You might also like
- NGT ProcedureDocument5 pagesNGT ProcedureFrances MercadoNo ratings yet
- Differential DiagnosisDocument1 pageDifferential Diagnosisririz b100% (1)
- Lesson Plan in Science 4 - LajieDocument10 pagesLesson Plan in Science 4 - LajieMar JenNo ratings yet
- Policies and Procedures Manual Tube FeedingDocument4 pagesPolicies and Procedures Manual Tube FeedingDerick RanaNo ratings yet
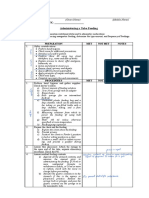
- Administering Tube FeedingDocument2 pagesAdministering Tube FeedingAlecsandra CabridoNo ratings yet
- Feeding Via Gastric GavageDocument3 pagesFeeding Via Gastric Gavageneleh gray0% (1)
- Tube FeedingDocument6 pagesTube FeedingKyla Shain GallegoNo ratings yet
- Tube Feeding (GavageDocument2 pagesTube Feeding (GavageevergrayelleNo ratings yet
- ) Administering Nasogastric Tube or Orogastric Tube FeedingDocument6 pages) Administering Nasogastric Tube or Orogastric Tube FeedingJohn Pearl FernandezNo ratings yet
- Skill 21 (1) ..Management of Gastrointestinal SuctionDocument1 pageSkill 21 (1) ..Management of Gastrointestinal SuctionnetsquadNo ratings yet
- NGT DemoDocument5 pagesNGT Demoeliza luisNo ratings yet
- PRS NGTDocument7 pagesPRS NGTMika Marielle TrincheraNo ratings yet
- Nasogastric Tube InsertionDocument8 pagesNasogastric Tube InsertionMayaPopbozhikovaNo ratings yet
- Nasogastric Tube FeedingDocument2 pagesNasogastric Tube FeedingKathrina Mendoza HembradorNo ratings yet
- NGTDocument5 pagesNGTElla CerenioNo ratings yet
- Sarasota Memorial Hospital Nursing Procedure Title: Date: Reviewed: Pages: Issued For: ResponsibilityDocument5 pagesSarasota Memorial Hospital Nursing Procedure Title: Date: Reviewed: Pages: Issued For: Responsibilitybalab2311No ratings yet
- IV InsertionDocument9 pagesIV InsertionSharmaine Grace FlorigNo ratings yet
- Nasogastric Tube Feeding Definition:: University of Eastern PhilippinesDocument2 pagesNasogastric Tube Feeding Definition:: University of Eastern PhilippinesJerika Shane MañosoNo ratings yet
- Nursing Procedure: Golden Gate Colleges College of NursingDocument9 pagesNursing Procedure: Golden Gate Colleges College of NursingJohn Paul Richard Mindanao100% (1)
- NGT and Colostomy Care ChecklistDocument8 pagesNGT and Colostomy Care ChecklistJurac AzilanaNo ratings yet
- NCM 321 RLE Procedural Checklist 2Document33 pagesNCM 321 RLE Procedural Checklist 2Eryl Franz HerreraNo ratings yet
- Nasogastric Tube - Enema ProceduresDocument3 pagesNasogastric Tube - Enema ProceduresJOSHUA DICHOSONo ratings yet
- Nasogastric Tube FeedingDocument2 pagesNasogastric Tube FeedingCelline Isabelle ReyesNo ratings yet
- NGT Feeding RemovingDocument2 pagesNGT Feeding RemovingMaria Carmela RoblesNo ratings yet
- Skill 24 (1) ..Administration of A Bolus FeedingDocument2 pagesSkill 24 (1) ..Administration of A Bolus FeedingnetsquadNo ratings yet
- Demo Bladder IrrigationDocument4 pagesDemo Bladder IrrigationTopeshwar TpkNo ratings yet
- Lavage Assisting With Gastric IntubationDocument3 pagesLavage Assisting With Gastric IntubationLea Jean Lobrigo OleaNo ratings yet
- NGT Feeding: by Group 2Document25 pagesNGT Feeding: by Group 2karl montano100% (1)
