You might also like
- Grassroots to Government: Creating joined-up working in AustraliaFrom EverandGrassroots to Government: Creating joined-up working in AustraliaNo ratings yet
- Decentralization and Health System Performance - A Focused Review of Dimensions, Difficulties, and Derivatives in IndiaDocument33 pagesDecentralization and Health System Performance - A Focused Review of Dimensions, Difficulties, and Derivatives in IndiaAbdirahman Hassan MohamedNo ratings yet
- Jurnal Inter 3Document7 pagesJurnal Inter 3Muhammad FadhliNo ratings yet
- Implementation of Human Development Policy in Health Sector in Decentralization PerspectiveDocument6 pagesImplementation of Human Development Policy in Health Sector in Decentralization PerspectiveIJPHSNo ratings yet
- Policy Impact of Regional Expansionconcerning Social and Economic in West Seram District, Maluku ProvinceDocument7 pagesPolicy Impact of Regional Expansionconcerning Social and Economic in West Seram District, Maluku ProvinceCukup AnggiatNo ratings yet
- Analisa Pengaruh Kebijakan Desentralisasi Fiskal Terhadap Outcomes Bidang Kesehatan Di Kabupaten/Kota Propinsi Sumatera BaratDocument13 pagesAnalisa Pengaruh Kebijakan Desentralisasi Fiskal Terhadap Outcomes Bidang Kesehatan Di Kabupaten/Kota Propinsi Sumatera BaratNengLukmanNo ratings yet
- Published Researches in The Year 2009Document17 pagesPublished Researches in The Year 2009hsrimediaNo ratings yet
- Examining The Influence of Regulatory Governance On Service Quality in Bwera District Hospital, Kasese District, Western Uganda.Document15 pagesExamining The Influence of Regulatory Governance On Service Quality in Bwera District Hospital, Kasese District, Western Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Social Welfare Policies and Administration in IndiaDocument64 pagesSocial Welfare Policies and Administration in IndiaMd ShamiNo ratings yet
- 13-24 IJHSS November IssueDocument12 pages13-24 IJHSS November IssueBarrouzNo ratings yet
- A Proposal For Public Health Information System-BaDocument14 pagesA Proposal For Public Health Information System-Baruuncadey89No ratings yet
- Final Proposal 610Document13 pagesFinal Proposal 610Sudip LamsalNo ratings yet
- Concept KUDocument9 pagesConcept KUBENARD LUKIBIANo ratings yet
- Indonesia's Decentralization Policy:: Initial Experiences and Emerging ProblemsDocument31 pagesIndonesia's Decentralization Policy:: Initial Experiences and Emerging ProblemsibborNo ratings yet
- s12961 018 0402 1 PDFDocument16 pagess12961 018 0402 1 PDFClarrisse Joy LolaNo ratings yet
- Transparansi Anggaran Sektor Kesehatan DaerahDocument14 pagesTransparansi Anggaran Sektor Kesehatan DaerahMohammad IrwanNo ratings yet
- Statecraft and Public Policy MPP-1001: Health Policy of PakistanDocument22 pagesStatecraft and Public Policy MPP-1001: Health Policy of Pakistansaad aliNo ratings yet
- Good Governance and Social AuditDocument6 pagesGood Governance and Social AuditDipu SinghNo ratings yet
- Decentralization and Health System Performance - A Focused Review of Dimensions, Difficulties, and Derivatives in IndiaDocument14 pagesDecentralization and Health System Performance - A Focused Review of Dimensions, Difficulties, and Derivatives in IndiaTriana Amaliah JayantiNo ratings yet
- Health Seeking BehaviourDocument27 pagesHealth Seeking BehaviourRommel IrabagonNo ratings yet
- Jurnal Nomor 17Document18 pagesJurnal Nomor 17Agusniko SinagaNo ratings yet
