You might also like
- Pediatric Community Acquired Pneumonia (PCAP)Document24 pagesPediatric Community Acquired Pneumonia (PCAP)deejayseroje93% (28)
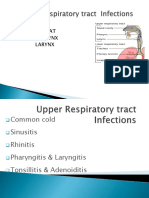
- Upper Respiratory Tract InfectionsDocument73 pagesUpper Respiratory Tract InfectionsankitaNo ratings yet
- ICU-Acquired Infections in Immunocompromised PatientsDocument18 pagesICU-Acquired Infections in Immunocompromised Patientsdarkangelmx1No ratings yet
- Science: Quarter 1, WK 2 - Module 2Document31 pagesScience: Quarter 1, WK 2 - Module 2Andres Boni85% (13)
- URTIDocument41 pagesURTIGetaneh LiknawNo ratings yet
- Chapter 6 Disorders Respiratory in ClientDocument101 pagesChapter 6 Disorders Respiratory in Clientanisa ahmedNo ratings yet
- Sinusitis Symptoms and TreatmentDocument33 pagesSinusitis Symptoms and TreatmentshyamashaNo ratings yet
- Respi Patho 1Document111 pagesRespi Patho 1Quolette ConstanteNo ratings yet
- The Child With Respiratory DysfunctionDocument91 pagesThe Child With Respiratory DysfunctionSerbanNo ratings yet
- Alvin M. Hernandez, RN, RM, MSN, Man Faculty, School of NursingDocument37 pagesAlvin M. Hernandez, RN, RM, MSN, Man Faculty, School of NursingkathnlscNo ratings yet
- Referat Batuk NurfitriDocument45 pagesReferat Batuk NurfitribellabelbonNo ratings yet
- Otitis Media: Prepared By: - Priyanka ThapaDocument38 pagesOtitis Media: Prepared By: - Priyanka ThapaKalo kajiNo ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- Rhinitis and Sinusitis in Guinea PigsDocument3 pagesRhinitis and Sinusitis in Guinea PigsDivya KashyapNo ratings yet
- Whooping Cough: Dr. MwendwaDocument39 pagesWhooping Cough: Dr. MwendwaAlvin OmondiNo ratings yet
- MS RESPIbfrDocument13 pagesMS RESPIbfrEmeroot RootNo ratings yet
- Diseases of Throat: Pharyngitis, Tonsillitis and AdenoiditisDocument39 pagesDiseases of Throat: Pharyngitis, Tonsillitis and Adenoiditismaria jacobNo ratings yet
- Nursing Management of Children With Respiratory System DysfunctionsDocument27 pagesNursing Management of Children With Respiratory System DysfunctionsDody ZainNo ratings yet
- Upper Respiratory Tract Infection: Features of Respiratory Disorders in Children AreDocument16 pagesUpper Respiratory Tract Infection: Features of Respiratory Disorders in Children AreMerna MahrousNo ratings yet
- II. Upper Respiratory Tract DisordersDocument98 pagesII. Upper Respiratory Tract DisordersarielleortuosteNo ratings yet
- Deseases of The LarynxDocument78 pagesDeseases of The Larynxabarna abiNo ratings yet
- Pediatric Cough CMEDocument59 pagesPediatric Cough CMEkurutalaNo ratings yet
- Upper Respiratory Infections: Symptoms and TreatmentsDocument45 pagesUpper Respiratory Infections: Symptoms and TreatmentsNatasha Abdulla100% (2)
- Respi SDG Cluster3Document45 pagesRespi SDG Cluster3faye kimNo ratings yet
- Pulmonary and Respiratory Nursing Assessment GuideDocument48 pagesPulmonary and Respiratory Nursing Assessment GuideEmjay JapitanaNo ratings yet
- Nursing Care of High Risk InfantDocument48 pagesNursing Care of High Risk InfantDianne Rose AgliamNo ratings yet
- Parts: Nose Throat Pharynx LarynxDocument47 pagesParts: Nose Throat Pharynx LarynxRANJIT GOGOINo ratings yet
- Nursing Care of The Child With Respiratory DysfunctionDocument54 pagesNursing Care of The Child With Respiratory DysfunctionAlexis Coronado100% (1)
- Tonsillitis and Adenoiditis: Islamic University Nursing CollegeDocument15 pagesTonsillitis and Adenoiditis: Islamic University Nursing CollegeNinaNo ratings yet
- Respiratory System 2017 PDFDocument158 pagesRespiratory System 2017 PDFdarla ryanNo ratings yet