- Assisting in Gastric LavageDocument5 pagesAssisting in Gastric LavageJannen Casas100% (1)
- Naso Gastric Tube Insertion and RemovalDocument5 pagesNaso Gastric Tube Insertion and RemovalPia Mae BuayaNo ratings yet
- Medical Surgical Nursing: Gracious Colleg of Nursing Abhanpur Raipur (C.G.)Document9 pagesMedical Surgical Nursing: Gracious Colleg of Nursing Abhanpur Raipur (C.G.)Topeshwar TpkNo ratings yet
- Trach SuctionDocument3 pagesTrach SuctionKey Charyeth AlbanoNo ratings yet
- NGT InsertionDocument4 pagesNGT InsertionAngela Joy AmparadoNo ratings yet
- NGT NCM-116 ChecklistDocument9 pagesNGT NCM-116 ChecklistclaribelleNo ratings yet
- NCM 116 ChecklistsDocument11 pagesNCM 116 ChecklistsJoy DamoNo ratings yet
- Mabini Colleges Fundamentals of Nursing Gastric Gavage B. Continuous Drip Method EquipmentDocument2 pagesMabini Colleges Fundamentals of Nursing Gastric Gavage B. Continuous Drip Method EquipmentLea Jean Lobrigo OleaNo ratings yet
- Cebu City Medical Center-College of NursingDocument5 pagesCebu City Medical Center-College of NursingJimnah Rhodrick BontilaoNo ratings yet
- Nasogastric & Gavage - NsoDocument5 pagesNasogastric & Gavage - NsojamesNo ratings yet
- Identify Any Deficiencies, Excesses or Problems With DeliveryDocument3 pagesIdentify Any Deficiencies, Excesses or Problems With DeliveryWenalyn Grace Abella LlavanNo ratings yet
- Learning Activity N3A & N3BDocument3 pagesLearning Activity N3A & N3BMikaela JosonNo ratings yet
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Document18 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Nashebah A. BatuganNo ratings yet
- NGT Insertion Directly From CanvasDocument6 pagesNGT Insertion Directly From CanvasRico Delgado of WorldbexNo ratings yet
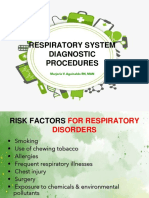
- Respiratory System Diagnostic Procedures: Marjorie V. Aguinaldo RN, MANDocument32 pagesRespiratory System Diagnostic Procedures: Marjorie V. Aguinaldo RN, MANKun KandaNo ratings yet
- Nasogastric Tube A. DefinitionDocument5 pagesNasogastric Tube A. Definitionkarl montanoNo ratings yet
- Fundamentals BulletsDocument12 pagesFundamentals Bulletsmaya reyesNo ratings yet
- Insertion of A Nasogastric TubeDocument3 pagesInsertion of A Nasogastric TubeJames Andre P. MoralesNo ratings yet
- Bladder IrrigationDocument14 pagesBladder IrrigationsandhyaNo ratings yet
- New NGT Checklist EditedDocument7 pagesNew NGT Checklist EditedRhona Marie AcuñaNo ratings yet
- Tube FeedingDocument50 pagesTube FeedingHari Priya TangiralaNo ratings yet
- Health Care Procedures - Nutrition and EliminationDocument11 pagesHealth Care Procedures - Nutrition and EliminationRS BuenavistaNo ratings yet
- PowerpointDocument78 pagesPowerpointMiNa SUy FullNo ratings yet
- Gavage FedingDocument9 pagesGavage FedingGeetha ReddyNo ratings yet
- Nasogastric Tube (Assissting in Indertion, Feeding) .ProcedureDocument4 pagesNasogastric Tube (Assissting in Indertion, Feeding) .ProcedureJeonoh FloridaNo ratings yet
- Nasogastric Tube FeedingDocument19 pagesNasogastric Tube FeedingMicah Alexis CandelarioNo ratings yet
