You might also like
- Sample Treatment Plan With Goals For Anxiety and DepressionDocument3 pagesSample Treatment Plan With Goals For Anxiety and Depressionapi-310813184100% (1)
- CCRP CourseDocument19 pagesCCRP CourseKathryn May0% (1)
- Physiology: Guevara, Henaku-Larbi, Inciong, JutizDocument3 pagesPhysiology: Guevara, Henaku-Larbi, Inciong, JutizMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: Block 1Document9 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: Block 1Mavic Villanueva100% (1)
- Ethics and Law For The Health Professions PDFDocument2 pagesEthics and Law For The Health Professions PDFDavid14% (7)
- HypoglycaemiaDocument3 pagesHypoglycaemiakristine keen buanNo ratings yet
- Clinical Trial Gadavala SarahDocument60 pagesClinical Trial Gadavala SarahSejal khuman100% (1)
- 01 - Overview of The Cardiovascular Physiology - ACPDocument6 pages01 - Overview of The Cardiovascular Physiology - ACPMavic VillanuevaNo ratings yet
- Clinical Research MethodologyDocument11 pagesClinical Research MethodologymisganaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument4 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic Villanueva100% (1)
- National University of Study and Research in Law, RanchiDocument10 pagesNational University of Study and Research in Law, RanchiRakesh K SNo ratings yet
- Impaired Physical Mobility Related To Pain and DiscomfortDocument2 pagesImpaired Physical Mobility Related To Pain and DiscomfortRis NapolisNo ratings yet
- Initial Pages PDFDocument16 pagesInitial Pages PDFIulia ElenaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument6 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic Villanueva100% (1)
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument4 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic VillanuevaNo ratings yet
- Primer: Must-Know On PH Vaccine TrialsDocument20 pagesPrimer: Must-Know On PH Vaccine TrialsWeeaboo Franz VlogsNo ratings yet
- Clinical Trials PDFDocument17 pagesClinical Trials PDFBin Hip100% (2)
- Introduction To Clinical TrialsDocument31 pagesIntroduction To Clinical Trialsmuhammad murtaza89% (9)
- Unani Formulations For Management of DiaDocument15 pagesUnani Formulations For Management of Diacharanmann9165No ratings yet
- Clinical Trials:Overview and OpportunitiesDocument23 pagesClinical Trials:Overview and OpportunitiesSasidhar RlcNo ratings yet
- Clinical Trials and Review & Approval of Clinical StudiesDocument55 pagesClinical Trials and Review & Approval of Clinical StudiesKinal MehtaNo ratings yet
- Principles of Translational Science in Medicine: From Bench to BedsideFrom EverandPrinciples of Translational Science in Medicine: From Bench to BedsideNo ratings yet
- Declaration of HelsinkiDocument11 pagesDeclaration of HelsinkiYzel Vasquez AdavanNo ratings yet
- Nurse Patient Ratio PDFDocument7 pagesNurse Patient Ratio PDFSafrina WaldiniNo ratings yet
- Medical Surgical Nursing AssignmentDocument166 pagesMedical Surgical Nursing AssignmentSonali Sengar0% (1)
- Clinical Trial: A Review: S. B. Thorat, S. K. Banarjee, D. D. Gaikwad, S. L. Jadhav, R. M. ThoratDocument6 pagesClinical Trial: A Review: S. B. Thorat, S. K. Banarjee, D. D. Gaikwad, S. L. Jadhav, R. M. ThoratResolve ItechNo ratings yet
- A Comprehensive Review of Clinical Trials and Their Role in Clinical Study DesignDocument8 pagesA Comprehensive Review of Clinical Trials and Their Role in Clinical Study DesignInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Design in Medical ResearchDocument6 pagesStudy Design in Medical ResearchAngelo Jude CobachaNo ratings yet
