You might also like
- DrMercola SiimLandandJamesDiNicolantonio TheImmunityFixDocument28 pagesDrMercola SiimLandandJamesDiNicolantonio TheImmunityFixRocco LamponeNo ratings yet
- Guide To Graphene Oxide DetoxDocument5 pagesGuide To Graphene Oxide Detoxeu100% (3)
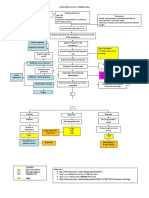
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaAzria John DemetriNo ratings yet
- ICU One Pager Tracheostomy EmergenciesDocument1 pageICU One Pager Tracheostomy EmergenciesJonathan JohnsonNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)aishwaryaNo ratings yet
- Pediatrics Physical ExaminationDocument1 pagePediatrics Physical ExaminationdzaddNo ratings yet
- Trigeminal Neuralgia: Causes and TreatmentsDocument79 pagesTrigeminal Neuralgia: Causes and TreatmentsIsyana Khaerunisa100% (2)
- Chronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultsDocument14 pagesChronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultschristineNo ratings yet
- Preoperative PreparationDocument22 pagesPreoperative Preparationjackyploes100% (1)
- Trigeminal Neuralgia PresentationDocument27 pagesTrigeminal Neuralgia Presentationmelencio olivasNo ratings yet
- Pertussis (Whooping Cough) : University of BuroaDocument42 pagesPertussis (Whooping Cough) : University of BuroaMumin Alamin AllaminNo ratings yet
- Ear DisordersDocument7 pagesEar DisordersGéorel John Colonia GoteraNo ratings yet
- TympanoplastyDocument75 pagesTympanoplastylisabdaNo ratings yet
- Upper Airway ObstructionDocument31 pagesUpper Airway ObstructiontrimardiyanaisyanNo ratings yet
- Assessing The Skull and Face PerformanceDocument1 pageAssessing The Skull and Face PerformanceAbigail BrillantesNo ratings yet
- First Aide 2023Document97 pagesFirst Aide 2023jrfdcafprescomNo ratings yet
- Application of Orem's Self-CareDocument36 pagesApplication of Orem's Self-CaresonaNo ratings yet
- RhinosinusitisDocument45 pagesRhinosinusitisMuhammad Ade RahmanNo ratings yet
- Causes and Treatment of EpistaxisDocument40 pagesCauses and Treatment of EpistaxisSilar KhanNo ratings yet
- Lower Respiratory Tract Diseases - KeyDocument45 pagesLower Respiratory Tract Diseases - KeyYugmaPandyaNo ratings yet
- 10.folliculitis, Furuncle, and CarbuncleDocument27 pages10.folliculitis, Furuncle, and CarbuncleWorku KifleNo ratings yet
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 33 - Nasal Fractures PDFDocument15 pages33 - Nasal Fractures PDFcarlosNo ratings yet
- Ear AssessmentDocument39 pagesEar AssessmentLyn MendeNo ratings yet
- Antrochoanal PolypDocument18 pagesAntrochoanal PolypReem Eshra100% (1)
- Acute Sinusitis 08Document2 pagesAcute Sinusitis 08ativonNo ratings yet
- Trigeminal Neuralgia GuideDocument15 pagesTrigeminal Neuralgia Guideandreas kevinNo ratings yet
- Perichondritis PinnaDocument2 pagesPerichondritis PinnaAnish RajNo ratings yet
- Fracture Nasal BonesDocument16 pagesFracture Nasal BonesGẽrman DiãzNo ratings yet
- NCP DIarrheaDocument8 pagesNCP DIarrheakamini ChoudharyNo ratings yet
- Laryngitis: SpasmDocument13 pagesLaryngitis: Spasm44-Shruti paghdalNo ratings yet
- Croup SyndromeDocument3 pagesCroup SyndromeMabesNo ratings yet
- Stridor & Stertor: by Dr. Baseem N. AbdulhadiDocument20 pagesStridor & Stertor: by Dr. Baseem N. AbdulhadiAli Abd AlrezaqNo ratings yet
- Case Study: PharyngitisDocument3 pagesCase Study: PharyngitisRestian Rony SaragiNo ratings yet
- Pediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyDocument4 pagesPediatric Imperforate Anus - Background, Pathophysiology, EpidemiologyYehuda Agus SantosoNo ratings yet
- Foreign Body in The NoseDocument32 pagesForeign Body in The NoseLady350zNo ratings yet
- Donning and Doffing Personal Protective Eqquipment (Ppe) : PreparationDocument2 pagesDonning and Doffing Personal Protective Eqquipment (Ppe) : PreparationPam RuizNo ratings yet
- Acute Laryngitis: Li SGD 21 LBM 5Document40 pagesAcute Laryngitis: Li SGD 21 LBM 511juni09No ratings yet
- Chronic SinusitisDocument19 pagesChronic SinusitisMunawwar AwaNo ratings yet
- Stridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiDocument33 pagesStridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiVishal GauravNo ratings yet
- Otitis MediaDocument6 pagesOtitis MediaririNo ratings yet
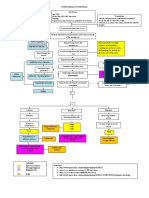
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJuneNo ratings yet
- Asthma Training Module - 2013Document204 pagesAsthma Training Module - 2013Dr_Bhavesh_ParmarNo ratings yet
- The Pathophysiology of Otosclerosis: Review of Current ResearchDocument6 pagesThe Pathophysiology of Otosclerosis: Review of Current ResearchFelipeAsenjoÁlvarezNo ratings yet
- Vitamin A and XerophthalmiaDocument29 pagesVitamin A and XerophthalmiaJayashree IyerNo ratings yet
- EpistaxisDocument9 pagesEpistaxisapi-285171922No ratings yet
- GlaucomaDocument14 pagesGlaucomaWilliam SumoroNo ratings yet
- Ear Infection Assessment and ManagementDocument8 pagesEar Infection Assessment and ManagementArt Christian Ramos100% (1)
- Drugs Study For PneumoniaDocument5 pagesDrugs Study For PneumoniaLucelle ArellanoNo ratings yet
- Recurrent Respiratory Papillomatosis: FaringDocument49 pagesRecurrent Respiratory Papillomatosis: FaringIchsanJuliansyahNo ratings yet
- Thoracentesis Is Also Known As Pleural Fluid AnalysisDocument3 pagesThoracentesis Is Also Known As Pleural Fluid AnalysisJ.r. MercadoNo ratings yet
- Systemic Lupus ErythemathosusDocument23 pagesSystemic Lupus ErythemathosusFransisca HardimartaNo ratings yet
- ConjunctivitisDocument18 pagesConjunctivitisPrashanth Padmini VenugopalNo ratings yet
- Anatomy and Physiology of the ConjunctivaDocument43 pagesAnatomy and Physiology of the ConjunctivaVincentius Okta VidiandickaNo ratings yet
- Upper Respiratory Tract Infection (Urti)Document2 pagesUpper Respiratory Tract Infection (Urti)wen_pilNo ratings yet
- EXTERNAL EAR DISORDERS AND DEFORMITIESDocument48 pagesEXTERNAL EAR DISORDERS AND DEFORMITIEShemaanandhyNo ratings yet
- Osce EarexamDocument2 pagesOsce EarexamminhaapNo ratings yet
- DiphtheriaDocument22 pagesDiphtheriaLovely Acabado TampocoNo ratings yet
- SinusitisDocument37 pagesSinusitismalathiNo ratings yet
- Contemporary Treatment of AmeloblastomaDocument7 pagesContemporary Treatment of AmeloblastomaomeerulrafieNo ratings yet
- Cord Care MillerDocument4 pagesCord Care MillerCG Patron BamboNo ratings yet
- Annotated Group 2 Impetigo Concept Mapping 1Document30 pagesAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANONo ratings yet
- Case Study UrtiDocument9 pagesCase Study UrtiHomework PingNo ratings yet
- EpistaxisDocument22 pagesEpistaxisDood100% (1)
- ParacetamolDocument2 pagesParacetamolsleep whatNo ratings yet
- Listeria Monocytogenes 1Document27 pagesListeria Monocytogenes 1Mumin Alamin AllaminNo ratings yet
- TB Symptoms, Causes and TypesDocument65 pagesTB Symptoms, Causes and TypesMumin Alamin AllaminNo ratings yet