- Pure Public Administration (3)Document30 pagesPure Public Administration (3)Zainab Tariq AliNo ratings yet
- Human Resources For HealthDocument16 pagesHuman Resources For HealthpfheywoodNo ratings yet
- Decentralisation in Indonesia: The Impact On Local Health ProgramsDocument10 pagesDecentralisation in Indonesia: The Impact On Local Health ProgramsMoken ClNo ratings yet
- DECISION-MAKING PROCESSES FOR EFFECTIVE HEALTH POLICYDocument12 pagesDECISION-MAKING PROCESSES FOR EFFECTIVE HEALTH POLICYjazzskyblueNo ratings yet
- Analysis of Integrated Health Referral Systems in The Era of Regional Autonomy in West SulawesiDocument7 pagesAnalysis of Integrated Health Referral Systems in The Era of Regional Autonomy in West SulawesiHusny MubarakNo ratings yet
- Kode: ASP Dampak Desentralisasi Fiskal Terhadap Outcomes Bidang Kesehatan: Studi Empiris Di Kabupaten/Kota Propinsi Sumatera BaratDocument29 pagesKode: ASP Dampak Desentralisasi Fiskal Terhadap Outcomes Bidang Kesehatan: Studi Empiris Di Kabupaten/Kota Propinsi Sumatera Baratpriandhita asmoroNo ratings yet
- Public Policy Coursework EditedDocument7 pagesPublic Policy Coursework EditedVivian NabulyaNo ratings yet
- Health Decentralization and Its Effects in PhilippinesDocument19 pagesHealth Decentralization and Its Effects in Philippinesshivrajsinghnegi100% (5)
- Policy Research and Governance DR FerrerDocument11 pagesPolicy Research and Governance DR FerrerRia Tiglao FortugalizaNo ratings yet
- Public Service Reform in EthiopiaDocument11 pagesPublic Service Reform in EthiopiaWayyeessaa MargaaNo ratings yet
- Ros and TFDocument3 pagesRos and TFゝ NicoleNo ratings yet
- Bureaucracy Reforms of Public Service (Case Study of Governance Structuring of Passport Issuance System at Class I Makassar Immigration Office)Document10 pagesBureaucracy Reforms of Public Service (Case Study of Governance Structuring of Passport Issuance System at Class I Makassar Immigration Office)Andi EMil MattotorangNo ratings yet
- Health RefomsDocument11 pagesHealth RefomsDr. Muhammad Zaman ZahidNo ratings yet
- Understanding the Functions of an OrganizationDocument61 pagesUnderstanding the Functions of an OrganizationTwinkle VlogsNo ratings yet
- Public Health and Project Management: Do Projects Deliver?Document11 pagesPublic Health and Project Management: Do Projects Deliver?Ali AzanNo ratings yet
- Managing Financial Resources in Health and Social CareDocument15 pagesManaging Financial Resources in Health and Social Caresusikaran1981No ratings yet
- Policy EvaluationDocument3 pagesPolicy Evaluation8910 Areej100% (1)
- Measurement of Community Empowerment in Three Community Programs in Rapla (Estonia)Document19 pagesMeasurement of Community Empowerment in Three Community Programs in Rapla (Estonia)Lin AungNo ratings yet
- Jurnal BPJSDocument7 pagesJurnal BPJSSyafiraaNo ratings yet
- Public Policy Formulation in NigeriaDocument6 pagesPublic Policy Formulation in NigeriaLal Bux SoomroNo ratings yet
- The Devolution of The Philippine Health SystemDocument27 pagesThe Devolution of The Philippine Health SystemKizito Lubano100% (1)
- Corresponding Author's Email: Jaimefonseca@i: Purpose: Design/Methodology/ApproachDocument14 pagesCorresponding Author's Email: Jaimefonseca@i: Purpose: Design/Methodology/ApproachabibNo ratings yet
- Joranal 1Document5 pagesJoranal 1hsrimediaNo ratings yet
- Kajian Pengaruh Kebijakan Desentralisasi Pada Peningkatan Kesejahteraan Masyarakat (Studi Kasus: Kabupaten/Kota Di Provinsi Jawa Barat)Document24 pagesKajian Pengaruh Kebijakan Desentralisasi Pada Peningkatan Kesejahteraan Masyarakat (Studi Kasus: Kabupaten/Kota Di Provinsi Jawa Barat)JedhungNo ratings yet
