You might also like
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- ABCs of ECGs: A Guide to Basic ECG InterpretationDocument67 pagesABCs of ECGs: A Guide to Basic ECG InterpretationSuresh ChevagoniNo ratings yet
- Presentasi Ws Ekg SakinahDocument40 pagesPresentasi Ws Ekg SakinahsiskaNo ratings yet
- Abnormal ECG Findings ExplainedDocument26 pagesAbnormal ECG Findings ExplainedApriliani Nur Puspita SariNo ratings yet
- EKG Abnormalities: Types of Pathology IdentifiedDocument133 pagesEKG Abnormalities: Types of Pathology IdentifiedShofiyyatunnisa' WsNo ratings yet
- Common ECGsDocument40 pagesCommon ECGsTejwani MuskanNo ratings yet
- Abnormal ECG 1Document26 pagesAbnormal ECG 1Apriliani Nur Puspita SariNo ratings yet
- Ecg Cheat Sheet 35Document2 pagesEcg Cheat Sheet 35jessjaylee80% (5)
- ELECTROCARDIOGRAMDocument63 pagesELECTROCARDIOGRAMMbah GapinbissiNo ratings yet
- Basics and Interpretation: Sif HansdottirDocument65 pagesBasics and Interpretation: Sif Hansdottirwenny1186100% (1)
- Read ECGDocument128 pagesRead ECGrehmatakuNo ratings yet
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (9)
- Technical AspectsDocument4 pagesTechnical AspectsNathan T. CheungNo ratings yet
- ARITMIA, Gangguan Irama JantungDocument37 pagesARITMIA, Gangguan Irama JantungNovriefta NugrahaNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- THE NORMAL ELECTROCARDIOGRAM: DIAGNOSING MEDICAL PROBLEMS WITH AN ECGDocument63 pagesTHE NORMAL ELECTROCARDIOGRAM: DIAGNOSING MEDICAL PROBLEMS WITH AN ECGPuravin Crishan VeerasamyNo ratings yet
- ECGDocument198 pagesECGKatrina Maravilla100% (1)
- Cardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyDocument87 pagesCardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyummimalikihamidNo ratings yet
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniNo ratings yet
- Cardiac Arrhythmia GuideDocument93 pagesCardiac Arrhythmia GuideEdalyn CapiliNo ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Workshop Pit IV THN 2017Document57 pagesWorkshop Pit IV THN 2017anettepardedeNo ratings yet
- 3881 - Prosedur Pendaftaran Internship Per November 2016Document57 pages3881 - Prosedur Pendaftaran Internship Per November 2016Munawir_Syam91No ratings yet
- ECG Basics Lecture 1Document116 pagesECG Basics Lecture 1AreebaNo ratings yet
- Normal ECGDocument63 pagesNormal ECGMohd Johari Mohd ShafuwanNo ratings yet
- EKG Common Clinical ArrhythmiasDocument54 pagesEKG Common Clinical ArrhythmiasFaisal AlhasNo ratings yet
- ECGDocument70 pagesECGgemergencycareNo ratings yet
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- PacemakerDocument156 pagesPacemakerDhruv DesaiNo ratings yet
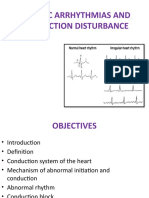
- Cardiac Arrhythmias and Conduction Disturbances GuideDocument42 pagesCardiac Arrhythmias and Conduction Disturbances GuideassumptaNo ratings yet
- Topnotch ECG Interpretation For MoonlightersDocument25 pagesTopnotch ECG Interpretation For Moonlightersmefav7778520100% (1)
- EKG 12 Lead GuideDocument59 pagesEKG 12 Lead GuideM Lukman HakimNo ratings yet
- ECGDocument115 pagesECGBhakti WashilkarNo ratings yet
- EKG Eh Kasi GanitoDocument44 pagesEKG Eh Kasi GanitoAnonymous ic2CDkFNo ratings yet
- Dysrhythmia Recognition Pocket Reference Card PDFDocument14 pagesDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (2)
