You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Apple's Global Supply ChainDocument22 pagesApple's Global Supply Chaindilip jadeja75% (4)
- Demo Teaching - FinalDocument28 pagesDemo Teaching - FinalZyza Gracebeth Elizalde - RolunaNo ratings yet
- NST Application - GmiDocument14 pagesNST Application - GmiAnmol SinghNo ratings yet
- The Influence of Managerial Ability On Future Performance: Journal of Economics, Business, and Government ChallengesDocument7 pagesThe Influence of Managerial Ability On Future Performance: Journal of Economics, Business, and Government ChallengesKevinNo ratings yet
- ML QuestionsDocument56 pagesML QuestionsPavan KumarNo ratings yet
- Multiple Choice QuizDocument3 pagesMultiple Choice QuizRavi Arjun KumarNo ratings yet
- SOP (Business Analytics)Document3 pagesSOP (Business Analytics)saurabhjadhav09No ratings yet
- Informs Schedule PDFDocument39 pagesInforms Schedule PDFYuvraj GuptaNo ratings yet
- Data Analysis Course: Time Series Analysis & Forecasting (Version-1)Document43 pagesData Analysis Course: Time Series Analysis & Forecasting (Version-1)vishal rajNo ratings yet
- Saketh Rao Data AnalystDocument2 pagesSaketh Rao Data Analystvalish silverspace100% (1)
- Data Processing & StatisticalDocument21 pagesData Processing & StatisticalJhonwyn Orgas0% (1)
- Data Analysis and Mixed MethodsDocument23 pagesData Analysis and Mixed MethodsBeria Panalangin DungaoNo ratings yet
- SSC 201Document14 pagesSSC 201Adebayo OmojuwaNo ratings yet
- Slides 06 - Data AnalysisDocument24 pagesSlides 06 - Data AnalysisNathaniel FelicianoNo ratings yet
- Menstrual Hygiene and PracticesDocument24 pagesMenstrual Hygiene and PracticesShaji Viswanathan. Mcom, MBA (U.K)No ratings yet
- BRM Unit 5Document6 pagesBRM Unit 5nileshNo ratings yet
- ML FinalDocument28 pagesML FinalShreya100% (1)
- 05 Soares+et+al V3Document7 pages05 Soares+et+al V3Elsa Marta SoaresNo ratings yet
- Great Step Data AbstractDocument3 pagesGreat Step Data AbstractSri Chandra DudduNo ratings yet
- Marks Hi Marks: Be Comp MCQ PDFDocument878 pagesMarks Hi Marks: Be Comp MCQ PDFSpiderspider2021100% (1)
- Stat. & Prob. 4th Q.Document4 pagesStat. & Prob. 4th Q.romulito.sanicoNo ratings yet
- Geostatistical AnalisysDocument17 pagesGeostatistical AnalisysRizal Adi PrabowoNo ratings yet
- Meta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingDocument21 pagesMeta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingTyler Lawrence CoyeNo ratings yet
- Two-Way ANOVA RCBDDocument32 pagesTwo-Way ANOVA RCBDNathan DrakeNo ratings yet
- 2020 - (Sankaran) - Data Analytics in Reservoir EngineeringDocument107 pages2020 - (Sankaran) - Data Analytics in Reservoir EngineeringPedro100% (1)
- Audit Delay Sinta 4 - 24774782Document16 pagesAudit Delay Sinta 4 - 24774782Trisujatmiko winataNo ratings yet
- Hss 4101 Quizlet FinalDocument4 pagesHss 4101 Quizlet FinalAyman WNo ratings yet
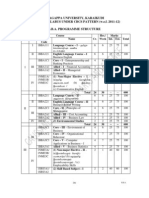
- Alagappa University, Karaikudi Revised Syllabus Under Cbcs Pattern (W.E.F. 2011-12) B.B.A. Programme StructureDocument23 pagesAlagappa University, Karaikudi Revised Syllabus Under Cbcs Pattern (W.E.F. 2011-12) B.B.A. Programme StructureMathan NaganNo ratings yet
- Lecture 6 MulticollinearityDocument25 pagesLecture 6 MulticollinearityMah DoNo ratings yet
- (Anna Esposito, Marcos Faundez-Zanuy, Eric Keller, (BookFi)Document337 pages(Anna Esposito, Marcos Faundez-Zanuy, Eric Keller, (BookFi)Anonymous AdKJGlXHNo ratings yet