You might also like
- DSM-IV Adult ADHD Symptom Checklist-Self Report Version # 6182Document1 pageDSM-IV Adult ADHD Symptom Checklist-Self Report Version # 6182Chris0% (1)
- Drug Desinging 4.1 Drug OptimizationDocument8 pagesDrug Desinging 4.1 Drug OptimizationVijay IyerNo ratings yet
- 2017 (G.R. No. 204262, Madridejos v. NYK-Fil Ship Management) PDFDocument19 pages2017 (G.R. No. 204262, Madridejos v. NYK-Fil Ship Management) PDFFrance SanchezNo ratings yet
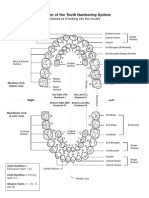
- Diagram of The Tooth Numbering SystemDocument1 pageDiagram of The Tooth Numbering Systemsaleh900No ratings yet
- 2019 - Zhi-Yong Wang - Effect - of - An - Indwelling - Nasogastric - Tube - On - SwalloDocument8 pages2019 - Zhi-Yong Wang - Effect - of - An - Indwelling - Nasogastric - Tube - On - Swallomackay00917No ratings yet
- 5 NGTDocument9 pages5 NGTPipit PitalokaNo ratings yet
- The Use of Inhaled NaceDocument7 pagesThe Use of Inhaled NaceYondi Piter PapulungNo ratings yet
- Clinical Nutrition: Original ArticleDocument7 pagesClinical Nutrition: Original ArticleBby AdelinaNo ratings yet
- Aex 091Document9 pagesAex 091enriquegarciagalianaNo ratings yet
- Factors Affecting The Prevalence of Gastro-Oesophageal Reflux in Childhood Corrosive Oesophageal StricturesDocument6 pagesFactors Affecting The Prevalence of Gastro-Oesophageal Reflux in Childhood Corrosive Oesophageal StricturesAlinaRellyyNo ratings yet
- Axelsson 2017Document8 pagesAxelsson 2017Yondi Piter PapulungNo ratings yet
- Nerjm SesionDocument12 pagesNerjm SesionjorgeNo ratings yet
- Inhibidor Bomba de Protones e Infecci - NDocument10 pagesInhibidor Bomba de Protones e Infecci - NSMIBA Medicina100% (1)
- Artículo 2Document10 pagesArtículo 2edunapedNo ratings yet
- Septic ShockDocument12 pagesSeptic ShockPatrick CommettantNo ratings yet
- Ramirez 2013Document10 pagesRamirez 2013Nadia Farah FadhilaNo ratings yet
- Effects of Tracheostomy Tube On SwallowingDocument21 pagesEffects of Tracheostomy Tube On SwallowingPaola A. MartinezNo ratings yet
- Conservative Treatment of Early Postoperative Small Bowel Obstruction With Obliterative PeritonitisDocument10 pagesConservative Treatment of Early Postoperative Small Bowel Obstruction With Obliterative Peritonitisalemago90No ratings yet
- Is Nasogastric Tube Necessary After Alimentary Tract Surgery?Document4 pagesIs Nasogastric Tube Necessary After Alimentary Tract Surgery?Coy EnNo ratings yet
- Bedside Assessment of Swallowing: A Useful Screening Tool For Dysphagia in An Acute Geriatric WardDocument6 pagesBedside Assessment of Swallowing: A Useful Screening Tool For Dysphagia in An Acute Geriatric WardAulia RaysNo ratings yet
- Relationship Between The Incidence and Risk Factors of Postoperative Nausea and Vomiting in Patients With Intravenous Patient-Controlled AnalgesiaDocument6 pagesRelationship Between The Incidence and Risk Factors of Postoperative Nausea and Vomiting in Patients With Intravenous Patient-Controlled AnalgesiaRandi KhampaiNo ratings yet
- Afferent Loop Decompression Technique Is Associated With A Reduction in Pancreatic Fistula Following PancreaticoduodenectomyDocument10 pagesAfferent Loop Decompression Technique Is Associated With A Reduction in Pancreatic Fistula Following PancreaticoduodenectomyDrDipesh Kumar YadavNo ratings yet
- Timing of Oral Intake After Esophagectomy A Narrative Review ofDocument19 pagesTiming of Oral Intake After Esophagectomy A Narrative Review ofAna RosiNo ratings yet
- Percutaneous Radiological Gastrostomy: A Safe and Effective Method of Nutritional Tube Placement in Advanced ALSDocument3 pagesPercutaneous Radiological Gastrostomy: A Safe and Effective Method of Nutritional Tube Placement in Advanced ALSaruna pramaNo ratings yet
- Editorial What Is The Best Endoscopic Treatment For Pancreatic PseudocystDocument4 pagesEditorial What Is The Best Endoscopic Treatment For Pancreatic PseudocystLogical MonsterNo ratings yet
- 2014 Maeda Neumonia y Higiene AncianosDocument6 pages2014 Maeda Neumonia y Higiene AncianosIvan Ramos GutarraNo ratings yet
- Endoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudyDocument6 pagesEndoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudySamuel0651No ratings yet
