You might also like
- Golden Dawn 2 9 The Moon BreathDocument4 pagesGolden Dawn 2 9 The Moon BreathF_RCNo ratings yet
- Medical Terminology TermsDocument28 pagesMedical Terminology TermsNikka Moreen DagdagNo ratings yet
- ES vs SIGINT: Understanding the DifferencesDocument9 pagesES vs SIGINT: Understanding the DifferencesYasir ShigileeniNo ratings yet
- Trilogy Suite Op. 5 (Instrumental) : ' B B B B 'Document21 pagesTrilogy Suite Op. 5 (Instrumental) : ' B B B B 'xander trujillo100% (1)
- Captured Ammunition Bulletin No 1Document34 pagesCaptured Ammunition Bulletin No 1roberto porto100% (1)
- Aplastic AnemiaDocument26 pagesAplastic AnemiaIrina Moldovan100% (1)
- ABC of Clinical HematologyDocument82 pagesABC of Clinical Hematologydokice100% (1)
- Engineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignDocument28 pagesEngineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignMehdi NouriNo ratings yet
- Miniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDocument4 pagesMiniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDenis CarlosNo ratings yet
- Pathogenesis and Classification of Eosinophil Disorders A Review of Recent Developments in The FieldDocument21 pagesPathogenesis and Classification of Eosinophil Disorders A Review of Recent Developments in The FieldpanduNo ratings yet
- Angle of Depression Lesson for Grade 9 MathDocument6 pagesAngle of Depression Lesson for Grade 9 MathPatrick Guerra100% (1)
- Mechanisms of Disease: Review ArticlesDocument9 pagesMechanisms of Disease: Review ArticlesNurhaslina HasNo ratings yet
- Understanding Eosinophilia: Causes, Pathogenesis and Treatment ApproachesDocument6 pagesUnderstanding Eosinophilia: Causes, Pathogenesis and Treatment ApproachesDanielSeneorNo ratings yet
- Eosinophilia: A Pragmatic Approach To Diagnosis and TreatmentDocument6 pagesEosinophilia: A Pragmatic Approach To Diagnosis and TreatmentLucas BrasilNo ratings yet
- Blood and Bone Marrow Evaluation for EosinophiliaDocument8 pagesBlood and Bone Marrow Evaluation for Eosinophilialubna aloshibiNo ratings yet
- Eosinophilic Maignancies ClassificationDocument7 pagesEosinophilic Maignancies ClassificationshirlvetNo ratings yet
- Eosinophil Biology and Causes of Eosinophilia - UpToDateDocument35 pagesEosinophil Biology and Causes of Eosinophilia - UpToDateBls PriyaNo ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptNabila ApriyanNo ratings yet
- Approach To Suspected Hypereosinophilic Syndrome ASHBloodDocument8 pagesApproach To Suspected Hypereosinophilic Syndrome ASHBloodarimasen88No ratings yet
- 3,.algoritmo Eosinofilia PDFDocument9 pages3,.algoritmo Eosinofilia PDFMiguel ArmidaNo ratings yet
- Eosinophilic Disorders: Current Reviews of Allergy and Clinical ImmunologyDocument10 pagesEosinophilic Disorders: Current Reviews of Allergy and Clinical ImmunologyItzi PaNo ratings yet
- Eo Pulmonares 2016Document22 pagesEo Pulmonares 2016Jaime BarraganNo ratings yet
- I How I Treat Hypereosinophilic SyndromesDocument10 pagesI How I Treat Hypereosinophilic SyndromesCesia ConstanzaNo ratings yet
- Eosinophin in Infectious DiseaseDocument29 pagesEosinophin in Infectious DiseasentnquynhproNo ratings yet
- Eosinophilia StatPearls NCBIBookshelfDocument7 pagesEosinophilia StatPearls NCBIBookshelfLinh HươngNo ratings yet
- Neumopatia EosinofilicaDocument22 pagesNeumopatia EosinofilicaSaidNo ratings yet
