You might also like
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- The Immediate Effects of Lumbar Rotational Mobilization On Trunk Control and Gait Parameter in Patients With StrokeDocument7 pagesThe Immediate Effects of Lumbar Rotational Mobilization On Trunk Control and Gait Parameter in Patients With Stroke林良駿No ratings yet
- Jurnal RomDocument8 pagesJurnal RomPutri WulandariNo ratings yet
- 2.robot Assisted ArmDocument6 pages2.robot Assisted Armnataly545426No ratings yet
- 28 - Jpts 2016 190Document6 pages28 - Jpts 2016 190alsyafarinoorNo ratings yet
- 79b6 PDFDocument5 pages79b6 PDFcnsatishNo ratings yet
- 10 1155@2019@1694695Document8 pages10 1155@2019@1694695DATO13No ratings yet
- Effects On Lower Extremity Neuromuscular Control Exercises On Knee PDFDocument7 pagesEffects On Lower Extremity Neuromuscular Control Exercises On Knee PDFEva MartinezNo ratings yet
- DONEDocument7 pagesDONEpashaNo ratings yet
- X Xdonghwan Park, XX X Xji-Hyun Lee, XX X Xtae-Woo Kang, XX and X Xheon-Seock Cynn, XXDocument9 pagesX Xdonghwan Park, XX X Xji-Hyun Lee, XX X Xtae-Woo Kang, XX and X Xheon-Seock Cynn, XXRay HannaNo ratings yet
- Comparison Between Effectiveness of Hand Arm Bimanual Intensive Training and Repetitive Facilitation Exercises On Upper Limb Functions in Post Stroke Hemiparetic PatientsDocument10 pagesComparison Between Effectiveness of Hand Arm Bimanual Intensive Training and Repetitive Facilitation Exercises On Upper Limb Functions in Post Stroke Hemiparetic PatientsEditor IJTSRDNo ratings yet
- Combined Arm Stretch Positioning and Neuromuscular Electrical Stimulation in Patients After Stroke A Random TrialDocument10 pagesCombined Arm Stretch Positioning and Neuromuscular Electrical Stimulation in Patients After Stroke A Random TrialwahyonoNo ratings yet
- Restricion Del TroncoDocument7 pagesRestricion Del TroncoJason SalazarNo ratings yet
- 2 Ijmtst0810098Document6 pages2 Ijmtst0810098Vijay MuniNo ratings yet
- Effectiveness of Gluteus Maximus Strengthening On Gait in Patients With HemiparesisDocument6 pagesEffectiveness of Gluteus Maximus Strengthening On Gait in Patients With HemiparesisMufidah AlhadarNo ratings yet
- 1 s2.0 S1607551X09703614 MainDocument8 pages1 s2.0 S1607551X09703614 MainAchenk BarcelonistaNo ratings yet
- 03IJPHY840Document6 pages03IJPHY840Dzihan NabilahNo ratings yet
- Lex D de Jong, Pieter U Dijkstra, Johan Gerritsen, Alexander CH Geurts and Klaas PostemaDocument12 pagesLex D de Jong, Pieter U Dijkstra, Johan Gerritsen, Alexander CH Geurts and Klaas PostemaAnggelia jopa sariNo ratings yet
- CMJ2009 - 7 (2) E4Document5 pagesCMJ2009 - 7 (2) E4sulis tiyowatiNo ratings yet
- Halbert Sma 1994Document6 pagesHalbert Sma 1994Irsa SevenfoldismNo ratings yet
- Choi Et. Al. (2005) - Exercício IsoladDocument9 pagesChoi Et. Al. (2005) - Exercício IsoladFrancieleNo ratings yet
- 2018 Article 642Document14 pages2018 Article 642Faqih FathurrozanNo ratings yet
- 2009 Ericsson Et Al-2009-Scandinavian Journal of Medicine & Science in SportsDocument10 pages2009 Ericsson Et Al-2009-Scandinavian Journal of Medicine & Science in SportsLuis MiguelNo ratings yet
- This Item Is The Archived Peer-Reviewed Author-Version ofDocument12 pagesThis Item Is The Archived Peer-Reviewed Author-Version ofK scuddsNo ratings yet
