You might also like
- Coordinate Geometry Solutions Class 10 SSC: Exercise 7.1Document42 pagesCoordinate Geometry Solutions Class 10 SSC: Exercise 7.1Rajendra PilludaNo ratings yet
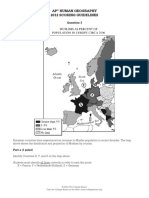
- AP HuG Chapter 7 2014Document5 pagesAP HuG Chapter 7 2014Rajendra PilludaNo ratings yet
- ch.9 Test BankDocument32 pagesch.9 Test BankRajendra PilludaNo ratings yet
- Ap14 FRQ Human GeographyDocument3 pagesAp14 FRQ Human Geographyapi-314084641No ratings yet
- About Microfinance: Microfinance - Also Called Microcredit, Microlending, or MicroloansDocument2 pagesAbout Microfinance: Microfinance - Also Called Microcredit, Microlending, or MicroloansRajendra PilludaNo ratings yet
- Drilldown Diagnostics ScriptDocument1 pageDrilldown Diagnostics ScriptRajendra PilludaNo ratings yet
- About Microfinance: Microfinance - Also Called Microcredit, Microlending, or MicroloansDocument2 pagesAbout Microfinance: Microfinance - Also Called Microcredit, Microlending, or MicroloansRajendra PilludaNo ratings yet
- AP Human Geography FRQs on Urbanization, Models and TransportationDocument6 pagesAP Human Geography FRQs on Urbanization, Models and TransportationRajendra PilludaNo ratings yet
- Possible Frqs For Chapter 10 and Chapter 11 ExamDocument3 pagesPossible Frqs For Chapter 10 and Chapter 11 ExamRajendra PilludaNo ratings yet
- About Microfinance: Microfinance - Also Called Microcredit, Microlending, or MicroloansDocument2 pagesAbout Microfinance: Microfinance - Also Called Microcredit, Microlending, or MicroloansRajendra PilludaNo ratings yet
- CH 9-10 Outline and Test ReviewDocument12 pagesCH 9-10 Outline and Test ReviewRajendra PilludaNo ratings yet
- ch.9 Test BankDocument32 pagesch.9 Test BankRajendra PilludaNo ratings yet
- How To Create A Service Request PDFDocument6 pagesHow To Create A Service Request PDFRajendra PilludaNo ratings yet
- Received Amount Not EqualDocument2 pagesReceived Amount Not EqualRajendra PilludaNo ratings yet
- AP Human Geography 2012 Scoring Guidelines: Part A (1 Point)Document11 pagesAP Human Geography 2012 Scoring Guidelines: Part A (1 Point)Rajendra PilludaNo ratings yet
- Vi Cheat SheetDocument2 pagesVi Cheat Sheetvaaz205No ratings yet
- CH 07Document48 pagesCH 07Rajendra PilludaNo ratings yet
- P2P Life Cycle PDFDocument72 pagesP2P Life Cycle PDFRajendra PilludaNo ratings yet
- CH 07Document48 pagesCH 07Rajendra PilludaNo ratings yet
- AP Human Geography Chapter 6 NotesDocument20 pagesAP Human Geography Chapter 6 NotesSeth Adler93% (74)
- APHG CHPT 4 PDFDocument16 pagesAPHG CHPT 4 PDFRajendra PilludaNo ratings yet
- Ap Human Geography Course Outline: I. Geography: Its Nature and Perspectives (5-10% of The AP Exam)Document7 pagesAp Human Geography Course Outline: I. Geography: Its Nature and Perspectives (5-10% of The AP Exam)Rajendra PilludaNo ratings yet
- Human Geography Chapter 04 Practice QuestionsDocument3 pagesHuman Geography Chapter 04 Practice QuestionsRajendra PilludaNo ratings yet
- CSSSamantha GermanSLA201406Document117 pagesCSSSamantha GermanSLA201406rpillz100% (1)
- GL-Inventory ReconciliationDocument12 pagesGL-Inventory ReconciliationRajendra PilludaNo ratings yet
- APHG CHPT 4 PDFDocument16 pagesAPHG CHPT 4 PDFRajendra PilludaNo ratings yet
- Scripted ISO 20022 PPT Long Version v55Document48 pagesScripted ISO 20022 PPT Long Version v55fsdafNo ratings yet
- MJE ManualDocument32 pagesMJE ManualSonaliNo ratings yet
- Web ADI User Guide PDFDocument26 pagesWeb ADI User Guide PDFRajendra PilludaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Marijuana Grow Basics - Jorge CervantesDocument389 pagesMarijuana Grow Basics - Jorge CervantesHugo Herrera100% (1)
