You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
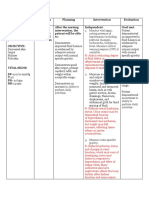
- Medicines That Affect Fluid Balance in The Body: AntacidsDocument2 pagesMedicines That Affect Fluid Balance in The Body: AntacidsSri IriantiNo ratings yet
- Group Project: Gabungan Aqrs Vs Crest Builder HoldingsDocument43 pagesGroup Project: Gabungan Aqrs Vs Crest Builder HoldingsNURUL SYAFIQAH MOHD IDRISNo ratings yet
- Chapter 5-Leadership and MotivationDocument62 pagesChapter 5-Leadership and MotivationAklilu GirmaNo ratings yet
- Government AccountingDocument32 pagesGovernment AccountingLaika Mae D. CariñoNo ratings yet
- Carbapenem Resistance A ReviewDocument28 pagesCarbapenem Resistance A ReviewSri IriantiNo ratings yet
- Sailor Mini MoonDocument9 pagesSailor Mini MoonCarytoNo ratings yet
- 5 Time Management Tips To Work Smarter, Not HarderDocument2 pages5 Time Management Tips To Work Smarter, Not Harderwindell pantinople100% (2)
- Summative Exam 4 Sets Inquiry, Investigation and ImmersionDocument7 pagesSummative Exam 4 Sets Inquiry, Investigation and ImmersionAruel Delim100% (4)
- Fishing in The Roman WorldDocument69 pagesFishing in The Roman Worldmnm06100% (1)
- MEDDEV 2 - 7 - 1 - Rev4 - enDocument65 pagesMEDDEV 2 - 7 - 1 - Rev4 - enSalvatore CannataNo ratings yet
- Church-State Relations, National Identity, and Security in Post-Cold War GreeceDocument31 pagesChurch-State Relations, National Identity, and Security in Post-Cold War GreeceTeo ThemaNo ratings yet
- Koagulasi Intravaskuler Diseminata Pada Kanker: January 2015Document13 pagesKoagulasi Intravaskuler Diseminata Pada Kanker: January 2015Sri IriantiNo ratings yet
- Ahmed 2004Document7 pagesAhmed 2004Sri IriantiNo ratings yet
- Price List DKI 22 Mei 2023Document4 pagesPrice List DKI 22 Mei 2023Usodo UdiNo ratings yet
- Guidotti 2006Document41 pagesGuidotti 2006Sri IriantiNo ratings yet
- Alswaff 2012Document6 pagesAlswaff 2012Sri IriantiNo ratings yet
- NaokoDocument4 pagesNaokoSri IriantiNo ratings yet
- WJH 10 186 PDFDocument32 pagesWJH 10 186 PDFSri IriantiNo ratings yet
- Kar Yo TypingDocument2 pagesKar Yo TypingSri IriantiNo ratings yet
- Chronic Lymphocytic LeukemiaDocument8 pagesChronic Lymphocytic LeukemiaSri IriantiNo ratings yet
- Karyotyping PDFDocument2 pagesKaryotyping PDFSri IriantiNo ratings yet
- Anti-Mu Llerian Hormone: Ovarian Reserve Testing and Its Potential Clinical ImplicationsDocument14 pagesAnti-Mu Llerian Hormone: Ovarian Reserve Testing and Its Potential Clinical ImplicationsSri IriantiNo ratings yet
- Worksheet ExerciseDocument2 pagesWorksheet Exerciseshaan shekharNo ratings yet
- SMS2008 DX33Document4 pagesSMS2008 DX33Imam DinNo ratings yet
- Q2 - Melc 10 - 11Document56 pagesQ2 - Melc 10 - 11Geraldine MatiasNo ratings yet
- Tendor of EsiDocument7 pagesTendor of EsiRaj KumarNo ratings yet
- Cloudworx Microstation UsDocument2 pagesCloudworx Microstation Usguru4lifegmailcomNo ratings yet
- Dealroom Fintech 2024 Europe US Report - ABN Amro - Motive Ventures - 26032024Document32 pagesDealroom Fintech 2024 Europe US Report - ABN Amro - Motive Ventures - 26032024gemelli02No ratings yet
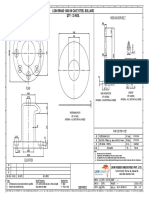
- M56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NosDocument1 pageM56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NossanaNo ratings yet
- SustainabilityDocument856 pagesSustainabilityErnest AcarNo ratings yet
- Water Coolers CatalogDocument34 pagesWater Coolers CatalogSinergroup Water Filters Water Purifiers Water SoftenersNo ratings yet
- Math 237 p02 - Inexact de and Integrating Factors - 3172023-1Document18 pagesMath 237 p02 - Inexact de and Integrating Factors - 3172023-1Shunsui SyNo ratings yet
- Orthogonal CirclesDocument7 pagesOrthogonal CirclesErebus OneirosNo ratings yet
- Peritonitis NCPDocument3 pagesPeritonitis NCPANNA V. LARITANo ratings yet
- Economics of Animal-Rearing: Dairy and Livestock ProductionDocument6 pagesEconomics of Animal-Rearing: Dairy and Livestock ProductionRaghav BawaNo ratings yet
- Some Observable Classroom BehaviorDocument33 pagesSome Observable Classroom BehaviorMaNerissa Peñamora SanchezNo ratings yet
- Catalog Sydor 2022Document21 pagesCatalog Sydor 2022Chonk LeeNo ratings yet
- A Charge of A Light BrigadeDocument26 pagesA Charge of A Light Brigadeniluka welagedaraNo ratings yet
- Assignment 1-Vignesh Prasad VDocument14 pagesAssignment 1-Vignesh Prasad VVignesh Veera Prasad100% (1)
- Speech As A Signal of Social IdentityDocument25 pagesSpeech As A Signal of Social IdentityAysha BahaaNo ratings yet
- Unit - IDocument86 pagesUnit - IZeeshanMirzaNo ratings yet
- Zoology 100 Notes 1Document8 pagesZoology 100 Notes 1Bethany Jane Ravelo IsidroNo ratings yet
- Physics MCQs For Class 12 With Answers Chapter 10Document12 pagesPhysics MCQs For Class 12 With Answers Chapter 10Akshith ReddyNo ratings yet