- Causes and Evaluation of Eosinophilia: An OverviewTITLEDocument11 pagesCauses and Evaluation of Eosinophilia: An OverviewTITLEmaryNo ratings yet
- Amoebiasi S: Prof. Mrs. Vibha JacobDocument54 pagesAmoebiasi S: Prof. Mrs. Vibha JacobVibha JacobNo ratings yet
- Allergology International: Hironobu IhnDocument3 pagesAllergology International: Hironobu Ihncreyesdear3978No ratings yet
- Abordaje Del Paciente Con EosinofiliaDocument14 pagesAbordaje Del Paciente Con EosinofiliaSaidNo ratings yet
- DownloadDocument3 pagesDownloadbesttiktokfindsshopNo ratings yet
- Arpa - 2018 0219 RaDocument6 pagesArpa - 2018 0219 Rahuseikha velayazulfahdNo ratings yet
- Eosinophilic DermatosesDocument15 pagesEosinophilic DermatosesmikelNo ratings yet
- Steven Johnson SyndromeDocument13 pagesSteven Johnson SyndromeKhairul AnwarNo ratings yet
- Applied Therapeutics Lec 8Document18 pagesApplied Therapeutics Lec 8human.44697No ratings yet
- Systemic Lupus Erythematosus in Dogs and CatsDocument7 pagesSystemic Lupus Erythematosus in Dogs and CatsJireh SlatNo ratings yet
- Case Report: Wouter Meersseman, Patrick Verschueren, Thomas Tousseyn, Rita de Vos, David CassimanDocument1 pageCase Report: Wouter Meersseman, Patrick Verschueren, Thomas Tousseyn, Rita de Vos, David Cassimanmafe alvarezNo ratings yet
- Peripheral blood eosinophilia in atopic dermatitisDocument6 pagesPeripheral blood eosinophilia in atopic dermatitisdhita01No ratings yet
- 10 1111@jdv 13706Document15 pages10 1111@jdv 13706Raisa KhairuniNo ratings yet
- Piis0002934310002937 PDFDocument2 pagesPiis0002934310002937 PDFMuhammad TamlikhaNo ratings yet
- CANINE-CAnine Systemic Lupus Erythematosus - Part IDocument7 pagesCANINE-CAnine Systemic Lupus Erythematosus - Part Itaner_soysurenNo ratings yet
- Paper English 3 - DONEDocument21 pagesPaper English 3 - DONESarita AmeliaNo ratings yet
- Review of LiteratureDocument20 pagesReview of LiteratureNithya sudevNo ratings yet
- Caz de Toxoplasmoza CutanataDocument7 pagesCaz de Toxoplasmoza Cutanatacatalina criceaNo ratings yet
- Autoimmune Polyendocrine Syndromes: Review ArticleDocument10 pagesAutoimmune Polyendocrine Syndromes: Review Articleinterna MANADONo ratings yet
- Erythema Nodosum Leprosum: A Review of the Pathogenesis and ManagementDocument10 pagesErythema Nodosum Leprosum: A Review of the Pathogenesis and ManagementSelly DamayantiNo ratings yet
- OpsoclonusDocument3 pagesOpsoclonusIRENA GENINo ratings yet
- Eosinophil Diversity in AsthmaDocument7 pagesEosinophil Diversity in AsthmaRodríguez PabloNo ratings yet
- Prolonged Fever, Hepatosplenomegaly, and Pancytopenia in A 46-Year-Old WomanDocument6 pagesProlonged Fever, Hepatosplenomegaly, and Pancytopenia in A 46-Year-Old WomanFerdy AlviandoNo ratings yet
- Urology Case Reports: Shakhawan Hama Amin Said, Rezhin Yaseen Abdalla, Ismaeel Aghaways, Ari Mohammed AbdullahDocument3 pagesUrology Case Reports: Shakhawan Hama Amin Said, Rezhin Yaseen Abdalla, Ismaeel Aghaways, Ari Mohammed AbdullahHardiTariqHammaNo ratings yet
- Psoriais PDF NemDocument14 pagesPsoriais PDF NemFabiola VillanuevaNo ratings yet
- Eosinophils in The GI TractDocument15 pagesEosinophils in The GI TractdkbritobNo ratings yet
- Case Report Hypereosinophilic Syndrome PDFDocument11 pagesCase Report Hypereosinophilic Syndrome PDFFriska RamadayantiNo ratings yet