- LM 7 - 2020.02.22Document35 pagesLM 7 - 2020.02.22hiruniNo ratings yet
- ClinicalTrialTermsMethods LongForm 05NOV2021Document5 pagesClinicalTrialTermsMethods LongForm 05NOV2021ingles.kesherNo ratings yet
- 215 ArticleText 430 1 10 20170629Document6 pages215 ArticleText 430 1 10 20170629star warNo ratings yet
- Medical Research EthicsDocument20 pagesMedical Research EthicssaritahamdNo ratings yet
- 1 B Introduction To Clinical ResearchDocument21 pages1 B Introduction To Clinical ResearchanishphistarNo ratings yet
- Phases: ResearchDocument9 pagesPhases: ResearchMuskan AhujaNo ratings yet
- Human Experimentation With DrugsDocument11 pagesHuman Experimentation With Drugsllr.tyllbNo ratings yet
- PMOC 311 ASSIGNMENT 1 Drug Discovery and Drug Product Development 1184739989Document4 pagesPMOC 311 ASSIGNMENT 1 Drug Discovery and Drug Product Development 1184739989JUDYANN PINEDANo ratings yet
- Epidemiology and Clinical Research Design, Part 1 - Study TypesDocument23 pagesEpidemiology and Clinical Research Design, Part 1 - Study TypesShahiza Isa100% (1)
- MC N Med Dev Trials Compare With Drug TrialsDocument4 pagesMC N Med Dev Trials Compare With Drug TrialsAndrie JavsNo ratings yet
- Investigational New Drug Application (INDA)Document25 pagesInvestigational New Drug Application (INDA)Mallikarjun MangapuramNo ratings yet
- Nidhi - Human Experimentation With DrugsDocument12 pagesNidhi - Human Experimentation With Drugsllr.tyllbNo ratings yet
- Screening ProgramsDocument76 pagesScreening ProgramsMihretNo ratings yet
- 4b Experimental Studies 1Document68 pages4b Experimental Studies 1Emaan NoorNo ratings yet
- Investigational Use of DrugsDocument26 pagesInvestigational Use of DrugsShafaqat Ghani Shafaqat GhaniNo ratings yet
- Clinical Trial ProcessDocument16 pagesClinical Trial ProcessMohammed HammedNo ratings yet
- Science and Engineering: Background/IntroductionDocument8 pagesScience and Engineering: Background/IntroductionLustre GlarNo ratings yet
- Clinical TrialsDocument51 pagesClinical TrialsRajan JattNo ratings yet
- Chapter 13 NotesDocument3 pagesChapter 13 NotesRPh Krishna Chandra JagritNo ratings yet
- Overview of PharmacovigilanceDocument12 pagesOverview of PharmacovigilanceEditor IJTSRDNo ratings yet
- 17-6-2 CM Ethics in Trials PPDocument17 pages17-6-2 CM Ethics in Trials PPGeronimoNo ratings yet
- PMLS1Document9 pagesPMLS1julianneNo ratings yet
- Introduction To EpidemiologyDocument34 pagesIntroduction To Epidemiologyhamza khanNo ratings yet
- Preclinical TrialsDocument21 pagesPreclinical Trialsjeevalakshmanan29No ratings yet
- Canadian Fundamentals of Nursing - Chapter 6, 11Document9 pagesCanadian Fundamentals of Nursing - Chapter 6, 11elen.myNo ratings yet
- Module 1 - 2022 RevDocument46 pagesModule 1 - 2022 RevRaquel VargasNo ratings yet
- Research 101: Sponsored byDocument34 pagesResearch 101: Sponsored byMohammed HammedNo ratings yet
- EBM - DR BalqisDocument40 pagesEBM - DR BalqiscallNo ratings yet
- Screening For DiseaseDocument29 pagesScreening For DiseaseSrinidhi Nandhini Pandian100% (2)
- Preclinical Research ARiseor DawnDocument5 pagesPreclinical Research ARiseor DawnmarnNo ratings yet
- MTPMLSP111 Lesson 2Document7 pagesMTPMLSP111 Lesson 2lizdestacamento0625No ratings yet
- Drug Discovery and DevelopmentDocument17 pagesDrug Discovery and DevelopmentMarchelino Devan WibisonoNo ratings yet
- What Is Clinical Research?: 5520 Lyndon B Johnson FWY, Suite 100 Dallas, TX 75240Document3 pagesWhat Is Clinical Research?: 5520 Lyndon B Johnson FWY, Suite 100 Dallas, TX 75240Stacey HillNo ratings yet