- Non-Invasive Assessment Determine The Swallowing and RespirationDocument6 pagesNon-Invasive Assessment Determine The Swallowing and RespirationDaniela OrtizNo ratings yet
- Wang, CH Et Al (2016) Non-Invasive Assessment of Swallowing and Respiration Coordination For The OSA Patient.Document10 pagesWang, CH Et Al (2016) Non-Invasive Assessment of Swallowing and Respiration Coordination For The OSA Patient.Carla Francisca Rojas MerelloNo ratings yet
- Restrictive Fluids in Septic Shock. NEJM 2022Document12 pagesRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- Original Contribution: Abd-Elazeem Elbakry, Wesam-Eldin Sultan, Ezzeldin IbrahimDocument6 pagesOriginal Contribution: Abd-Elazeem Elbakry, Wesam-Eldin Sultan, Ezzeldin IbrahimWALTER GARCÍA TERCERONo ratings yet
- Background: ISRCTN08758735Document2 pagesBackground: ISRCTN08758735Sav GaNo ratings yet
- @medicinejournal European Journal of Pediatric Surgery January 2020Document126 pages@medicinejournal European Journal of Pediatric Surgery January 2020Ricardo Uzcategui ArreguiNo ratings yet
- Objectively Measured Vs Self-Reported Compliance During Oral Appliance Therapy For Sleep-Disordered BreathingDocument8 pagesObjectively Measured Vs Self-Reported Compliance During Oral Appliance Therapy For Sleep-Disordered Breathing陈延珑No ratings yet
- Evaluación de TosDocument8 pagesEvaluación de TosCarolina CelisNo ratings yet
- Yilmaz, 2006Document7 pagesYilmaz, 2006titaNo ratings yet
- Influence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientsDocument6 pagesInfluence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientscamiladelgadomNo ratings yet
- Research Article: Pancreatoduodenectomy With or Without Pyloric Preservation: A Clinical Outcomes ComparisonDocument9 pagesResearch Article: Pancreatoduodenectomy With or Without Pyloric Preservation: A Clinical Outcomes ComparisonHiroj BagdeNo ratings yet
- Singer 1999Document7 pagesSinger 1999anton.neonatusNo ratings yet
- Efficacy of Bronchoalveolar Lavage As Adjunct Therapy in The Treatment of Neonatal Severe PneumoniaDocument6 pagesEfficacy of Bronchoalveolar Lavage As Adjunct Therapy in The Treatment of Neonatal Severe Pneumoniaanita awNo ratings yet
- Estenosis Traqueal ComplejaDocument8 pagesEstenosis Traqueal ComplejaFabiolaNo ratings yet
- Lidocaine Spray On An Endoscope Immediately Before Gi-5-067Document5 pagesLidocaine Spray On An Endoscope Immediately Before Gi-5-067Byung ChaNo ratings yet
- Wang 2015Document7 pagesWang 2015api-307002076No ratings yet
- 08.screening Pacientes Con TQTDocument11 pages08.screening Pacientes Con TQTCarlonchaCáceresNo ratings yet
- Comparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous NephrolithotomyDocument5 pagesComparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous Nephrolithotomynaufal12345No ratings yet
- 702 1383 1 PB PDFDocument7 pages702 1383 1 PB PDFEko RistiyantoNo ratings yet
- 10 1056@NEJMoa1908681Document10 pages10 1056@NEJMoa1908681alvaroNo ratings yet
- The Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrenceDocument5 pagesThe Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrencezanafiraNo ratings yet
- Chapter-41 Nasojejunal Tube Placement: January 2016Document12 pagesChapter-41 Nasojejunal Tube Placement: January 2016Issa AbuzeidNo ratings yet
- Tracheostomy and Intubation Related DysphagiaDocument25 pagesTracheostomy and Intubation Related DysphagiaVikashNo ratings yet
- Point-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFDocument12 pagesPoint-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFJohana FuentesNo ratings yet
- International Wound Journal - 2016 - Bobkiewicz - Management of Enteroatmospheric Fistula With Negative Pressure WoundDocument10 pagesInternational Wound Journal - 2016 - Bobkiewicz - Management of Enteroatmospheric Fistula With Negative Pressure WoundDiana Carolina RochaNo ratings yet
- EsomeprazoleDocument7 pagesEsomeprazoleSanjay NavaleNo ratings yet
- Epidural Analgesia in Critically Ill Patients With Acute Pancreatitis: The Multicentre Randomised Controlled EPIPAN Study ProtocolDocument10 pagesEpidural Analgesia in Critically Ill Patients With Acute Pancreatitis: The Multicentre Randomised Controlled EPIPAN Study ProtocolApriany Fitri SangajiNo ratings yet
