You might also like
- HR Process Improvements Needed at Kelso ToyDocument13 pagesHR Process Improvements Needed at Kelso ToyJay Mendoza100% (1)
- Case StudyDocument10 pagesCase Studygeetukumari100% (1)
- Theoretical FrameworkDocument7 pagesTheoretical FrameworkArianne June AbarquezNo ratings yet
- Prulife Vs CirDocument12 pagesPrulife Vs CirERWINLAV2000No ratings yet
- Sample Research ProposalDocument14 pagesSample Research ProposalTafadzwa James ZibakoNo ratings yet
- Competitive Profile Matrix (CPM) SampleDocument2 pagesCompetitive Profile Matrix (CPM) SampleApril DeeNo ratings yet
- A Silent Initiative Case Analysis - GRP 5Document29 pagesA Silent Initiative Case Analysis - GRP 5Cyrelle PerezNo ratings yet
- Critique Paper BA211 12 NN HRM - DacumosDocument2 pagesCritique Paper BA211 12 NN HRM - DacumosCherBear A. DacumosNo ratings yet
- Children's Hospital Patient Safety InitiativeDocument5 pagesChildren's Hospital Patient Safety InitiativeSmile MaNo ratings yet
- Net Present ValueDocument8 pagesNet Present ValueDagnachew Amare DagnachewNo ratings yet
- Unit Five Case QuestionsDocument7 pagesUnit Five Case Questionsapi-341637116No ratings yet
- 6 Holly Fashion Case StudyDocument3 pages6 Holly Fashion Case StudyCaramalau Mirela-Georgiana0% (1)
- SPSS Linear Regression GuideDocument7 pagesSPSS Linear Regression Guidemesay83No ratings yet
- Group 6 - Case 2 - UnionDocument21 pagesGroup 6 - Case 2 - UnionKristofferson AustriaNo ratings yet
- State University Board of Regents Conflict of InterestDocument1 pageState University Board of Regents Conflict of Interestdivina lagaNo ratings yet
- Operations and Production Management: MSC512M Enrique J. MartinezDocument28 pagesOperations and Production Management: MSC512M Enrique J. MartinezDu Baladad Andrew MichaelNo ratings yet
- Ethical Behaviour in Business PDFDocument2 pagesEthical Behaviour in Business PDFChanceNo ratings yet
- Eduardo Cuano Case IncidentDocument10 pagesEduardo Cuano Case IncidentAllen Lemence100% (1)
- Public Sector EthicsDocument15 pagesPublic Sector EthicsJones Lyndon Crumb DamoNo ratings yet
- GROUP 3 - Europe BookDocument8 pagesGROUP 3 - Europe BookIrish June TayagNo ratings yet
- Employee Turnover in Hospitality IndustryDocument31 pagesEmployee Turnover in Hospitality IndustryJuna BeqiriNo ratings yet
- Revenue Regulations No. 3-98 - Fringe Benefit TaxDocument14 pagesRevenue Regulations No. 3-98 - Fringe Benefit TaxRaiza Radoc100% (1)
- Impact of Employee Turnover in Ssme ConstructionsDocument9 pagesImpact of Employee Turnover in Ssme ConstructionsPinyapatch Fern ChaiyasirisilpNo ratings yet
- Clinical Governance: The Challenges of Implementation in IranDocument10 pagesClinical Governance: The Challenges of Implementation in Iransunny100% (1)
- Individual Assignment - Critique Paper HornsteinDocument6 pagesIndividual Assignment - Critique Paper HornsteinAnkita T. MooreNo ratings yet
- De La Salle University Medical Center (Dlsumc) : Hospital AdministrationDocument1 pageDe La Salle University Medical Center (Dlsumc) : Hospital AdministrationFerl ElardoNo ratings yet
- Derequito Eba201 MidtermsDocument6 pagesDerequito Eba201 MidtermsElvz Derequito0% (1)
- Importance of Competitive AdvantageDocument3 pagesImportance of Competitive AdvantageMihai JuncuNo ratings yet
- PEARSON FORMAT For STRAMA PAPERDocument15 pagesPEARSON FORMAT For STRAMA PAPERmarkanthony08No ratings yet
- Accountancy Service Requirements of Micro, Small, and Medium Enterprises in The PhilippinesDocument10 pagesAccountancy Service Requirements of Micro, Small, and Medium Enterprises in The PhilippinesJEROME ORILLOSANo ratings yet