- Efficacy of A Hybrid Assistive Limb in Post-Stroke Hemiplegic Patients: A Preliminary ReportDocument6 pagesEfficacy of A Hybrid Assistive Limb in Post-Stroke Hemiplegic Patients: A Preliminary ReportJoão Pedro Lemos MoraisNo ratings yet
- Parent ArticleDocument6 pagesParent ArticleBhagyashree HajareNo ratings yet
- 08IJPHY696Document8 pages08IJPHY696charleskimNo ratings yet
- 01d3c134-0005-450f-9e4e-d814211ee29a (1)Document7 pages01d3c134-0005-450f-9e4e-d814211ee29a (1)Pinekeshi NikithaNo ratings yet
- Jpts 27 2621Document4 pagesJpts 27 2621vvNo ratings yet
- Anusha Article IJIRMFDocument5 pagesAnusha Article IJIRMFAnusha SampathNo ratings yet
- Jurnal Stroke IskemikDocument7 pagesJurnal Stroke IskemikDian NellisaNo ratings yet
- Bobath en Prevenciòn de Subuxacion de Hombro Despues de ECVDocument10 pagesBobath en Prevenciòn de Subuxacion de Hombro Despues de ECVLuisa SánchezNo ratings yet
- Icorr 2005 1501051Document4 pagesIcorr 2005 1501051Amanuel TilayeNo ratings yet
- DS Ahmed A. R. 2011Document6 pagesDS Ahmed A. R. 2011jul yanNo ratings yet
- Hamstring 2Document7 pagesHamstring 2Ardhyan ArdhyanNo ratings yet
- Beda Pir Dan Met Pada FleksibilitasDocument5 pagesBeda Pir Dan Met Pada FleksibilitasPradipta EstuNo ratings yet
- Impact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsDocument4 pagesImpact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsCristian Florin CrasmaruNo ratings yet
- Effectiveness of Maitland vs. Mulligan Mobilization Techniques in (Ingles)Document4 pagesEffectiveness of Maitland vs. Mulligan Mobilization Techniques in (Ingles)mauricio castroNo ratings yet
- Sensors 23 06158Document11 pagesSensors 23 06158thki jiNo ratings yet
- Asj 2020 0146Document6 pagesAsj 2020 0146Mandeep JangraNo ratings yet
- MulliganDocument13 pagesMulliganAgustina AverameNo ratings yet
- Original Original Original Original Article Article Article Article 2010, 4 (1) : 41-46Document6 pagesOriginal Original Original Original Article Article Article Article 2010, 4 (1) : 41-46sulis tiyowatiNo ratings yet
- 1 s2.0 S0966636221001338 MainDocument7 pages1 s2.0 S0966636221001338 MainLiesapriyantiNo ratings yet
- Efficacy of Sot in FemalesDocument7 pagesEfficacy of Sot in FemalesDenise MathreNo ratings yet
- Klooster ManDocument12 pagesKlooster ManAnonymous b2k9ABe7eNo ratings yet
- Task Oriented Improves Strength - Stroke PatientsDocument7 pagesTask Oriented Improves Strength - Stroke PatientsPedro FonsecaNo ratings yet
- Flexibilidade Dos Isquiotibiais em Mulheres Jovens Após TécnicaDocument7 pagesFlexibilidade Dos Isquiotibiais em Mulheres Jovens Após TécnicaAdilson MarquesNo ratings yet
- Faghri 1994Document7 pagesFaghri 1994Leticia PereiraNo ratings yet
- Jurnal Rehab 1Document7 pagesJurnal Rehab 1Sanyuki KhoirunnisaNo ratings yet
- Diafragma Ant Posterior ChainDocument7 pagesDiafragma Ant Posterior ChainJulijus MotiejunasNo ratings yet
- Manual Therapy, Therapeutic Exercise, and Hiptrac For Patients With Hip Osteoarthritis: A Case SeriesDocument12 pagesManual Therapy, Therapeutic Exercise, and Hiptrac For Patients With Hip Osteoarthritis: A Case SeriesdoneitwellNo ratings yet
- Does Sarcopenia Predict Change in Mobility After Hip Fracture? A Multicenter Observational Study With One-Year Follow-UpDocument10 pagesDoes Sarcopenia Predict Change in Mobility After Hip Fracture? A Multicenter Observational Study With One-Year Follow-UpliantariNo ratings yet
- Fatigue in Robotic Vs LapDocument17 pagesFatigue in Robotic Vs LapFlaviu Ionuț FaurNo ratings yet