- Disclaimer: Christian Medical College Networked HospitalsDocument44 pagesDisclaimer: Christian Medical College Networked HospitalsJohn DorNo ratings yet
- Acute Lower Respiratory Tract Infection (ALRTI)Document43 pagesAcute Lower Respiratory Tract Infection (ALRTI)yosephNo ratings yet
- Managing Upper Respiratory Tract InfectionsDocument93 pagesManaging Upper Respiratory Tract InfectionsErica Clerigo LandichoNo ratings yet
- Respiratory Disorders in PediatricsDocument11 pagesRespiratory Disorders in PediatricsMateo Geoff100% (1)
- 5 Sore ThroatDocument45 pages5 Sore ThroatNurul Wandasari SNo ratings yet
- Upper Respiratory JerusalemDocument24 pagesUpper Respiratory JerusalemAYO NELSONNo ratings yet
- ARIs CME2Document50 pagesARIs CME2JunaidahMubarakAliNo ratings yet
- Common ENT Conditions PresentationDocument60 pagesCommon ENT Conditions PresentationMICHAEL SAKALANo ratings yet
- Anatomi Tenggorokan Dan Penerapan Klinisnya: Dr. Adi Arianto, M. BiomedDocument39 pagesAnatomi Tenggorokan Dan Penerapan Klinisnya: Dr. Adi Arianto, M. BiomedAl AdinNo ratings yet
- P 3 The Upper Respiratory Tract 2Document61 pagesP 3 The Upper Respiratory Tract 2Christelle CilliersNo ratings yet
- 4 - Pharyngitis BronchitisDocument31 pages4 - Pharyngitis BronchitisAishwaryaNo ratings yet
- Day 15 - NCM-109 Children With Alteration in Oxygenation (A)Document50 pagesDay 15 - NCM-109 Children With Alteration in Oxygenation (A)Sheena Patricia ArasulaNo ratings yet
- Pediatric Nasopharyngeal Mass: Causes and ManagementDocument79 pagesPediatric Nasopharyngeal Mass: Causes and ManagementShahnawazNo ratings yet
- Respiratory Immun AllergyDocument125 pagesRespiratory Immun Allergyhasanatiya41No ratings yet
- Approach Child With Recurrent WheezeDocument41 pagesApproach Child With Recurrent Wheezecristina_zaharia865440No ratings yet
- Managing Illness: BY: S. Tolentino, RNDocument170 pagesManaging Illness: BY: S. Tolentino, RNSabrina TolentinoNo ratings yet
- Treat Acute Chronic Ear InfectionsDocument32 pagesTreat Acute Chronic Ear InfectionsAndrew KaumbaNo ratings yet
- Respiratory Tract InfectionDocument30 pagesRespiratory Tract InfectionNaresh JoshiNo ratings yet
- Otits MediaDocument68 pagesOtits MediaSaidi EdwardNo ratings yet
- Respiratory Disorders 1uK 2Document7 pagesRespiratory Disorders 1uK 2zainahalqahtani3No ratings yet
- BSC Nursing Guide: Tonsillitis and AdenoiditisDocument41 pagesBSC Nursing Guide: Tonsillitis and AdenoiditisYAMINIPRIYANNo ratings yet
- Disorders of EarDocument17 pagesDisorders of EarharpreetNo ratings yet
- Acute Respiratory Infection in ChildrenDocument70 pagesAcute Respiratory Infection in Childrenmayadwintas100% (1)
- SinusitisDocument23 pagesSinusitisMumin Alamin AllaminNo ratings yet
- Unit V: Conti Upper Respiratory Tract Infection: PharyngitisDocument17 pagesUnit V: Conti Upper Respiratory Tract Infection: PharyngitisshaistaNo ratings yet
- Nursing Care of A Child With Respiratory DisorderDocument85 pagesNursing Care of A Child With Respiratory DisorderChris CharzNo ratings yet
- Diseases of The Oropharynx & NasopharynxDocument38 pagesDiseases of The Oropharynx & Nasopharynxalmazmulu76No ratings yet
- Acute Pharyngitis and Tonsillitis GuideDocument56 pagesAcute Pharyngitis and Tonsillitis Guidewilliam_SatyanegaraNo ratings yet
- Resp System KoleyaDocument96 pagesResp System KoleyaAlberto MeroNo ratings yet
- MED SURG OUTLINE Chapter 14 Care of Patients With Disorders of Upper Respiratory SystemDocument6 pagesMED SURG OUTLINE Chapter 14 Care of Patients With Disorders of Upper Respiratory SystemMichaela LemanNo ratings yet