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocument34 pagesEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- Normal Impulse Conduction: Sinoatrial NodeDocument80 pagesNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- Cardiocon ECG Workshop Basics of ECGDocument80 pagesCardiocon ECG Workshop Basics of ECGshazia kaziNo ratings yet
- 35ekg 1Document103 pages35ekg 1Veerapong Vattanavanit100% (2)
- ECG tutorial covers basics, axis, waves, intervals, hypertrophy and moreDocument56 pagesECG tutorial covers basics, axis, waves, intervals, hypertrophy and morefeby_valNo ratings yet
- ECG UpdatedDocument115 pagesECG Updatedmominarasool7No ratings yet
- Cardiovascular Alterations (1)Document46 pagesCardiovascular Alterations (1)aneesnair86No ratings yet
- ECG InterpretationDocument95 pagesECG InterpretationShiela Mae Lopez100% (10)
- ECG AbnormalDocument60 pagesECG Abnormalvidishmalaviya300No ratings yet
- ECG Rhythm Interpretation: Recognize Arrhythmias and Interpret ECGsDocument232 pagesECG Rhythm Interpretation: Recognize Arrhythmias and Interpret ECGslaureeateNo ratings yet
- Normal R Wave - R Wave Height Gradually Increased Up To V4 and Then DecreaseDocument6 pagesNormal R Wave - R Wave Height Gradually Increased Up To V4 and Then DecreaseNabighah ZukriNo ratings yet
- PDF DocumentDocument40 pagesPDF DocumentsalikiqbalNo ratings yet
- Ecg Basics - NAVEENDocument65 pagesEcg Basics - NAVEENNaveen MathieuNo ratings yet
- Ecg 1Document40 pagesEcg 1doctorhanifNo ratings yet
- Nursing School EKGDocument43 pagesNursing School EKGRob Dickerson100% (1)
- THE Electrocardiogram (Ecg / Ekg) : By: DR Yasir MansouriDocument83 pagesTHE Electrocardiogram (Ecg / Ekg) : By: DR Yasir Mansourirofi modiNo ratings yet
- EKG Interpretation Guide: The 10 Key Steps for Reading EKGsDocument66 pagesEKG Interpretation Guide: The 10 Key Steps for Reading EKGsAltama L. SidartaNo ratings yet
- Ecg Crit - CareDocument55 pagesEcg Crit - CarekrismatactayNo ratings yet
- NURV 456 Telemetry Interpretation StudentDocument56 pagesNURV 456 Telemetry Interpretation StudentMarie Yi100% (2)
- Basic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalDocument79 pagesBasic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalVeerapong Vattanavanit0% (1)
- Wswecocekgdasar2018Document34 pagesWswecocekgdasar2018Hendra AbeitNo ratings yet
- Cardiology Ekg BoardDocument87 pagesCardiology Ekg BoardPutri WijayaNo ratings yet
- CardiologyDocument99 pagesCardiologySimple LyricsNo ratings yet
- Basic Ecg Interpretation Powerpoint For The OsceDocument20 pagesBasic Ecg Interpretation Powerpoint For The OsceCHARLOTTE DU PREEZNo ratings yet
- Law Terms PDFDocument65 pagesLaw Terms PDFtarunaggarwal11No ratings yet
- Criminal Law (Arts. 1-237)Document124 pagesCriminal Law (Arts. 1-237)MiGay Tan-Pelaez94% (18)
- Complaint Affidavit MayapaDocument3 pagesComplaint Affidavit MayapaLuke Concepcion-ButayNo ratings yet
- Sample Affidavit Arresting OfficersDocument2 pagesSample Affidavit Arresting OfficersVonAllenBatario100% (6)
- Natsci2 Sy 2013-2014Document10 pagesNatsci2 Sy 2013-2014VonAllenBatarioNo ratings yet
- Poker Strategies: Joe Pasquale CSE87: UCSD Freshman Seminar On The Science of Casino Games: Theory of Poker Spring 2006Document71 pagesPoker Strategies: Joe Pasquale CSE87: UCSD Freshman Seminar On The Science of Casino Games: Theory of Poker Spring 2006antohif100% (2)
- Forensic Science Chapter 2 Notes: 2-1 Processing The Crime SceneDocument6 pagesForensic Science Chapter 2 Notes: 2-1 Processing The Crime SceneVonAllenBatarioNo ratings yet
