You might also like
- Wisdom Chi KungDocument0 pagesWisdom Chi KungDevlinPyxNo ratings yet
- How to Give a Woman the Most Powerful OrgasmDocument10 pagesHow to Give a Woman the Most Powerful OrgasmFederico Ceferino BrizuelaNo ratings yet
- Atty. Carla Santamaria-Seña Wills and Succession ReviewDocument111 pagesAtty. Carla Santamaria-Seña Wills and Succession ReviewvickimabelliNo ratings yet
- CA Prostate by Dr. Musaib MushtaqDocument71 pagesCA Prostate by Dr. Musaib MushtaqDr. Musaib MushtaqNo ratings yet
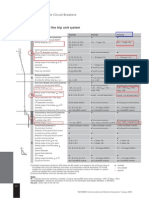
- ETU 776 TripDocument1 pageETU 776 TripbhaskarinvuNo ratings yet
- Neuromodulation PDFDocument18 pagesNeuromodulation PDFSureshNo ratings yet
- Comp Carlyle Torque PDFDocument125 pagesComp Carlyle Torque PDFjsnavarro1o100% (2)
- Connectomic Deep Brain StimulationFrom EverandConnectomic Deep Brain StimulationAndreas HornNo ratings yet
- Module 6 - Accounting Cycle 1 - Recording Business Transactions and Accounting For Service Entities - Part BDocument29 pagesModule 6 - Accounting Cycle 1 - Recording Business Transactions and Accounting For Service Entities - Part BAbelNo ratings yet
- Nerve Conduction StudiesDocument10 pagesNerve Conduction StudiesRyanNo ratings yet
- Stereotactic Implantation of Deep BrainDocument28 pagesStereotactic Implantation of Deep Brainberna chuaNo ratings yet
- Neurostimulation For Functional Recovery After.2Document8 pagesNeurostimulation For Functional Recovery After.2Mateo MendozaNo ratings yet
- Pi Is 2949669123000179Document3 pagesPi Is 2949669123000179Santoso SantosoNo ratings yet
- Deep Brain Stimulation: Applications and Challenges: Neeraj Tripathi Vipan KakkarDocument4 pagesDeep Brain Stimulation: Applications and Challenges: Neeraj Tripathi Vipan KakkarRahul SharmaNo ratings yet
- 1 s2.0 S000632232101461X MainDocument11 pages1 s2.0 S000632232101461X MainMayner MoranNo ratings yet
- Translational Principles of Deep Brain Stimulation: ReviewsDocument13 pagesTranslational Principles of Deep Brain Stimulation: ReviewsbleaurosenNo ratings yet
- HILL Et Al, 2015Document12 pagesHILL Et Al, 2015Gilson Mariano NeryNo ratings yet
- Montgomery 2014Document26 pagesMontgomery 2014Santoso SantosoNo ratings yet
- A Systematic Review and Meta-Analysis of Transcranial Direct-Current Stimulation Effects On Cognitive Function in Patients With Alzheimer 'S DiseaseDocument10 pagesA Systematic Review and Meta-Analysis of Transcranial Direct-Current Stimulation Effects On Cognitive Function in Patients With Alzheimer 'S DiseaseAlireza MajdiNo ratings yet
- Brainsci 09 00005Document8 pagesBrainsci 09 00005Javier Leonardo Rocha BeltranNo ratings yet
- Review DBSDocument8 pagesReview DBSEtonia PangNo ratings yet
- ML in DBS Systematic Review PreprintDocument20 pagesML in DBS Systematic Review PreprintBen AllenNo ratings yet
- Deep Brain Stimulation Mechanisms and Next-Generation Therapies in PsychiatryDocument11 pagesDeep Brain Stimulation Mechanisms and Next-Generation Therapies in PsychiatryDhino Armand Quispe SánchezNo ratings yet
- França (2018) Brain StimulationDocument12 pagesFrança (2018) Brain StimulationAna paula CamargoNo ratings yet
- Lee Et Al, 2022Document11 pagesLee Et Al, 2022Bruno KudekenNo ratings yet
- Yco 0000000000000361Document16 pagesYco 0000000000000361Büşra Züleyha DoğanNo ratings yet
- Lozano DBS CurrentStatus NatReviews2020Document13 pagesLozano DBS CurrentStatus NatReviews2020bobNo ratings yet
- Estimulação Cerebral Não Invasiva para o Tratamento Da Disartria Neurogênica - RevisãoDocument10 pagesEstimulação Cerebral Não Invasiva para o Tratamento Da Disartria Neurogênica - Revisãonathalia suellenNo ratings yet
- Clinical Implementation of Noninvasive Brain.15Document6 pagesClinical Implementation of Noninvasive Brain.15Papu FloresNo ratings yet