- Entamoeba Histolytica PDFDocument5 pagesEntamoeba Histolytica PDFViand NugrohoNo ratings yet
- Mank Ad 2015Document8 pagesMank Ad 2015IleNo ratings yet
- EosinófilosDocument13 pagesEosinófilosdkbritobNo ratings yet
- Eosinophils in Vasculitis Characteristics - Khoury-Nrrheum.2014.98Document11 pagesEosinophils in Vasculitis Characteristics - Khoury-Nrrheum.2014.98Francisco Baca DejoNo ratings yet
- Medical Management Update: Oral Surgery Oral Medicine Oral PathologyDocument5 pagesMedical Management Update: Oral Surgery Oral Medicine Oral PathologyLujainNo ratings yet
- Epithelioid Soft Tissue Tumors PDFDocument11 pagesEpithelioid Soft Tissue Tumors PDFnohemi9No ratings yet
- Example of Presentations For ResidentsDocument112 pagesExample of Presentations For Residentsapi-303541804No ratings yet
- EOSINOFILIADocument23 pagesEOSINOFILIAMarcoNo ratings yet
- Crows On 2009Document29 pagesCrows On 2009woouuw0903No ratings yet
- Vesicubullous Diseases & Mucocutaneous DisordersDocument23 pagesVesicubullous Diseases & Mucocutaneous Disordersshahlaraib001No ratings yet
- Atypical Lymphocytes in Peripheral BloodDocument11 pagesAtypical Lymphocytes in Peripheral BloodAfni YusnitaNo ratings yet
- Congenital Nevus Skull Defect Risk MelanomaDocument3 pagesCongenital Nevus Skull Defect Risk MelanomaAna Flavia BaptistaNo ratings yet
- Angiolymphoid Hyperplasia With Eosinophilia in The Lungs: A Complex Name For An Innocuous Disease?Document2 pagesAngiolymphoid Hyperplasia With Eosinophilia in The Lungs: A Complex Name For An Innocuous Disease?Sango AyraNo ratings yet
- White Blood CellsDocument2 pagesWhite Blood Cellsهاشم ابوطالبNo ratings yet
- Tumor PleuraDocument6 pagesTumor PleuraJuan Pablo PérezNo ratings yet
- Falciforme y Pulmon 2008Document12 pagesFalciforme y Pulmon 2008xander trujilloNo ratings yet
- Distúrbios Ácido Básicos Revisão NEJM 2014-1Document12 pagesDistúrbios Ácido Básicos Revisão NEJM 2014-1sabrinamgrNo ratings yet
- Eferesis 2008Document17 pagesEferesis 2008xander trujilloNo ratings yet
- Resistant or Difficult-To-Control HypertensionDocument8 pagesResistant or Difficult-To-Control Hypertensionxander trujilloNo ratings yet
- Anmia MicrociticaDocument8 pagesAnmia MicrociticafabitoxxpepeNo ratings yet
- ADA Guidelines 2012Document53 pagesADA Guidelines 2012Jones PessoaNo ratings yet
- ADA Guidelines 2012Document53 pagesADA Guidelines 2012Jones PessoaNo ratings yet
- WR2 PDFDocument9 pagesWR2 PDFJoni MokodoNo ratings yet
- Thyroiditis: Review ArticleDocument10 pagesThyroiditis: Review Articlexander trujilloNo ratings yet
- Adrenal Urgencias Urgencias 2014Document20 pagesAdrenal Urgencias Urgencias 2014xander trujilloNo ratings yet
- Guia Del EspiritistaDocument8 pagesGuia Del Espiritistaxander trujilloNo ratings yet
- Hiperparatiro e HipoparatiroismoDocument13 pagesHiperparatiro e Hipoparatiroismoxander trujilloNo ratings yet
- Adrenal DX y TX EmergenciasDocument20 pagesAdrenal DX y TX Emergenciasxander trujilloNo ratings yet
- TX LipidosDocument14 pagesTX Lipidosxander trujilloNo ratings yet
- Clinical Practice: Subclinical HyperthyroidismDocument5 pagesClinical Practice: Subclinical Hyperthyroidismxander trujilloNo ratings yet
- Hypothyroidism: Causes, Killers, and Life-Saving TreatmentsDocument15 pagesHypothyroidism: Causes, Killers, and Life-Saving Treatmentsxander trujilloNo ratings yet