- Presentation On PharmacologyDocument42 pagesPresentation On PharmacologySalehin2020No ratings yet
- GCP PDFDocument4 pagesGCP PDFbudiutom8307No ratings yet
- Clinical Research Trials and You: Questions & AnswersDocument4 pagesClinical Research Trials and You: Questions & AnswersNitya KrishnaNo ratings yet
- Test Bank For Pharmacology For Nurses A Pathophysiological Approach 1st Edition Michael Patrick Adams DownloadDocument36 pagesTest Bank For Pharmacology For Nurses A Pathophysiological Approach 1st Edition Michael Patrick Adams Downloadkentcarsonfxivk100% (28)
- Clinnical Trials-Zhou-2020Document21 pagesClinnical Trials-Zhou-2020mirabel IvanaliNo ratings yet
- Test Bank For Pharmacology For Nurses A Pathophysiological Approach 1st Edition Michael Patrick Adams DownloadDocument24 pagesTest Bank For Pharmacology For Nurses A Pathophysiological Approach 1st Edition Michael Patrick Adams Downloadroyfideliagxzq6No ratings yet
- Basic Clinical Trial TerminologyDocument2 pagesBasic Clinical Trial Terminologysatty1979No ratings yet
- Takind Part in Cancer TreatmentDocument11 pagesTakind Part in Cancer Treatmentfares HACIBNo ratings yet
- CLINICAL-PHARMACY ReviewerDocument21 pagesCLINICAL-PHARMACY ReviewerParamjit KaurNo ratings yet
- Screening TestsDocument9 pagesScreening Testssunma09082001No ratings yet
- Sample Presentation - Science InternshipDocument29 pagesSample Presentation - Science InternshipAmaayaNo ratings yet
- Types of Medical ResearchDocument31 pagesTypes of Medical ResearchTurkay Yildiz BayrakNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic VillanuevaNo ratings yet
- Physiology: Block 1Document3 pagesPhysiology: Block 1Mavic VillanuevaNo ratings yet
- Physiology: Table 1. Distinguishing Properties of Electrical and Chemical SynapsesDocument5 pagesPhysiology: Table 1. Distinguishing Properties of Electrical and Chemical SynapsesMavic VillanuevaNo ratings yet
- 08.17.2015 - Physiology - Lecture10 - ARN (EA)Document3 pages08.17.2015 - Physiology - Lecture10 - ARN (EA)Mavic VillanuevaNo ratings yet
- Physiology: Block 1Document5 pagesPhysiology: Block 1Mavic VillanuevaNo ratings yet
- 08.05.15 - Histology Lab Muscles Bones Cartilages Session01Document13 pages08.05.15 - Histology Lab Muscles Bones Cartilages Session01Mavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha MemorialDocument3 pagesSt. Luke's College of Medicine - William H. Quasha MemorialMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: EmbryologyDocument23 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: EmbryologyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: Block 1 Lab Session: 1 Facilitator: Dr. Arturo DecanoDocument11 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: Block 1 Lab Session: 1 Facilitator: Dr. Arturo DecanoMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument6 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- 08.17.15 - Histology Lab Epithelial Tissues and Skin Session01Document11 pages08.17.15 - Histology Lab Epithelial Tissues and Skin Session01Mavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument2 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument7 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: I. A. 1. 2. 3. B. 1. I. Ii. 2. C. 1. 2. 3. II. Iii. ADocument7 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: I. A. 1. 2. 3. B. 1. I. Ii. 2. C. 1. 2. 3. II. Iii. AMavic VillanuevaNo ratings yet