- NGT PowerpointDocument19 pagesNGT Powerpointسانو روديلNo ratings yet
- Changing Fecal Pouching Colostomy)Document48 pagesChanging Fecal Pouching Colostomy)Champola Pola Camille BernardoNo ratings yet
- Pediatric Procedures PDFDocument6 pagesPediatric Procedures PDFSanjida Mithila100% (1)
- Peg Feeding RationaleDocument3 pagesPeg Feeding RationaleAlyzza Dagoy100% (1)
- NGT FeedingDocument74 pagesNGT FeedingGoddy Manzano100% (1)
- NGT Feeding ChecklistDocument4 pagesNGT Feeding ChecklistCee Sanchez100% (6)
- Diabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument12 pagesDiabetes Mellitus: Assessment Diagnosis Planning Intervention Rationale EvaluationDerick RanaNo ratings yet
- Letter of ProfessionalismDocument1 pageLetter of ProfessionalismDerick RanaNo ratings yet
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- Ic-01-048 Infection Control in Pediatric Intensive Care UnitDocument6 pagesIc-01-048 Infection Control in Pediatric Intensive Care UnitDerick RanaNo ratings yet
- Ic-01-047 Infection Control in Operating RoomDocument13 pagesIc-01-047 Infection Control in Operating RoomDerick RanaNo ratings yet
- Diabetes Nursing EducationDocument4 pagesDiabetes Nursing EducationDerick RanaNo ratings yet
- Diabetes Group ReportDocument34 pagesDiabetes Group ReportDerick RanaNo ratings yet
- Ic-01-040 Infection Control in Dental ClinicDocument11 pagesIc-01-040 Infection Control in Dental ClinicDerick RanaNo ratings yet
- Ic-01-049 Infection Control in Clinical EngineeringDocument4 pagesIc-01-049 Infection Control in Clinical EngineeringDerick RanaNo ratings yet
- Ic-01-041 Infection Control in DialysisDocument15 pagesIc-01-041 Infection Control in DialysisDerick RanaNo ratings yet
- Recruitment Checklist: Security Forces Hospital ProgramDocument4 pagesRecruitment Checklist: Security Forces Hospital ProgramDerick RanaNo ratings yet
- Ic-01-042 Infection Control in Emergency RoomDocument13 pagesIc-01-042 Infection Control in Emergency RoomDerick RanaNo ratings yet
- Policies and Procedures Manual Infection Control in General Nursing UnitDocument9 pagesPolicies and Procedures Manual Infection Control in General Nursing UnitDerick RanaNo ratings yet
- Ic-01-039 Infection Control in Adult Intensive Care UnitDocument7 pagesIc-01-039 Infection Control in Adult Intensive Care UnitDerick RanaNo ratings yet
- DEMENTIA Citical ExamDocument4 pagesDEMENTIA Citical ExamDerick RanaNo ratings yet
- Smith L (2017) Nursing Times 113: 12, 20-23Document59 pagesSmith L (2017) Nursing Times 113: 12, 20-23Derick RanaNo ratings yet
- Critical Care Notes BookDocument142 pagesCritical Care Notes BookDerick RanaNo ratings yet
- Ohhc Clean CatchDocument5 pagesOhhc Clean CatchDerick RanaNo ratings yet
- Emergency NursingDocument5 pagesEmergency NursingDerick RanaNo ratings yet
- NX Service Admin Practicum Packet-1Document12 pagesNX Service Admin Practicum Packet-1Derick RanaNo ratings yet
- Ohhc Laboratory ProceduresDocument3 pagesOhhc Laboratory ProceduresDerick RanaNo ratings yet
- Job Description: 1.1 Professional, Ethical and LegalDocument11 pagesJob Description: 1.1 Professional, Ethical and LegalDerick RanaNo ratings yet