- Boissonnault2021 Article BrainStimulationInAttentionDefDocument9 pagesBoissonnault2021 Article BrainStimulationInAttentionDef奚浩然No ratings yet
- 10.1007@s10916 020 1535 7Document10 pages10.1007@s10916 020 1535 7Lim Chia SeangNo ratings yet
- 2021Document21 pages2021yaoqi903No ratings yet
- De BerkerDocument6 pagesDe Berkerhyperion1No ratings yet
- Linköping University Post PrintDocument26 pagesLinköping University Post PrintVidya MuthukrishnanNo ratings yet
- Brainsci 10 00310Document14 pagesBrainsci 10 00310GUSTAVO CARIBÉNo ratings yet
- 1 s2.0 S0933365721001913 MainDocument13 pages1 s2.0 S0933365721001913 MainBen AllenNo ratings yet
- Eeg UsDocument6 pagesEeg UsnetoNo ratings yet
- World Neurosurgery: X: Teodor Svedung Wettervik, Anders Lew En, Per EnbladDocument13 pagesWorld Neurosurgery: X: Teodor Svedung Wettervik, Anders Lew En, Per EnbladVictor Hugo SilveiraNo ratings yet
- Diving Into The Subcortex The Potential of Chronic Subcortical Se - 2022 - NeurDocument12 pagesDiving Into The Subcortex The Potential of Chronic Subcortical Se - 2022 - NeurÍtalo CésarNo ratings yet
- 2023 Article 1776Document32 pages2023 Article 1776Bruno MañonNo ratings yet
- New approaches to stroke recoveryDocument9 pagesNew approaches to stroke recoverymandeep axonNo ratings yet
- Paper Frontiers TOC-DBS Varjao21Document12 pagesPaper Frontiers TOC-DBS Varjao21TatianeDanielNo ratings yet
- Improving Working Memory Exploring The Effect of Transcranial RandomDocument6 pagesImproving Working Memory Exploring The Effect of Transcranial RandomDanish MujibNo ratings yet
- Defeito Craniano Tdcs TbiDocument19 pagesDefeito Craniano Tdcs TbiAmandavictooriaNo ratings yet
- Periodic Artifact Removal With Applications To Deep Brain StimulationDocument8 pagesPeriodic Artifact Removal With Applications To Deep Brain StimulationRuiqi GuoNo ratings yet
- ArticuloDocument17 pagesArticuloregina albertosNo ratings yet
- Stagg 2018Document9 pagesStagg 2018GUSTAVO CARIBÉNo ratings yet
- Cranial Electrotherapy Stimulation and TDocument8 pagesCranial Electrotherapy Stimulation and TMarcel J. SiemeNo ratings yet
- 2348 0548.190064 1Document8 pages2348 0548.190064 1Ankita MohtaNo ratings yet
- safetyaspect in tDCS in patient and healthy subjectsDocument7 pagessafetyaspect in tDCS in patient and healthy subjectslabsoneducationNo ratings yet
- Kuo Et Al., 2013Document5 pagesKuo Et Al., 2013casNo ratings yet
- Cognitive Enhancement - StimulationDocument2 pagesCognitive Enhancement - StimulationSwathi KartikNo ratings yet
- NERVE CONDUCTION STUDIES: ESSENTIALS AND PITFALLS IN PRACTICEpdfDocument9 pagesNERVE CONDUCTION STUDIES: ESSENTIALS AND PITFALLS IN PRACTICEpdfEduardo BessoloNo ratings yet
- Neuromodulation by Means of Electrical Brain Stimulation: AbstractsDocument5 pagesNeuromodulation by Means of Electrical Brain Stimulation: AbstractsmoiNo ratings yet
- Wenzel 2021Document13 pagesWenzel 2021T.U. Pai João da Caridade & Caboclo FlechasNo ratings yet
- J Neurol Neurosurg Psychiatry 2005 Mallik Ii23 31Document10 pagesJ Neurol Neurosurg Psychiatry 2005 Mallik Ii23 31أحمد عطيةNo ratings yet
- Neuromodulación No Invasiva para Potenciar La Rehabilitación de La Heminegligencia Tras Un IctusDocument1 pageNeuromodulación No Invasiva para Potenciar La Rehabilitación de La Heminegligencia Tras Un IctusRed Menni de Daño CerebralNo ratings yet
- Effects of Repeated Anodal TDCS Coupled With Cognitive Training For Patients With Severe Traumatic Brain Injury: A Pilot Randomized Controlled TrialDocument10 pagesEffects of Repeated Anodal TDCS Coupled With Cognitive Training For Patients With Severe Traumatic Brain Injury: A Pilot Randomized Controlled TrialAmandaNo ratings yet