- General Pathology Supertrans Block 1Document10 pagesGeneral Pathology Supertrans Block 1Mavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument10 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument4 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument6 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument7 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- Basic Science Research: Lecture 1: Post-Ischemic Neovascularization and Blood FlowDocument3 pagesBasic Science Research: Lecture 1: Post-Ischemic Neovascularization and Blood FlowMavic VillanuevaNo ratings yet
- Pet/Ct Scan Information For Patients With DiabetesDocument3 pagesPet/Ct Scan Information For Patients With DiabetesAmethyst EsmeNo ratings yet
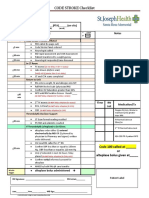
- CODE STROKE Checklist:: NotesDocument1 pageCODE STROKE Checklist:: NotesAdam MochtarNo ratings yet
- COPD vs. Asthma Symptoms: 6 Differences and 6 SimilaritiesDocument3 pagesCOPD vs. Asthma Symptoms: 6 Differences and 6 Similaritiessd saklineNo ratings yet
- Pengaruh Cara Pengambilan Darah Kapiler Terhadap Kadar Glukosa Darah Sewaktu Pada Penderita Diabetes MelitusDocument7 pagesPengaruh Cara Pengambilan Darah Kapiler Terhadap Kadar Glukosa Darah Sewaktu Pada Penderita Diabetes MelitusLinna Dedek KecillNo ratings yet
- Ritalin Gone WrongDocument6 pagesRitalin Gone WrongohlakhNo ratings yet
- Current Management of Cerebral GliomasDocument6 pagesCurrent Management of Cerebral GliomasResiden BedahNo ratings yet
- The Impact of Imagery On Cognition and Belief SystemsDocument5 pagesThe Impact of Imagery On Cognition and Belief Systemsblanca1958No ratings yet
- (RLE) Assessment of High-Risk Infants: Sumalinog, Tiffany Marie L. BSN 2BDocument19 pages(RLE) Assessment of High-Risk Infants: Sumalinog, Tiffany Marie L. BSN 2Blala byuNo ratings yet
- Naloxone PinsDocument8 pagesNaloxone PinsSherif IbrahimNo ratings yet
- Vallamai Event BrochureDocument3 pagesVallamai Event BrochureJağğuNo ratings yet
- Tentative Examination Schedule of Nursing Courses University Annual Exam - 2023Document5 pagesTentative Examination Schedule of Nursing Courses University Annual Exam - 2023ArtiNo ratings yet
- Curriculum Vitae: Personal Identification - : Name: Date of Birth Nationality: Gender: Social Situation: ResidencyDocument3 pagesCurriculum Vitae: Personal Identification - : Name: Date of Birth Nationality: Gender: Social Situation: ResidencyABDEL NASER TAWFIKNo ratings yet
- Cirrhosis: On This PageDocument23 pagesCirrhosis: On This PageHasna FauziyahNo ratings yet
- National Programme For Control of Blindness PDFDocument23 pagesNational Programme For Control of Blindness PDFRabiu Hassan MusaNo ratings yet
- What Is Medical Technology?Document5 pagesWhat Is Medical Technology?Bernadine Salado100% (1)
- Ritmupdate V01iss01 Apr Jun 2014 PDFDocument8 pagesRitmupdate V01iss01 Apr Jun 2014 PDFkaymartgNo ratings yet
- General Introduction To Medical LaboratoryDocument9 pagesGeneral Introduction To Medical Laboratorymisgana negeraNo ratings yet
- Case Report Analysis: Angeles University Foundation College of Nursing Medical Surgical Nursing Laboratory (NCM 0112 RLE)Document15 pagesCase Report Analysis: Angeles University Foundation College of Nursing Medical Surgical Nursing Laboratory (NCM 0112 RLE)Katreena SalvadorNo ratings yet
- The CONSORT Statement: ArticleDocument4 pagesThe CONSORT Statement: ArticleiikhsanhNo ratings yet
- Book Garba SamskaraDocument3 pagesBook Garba SamskaraYogaguru NehaNo ratings yet
- Direct Pulp Capping in Primary Molars: Report of Two CasesDocument3 pagesDirect Pulp Capping in Primary Molars: Report of Two Casesemie sitorusNo ratings yet
- Lady GuardDocument6 pagesLady Guardidayu9779No ratings yet