- DOH - Philippine National Environmental Health Action Plan (NEHAP) 2010-2013Document65 pagesDOH - Philippine National Environmental Health Action Plan (NEHAP) 2010-2013Jayme Hora AbrinaNo ratings yet
- Role of Internal Auditors in Promoting Good GovernanceDocument5 pagesRole of Internal Auditors in Promoting Good GovernanceDiptoDCastleNo ratings yet
- Materials & MethodsDocument3 pagesMaterials & MethodsJohnpatrick DejesusNo ratings yet
- 1a Table of ContentDocument38 pages1a Table of Contentlunaazul75No ratings yet
- Socially Responsible MarketingDocument37 pagesSocially Responsible MarketingRahela FarooqiNo ratings yet
- The Impact of Employee Turnover On Organizational PerformanceDocument13 pagesThe Impact of Employee Turnover On Organizational PerformanceHarish DekaNo ratings yet
- Covid-19 Impact on Tourism in San Juan VillageDocument74 pagesCovid-19 Impact on Tourism in San Juan VillageFathrizia PanizaNo ratings yet
- Chingozho Takawira DissertationDocument92 pagesChingozho Takawira DissertationTrust MarongedzeNo ratings yet
- Managerial EconomicsDocument33 pagesManagerial EconomicsPrakhar SahayNo ratings yet
- FIS IntroductionDocument23 pagesFIS IntroductionEngi YehiaNo ratings yet
- Title Topic For Business Research For EditingDocument11 pagesTitle Topic For Business Research For EditingKrishna Aimee BayNo ratings yet
- Assessessment of Financial Management Practices inDocument89 pagesAssessessment of Financial Management Practices inFasil Eshetu Asefa100% (1)
- MANAGERIAL ECONOMICS DECISIONSDocument12 pagesMANAGERIAL ECONOMICS DECISIONSChinni DurgaNo ratings yet
- CASE STUDY FINANCIAL PLANNING FOR A STUDENT ENTREPRENEURDocument1 pageCASE STUDY FINANCIAL PLANNING FOR A STUDENT ENTREPRENEURBetty SantiagoNo ratings yet
- Work Efficiency of Hearing Impaired Employees of LamoiyanDocument26 pagesWork Efficiency of Hearing Impaired Employees of LamoiyanPaul Varela MoralesNo ratings yet
- Value Chain Analysis - ElardoDocument3 pagesValue Chain Analysis - ElardoFerl ElardoNo ratings yet
- Online Learning Success in Lebanese UniversitiesDocument38 pagesOnline Learning Success in Lebanese Universitiesrahif shNo ratings yet
- Resume Journal A Study On Capital Budgeting Practices of Some Selected Companies in BangladeshDocument5 pagesResume Journal A Study On Capital Budgeting Practices of Some Selected Companies in Bangladeshfarah_pawestriNo ratings yet
- Case Study AnswersDocument3 pagesCase Study AnswersSumita SawantNo ratings yet
- Order To CashDocument3 pagesOrder To CashPrashanth ChidambaramNo ratings yet
- Group 2 ResearchDocument21 pagesGroup 2 ResearchCyrel Ann Baldono NaagNo ratings yet
- A Study On The Effectiveness of Entrepreneurship 2018Document14 pagesA Study On The Effectiveness of Entrepreneurship 2018haiirinnisaNo ratings yet
- MANAGERDocument8 pagesMANAGERzealousNo ratings yet
- Views on whether incentive pay programs manipulate employees more than other pay programsDocument1 pageViews on whether incentive pay programs manipulate employees more than other pay programsVikram KumarNo ratings yet
- Workplace Ergonomics and Employees Performance in MSII Final naIPRINT NI OKAY NA NIIII ELJENDocument55 pagesWorkplace Ergonomics and Employees Performance in MSII Final naIPRINT NI OKAY NA NIIII ELJENEljenColanggoNo ratings yet
- Assignment No .3: Name - Aniket Salvi GR No.-21810407 Subject - DA Roll No. - 351049Document18 pagesAssignment No .3: Name - Aniket Salvi GR No.-21810407 Subject - DA Roll No. - 351049aniket salviNo ratings yet