- Personalised, Image-Guided, Noninvasive Brain Stimulation in Gliomas - Rationale, Challenges & OpportunitiesDocument12 pagesPersonalised, Image-Guided, Noninvasive Brain Stimulation in Gliomas - Rationale, Challenges & OpportunitiesshylajaNo ratings yet
- Brain Stimulation DeviceDocument17 pagesBrain Stimulation DevicedheenadayalanNo ratings yet
- Neuro-Cardiac-guided TMSDocument11 pagesNeuro-Cardiac-guided TMSRafael MoreiraNo ratings yet
- PIIS2058534917300975Document6 pagesPIIS2058534917300975phaniNo ratings yet
- % Dextrose Water As The Primary: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengDocument18 pages% Dextrose Water As The Primary: Stanley K. H. Lam, Kenneth Dean Reeves, and An-Lin ChengFloyd. BNo ratings yet
- Deep Brain Stimulation Research PaperDocument8 pagesDeep Brain Stimulation Research Papergipinin0jev2100% (1)
- henry-c-skrehot-neuro-stimulation-in-focal-epilepsy-aDocument10 pageshenry-c-skrehot-neuro-stimulation-in-focal-epilepsy-aArbey Aponte PuertoNo ratings yet
- tDCS in pediatric hemiparesisDocument1 pagetDCS in pediatric hemiparesislabsoneducationNo ratings yet
- tmp9F14 TMPDocument24 pagestmp9F14 TMPFrontiersNo ratings yet
- Medical School Admission RequirementsDocument2 pagesMedical School Admission RequirementskensusantoNo ratings yet
- UCLA El Camino English MajorDocument1 pageUCLA El Camino English MajorkensusantoNo ratings yet
- UCLA Chemistry El Camino Transfer 2021-2022Document2 pagesUCLA Chemistry El Camino Transfer 2021-2022kensusantoNo ratings yet
- BS in Mathematics for Medical and Life SciencesDocument1 pageBS in Mathematics for Medical and Life ScienceskensusantoNo ratings yet
- Easy GE's - Easy GEsDocument2 pagesEasy GE's - Easy GEskensusantoNo ratings yet
- Tarzan Problem in PhysicsDocument1 pageTarzan Problem in PhysicskensusantoNo ratings yet
- Assist Org Articulation Agreement UCI & El Camino Applied Physics 2020Document2 pagesAssist Org Articulation Agreement UCI & El Camino Applied Physics 2020kensusantoNo ratings yet
- Assist Org Articulation Agreement UCI & El Camino Biological Sciences 2020Document3 pagesAssist Org Articulation Agreement UCI & El Camino Biological Sciences 2020kensusantoNo ratings yet
- Multivariable Exam Placement Practice - TestDocument4 pagesMultivariable Exam Placement Practice - TestkensusantoNo ratings yet
- Math of Computation PlanDocument1 pageMath of Computation PlanNikhil KurmalaNo ratings yet
- 2020 - 2021 El Camino Transfer Timeline - v10.5.20Document1 page2020 - 2021 El Camino Transfer Timeline - v10.5.20kensusantoNo ratings yet
- Tarzan Problem in PhysicsDocument1 pageTarzan Problem in PhysicskensusantoNo ratings yet
- RoboTurret ManualDocument2 pagesRoboTurret ManualkensusantoNo ratings yet
- 2020 - FACTS - of Most Applicants From Which Univ To Medical SchoolsDocument7 pages2020 - FACTS - of Most Applicants From Which Univ To Medical SchoolskensusantoNo ratings yet
- Arduino Curriculum Grid - Starterkit - Engineeringr2Document2 pagesArduino Curriculum Grid - Starterkit - Engineeringr2kensusantoNo ratings yet
- Binary Socket ProtocolDocument9 pagesBinary Socket ProtocolkensusantoNo ratings yet
- UCLA EE-worksheet - 16 - 20Document1 pageUCLA EE-worksheet - 16 - 20kensusantoNo ratings yet
- Mobile inverted pendulum vehicle prototype analyzed in IEEE paperDocument7 pagesMobile inverted pendulum vehicle prototype analyzed in IEEE paperkensusantoNo ratings yet
- UCR Computer Science Requirement CoursesDocument2 pagesUCR Computer Science Requirement CourseskensusantoNo ratings yet
- College of Natural and Agricultural Sciences B.S. Breadth RequirementsDocument2 pagesCollege of Natural and Agricultural Sciences B.S. Breadth RequirementskensusantoNo ratings yet
