You might also like
- Upper Airway InfectionDocument47 pagesUpper Airway Infectionjm_john0% (1)
- Ent OralDocument34 pagesEnt OralDrashti kamodiaNo ratings yet
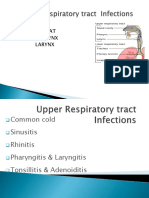
- Parts: Nose Throat Pharynx LarynxDocument47 pagesParts: Nose Throat Pharynx LarynxRANJIT GOGOINo ratings yet
- Respiratory Tract InfectionDocument30 pagesRespiratory Tract InfectionNaresh JoshiNo ratings yet
- Assessing The Ears and HearingDocument22 pagesAssessing The Ears and HearingGrace RamosNo ratings yet
- Disorder of NoseDocument31 pagesDisorder of NoseSumit YadavNo ratings yet
- NCM 113 Upper Respiratory DiseaseDocument68 pagesNCM 113 Upper Respiratory DiseaseJerah Aceron SatorreNo ratings yet
- Eye and Ear DisordersDocument14 pagesEye and Ear Disorderslemesa abdisaNo ratings yet
- Understanding Otitis Media: Causes, Symptoms and Treatment of Ear InfectionsDocument98 pagesUnderstanding Otitis Media: Causes, Symptoms and Treatment of Ear InfectionsLody Lean CruzNo ratings yet
- Common Diseases of PharynxDocument72 pagesCommon Diseases of PharynxPinak DeNo ratings yet
- Chapter 22 Management of Patients With Upper Respiratory Tract DisordersDocument7 pagesChapter 22 Management of Patients With Upper Respiratory Tract DisordersPeej Reyes100% (2)
- Otits MediaDocument68 pagesOtits MediaSaidi EdwardNo ratings yet
- Med 3, Chloe SaadeDocument53 pagesMed 3, Chloe Saadeanon_767794134No ratings yet
- URTDDocument61 pagesURTDfcgabasanNo ratings yet
- MANAGEMENT OF EAR, NOSE AND THROAT DISEASESDocument16 pagesMANAGEMENT OF EAR, NOSE AND THROAT DISEASESSaurabh LamkhadeNo ratings yet
- Treatment of Maxillary SinusitisDocument15 pagesTreatment of Maxillary SinusitisRabina PantaNo ratings yet
- Acute Laryngitis: Li SGD 21 LBM 5Document40 pagesAcute Laryngitis: Li SGD 21 LBM 511juni09No ratings yet
- Acute TonsillitisDocument22 pagesAcute Tonsillitisg0ldz21100% (10)
- Ear DisorderDocument61 pagesEar DisorderSakthi DeviNo ratings yet
- Acute and Chronic LaryngitisDocument20 pagesAcute and Chronic LaryngitisBirjesh KumarNo ratings yet
- External Ear DiseasesDocument6 pagesExternal Ear DiseasesJohn Christopher LucesNo ratings yet
- Sinus Infection Symptoms and TreatmentsDocument1 pageSinus Infection Symptoms and TreatmentsfakrulnersmudaNo ratings yet
- Respiratory Disorders ExplainedDocument89 pagesRespiratory Disorders ExplainedSyed MaazNo ratings yet
- 1.0 Upper Airway InfectionsDocument45 pages1.0 Upper Airway InfectionsMariahNo ratings yet
- NRSG 364 - Respiratory DisordersDocument65 pagesNRSG 364 - Respiratory DisordersJoanNo ratings yet
- Concept Map FinaleDocument31 pagesConcept Map FinaleDeVineNo ratings yet
- Upper Respiratory Infections: Symptoms and TreatmentsDocument45 pagesUpper Respiratory Infections: Symptoms and TreatmentsNatasha Abdulla100% (2)
- Treat Acute Chronic Ear InfectionsDocument32 pagesTreat Acute Chronic Ear InfectionsAndrew KaumbaNo ratings yet
- Nasal Obstruction: Nitha K 2nd Year MSC NursingDocument65 pagesNasal Obstruction: Nitha K 2nd Year MSC NursingNITHA KNo ratings yet
- Upper Respiratory Tract Infection GuideDocument45 pagesUpper Respiratory Tract Infection GuideFarwaNo ratings yet
- Pulmonary and Respiratory Nursing Assessment GuideDocument48 pagesPulmonary and Respiratory Nursing Assessment GuideEmjay JapitanaNo ratings yet
- Ear DisordersDocument23 pagesEar DisordersJoana MarauNo ratings yet
- Nur 218 Peds Exam 1 Study Guide Role of The Pediatric NurseDocument9 pagesNur 218 Peds Exam 1 Study Guide Role of The Pediatric NurseNurseme13No ratings yet
- Otitis Media: Prepared By: - Priyanka ThapaDocument38 pagesOtitis Media: Prepared By: - Priyanka ThapaKalo kajiNo ratings yet
- Acute Sinusitis Types and TreatmentsDocument11 pagesAcute Sinusitis Types and Treatmentsعبدالله فائز غلامNo ratings yet
- Sinusitis: Causes, Symptoms and TreatmentDocument19 pagesSinusitis: Causes, Symptoms and TreatmentArvindhanNo ratings yet
- SinusitisDocument23 pagesSinusitisMumin Alamin AllaminNo ratings yet