- Manual Therapy: Original ArticleDocument6 pagesManual Therapy: Original ArticleRyan SetyantoNo ratings yet
- Effects of Scapular Stabilization Exercise Training OnDocument12 pagesEffects of Scapular Stabilization Exercise Training OnNajoua SalomaoNo ratings yet
- HVT With Lumbar Disc HerniationDocument12 pagesHVT With Lumbar Disc HerniationSheena McLennanNo ratings yet
- The Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyDocument5 pagesThe Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- JurnalDocument8 pagesJurnalSelingan SenjaNo ratings yet
- Neurorobotics Presentation 3Document8 pagesNeurorobotics Presentation 3Hamza MinhasNo ratings yet
- Effectiveness of Spencer Muscle Energy Technique On Periarthritis ShoulderDocument5 pagesEffectiveness of Spencer Muscle Energy Technique On Periarthritis Shoulderplaboni banerjeeNo ratings yet
- CIT Training MAL Manual PDFDocument18 pagesCIT Training MAL Manual PDFFilozófus ÖnjelöltNo ratings yet
- Clinimetric Properties of The Motor Activity Log For The Assessment of Arm Use in Hemiparetic PatientsDocument6 pagesClinimetric Properties of The Motor Activity Log For The Assessment of Arm Use in Hemiparetic PatientsMunni KNo ratings yet
- Effect of Task-Oriented Training With and Without Trunk Restraint On Reaching Activity in Adult HemipareticsDocument5 pagesEffect of Task-Oriented Training With and Without Trunk Restraint On Reaching Activity in Adult HemipareticsMunni KNo ratings yet
- Effect of Task-Oriented Training With and Without Trunk Restraint On Reaching Activity in Adult HemipareticsDocument5 pagesEffect of Task-Oriented Training With and Without Trunk Restraint On Reaching Activity in Adult HemipareticsMunni KNo ratings yet
- Clinimetric Properties of The Motor Activity Log For The Assessment of Arm Use in Hemiparetic PatientsDocument6 pagesClinimetric Properties of The Motor Activity Log For The Assessment of Arm Use in Hemiparetic PatientsMunni KNo ratings yet
- MCQ 2Document9 pagesMCQ 2Munni KNo ratings yet
- CIT Training MAL Manual PDFDocument18 pagesCIT Training MAL Manual PDFFilozófus ÖnjelöltNo ratings yet
- 27 PDFDocument7 pages27 PDFMunni KNo ratings yet
- Effectiveness of Modified Constraint-Induced Movement Therapy in Children With Unilateral Spastic Cerebral Palsy: A Randomized Controlled TrialDocument10 pagesEffectiveness of Modified Constraint-Induced Movement Therapy in Children With Unilateral Spastic Cerebral Palsy: A Randomized Controlled TrialMunni KNo ratings yet
- Background:: Kiran Prakash PappalaDocument7 pagesBackground:: Kiran Prakash PappalaMunni KNo ratings yet
- Effect of Task-Oriented Training With and Without Trunk Restraint On Reaching Activity in Adult HemipareticsDocument5 pagesEffect of Task-Oriented Training With and Without Trunk Restraint On Reaching Activity in Adult HemipareticsMunni KNo ratings yet
- Effectiveness of Modified Constraint-Induced Movement Therapy in Children With Unilateral Spastic Cerebral Palsy: A Randomized Controlled TrialDocument10 pagesEffectiveness of Modified Constraint-Induced Movement Therapy in Children With Unilateral Spastic Cerebral Palsy: A Randomized Controlled TrialMunni KNo ratings yet
- Bones and Joints of TrunkDocument56 pagesBones and Joints of Trunkapi-196413370% (1)
- BODYSTART Fitness Tests: Hover - Core StrengthDocument4 pagesBODYSTART Fitness Tests: Hover - Core StrengthCharles Vincent AguilaNo ratings yet