- Diphtheria: University of BuroaDocument80 pagesDiphtheria: University of BuroaMumin Alamin AllaminNo ratings yet
- Health Management SynopsisDocument3 pagesHealth Management SynopsisSubrat PatnaikNo ratings yet
- Ayurvedic Bhasma PDFDocument9 pagesAyurvedic Bhasma PDFFARIS NATTUKALNo ratings yet
- An Introduction To Anatomy and Physiology: Powerpoint Lecture Presentations Prepared by Jason LapresDocument67 pagesAn Introduction To Anatomy and Physiology: Powerpoint Lecture Presentations Prepared by Jason LapresLina TasamaNo ratings yet
- Mercury Mercruiser Marine Engine 32-4-3l Mpi Gasoline Service ManualDocument22 pagesMercury Mercruiser Marine Engine 32-4-3l Mpi Gasoline Service Manualjamesmiller060901qms100% (30)
- IMMUNOMODULATORY ACTIVITIES OF SOME ZINGIBERACEAE PLANTSDocument13 pagesIMMUNOMODULATORY ACTIVITIES OF SOME ZINGIBERACEAE PLANTSZalfa SalsabilaNo ratings yet
- Patent Ductus ArteriosusDocument49 pagesPatent Ductus Arteriosusarchana vermaNo ratings yet
- Assessing Hygiene of Canteen WorkersDocument4 pagesAssessing Hygiene of Canteen WorkersRutvik ChawareNo ratings yet
- Reading Passage 1: Test 16 DiabetesDocument7 pagesReading Passage 1: Test 16 DiabetesRavi ZaiminNo ratings yet
- Milpersman 1910-402Document1 pageMilpersman 1910-402benpickensNo ratings yet
- Nursing Care Plan for Risk of Bleeding During PregnancyDocument4 pagesNursing Care Plan for Risk of Bleeding During PregnancybananakyuNo ratings yet
- Rodela Et AlDocument14 pagesRodela Et AlDanish KhanNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlintana JobelleNo ratings yet
- Reasons BSN Students Are LateDocument4 pagesReasons BSN Students Are LateKizza SaavedraNo ratings yet
- School Form 8 (SF 8)Document3 pagesSchool Form 8 (SF 8)yZNo ratings yet
- TRN2044095 7939696 Clinical ReportDocument10 pagesTRN2044095 7939696 Clinical ReportWARNET SANTONo ratings yet
- Kuo 2014Document13 pagesKuo 2014Instituto Integrado em PsicologiaNo ratings yet
- What Is Your Reflection About The Current ECQ? How Do People Behave and Communicate During This ECQ?Document3 pagesWhat Is Your Reflection About The Current ECQ? How Do People Behave and Communicate During This ECQ?Allijah Trish HernandezNo ratings yet
- Gestational Diabetes Mellitus - : One Disease Two Lives at StakeDocument31 pagesGestational Diabetes Mellitus - : One Disease Two Lives at StakeSadia YousafNo ratings yet
- Dental Clinic Covid-19 FormsDocument4 pagesDental Clinic Covid-19 FormsButch EnalpeNo ratings yet
- Proposal 41Document49 pagesProposal 41Abdulahi SaedNo ratings yet
- Lesson Plan AddictionDocument3 pagesLesson Plan AddictionJacqueline ElleNo ratings yet
- Rehabilitation of A Complex Oro-Facial Defect by Modified Prosthetic ApproachDocument3 pagesRehabilitation of A Complex Oro-Facial Defect by Modified Prosthetic ApproachBharat KhemaniNo ratings yet
- Module Goals: College of Criminal Justice EducationDocument8 pagesModule Goals: College of Criminal Justice EducationAila EchemaneNo ratings yet
- Treatment of Positional Obstructive Sleep Apnea (POSA)Document5 pagesTreatment of Positional Obstructive Sleep Apnea (POSA)kiran kumarNo ratings yet
- Kettering Business PlanDocument22 pagesKettering Business PlanfrankNo ratings yet
- Clinical Considerations Case Catalog Screenshots and TimecodesDocument4 pagesClinical Considerations Case Catalog Screenshots and TimecodesnenitaNo ratings yet