- Health-Seeking Behaviour Studies: A Literature Review of Study Design and Methods With A Focus On Cambodia (WP7)Document17 pagesHealth-Seeking Behaviour Studies: A Literature Review of Study Design and Methods With A Focus On Cambodia (WP7)Nossal Institute for Global HealthNo ratings yet
- Competency For Public Health Policy Analysis A Case Study of PakistanDocument5 pagesCompetency For Public Health Policy Analysis A Case Study of PakistanImaanNo ratings yet
- Public Health Care ManagementDocument33 pagesPublic Health Care Managementalexandercecilia67No ratings yet
- Healthcare Financing Infrastructure PaperDocument25 pagesHealthcare Financing Infrastructure Papersri_cbmNo ratings yet
- The Effect of Behavior Change Communication Training On The Performance of Health Promotion Officers in SamarindaDocument9 pagesThe Effect of Behavior Change Communication Training On The Performance of Health Promotion Officers in SamarindaCarissa AramitaNo ratings yet
- Introduction to Public AdministrationDocument4 pagesIntroduction to Public AdministrationnathanharyehrinNo ratings yet
- Jkap English VersionDocument17 pagesJkap English VersionJoko SubagyoNo ratings yet
- E GovernanceDocument19 pagesE GovernanceZihan AbdullahNo ratings yet
- Innovation Study in Improving The Quality of Planning and Budgeting GovernanceDocument9 pagesInnovation Study in Improving The Quality of Planning and Budgeting Governancehilzone_No ratings yet
- Discussion 1Document3 pagesDiscussion 1chisomoNo ratings yet
- Usaid TZ Hss Strategy Sept 30 FinalDocument25 pagesUsaid TZ Hss Strategy Sept 30 FinalEugen R. MwamafupaNo ratings yet
- Effects of Health Decentralization, Financing and Governance in MexicoDocument9 pagesEffects of Health Decentralization, Financing and Governance in Mexicoeris31No ratings yet
- Jurnal Ekonomi Dan Bisnis, Vol. 6 No. 1 Februari 2017 IssnDocument17 pagesJurnal Ekonomi Dan Bisnis, Vol. 6 No. 1 Februari 2017 IssnEni NuraeniNo ratings yet
- Strategic MeseDocument8 pagesStrategic MeseShemu PlcNo ratings yet
- Health Policy and Systems Research Priority SettingDocument10 pagesHealth Policy and Systems Research Priority SettingMohd ImtiazNo ratings yet
- Mercado Libre Press Release 2Q21Document12 pagesMercado Libre Press Release 2Q21BAE NegociosNo ratings yet
- Multi State Resale CertDocument1 pageMulti State Resale CertJavier ReyesNo ratings yet
- Impact of Globalization On PakistanDocument17 pagesImpact of Globalization On PakistanEngr Majid Ali Baig85% (48)
- Vanderbilt Journal of Entertainment Law & Practice. Volume 2, Number 1. Winter, 2000.Document133 pagesVanderbilt Journal of Entertainment Law & Practice. Volume 2, Number 1. Winter, 2000.Steven_Lopez123No ratings yet
- Bill 2Document1 pageBill 2Divya ThomasNo ratings yet
- Absli 3140206 PDFDocument2 pagesAbsli 3140206 PDFSakthivelNo ratings yet
- Morpheus Proposal PoLL 2Document12 pagesMorpheus Proposal PoLL 2Papers of the Libertarian LeftNo ratings yet
- PWC QaDocument14 pagesPWC QaClyde RamosNo ratings yet
- Phil Hawk Vs Vivian Tan Lee DigestDocument2 pagesPhil Hawk Vs Vivian Tan Lee Digestfina_ong62590% (1)
- Governtment AccountingDocument2 pagesGoverntment Accountingjessica amorosoNo ratings yet
- Chapter 3 MCQs On DepreciationDocument14 pagesChapter 3 MCQs On DepreciationGrace StylesNo ratings yet
