You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Seal of Good Local Act of 2019: GovernanceDocument17 pagesThe Seal of Good Local Act of 2019: GovernanceRohaina Sapal100% (2)
- Foam Sprinkler System CalculationDocument5 pagesFoam Sprinkler System CalculationJitheesh Sahadevan75% (4)
- Food SecurityDocument7 pagesFood SecurityPrerna GillNo ratings yet
- 8100 FAAST Fire Alarm Aspiration Sensing Technology: Installation and Maintenance InstructionsDocument12 pages8100 FAAST Fire Alarm Aspiration Sensing Technology: Installation and Maintenance InstructionsIbrahim MohamedNo ratings yet
- Business Description Key Information: Series CDocument2 pagesBusiness Description Key Information: Series CYASH AGRAWALNo ratings yet
- The Effects of Unbalanced Circuit in Power Losses and EfficienyDocument9 pagesThe Effects of Unbalanced Circuit in Power Losses and EfficienyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter 2Document43 pagesChapter 2Puvaneswary SegharanNo ratings yet
- Human Error and Commercial Aviation Accidents: A Comprehensive, Fine-Grained Analysis Using HFACSDocument24 pagesHuman Error and Commercial Aviation Accidents: A Comprehensive, Fine-Grained Analysis Using HFACSRenata BuenoNo ratings yet
- Create Your Own Genetically Modified Organism 1Document2 pagesCreate Your Own Genetically Modified Organism 1api-264041142No ratings yet
- Memorandum of Association NokiaDocument45 pagesMemorandum of Association NokiaRoohi Salvi100% (1)
- Module 2 SolutionDocument2 pagesModule 2 SolutionLJ Valdez100% (1)
- The Mysteries of The RosaryDocument3 pagesThe Mysteries of The RosarysavannahbeeNo ratings yet
- ONOMANIADocument15 pagesONOMANIASUZAINE SARUCAMNo ratings yet
- Eco Center Latinovac, CroatiaDocument5 pagesEco Center Latinovac, CroatiaekoselaNo ratings yet
- Adorable Pet PhotographyDocument24 pagesAdorable Pet PhotographyMario ObadNo ratings yet
- SIP M&E PlanDocument5 pagesSIP M&E PlanLeopoldo Junevil T PilapilNo ratings yet
- PHD Thesis Proposal Gokhan KazarDocument29 pagesPHD Thesis Proposal Gokhan Kazarserhat yaşpalaNo ratings yet
- Basic Principles of GMP: Qualification and ValidationDocument28 pagesBasic Principles of GMP: Qualification and Validationhyde2520015754100% (1)
- Regional Overview:: ExplanationDocument7 pagesRegional Overview:: ExplanationArlyn Joy GlutonNo ratings yet
- Formulation and Evaluation of Moxifloxacin Loaded Alginate Chitosan NanoparticlesDocument5 pagesFormulation and Evaluation of Moxifloxacin Loaded Alginate Chitosan NanoparticlesSriram NagarajanNo ratings yet
- Item 25045 Power SupplyDocument11 pagesItem 25045 Power SupplyGerman ToledoNo ratings yet
- A Bridge Between Early Childhood Research and PracticeDocument4 pagesA Bridge Between Early Childhood Research and Practicehera hmNo ratings yet
- A Rich Life With Less Stuff by The Minimalists: Before You WatchDocument5 pagesA Rich Life With Less Stuff by The Minimalists: Before You WatchFelipe AndradeNo ratings yet
- A. Multiple Choice Choose A, B, C, D, or E On Your Answer SheetDocument11 pagesA. Multiple Choice Choose A, B, C, D, or E On Your Answer Sheettoede alesanaNo ratings yet
- Dabat Water Supply Design ReportDocument70 pagesDabat Water Supply Design ReportNaaf67% (3)
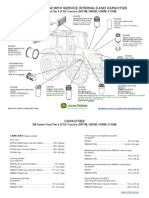
- 5 MFT4 Series TractorsDocument2 pages5 MFT4 Series TractorsBogdan PopescuNo ratings yet
- Importance of Laws and Regulations Identification of Existing Business LawsDocument4 pagesImportance of Laws and Regulations Identification of Existing Business LawsShanika GanonNo ratings yet
- High Duty Cartridge O-Ring Seal: Product Description Performance CapabilitiesDocument8 pagesHigh Duty Cartridge O-Ring Seal: Product Description Performance CapabilitiesimtiyazNo ratings yet
- DZ Value DonutDocument7 pagesDZ Value DonutAmira RosliNo ratings yet
- Precast Mix Design 2020Document2 pagesPrecast Mix Design 2020Dilhara WickramaarachchiNo ratings yet