- Brain Control RobotDocument9 pagesBrain Control RobotkensusantoNo ratings yet
- UCLA Mathematics of ComputationDocument2 pagesUCLA Mathematics of ComputationkensusantoNo ratings yet
- College of Natural and Agricultural Sciences B.S. Breadth RequirementsDocument2 pagesCollege of Natural and Agricultural Sciences B.S. Breadth RequirementskensusantoNo ratings yet
- UCLA MAE Robotics PHD SyllabusDocument7 pagesUCLA MAE Robotics PHD SyllabuskensusantoNo ratings yet
- Lab EquipmentDocument2 pagesLab EquipmentkensusantoNo ratings yet
- UCLA Engineering Orientation-Handbook-2019-2020Document28 pagesUCLA Engineering Orientation-Handbook-2019-2020kensusantoNo ratings yet
- El Camino Transfer To UCLA Math MajorDocument3 pagesEl Camino Transfer To UCLA Math MajorkensusantoNo ratings yet
- UCLA Computer Science and Engineering B.S.Document3 pagesUCLA Computer Science and Engineering B.S.kensusantoNo ratings yet
- LAHC Summer 2019 Class ScheduleDocument26 pagesLAHC Summer 2019 Class SchedulekensusantoNo ratings yet
- Periodic Table AdvancedDocument1 pagePeriodic Table Advancedapi-287426421No ratings yet
- Method Statement - 23apr18Document5 pagesMethod Statement - 23apr18hinitahNo ratings yet
- Presentation 1Document20 pagesPresentation 1anon_658550121No ratings yet
- Common Admission Test (CAT) 2020 Admit Card: BarcodeDocument2 pagesCommon Admission Test (CAT) 2020 Admit Card: BarcodeViraaj ThakurNo ratings yet
- All India Integrated Test Series: JEE (Main) - 2022Document17 pagesAll India Integrated Test Series: JEE (Main) - 2022Beyond ur imagination100% (1)
- UK-India Coffee Market ReportDocument27 pagesUK-India Coffee Market ReportNikhil MunjalNo ratings yet
- Sri Venkateswara Caterers Tiffin MenuDocument4 pagesSri Venkateswara Caterers Tiffin MenuJPDGLNo ratings yet
- Root of Women’s Oppression According to Psychoanalytic FeminismDocument8 pagesRoot of Women’s Oppression According to Psychoanalytic FeminismPrincess Janine SyNo ratings yet
- CP107 Vol II-ERT 2B - 12-Dec 2019 (PA) - 3Document209 pagesCP107 Vol II-ERT 2B - 12-Dec 2019 (PA) - 3NghiaNo ratings yet
- Goat anatomy and physiology guideDocument8 pagesGoat anatomy and physiology guideLochi GmNo ratings yet
- 17EEX01-FUNDAMENTALS OF FIBRE OPTICS AND LASER INSTRUMENTATION SyllabusDocument2 pages17EEX01-FUNDAMENTALS OF FIBRE OPTICS AND LASER INSTRUMENTATION SyllabusJayakumar ThangavelNo ratings yet
- The Giant First YearDocument1,234 pagesThe Giant First YearEthan DyerNo ratings yet
- Qatar ScriptDocument1 pageQatar ScriptTheodore Palmares ArellanoNo ratings yet
- Biochemistry I BCM211: Zatilfarihiah RasdiDocument24 pagesBiochemistry I BCM211: Zatilfarihiah Rasdiستي نوراسيقينNo ratings yet
- Spain-Final ProjectDocument29 pagesSpain-Final Projectapi-264431075No ratings yet
- The Bone DreamingDocument3 pagesThe Bone DreamingastrozzNo ratings yet
- Parts of The CellDocument3 pagesParts of The Cellapi-308745623No ratings yet
- Solutions: Key Words and ConceptsDocument4 pagesSolutions: Key Words and ConceptsSamuel Enrique Cano PatocNo ratings yet
- Ethics in Animal-Based Research: Dominik Gross René H. TolbaDocument15 pagesEthics in Animal-Based Research: Dominik Gross René H. TolbaIuliana MogaNo ratings yet
- Formula Costo SandblastingDocument20 pagesFormula Costo SandblastingSerch VillaNo ratings yet
- Under The Oak Tree Part 2Document94 pagesUnder The Oak Tree Part 2suakasenaNo ratings yet
- Assignment Estimates & Time Phased Student TEMPLATE V1Document4 pagesAssignment Estimates & Time Phased Student TEMPLATE V1Usman AwanNo ratings yet
- AcetophenoneDocument3 pagesAcetophenonepriteshpatNo ratings yet
- Xii Physical Education PracticalDocument3 pagesXii Physical Education PracticalAayush AdlakNo ratings yet