- Local Government AdministrationDocument56 pagesLocal Government AdministrationAnirtsNo ratings yet
- NoidaDocument23 pagesNoidaAmmar Tambawala100% (1)
- City Corporation Tax RulesDocument13 pagesCity Corporation Tax RulesMuktar Hossain Chowdhury100% (1)
- The Circular Flow of Economic ActivityDocument8 pagesThe Circular Flow of Economic ActivityShrahi Singh KaranwalNo ratings yet
- GST & BAS Detailed HandbookDocument60 pagesGST & BAS Detailed Handbooktestnation100% (1)
- Caltex Phils vs COA ruling on offsetting OPSF collectionsDocument2 pagesCaltex Phils vs COA ruling on offsetting OPSF collectionszahreenamolinaNo ratings yet
- 1 - 2019 - Fundamentals of Taxation An Introduction To Tax Policy Tax Law and Tax AdministrationDocument197 pages1 - 2019 - Fundamentals of Taxation An Introduction To Tax Policy Tax Law and Tax AdministrationSeydina-Ousmane Dramé100% (1)
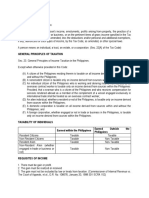
- TAXATION OF INDIVIDUAL INCOMEDocument3 pagesTAXATION OF INDIVIDUAL INCOMESaya PascualNo ratings yet
- Tax Assessment ManualDocument294 pagesTax Assessment ManualPrudvi RajNo ratings yet
- 10 Steps To Making A MillionDocument10 pages10 Steps To Making A Millionadeng96No ratings yet
- Recivable Management Bba 3rdDocument54 pagesRecivable Management Bba 3rdMuzameelAshrafNo ratings yet
- Tax Law Guide to Indian Income TaxDocument133 pagesTax Law Guide to Indian Income TaxTahaNo ratings yet
- Passing The Plate - Smith and EmersonDocument283 pagesPassing The Plate - Smith and EmersonIsmael Mendez ReyesNo ratings yet
- Tutorial 1Document7 pagesTutorial 1Shan JeefNo ratings yet
- Basco vs. PAGCOR (G.R. No. 91649) - Digest FactsDocument18 pagesBasco vs. PAGCOR (G.R. No. 91649) - Digest FactsApril CelestinoNo ratings yet
- 2019 Sunshine Law Manual Appendix ADocument33 pages2019 Sunshine Law Manual Appendix Ajohn shriverNo ratings yet
- Thane Municipal Corporation, ThaneDocument25 pagesThane Municipal Corporation, ThaneAshiwn PanchalNo ratings yet
- Wind Farm Project Analysis and Site AssessmentDocument29 pagesWind Farm Project Analysis and Site AssessmentayobamiNo ratings yet
- LU1 - Value-Added TaxDocument24 pagesLU1 - Value-Added Taxmandisanomzamo72No ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- The Five Dysfunctions of a Team SummaryFrom EverandThe Five Dysfunctions of a Team SummaryRating: 4.5 out of 5 stars4.5/5 (58)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Scaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0From EverandScaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0Rating: 5 out of 5 stars5/5 (1)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (5)
- Getting Along: How to Work with Anyone (Even Difficult People)From EverandGetting Along: How to Work with Anyone (Even Difficult People)Rating: 4.5 out of 5 stars4.5/5 (18)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- The 5 Languages of Appreciation in the Workplace: Empowering Organizations by Encouraging PeopleFrom EverandThe 5 Languages of Appreciation in the Workplace: Empowering Organizations by Encouraging PeopleRating: 4.5 out of 5 stars4.5/5 (46)
- 50 Top Tools for Coaching, 3rd Edition: A Complete Toolkit for Developing and Empowering PeopleFrom Everand50 Top Tools for Coaching, 3rd Edition: A Complete Toolkit for Developing and Empowering PeopleRating: 4.5 out of 5 stars4.5/5 (4)
- The Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceFrom EverandThe Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceRating: 5 out of 5 stars5/5 (22)