- Rehabilitation: Walking After Total Knee ReplacementDocument10 pagesRehabilitation: Walking After Total Knee ReplacementSandeep DhimanNo ratings yet
- Mobility AidsDocument43 pagesMobility AidsCHAITANYA SAHITHI100% (1)
- Strengthen ShoulderDocument5 pagesStrengthen Shouldernacole78No ratings yet
- Principles of Fixation For Maxillofacial Trauma PatientsDocument69 pagesPrinciples of Fixation For Maxillofacial Trauma PatientsSiyum MathewosNo ratings yet
- Internal RotationDocument15 pagesInternal RotationBrian ChimpmunkNo ratings yet
- Perdarahannya Banyak o Syarat: Catat Waktu Pemasangan - Mengetahui Ischemic TimeDocument6 pagesPerdarahannya Banyak o Syarat: Catat Waktu Pemasangan - Mengetahui Ischemic TimeFebryan Yovi SaputraNo ratings yet
- Arthrology: DR N. ChikumbaDocument50 pagesArthrology: DR N. ChikumbaNatty ChikumbaNo ratings yet
- Medial Collateral Ligament Injuries in Football (1980)Document4 pagesMedial Collateral Ligament Injuries in Football (1980)lite.trawler-0xNo ratings yet
- Act. 4c The Appendicular Skeleton For STUDENTSDocument15 pagesAct. 4c The Appendicular Skeleton For STUDENTSShane SayconNo ratings yet
- Rene Cailliet - Shoulder Pain PDFDocument170 pagesRene Cailliet - Shoulder Pain PDFm alfin alfauziNo ratings yet
- Course Content 1st Year DPT (1st Semester)Document20 pagesCourse Content 1st Year DPT (1st Semester)KhanNo ratings yet
- Ankylosing SpondylitisDocument29 pagesAnkylosing SpondylitisKrisna ajiNo ratings yet
- Pott's DiseaseDocument30 pagesPott's DiseaseBipin SolankiNo ratings yet
- Laporan Bu Tri FEBRUARI Newww YG LAINNAPDocument25 pagesLaporan Bu Tri FEBRUARI Newww YG LAINNAPDita Ayu LestariNo ratings yet
- Post Parturition Back PainDocument35 pagesPost Parturition Back PainARF TYONo ratings yet
- Adhesive CapsulitisDocument23 pagesAdhesive CapsulitisEldar SulejmanovicNo ratings yet
- Adductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionDocument9 pagesAdductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionElaine CspNo ratings yet
- PRI Integ For Pediatrics (Nov 2020) - Complete ManualDocument208 pagesPRI Integ For Pediatrics (Nov 2020) - Complete Manualzhang yangNo ratings yet
- Facial BoneDocument34 pagesFacial BoneIrfanHadiWijayaNo ratings yet
- What Is PNF Stretching and How Should You Use ItDocument12 pagesWhat Is PNF Stretching and How Should You Use Itsardianti dwitirtaNo ratings yet
- Extraocluar Muscle Anatomy Physiology: DR Helen Sisay (MD) MARCH 2013Document124 pagesExtraocluar Muscle Anatomy Physiology: DR Helen Sisay (MD) MARCH 2013Amare GetnetNo ratings yet
- Alain PDF CompressedDocument8 pagesAlain PDF CompressedCleber Anderson SilvestreNo ratings yet
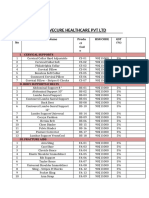
- Drivecure Healthcare PVT LTD: S. No Product Name Produ CT Cod e HSN Code GST (%)Document4 pagesDrivecure Healthcare PVT LTD: S. No Product Name Produ CT Cod e HSN Code GST (%)DRIVECURENo ratings yet
- Kinesio TapingDocument62 pagesKinesio TapingDiah Rahmat100% (1)
- Amputations and Ex ArticulationsDocument24 pagesAmputations and Ex ArticulationsTesmal FernandoNo ratings yet
- Thoracic CageDocument46 pagesThoracic CageEmtnan MuntiNo ratings yet
- Workout BookDocument13 pagesWorkout Bookfordy1usNo ratings yet
- Shoulder and Upper Extremity InjuriesDocument107 pagesShoulder and Upper Extremity InjuriesStaen KisNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)