- Acuite Otitis Media Final PresentationDocument26 pagesAcuite Otitis Media Final Presentationmohamedkallon1996No ratings yet
- Disorder of ThroatDocument21 pagesDisorder of ThroatSumit YadavNo ratings yet
- EPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Document34 pagesEPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Julliza Joy PandiNo ratings yet
- Otitis MediaDocument25 pagesOtitis Mediadmmwale1995No ratings yet
- Lesson 5 - Disaster ManagementDocument40 pagesLesson 5 - Disaster ManagementHampson MalekanoNo ratings yet
- Week 1 3 Management of Patients With Problems in Respiratory SystemDocument22 pagesWeek 1 3 Management of Patients With Problems in Respiratory SystemKIANA LOUISE ROMANONo ratings yet
- Acute Diffuse Otitis ExternaDocument36 pagesAcute Diffuse Otitis ExternaIlham Isnin Dolyanov HasibuanNo ratings yet
- Sinusitis in ChildDocument14 pagesSinusitis in ChildKin molikaNo ratings yet
- Otitis Media and ExternaDocument22 pagesOtitis Media and ExternaLhanz CayingNo ratings yet
- Ent Med RevisionDocument41 pagesEnt Med RevisionswamysamsonNo ratings yet
- Otitis ExternaDocument7 pagesOtitis ExternaJayson TrajanoNo ratings yet
- Expose On EntDocument20 pagesExpose On EntDUCHELNo ratings yet
- PRACTICE TEACHING On Otitis Media FinalDocument33 pagesPRACTICE TEACHING On Otitis Media FinalAjit ThangeNo ratings yet
- Sinusitis: Causes, Incidence, and Risk FactorsDocument5 pagesSinusitis: Causes, Incidence, and Risk FactorsDyane VatriciaNo ratings yet
- Causes, Signs, Treatment of Acute Otitis MediaDocument19 pagesCauses, Signs, Treatment of Acute Otitis MediaRajesh Sharma100% (1)
- Acute and Chronic RhinitisDocument25 pagesAcute and Chronic RhinitisagniajolandaNo ratings yet
- Ear Pathology GuideDocument34 pagesEar Pathology Guidenagham hamdanNo ratings yet
- Chronic SinusitisDocument30 pagesChronic SinusitisAbdiqani MahdiNo ratings yet
- EaracheDocument5 pagesEaracheclubsanatateNo ratings yet
- Otitis MediaDocument18 pagesOtitis MediatanmayatechtubeNo ratings yet
- Maternal Infections Overview PDFDocument16 pagesMaternal Infections Overview PDFsubiNo ratings yet
- Defibrillator1 200806145633Document28 pagesDefibrillator1 200806145633harpreetNo ratings yet
- DrHarrison GALLSTONE DISEASE Presentation 06 2016 2Document31 pagesDrHarrison GALLSTONE DISEASE Presentation 06 2016 2harpreetNo ratings yet
- Excel Basics Lesson Plan FiveDocument9 pagesExcel Basics Lesson Plan FiveharpreetNo ratings yet
- Urinary System PDFDocument27 pagesUrinary System PDFfiona100% (3)
- Hepetitis Day CelebrationDocument8 pagesHepetitis Day CelebrationharpreetNo ratings yet
- Vital Signs Procedures ChecklistDocument3 pagesVital Signs Procedures ChecklistharpreetNo ratings yet
- Concept of Disease Causation Theories (39Document28 pagesConcept of Disease Causation Theories (39harpreetNo ratings yet
- SodaPDF Converted Lymphaticsystemppt 180102075748Document63 pagesSodaPDF Converted Lymphaticsystemppt 180102075748harpreetNo ratings yet
- Problem Statement DocsDocument2 pagesProblem Statement DocsharpreetNo ratings yet
- Basic Life Support Video LessonDocument14 pagesBasic Life Support Video LessonharpreetNo ratings yet
- TACHOSTOMYDocument3 pagesTACHOSTOMYharpreetNo ratings yet
- BLS: Essential Steps for Cardiac EmergenciesDocument10 pagesBLS: Essential Steps for Cardiac EmergenciesharpreetNo ratings yet
- 19 AcidBaseBalanceDocument3 pages19 AcidBaseBalancesedaka26No ratings yet
- Leadership Final..Document3 pagesLeadership Final..harpreetNo ratings yet
- BLS Basics: Scene Safety, Circulation, Airway, BreathingDocument118 pagesBLS Basics: Scene Safety, Circulation, Airway, Breathingharpreet100% (1)
- ENT PresentationDocument79 pagesENT PresentationfelliciaNo ratings yet
- Disaster ManagementDocument12 pagesDisaster ManagementharpreetNo ratings yet
- Planning & Organizing A Hospital, Unit & Ancillary ServicesDocument31 pagesPlanning & Organizing A Hospital, Unit & Ancillary ServicesSimon Josan100% (4)