- Accf Aha Pulmonary HypertensionDocument49 pagesAccf Aha Pulmonary Hypertensionxander trujilloNo ratings yet
- Osteoporosis Esc Re NingDocument8 pagesOsteoporosis Esc Re Ningxander trujilloNo ratings yet
- Antiplatelet DrugsDocument33 pagesAntiplatelet Drugsxander trujilloNo ratings yet
- Diabetes Hiperglicemias UrgenciasDocument16 pagesDiabetes Hiperglicemias Urgenciasxander trujilloNo ratings yet
- MODULE-2-VETTECH325 (2)Document31 pagesMODULE-2-VETTECH325 (2)cejproiloNo ratings yet
- Enzyme ActivityDocument3 pagesEnzyme ActivityNabindra Ruwali100% (2)
- C32 MOTOR CAT Electronic Unit Injector - TestDocument2 pagesC32 MOTOR CAT Electronic Unit Injector - TestFreddy Villegas100% (1)
- Bernard BTB MIG GunsDocument8 pagesBernard BTB MIG GunsEdwin Mauricio Gallego OsorioNo ratings yet
- Eliminating False Detection: Sensing Guide Pulse Level SensorDocument16 pagesEliminating False Detection: Sensing Guide Pulse Level SensorRafael MirandaNo ratings yet
- 6kW V2G EV Charger Module Datasheet (2018)Document2 pages6kW V2G EV Charger Module Datasheet (2018)pysogaNo ratings yet
- Survival Analysis Tutorial on Mammary Carcinogenesis RiskDocument4 pagesSurvival Analysis Tutorial on Mammary Carcinogenesis Riskthermopolis3012100% (1)
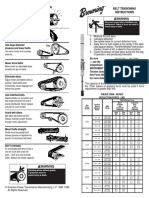
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- Pharmacy Preceptors Guild of The Philippines: ObjectiveDocument4 pagesPharmacy Preceptors Guild of The Philippines: ObjectiveCarline ScarletNo ratings yet
- Resume Curt JerromeDocument5 pagesResume Curt JerromeAashish MuraliNo ratings yet
- Al-Imam Al-Kadhum College For Islamic Science Department: Computer Eng. 1 Stage Electrical M.SC. Worod Adris ShutnanDocument38 pagesAl-Imam Al-Kadhum College For Islamic Science Department: Computer Eng. 1 Stage Electrical M.SC. Worod Adris ShutnanMêly CrêâzyGîrlNo ratings yet
- Solitaire Premier - Presentation (Small File)Document18 pagesSolitaire Premier - Presentation (Small File)Shrikant BadheNo ratings yet
- Part 1Document52 pagesPart 1Jeffry Daud BarrungNo ratings yet
- Orac Charts - BuenisimoDocument92 pagesOrac Charts - BuenisimosanthigiNo ratings yet
- Pres. Quirino Treasured Child School, Inc.: Grade 8-St. Joseph & ST MatthewDocument2 pagesPres. Quirino Treasured Child School, Inc.: Grade 8-St. Joseph & ST MatthewChristian jade QuijanoNo ratings yet
- Global Resort List by Country (38 charactersDocument51 pagesGlobal Resort List by Country (38 charactersMaulik ShahNo ratings yet
- Principles of Marketing - Product, Service and Experience DifferencesDocument26 pagesPrinciples of Marketing - Product, Service and Experience DifferencesVivien Leigh LopezNo ratings yet
- Entrepreneurship Macro Environment ForcesDocument26 pagesEntrepreneurship Macro Environment ForcesSivaNo ratings yet
- Material ManagementDocument106 pagesMaterial ManagementRomi AfriansyahNo ratings yet
- DesignDocument2 pagesDesignAmr AbdalhNo ratings yet
- Exercitii AdjectivDocument3 pagesExercitii AdjectivFirma GSCNo ratings yet
- Shangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Document2 pagesShangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Salma FarooqNo ratings yet
- Factors to Consider in Reactor Design for Industrial ProcessesDocument3 pagesFactors to Consider in Reactor Design for Industrial Processesuma villashini100% (2)