- DOH Standards (Indicators)Document2 pagesDOH Standards (Indicators)Derick RanaNo ratings yet
- Ohhc Obtaining Stool Specimens For Laboratory AnalysisDocument8 pagesOhhc Obtaining Stool Specimens For Laboratory AnalysisDerick RanaNo ratings yet
- Presenting Complaint: ConstipationDocument5 pagesPresenting Complaint: ConstipationmiranaNo ratings yet
- Higado 1Document86 pagesHigado 1Carlos CuadrosNo ratings yet
- Liver DiseasesDocument114 pagesLiver DiseasesDayang Feineliza Samman BahjinNo ratings yet
- Prof. Barmawi KULIAH 5 AMOEBIASISDocument43 pagesProf. Barmawi KULIAH 5 AMOEBIASISTommy HardiantoNo ratings yet
- Operative Procedures in Surgical Gastroenterology Volume IIDocument275 pagesOperative Procedures in Surgical Gastroenterology Volume IIsalah subbahNo ratings yet
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoNo ratings yet
- Salivary Secretion: Chapter OutlineDocument9 pagesSalivary Secretion: Chapter OutlineJoshika MahendranNo ratings yet
- 7985 - Jadwal GIS 1920Document12 pages7985 - Jadwal GIS 1920amelia rahayuNo ratings yet
- Quiz 5 NDocument16 pagesQuiz 5 NabezareljvenNo ratings yet
- Git GutDocument4 pagesGit GutAngelica Murillo Ang-AngcoNo ratings yet
- CASE STUDY #2 Digestive System (Acute Pancreatitis)Document3 pagesCASE STUDY #2 Digestive System (Acute Pancreatitis)Lerma PagcaliwanganNo ratings yet
- Colonoscopy LandmarkDocument4 pagesColonoscopy LandmarkSueNo ratings yet
- What's The Difference Between Gastric and Duodenal Ulcers?Document6 pagesWhat's The Difference Between Gastric and Duodenal Ulcers?Anonymous cDy4bZMMNo ratings yet
- Final: Gluconeogenesis - When The Liver and KidneysDocument43 pagesFinal: Gluconeogenesis - When The Liver and KidneysRashid DayaoNo ratings yet
- Peritoneum 2022Document86 pagesPeritoneum 2022Tayyib KhanNo ratings yet
- Digestive System PowerpointDocument19 pagesDigestive System Powerpointapi-277974939No ratings yet
- Science CH - 2 - Jantuon Main PoshanDocument19 pagesScience CH - 2 - Jantuon Main PoshanVijay TrivediNo ratings yet
- Peptic Ulcer DiseaseDocument18 pagesPeptic Ulcer DiseaseAESTHETIC PHOTONo ratings yet
- Konsensus Konstipasi 2010Document8 pagesKonsensus Konstipasi 2010Lidya Ayu LestariNo ratings yet
- Motility Disorders of The GITDocument57 pagesMotility Disorders of The GITMahmoud AjinehNo ratings yet
- Digestive SystemDocument4 pagesDigestive SystemJM MatiasNo ratings yet
- PBL 5.2 (Git 1)Document46 pagesPBL 5.2 (Git 1)aiman mazlanNo ratings yet
- Assessment and Management of Patients With Biliary DisordersDocument18 pagesAssessment and Management of Patients With Biliary DisordersBheru LalNo ratings yet
- Acute Pancreatitis 2023Document25 pagesAcute Pancreatitis 2023raphael chidiebereNo ratings yet
- Important SlidesDocument5 pagesImportant Slidesgeert.schalkNo ratings yet
- Chronic Constipation in Rome 4 Era The Indian PerspectiveDocument11 pagesChronic Constipation in Rome 4 Era The Indian PerspectiveAbulHasan Idrus IstarNo ratings yet
- NCP2 FinalDocument2 pagesNCP2 FinallinlynNo ratings yet
- CH 06Document19 pagesCH 06cyberyeung0% (1)