- Advantages of Lecture MethodDocument9 pagesAdvantages of Lecture MethodharpreetNo ratings yet
- DM-DECENTRALIZED DECISION MAKINGDocument19 pagesDM-DECENTRALIZED DECISION MAKINGharpreetNo ratings yet
- Personnel Management: Personnel:-It Is Defined As People Employed in An Organization or EngagedDocument30 pagesPersonnel Management: Personnel:-It Is Defined As People Employed in An Organization or EngagedharpreetNo ratings yet
- Theories and Models of ManagementDocument61 pagesTheories and Models of ManagementharpreetNo ratings yet
- PacemakerDocument3 pagesPacemakerharpreetNo ratings yet
- Educational Institutions and PhilosophiesDocument11 pagesEducational Institutions and PhilosophiesharpreetNo ratings yet
- FRACTUREDocument21 pagesFRACTUREharpreetNo ratings yet
- EPCC Hydrocarbon Downstream L&T 09.01.2014Document49 pagesEPCC Hydrocarbon Downstream L&T 09.01.2014shyaminannnaNo ratings yet
- St. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingDocument3 pagesSt. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingKristiene Kyle AquinoNo ratings yet
- 3 Point ProblemDocument8 pages3 Point ProblemDhana Strata NNo ratings yet
- Mysteries of The Pyramid - David H LewisDocument42 pagesMysteries of The Pyramid - David H LewisMeinathan Selvamoorthy0% (1)
- MIDTERM QUIZ 2 - Attempt ReviewDocument5 pagesMIDTERM QUIZ 2 - Attempt ReviewAshnesh YadavNo ratings yet
- CiviljointpdfDocument8 pagesCiviljointpdfAyashu PandeyNo ratings yet
- Gupea 2077 37037 1Document46 pagesGupea 2077 37037 1Guilherme PeresNo ratings yet
- Prescription AssignmentDocument6 pagesPrescription AssignmentChiela Alcantara BagnesNo ratings yet
- Break Even PresentationDocument18 pagesBreak Even PresentationLorraine NyikaNo ratings yet
- Welcome To This Unique Cpe Online Course: International Online Language SchoolDocument5 pagesWelcome To This Unique Cpe Online Course: International Online Language SchoolJairo JuniorNo ratings yet
- Busn 702Document9 pagesBusn 702Pablo GuzmánNo ratings yet
- CRMDocument32 pagesCRMJoel Dsouza100% (1)
- 641c558d1b24f3001801a8fd - ## - Sociology 52 - Daily Class Notes - (UPSC Optional Sociology)Document5 pages641c558d1b24f3001801a8fd - ## - Sociology 52 - Daily Class Notes - (UPSC Optional Sociology)Jai Ma DurgaNo ratings yet
- Realm of AngelsDocument9 pagesRealm of AngelsElisha100% (1)
- Synthesis: Turn Learnings into Opportunities for DesignDocument12 pagesSynthesis: Turn Learnings into Opportunities for DesignLuisana MartínNo ratings yet
- Shs Forms Ruby (First Semester)Document44 pagesShs Forms Ruby (First Semester)Jeanicar Culi - AsiñasNo ratings yet
- The Stoch OscilattorDocument6 pagesThe Stoch Oscilattorapi-3831404No ratings yet
- How Squirrel Got Its StripesDocument12 pagesHow Squirrel Got Its StripesVIJAYA MNo ratings yet
- 10 Steps For Avoiding Teacher BurnoutDocument3 pages10 Steps For Avoiding Teacher BurnoutSarah DeNo ratings yet
- Gramatica Limbii Engleze Cls 1-4 - Cristina JohnsonDocument8 pagesGramatica Limbii Engleze Cls 1-4 - Cristina JohnsonGeorgiana CosminaNo ratings yet
- Lesson PlanDocument3 pagesLesson Planapi-479604636No ratings yet
- Research in Daily Life 2Document166 pagesResearch in Daily Life 2Zianna Marie De RamosNo ratings yet
- (13a) Active and Passive VoiceDocument2 pages(13a) Active and Passive VoiceVedhNo ratings yet
- Special Subject 1.2Document25 pagesSpecial Subject 1.2Hà Trang Hoàng100% (1)
- Sparsh Gupta 14e-Anti Diabetes MCQDocument12 pagesSparsh Gupta 14e-Anti Diabetes MCQSubodh ChaudhariNo ratings yet
- CARAVAL - Opening ExtractDocument29 pagesCARAVAL - Opening ExtractHodder Stoughton100% (1)
- Points in Community Health NursingDocument9 pagesPoints in Community Health NursingkuyarahimNo ratings yet
- UML Modeling GuideDocument43 pagesUML Modeling Guideteddy haileNo ratings yet
- Criminal LiabilityDocument3 pagesCriminal LiabilityAqZarNo ratings yet
- RePAMO PDFDocument19 pagesRePAMO PDFRonald JosephNo ratings yet