- Vur KoreanDocument7 pagesVur KoreanIoannis ValioulisNo ratings yet
- EsofagusDocument7 pagesEsofagusWillie VanegasNo ratings yet
- Updates in Endourological Management of Urolithiasis: Joseph KM Li, Jeremy YC Teoh and Chi-Fai NGDocument12 pagesUpdates in Endourological Management of Urolithiasis: Joseph KM Li, Jeremy YC Teoh and Chi-Fai NGJorge Vazquez VazquezNo ratings yet
- Lee 2017Document6 pagesLee 2017Heine MüllerNo ratings yet
- Remifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized StudyDocument7 pagesRemifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized Studyade_liaNo ratings yet
- Complicacion Enteros Clinics 2015Document13 pagesComplicacion Enteros Clinics 2015Yoeli Marisa Escandon EspinozaNo ratings yet
- Posterior Tibial Nerve Stimulation As Treatment For The Overactive BladderDocument5 pagesPosterior Tibial Nerve Stimulation As Treatment For The Overactive BladderSendyA-AzizNo ratings yet
- Uri 2011Document5 pagesUri 2011anton.neonatusNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- HHS Public Access: Cognitive-Behavioral Therapy For A 9-Year-Old Girl With Disruptive Mood Dysregulation DisorderDocument20 pagesHHS Public Access: Cognitive-Behavioral Therapy For A 9-Year-Old Girl With Disruptive Mood Dysregulation DisorderRafael MartinsNo ratings yet
- Mud ArchitectureDocument13 pagesMud ArchitectureHarsha Madumali PadmasekaraNo ratings yet
- Global Tourism Travel Trends 2023Document5 pagesGlobal Tourism Travel Trends 2023DG Cooperación e Integración InternacionalNo ratings yet
- Harris Hotel and Convention Hall BekasiDocument14 pagesHarris Hotel and Convention Hall BekasiMonica VrettyciaNo ratings yet
- CCNA Cyber Ops (Version 1.1) - Chapter 6 Exam Answers FullDocument20 pagesCCNA Cyber Ops (Version 1.1) - Chapter 6 Exam Answers FullRawan AlharbiNo ratings yet
- 2018 Long Bow Insulator CUSTOMER OVERVIEWDocument10 pages2018 Long Bow Insulator CUSTOMER OVERVIEWJulian GuerreroNo ratings yet
- Restuarant KolkataDocument9 pagesRestuarant KolkataSulagna Basu DasNo ratings yet
- Crios BrochureDocument28 pagesCrios BrochureAhmed IbrahimNo ratings yet
- Grade 9 - Week - 4 - TLEDocument15 pagesGrade 9 - Week - 4 - TLEAlthea Marie MartinNo ratings yet
- MDR 9DDocument104 pagesMDR 9DDiana MarcelaNo ratings yet
- Keeler Portable Slit Lamp - Service ManualDocument16 pagesKeeler Portable Slit Lamp - Service ManualRajaram PanduranganNo ratings yet
- Designing An Ideal Operating Room Complex.5Document7 pagesDesigning An Ideal Operating Room Complex.5panda kohtetNo ratings yet
- Instructions For UseDocument16 pagesInstructions For UseMirkoNo ratings yet
- Mobilization With MovementDocument8 pagesMobilization With Movementapi-661333402No ratings yet
- Biomes & Food Security Booklet (7638)Document30 pagesBiomes & Food Security Booklet (7638)Ivy NguyenNo ratings yet
- Sikap Stakeholder Terhadap Inovasi, Implikasi, Dan Dampak Dari Penggunaan Bioteknologi Pada Usaha Ternak Sapi PerahDocument10 pagesSikap Stakeholder Terhadap Inovasi, Implikasi, Dan Dampak Dari Penggunaan Bioteknologi Pada Usaha Ternak Sapi PerahhasnaNo ratings yet
- Engineering Mechanics (ME 105) Tutorial Sheet-4Document4 pagesEngineering Mechanics (ME 105) Tutorial Sheet-4nsbaruaoleNo ratings yet
- MeningitisDocument2 pagesMeningitisiamELHIZANo ratings yet
- Acid Base Tit RationsDocument2 pagesAcid Base Tit RationsIra MunirahNo ratings yet
- Franchise ROIDocument1 pageFranchise ROI帝宝星 June WongNo ratings yet
- Bananaleaffoodpackaging IOSR JESTFT 2020Document6 pagesBananaleaffoodpackaging IOSR JESTFT 2020kannaNo ratings yet
- John Miller PerezDocument3 pagesJohn Miller PerezJomillPerezNo ratings yet
- Chapter 1Document13 pagesChapter 1babak84No ratings yet
- Worksheet in HCX - Absence - BRANCHES (1) (AutoRecovered)Document66 pagesWorksheet in HCX - Absence - BRANCHES (1) (AutoRecovered)Christian de LunaNo ratings yet
- Catálogo M-DA InglêsDocument20 pagesCatálogo M-DA Inglêsjf2003No ratings yet
- Pre-Work Identifying Facts 1.) Legal Dispute-Annulment 2.) Rewriting The Legal DisputeDocument10 pagesPre-Work Identifying Facts 1.) Legal Dispute-Annulment 2.) Rewriting The Legal DisputeDeb GonzalesNo ratings yet