- Working Mothers VS Stay at Home Mothers: The Impact On ChildrenDocument28 pagesWorking Mothers VS Stay at Home Mothers: The Impact On ChildrenArpita SahaNo ratings yet
- Section A: Compulsory: Case StudyDocument3 pagesSection A: Compulsory: Case StudyrenaldooNo ratings yet
- Zimbabwe Institute of Hiv & Aids TrustDocument16 pagesZimbabwe Institute of Hiv & Aids TrustCharlene NyazikaNo ratings yet
- Mutual harm: The potential and risks of using allelopathic chemicals in agricultureDocument11 pagesMutual harm: The potential and risks of using allelopathic chemicals in agricultureMinh Anh NguyễnNo ratings yet
- PARTNER Contact Closure Adjunct: Installation InstructionsDocument6 pagesPARTNER Contact Closure Adjunct: Installation InstructionslaurahotNo ratings yet
- DILEM 10 G (24VDC) MoellerDocument7 pagesDILEM 10 G (24VDC) MoellerElizabeth RamirezNo ratings yet
- Thai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)Document32 pagesThai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)DibbaSotaNanaNo ratings yet
- Factors Affecting Movement of Beta-Lain Pigment in Beetroot CellsDocument3 pagesFactors Affecting Movement of Beta-Lain Pigment in Beetroot Cellszarahirani25% (4)
- An Experimental Study of AcidizingDocument11 pagesAn Experimental Study of Acidizinggigi17No ratings yet
- Miller Toyota-Conversion-Kit Letter ENG WEBDocument4 pagesMiller Toyota-Conversion-Kit Letter ENG WEBskyduckNo ratings yet
- Work Permit Renewal Application FormDocument2 pagesWork Permit Renewal Application FormyamojodnabNo ratings yet
- GMP TD Ar FPL 11033Document1 pageGMP TD Ar FPL 11033Sammy NguyenNo ratings yet
- Rocket Motor Head-end Structural AnalysisDocument83 pagesRocket Motor Head-end Structural AnalysisRudra Sai SandeepNo ratings yet
- Symbol High Low R5 R4 R3 R2: DailyDocument8 pagesSymbol High Low R5 R4 R3 R2: Daily257597 rmp.mech.16No ratings yet
- Positive Thinking GuideDocument23 pagesPositive Thinking GuideSimon Brassard100% (1)
- Rational Choice TheoryDocument6 pagesRational Choice TheoryMaria Theresa HerbolingoNo ratings yet
- Old Fashioned Southern Tea CakesDocument2 pagesOld Fashioned Southern Tea CakesDB ScottNo ratings yet
- Lubricants: Chapter - 5 Lubricants and LubricationDocument5 pagesLubricants: Chapter - 5 Lubricants and LubricationMalaika AzeemNo ratings yet
- Pre-Final Exam in Audit 2-3Document5 pagesPre-Final Exam in Audit 2-3Shr BnNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- Dahong PalayDocument2 pagesDahong PalayAngela MontenegroNo ratings yet
- Market ReseachDocument3 pagesMarket ReseachSam Cy PuyalesNo ratings yet
- Experiment 1 Marble Race Virtual Science Lab Chem 2Document4 pagesExperiment 1 Marble Race Virtual Science Lab Chem 2Oribe, Narciso A.100% (1)
- How To Judge A Dasha in JyotishDocument2 pagesHow To Judge A Dasha in JyotishRavan SharmaNo ratings yet
- Papers Traducir CompletoDocument12 pagesPapers Traducir CompletoJuan Jesus Barreda TalaveraNo ratings yet
- Intro To GymnasticsDocument69 pagesIntro To GymnasticsMichaela Celerio50% (2)
- Galati penitentiary historyDocument2 pagesGalati penitentiary historyLupu IonutNo ratings yet
- Case 1Document25 pagesCase 1hamshiniNo ratings yet
- Comparing Food with Comparative AdjectivesDocument4 pagesComparing Food with Comparative AdjectivesLuisito GonzalezNo ratings yet
- Healthy Voice: by Dan VascDocument22 pagesHealthy Voice: by Dan VascscoutjohnyNo ratings yet
- Concrete Epoxy HV PDFDocument2 pagesConcrete Epoxy HV PDFGeovanni Mabiscay0% (1)
- Biomechinics PDFDocument8 pagesBiomechinics PDFImran KhanNo ratings yet
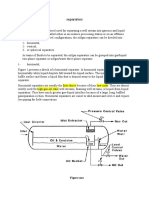
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)