- Psychological AutopsyDocument18 pagesPsychological AutopsytrancelucenceNo ratings yet
- Their First MillionDocument13 pagesTheir First MillionzamudiogpeNo ratings yet
- ALTERATION/ ABNORMAL FINDINGS IN PULSEDocument7 pagesALTERATION/ ABNORMAL FINDINGS IN PULSEShalabh JoharyNo ratings yet
- Circulation BioHackDocument9 pagesCirculation BioHackManav SinghNo ratings yet
- Desfibrilador, Mca. Zoll. Mod. PD 1400 - Manual Del OperadorDocument65 pagesDesfibrilador, Mca. Zoll. Mod. PD 1400 - Manual Del OperadorMiris RebollarNo ratings yet
- Normal Values ChartDocument1 pageNormal Values ChartHiesel Madera VaronaNo ratings yet
- Intensive Care Unit Arrhythmias: S.M. HollenbergDocument13 pagesIntensive Care Unit Arrhythmias: S.M. HollenbergEvita FebriyantiNo ratings yet
- Cardiogenic Shock NclexDocument81 pagesCardiogenic Shock NclexKrishna SapkotaNo ratings yet
- Physiology CVS MCQ (Dr. Nassar)Document23 pagesPhysiology CVS MCQ (Dr. Nassar)زياد سعيدNo ratings yet
- ACLS Rhythms For The ACLS Algorithms: AppendixDocument32 pagesACLS Rhythms For The ACLS Algorithms: Appendixyan_ricci19100% (4)
- Cardiovascular System Physiology LectureDocument28 pagesCardiovascular System Physiology LecturevincenzoNo ratings yet
- Intra Aortic Balloon Pump (IABP) : Past, Present and FutureDocument10 pagesIntra Aortic Balloon Pump (IABP) : Past, Present and FutureAlladi SrujanNo ratings yet
- 1851 8692 1 PBDocument9 pages1851 8692 1 PBFirda ShofiaNo ratings yet
- Cardiac ArrestDocument64 pagesCardiac ArrestJoel Estacio100% (1)
- (Nelson Hour) The CV System - HX and PEDocument30 pages(Nelson Hour) The CV System - HX and PEJustin Ng SincoNo ratings yet
- CardiostartDocument6 pagesCardiostartbiomedicaNo ratings yet
- Why 360j Clinical OverviewDocument8 pagesWhy 360j Clinical OverviewPepperNo ratings yet
- MOH Pocket Manual in Emergency MedicineDocument244 pagesMOH Pocket Manual in Emergency MedicineAli Al-Brahim (AlucardAli)No ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Test Bank For Ecg Essentials of Electrocardiography 1st Edition by SotoDocument9 pagesTest Bank For Ecg Essentials of Electrocardiography 1st Edition by Sotopamelachavezbawyoemckf100% (26)
- Kalnirnay 2023 Marathi CalendarDocument24 pagesKalnirnay 2023 Marathi CalendarAparna Sachin Tembulkar67% (3)
- Hypertensive Crisis JournalDocument5 pagesHypertensive Crisis JournalRaena SepryanaNo ratings yet
- Announcement List Displayed Poster 32nd ASMIHADocument36 pagesAnnouncement List Displayed Poster 32nd ASMIHADewi AmeliaNo ratings yet
- VT 2Document49 pagesVT 2Micija CucuNo ratings yet
- RV (Dys)function assessment by echocardiographyDocument52 pagesRV (Dys)function assessment by echocardiographyNag Mallesh RaoNo ratings yet
- Ecas 2015 PDFDocument154 pagesEcas 2015 PDFsilkairsNo ratings yet
- Cardiovascular SystemDocument34 pagesCardiovascular Systemurooj100% (1)
- Aha Acls Manual Pdf Free Download GuideDocument4 pagesAha Acls Manual Pdf Free Download GuideRidma Irsyam SeptadiNo ratings yet
- Circulatory System NotesDocument6 pagesCirculatory System NotesShayan UzzamanNo ratings yet
- Cardiovascular RegulationDocument40 pagesCardiovascular RegulationeliseudesafateNo ratings yet
- Acute Coronary Syndrome Case FileDocument4 pagesAcute Coronary Syndrome Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Effect of Deep Breathing on Blood Pressure in Hypertensive PatientsDocument10 pagesEffect of Deep Breathing on Blood Pressure in Hypertensive PatientssendyNo ratings yet