- HU675FE ManualDocument44 pagesHU675FE ManualMar VeroNo ratings yet
- Main Hoon Na - WikipediaDocument8 pagesMain Hoon Na - WikipediaHusain ChandNo ratings yet
- Delhi Public School: Class: XI Subject: Assignment No. 3Document1 pageDelhi Public School: Class: XI Subject: Assignment No. 3Aman Kumar BhagatNo ratings yet
- Febrile SeizureDocument3 pagesFebrile SeizureClyxille GiradoNo ratings yet
- Plant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirDocument20 pagesPlant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirSharad KokateNo ratings yet
- JR Hydraulic Eng. Waterways Bed Protection Incomat BelfastDocument2 pagesJR Hydraulic Eng. Waterways Bed Protection Incomat Belfastpablopadawan1No ratings yet
- CH - 3Document3 pagesCH - 3Phantom GamingNo ratings yet
- Strain Gauge Sensor PDFDocument12 pagesStrain Gauge Sensor PDFMario Eduardo Santos MartinsNo ratings yet
- EG-45-105 Material Information Sheet (Textura) V2Document4 pagesEG-45-105 Material Information Sheet (Textura) V2GPRNo ratings yet
- Medical filter performance specificationsDocument1 pageMedical filter performance specificationsPT.Intidaya Dinamika SejatiNo ratings yet
- Mark Dean GR6211 Fall 2018 Columbia University: - Choice Theory'Document5 pagesMark Dean GR6211 Fall 2018 Columbia University: - Choice Theory'bhaskkarNo ratings yet
- BỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔDocument5 pagesBỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔPhạm Thu NgaNo ratings yet
- Arduino Nano based K1EL Winkeyer compatible CW contest keyerDocument35 pagesArduino Nano based K1EL Winkeyer compatible CW contest keyerSreejith SreedharanNo ratings yet
- The Graduation Commencement Speech You Will Never HearDocument4 pagesThe Graduation Commencement Speech You Will Never HearBernie Lutchman Jr.No ratings yet
- Mechanical Questions & AnswersDocument161 pagesMechanical Questions & AnswersTobaNo ratings yet
- Manual Bombas CHWDocument16 pagesManual Bombas CHWFred GarciaNo ratings yet
- Module 4-Answer KeyDocument100 pagesModule 4-Answer KeyAna Marie Suganob82% (22)
- Center of Gravity and Shear Center of Thin-Walled Open-Section Composite BeamsDocument6 pagesCenter of Gravity and Shear Center of Thin-Walled Open-Section Composite Beamsredz00100% (1)
- Nature and Scope of Marketing Marketing ManagementDocument51 pagesNature and Scope of Marketing Marketing ManagementFeker H. MariamNo ratings yet
- ASD Manual and AISC LRFD Manual For Bolt Diameters Up To 6 Inches (150Document1 pageASD Manual and AISC LRFD Manual For Bolt Diameters Up To 6 Inches (150rabzihNo ratings yet
- E Learning: A Student Guide To MoodleDocument16 pagesE Learning: A Student Guide To MoodleHaytham Abdulla SalmanNo ratings yet
- Tupperware India's Perception StudyDocument10 pagesTupperware India's Perception StudyAnmol RahangdaleNo ratings yet
- BMXNRPDocument60 pagesBMXNRPSivaprasad KcNo ratings yet
- Credit Risk Management Practice in Private Banks Case Study Bank of AbyssiniaDocument85 pagesCredit Risk Management Practice in Private Banks Case Study Bank of AbyssiniaamogneNo ratings yet
- Done by Akansha Bharti Harshitha K.N. Ishika Sunil Rajput Rashmi NaikDocument12 pagesDone by Akansha Bharti Harshitha K.N. Ishika Sunil Rajput Rashmi NaikRamya BalanNo ratings yet
- IT SyllabusDocument3 pagesIT SyllabusNeilKumarNo ratings yet
- Dell EMC VPLEX For All-FlashDocument4 pagesDell EMC VPLEX For All-Flashghazal AshouriNo ratings yet
- EcohistDocument3 pagesEcohistRkmv EconNo ratings yet
- PGP TutorialDocument21 pagesPGP TutorialSabri AllaniNo ratings yet