You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Key Nursing SkillsDocument359 pagesKey Nursing Skillsmordanga100% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- JyothishaPrakaasham MeenaVijayaDocument52 pagesJyothishaPrakaasham MeenaVijayaAnonymous 5mSMeP2j100% (1)
- Piping TableDocument59 pagesPiping TableExsan Othman100% (2)
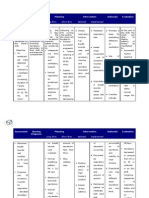
- Nursing Care Plan For Ineffective Airway ClearanceDocument7 pagesNursing Care Plan For Ineffective Airway Clearancearlee marquez96% (118)
- NCP-Risk For InfectionDocument2 pagesNCP-Risk For Infectioneihjay-bravo-804175% (81)
- Mini Project Report FinalDocument24 pagesMini Project Report FinalPrathamesh Parit100% (1)
- Study The Correlation of Clinker Quality, Reside, PSD On The Performance of Portland CementDocument12 pagesStudy The Correlation of Clinker Quality, Reside, PSD On The Performance of Portland CementIAEME PublicationNo ratings yet
- Pathophysiology AGEDocument2 pagesPathophysiology AGEMareeze Hatta100% (1)
- Pathophysiology AGEDocument2 pagesPathophysiology AGEMareeze Hatta100% (1)
- Mandibular Orthognathic ProceduresDocument104 pagesMandibular Orthognathic ProceduresDrSusmi ChebroluNo ratings yet
- TAHBSO PathophysiologyDocument5 pagesTAHBSO Pathophysiologybregette50% (2)
- Past Simple and Continuous-1Document8 pagesPast Simple and Continuous-1Prof. MARCU.CORINANo ratings yet
- Pathophysiology of Acute GastroenteritisDocument1 pagePathophysiology of Acute GastroenteritisJohn Glenn Bianzon80% (30)
- Blood and ImmunityDocument4 pagesBlood and ImmunityMareeze HattaNo ratings yet
- List of Successful Examinees in The May 2014 Nurse Licensure ExaminationDocument225 pagesList of Successful Examinees in The May 2014 Nurse Licensure ExaminationofwwatchNo ratings yet
- Product of Your Own Personal Library Research and Creative Thinking. If You Are Not Certain About The LevelDocument5 pagesProduct of Your Own Personal Library Research and Creative Thinking. If You Are Not Certain About The LevelMareeze HattaNo ratings yet
- Family Planning Allows People To Attain Their Desired Number of Children and Determine The Spacing of PregnanciesDocument6 pagesFamily Planning Allows People To Attain Their Desired Number of Children and Determine The Spacing of PregnanciesMareeze HattaNo ratings yet
- EDITED Health9 q1 Mod1Document17 pagesEDITED Health9 q1 Mod1Mary CrisNo ratings yet
- Katalog KLINGER Sight GlassDocument8 pagesKatalog KLINGER Sight GlassismailadmfNo ratings yet
- Mechanical Working of MetalsDocument53 pagesMechanical Working of Metalsmurari100% (3)
- Earth Moving Machines-A GlanceDocument27 pagesEarth Moving Machines-A GlanceVinod YbNo ratings yet
- The Method of The Siddhas 5 Walking The Dog PDF FreeDocument25 pagesThe Method of The Siddhas 5 Walking The Dog PDF FreeDesiré Angelica GANo ratings yet
- HyderabadDocument8 pagesHyderabadNaveen KumarNo ratings yet
- Third Semester Form Submitted SuccessfullyDocument1 pageThird Semester Form Submitted SuccessfullyMohit KumarNo ratings yet
- Theory of Magnetic Adjustment PDFDocument8 pagesTheory of Magnetic Adjustment PDFNoli VirgoNo ratings yet
- Köppen Climate Classification PDFDocument21 pagesKöppen Climate Classification PDFJohann S M MendezNo ratings yet
- Inventory ManagementDocument18 pagesInventory ManagementNeha Gupta100% (1)
- Online Smu Natural Science Text BookDocument32 pagesOnline Smu Natural Science Text BookspmajishNo ratings yet
- Report On Bharti Airtel Limited: Institute of Marketing and ManagementDocument26 pagesReport On Bharti Airtel Limited: Institute of Marketing and Managementsimply_cooolNo ratings yet
- LogDocument2 pagesLogAlexander HackerNo ratings yet
- IECEx CML 17.0023X 0Document9 pagesIECEx CML 17.0023X 0KittyNo ratings yet
- C&S Financial AnalysisDocument54 pagesC&S Financial AnalysishemantNo ratings yet
- Yamah F4 Owners ManualDocument70 pagesYamah F4 Owners ManualStil NoxNo ratings yet
- Tad 941 VeDocument2 pagesTad 941 VePdroGsus Abregú TerronesNo ratings yet
- Fimbristylis Littoralis (Lesser Fimbristylis)Document6 pagesFimbristylis Littoralis (Lesser Fimbristylis)MaelstromNo ratings yet
- Pro9500 PCDocument34 pagesPro9500 PCJonssonsNo ratings yet
- Number 3 Compiler Design CourseworkDocument3 pagesNumber 3 Compiler Design Courseworkiriama emmaNo ratings yet
- Z Transform Part 1 PDFDocument16 pagesZ Transform Part 1 PDFAnanth SettyNo ratings yet
- Radiographs in PeriodonticsDocument14 pagesRadiographs in Periodonticsyuanyuan100% (1)
- Application Note CORR-4 PDFDocument15 pagesApplication Note CORR-4 PDFaneesh19inNo ratings yet
- Wakatipu Trails MapDocument2 pagesWakatipu Trails Mapmiller999No ratings yet