- Powerful Phrases for Dealing with Difficult People: Over 325 Ready-to-Use Words and Phrases for Working with Challenging PersonalitiesFrom EverandPowerful Phrases for Dealing with Difficult People: Over 325 Ready-to-Use Words and Phrases for Working with Challenging PersonalitiesRating: 4 out of 5 stars4/5 (14)
- Developing Coaching Skills: A Concise IntroductionFrom EverandDeveloping Coaching Skills: A Concise IntroductionRating: 4.5 out of 5 stars4.5/5 (5)
- The New Executive Assistant : Exceptional Executive Office ManagementFrom EverandThe New Executive Assistant : Exceptional Executive Office ManagementNo ratings yet
- Strength-Based Leadership Coaching in Organizations: An Evidence-Based Guide to Positive Leadership DevelopmentFrom EverandStrength-Based Leadership Coaching in Organizations: An Evidence-Based Guide to Positive Leadership DevelopmentRating: 4 out of 5 stars4/5 (1)
- Irresistible: The Seven Secrets of the World's Most Enduring, Employee-Focused OrganizationsFrom EverandIrresistible: The Seven Secrets of the World's Most Enduring, Employee-Focused OrganizationsRating: 5 out of 5 stars5/5 (3)
- The Art of Active Listening: How People at Work Feel Heard, Valued, and UnderstoodFrom EverandThe Art of Active Listening: How People at Work Feel Heard, Valued, and UnderstoodRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: Who Moved My Cheese?: An A-Mazing Way to Deal with Change in Your Work and in Your Life by Spencer Johnson M.D. and Kenneth Blanchard: Key Takeaways, Summary & AnalysisFrom EverandSummary: Who Moved My Cheese?: An A-Mazing Way to Deal with Change in Your Work and in Your Life by Spencer Johnson M.D. and Kenneth Blanchard: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (3)
- DEI Deconstructed: Your No-Nonsense Guide to Doing the Work and Doing It RightFrom EverandDEI Deconstructed: Your No-Nonsense Guide to Doing the Work and Doing It RightRating: 5 out of 5 stars5/5 (8)
- The Way of the Shepherd: Seven Secrets to Managing Productive PeopleFrom EverandThe Way of the Shepherd: Seven Secrets to Managing Productive PeopleRating: 5 out of 5 stars5/5 (112)
- Leadership Coaching, 2nd Edition: Working with Leaders to Develop Elite PerformanceFrom EverandLeadership Coaching, 2nd Edition: Working with Leaders to Develop Elite PerformanceRating: 4.5 out of 5 stars4.5/5 (4)
- Radical Focus SECOND EDITION: Achieving Your Goals with Objectives and Key ResultsFrom EverandRadical Focus SECOND EDITION: Achieving Your Goals with Objectives and Key ResultsRating: 4.5 out of 5 stars4.5/5 (2)
- The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and GrowthFrom EverandThe Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and GrowthRating: 4.5 out of 5 stars4.5/5 (101)
- Crucial Conversations: Tools for Talking When Stakes are High, Third EditionFrom EverandCrucial Conversations: Tools for Talking When Stakes are High, Third EditionRating: 4 out of 5 stars4/5 (4)
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- The SHRM Essential Guide to Talent Management: A Handbook for HR Professionals, Managers, Businesses, and OrganizationsFrom EverandThe SHRM Essential Guide to Talent Management: A Handbook for HR Professionals, Managers, Businesses, and OrganizationsRating: 5 out of 5 stars5/5 (1)
- Crucial Conversations Tools for Talking When Stakes Are High, Second EditionFrom EverandCrucial Conversations Tools for Talking When Stakes Are High, Second EditionRating: 4 out of 5 stars4/5 (432)