- Hoarse Voice (Laryngitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHoarse Voice (Laryngitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Mood Disorders 1 PostingDocument56 pagesMood Disorders 1 PostingJoanNo ratings yet
- Psychotropic DrugsDocument81 pagesPsychotropic DrugsJoan100% (2)
- Obsessive-Compulsive and Related DisordersDocument16 pagesObsessive-Compulsive and Related DisordersJoanNo ratings yet
- Feeding and Eating DisordersDocument41 pagesFeeding and Eating DisordersJoanNo ratings yet
- Title: Integrated Case Study ReportDocument8 pagesTitle: Integrated Case Study ReportZunaira ArshadNo ratings yet
- GgoDocument6 pagesGgoAnupam ShrivastavaNo ratings yet
- PB 1 - NP 1 (Final)Document19 pagesPB 1 - NP 1 (Final)AnnizaNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanIsabelle Madrid100% (1)
- Accuracy of Death Certificates and Assessment of FactorsDocument8 pagesAccuracy of Death Certificates and Assessment of FactorsFaiz QintharNo ratings yet
- Acute Sinusitis: Practice EssentialsDocument22 pagesAcute Sinusitis: Practice EssentialsAna-Maria DuMiNo ratings yet
- Pulmonary PharmaDocument242 pagesPulmonary Pharmaarturo quevedoNo ratings yet
- Arab Board Orthopedic Exam June 2013Document35 pagesArab Board Orthopedic Exam June 2013Nasser AlbaddaiNo ratings yet
- MRCP Book 070709Document11 pagesMRCP Book 070709wwwrgrobinNo ratings yet
- MKSAP13-Pulmonary Medicine and Critical CareDocument85 pagesMKSAP13-Pulmonary Medicine and Critical CaresarfirazNo ratings yet
- Implementation Guide For VentilatorDocument9 pagesImplementation Guide For VentilatorDewi Ratna SariNo ratings yet
- Studies On Public Health and Hygiene Condition of Retailers at Fish Markets in South-Central BangladeshDocument8 pagesStudies On Public Health and Hygiene Condition of Retailers at Fish Markets in South-Central BangladeshHayyina FirdaniNo ratings yet
- Far Eastern University-Institute of Nursing In-House NursingDocument25 pagesFar Eastern University-Institute of Nursing In-House Nursingjonasdelacruz1111No ratings yet
- Opportunistic Infections PreventionDocument34 pagesOpportunistic Infections PreventionEvelyn LimNo ratings yet
- CHN FinalsDocument43 pagesCHN FinalsNHICOLE YAO PORCESONo ratings yet
- CAz Clinic Poliserozita UMFDocument16 pagesCAz Clinic Poliserozita UMFMariaIoanaCoroiuNo ratings yet
- NANDA Page 658Document5 pagesNANDA Page 658Ashley Gaton Alindogan100% (1)
- Ncle X RN Test Study GuideDocument199 pagesNcle X RN Test Study GuideKIT100% (1)
- Body temperature, vital signs, anthropometric measurementsDocument8 pagesBody temperature, vital signs, anthropometric measurementsApril Rae Obregon GarcesNo ratings yet
- PNEUMONIADocument44 pagesPNEUMONIAReshama JamankarNo ratings yet
- Interstitial Lung Disease: The Diagnostic Role of Bronchoscopy.Document15 pagesInterstitial Lung Disease: The Diagnostic Role of Bronchoscopy.Hitomi-No ratings yet
- IV Oral Table PDFDocument2 pagesIV Oral Table PDFRosyadi AkbarriNo ratings yet
- Upper Left Abdominal Pain Under Ribs - Symptoms and 18 CausesDocument34 pagesUpper Left Abdominal Pain Under Ribs - Symptoms and 18 CausesJayri FelNo ratings yet
- Tetracycline SDocument51 pagesTetracycline SPapaindoNo ratings yet
- Fungal Infections: Alma E. Malilong, MD, FPSPDocument33 pagesFungal Infections: Alma E. Malilong, MD, FPSPQurrataini IbanezNo ratings yet
- Question Bank PT-II SET 02 Question Paper 2021Document20 pagesQuestion Bank PT-II SET 02 Question Paper 2021xyzNo ratings yet
- 10-Effect of Chest Physical Therapy On Pediatrics Hospitalized With Pneumonia PDFDocument8 pages10-Effect of Chest Physical Therapy On Pediatrics Hospitalized With Pneumonia PDFandina100% (1)