
- MRDE 101 Full TextbookDocument512 pagesMRDE 101 Full TextbookSedekholie ChadiNo ratings yet
- 1st & 2nd Trimester Pregnancy LossDocument48 pages1st & 2nd Trimester Pregnancy LossAbdullah EssaNo ratings yet
- LS 2 M1L1L3Document7 pagesLS 2 M1L1L3Alvin Arquibel DescatamientoNo ratings yet
- TPCN 1295 FormDocument1 pageTPCN 1295 FormTeddy WilsonNo ratings yet
- PREECLAMPSIA Case ScenarioDocument2 pagesPREECLAMPSIA Case Scenariosabao kizuiteNo ratings yet
- Stages of Prenatal DevelopmentDocument36 pagesStages of Prenatal DevelopmentRuru LavariasNo ratings yet
- The Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesDocument9 pagesThe Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesimuhammadfahmiNo ratings yet
- Columbia Sexuality and Gender Law Clinic - Surrogacy Law and Policy Report - June 2016 PDFDocument90 pagesColumbia Sexuality and Gender Law Clinic - Surrogacy Law and Policy Report - June 2016 PDFShantanu AgnihotriNo ratings yet
- Mechanisms of Normal Vertex LabourDocument65 pagesMechanisms of Normal Vertex LabourBasmala We PasNo ratings yet
- Incompetent NCPDocument1 pageIncompetent NCPJohn Francis Velasco100% (6)
- NCM 107 Clinical Case in Gynecology 1Document35 pagesNCM 107 Clinical Case in Gynecology 1Kyle Randolf CuevasNo ratings yet
- Safe Abortion – A Moral ObligationDocument20 pagesSafe Abortion – A Moral ObligationJerico RelopezNo ratings yet
- Ibnu Sina Hospital, Tuesday, April 19th, 2022 (Period April 10th - 17th, 2022)Document4 pagesIbnu Sina Hospital, Tuesday, April 19th, 2022 (Period April 10th - 17th, 2022)MirahAvishaNo ratings yet
- UNIT - II - SUBCENTRE - AnandDocument34 pagesUNIT - II - SUBCENTRE - AnandAnand gowdaNo ratings yet
- Family PlanningDocument59 pagesFamily PlanningDhruva PatelNo ratings yet
- Edexcel: IgcseDocument15 pagesEdexcel: IgcseAdele FernandoNo ratings yet
- Female Reproductive System: Understanding Puberty and Hormonal ChangesDocument33 pagesFemale Reproductive System: Understanding Puberty and Hormonal ChangesHoneychrise ConcepcionNo ratings yet
- Glanville Williams Legal and Illegal AbortionDocument14 pagesGlanville Williams Legal and Illegal AbortionoduronyarkolawreneNo ratings yet
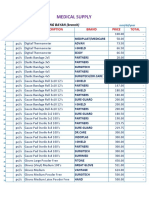
- Medical Supply and Baby Product ListingDocument5 pagesMedical Supply and Baby Product ListingParmasya Ng Bayan Bacolor Main BranchNo ratings yet
- Fundal Height MeasurementDocument2 pagesFundal Height MeasurementCuttie Anne GalangNo ratings yet
- Everything You Need to Know About the Menstrual CycleDocument16 pagesEverything You Need to Know About the Menstrual CycleCoxnxkNo ratings yet
- Obstetric History TakingDocument5 pagesObstetric History TakingAshish Mishra [33]No ratings yet
- Intrapartum Category I, II, and III Fetal Heart Rate Tracings - Management - UpToDateDocument18 pagesIntrapartum Category I, II, and III Fetal Heart Rate Tracings - Management - UpToDateMadeline lunaNo ratings yet
- Chapter 3 Human ReproductionDocument7 pagesChapter 3 Human Reproductionsara DaphneNo ratings yet
- Chapter#3 Developmental PsychologyDocument32 pagesChapter#3 Developmental Psychologyfatima bilalNo ratings yet
- Surrogacy Laws in India and in Other Foreign Countries - PowerpointDocument36 pagesSurrogacy Laws in India and in Other Foreign Countries - PowerpointSAYANTAN ROYNo ratings yet