You might also like
- Common Disorde Rs in ChildrenDocument172 pagesCommon Disorde Rs in Childrenblacklilha100% (1)
- Glue Ear, (Otitis Media with Effusion) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGlue Ear, (Otitis Media with Effusion) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cairo: Pilbeam's Mechanical Ventilation, 6th EditionDocument7 pagesCairo: Pilbeam's Mechanical Ventilation, 6th EditionLesly Peinado Torres100% (1)
- Pulmonary and Respiratory Nursing Assessment GuideDocument48 pagesPulmonary and Respiratory Nursing Assessment GuideEmjay JapitanaNo ratings yet
- Pulmonary TB RadiologyDocument45 pagesPulmonary TB RadiologyArina Windri RivartiNo ratings yet
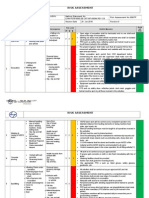
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Upper Respiratory Infections: Symptoms and TreatmentsDocument45 pagesUpper Respiratory Infections: Symptoms and TreatmentsNatasha Abdulla100% (2)
- Grief & Grieving ProcessDocument39 pagesGrief & Grieving Processelmerconde100% (4)
- Nursing Care of A Child With Respiratory DisorderDocument85 pagesNursing Care of A Child With Respiratory DisorderChris CharzNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- Respiratory DisordersDocument69 pagesRespiratory DisordersمشاعرمبعثرةNo ratings yet
- Respiratorydisease 170426125838Document69 pagesRespiratorydisease 170426125838Hayder MaqsadNo ratings yet
- Acute Respiratory Infection in ChildrenDocument70 pagesAcute Respiratory Infection in Childrenmayadwintas100% (1)
- Tung DocumentreviewDocument8 pagesTung DocumentreviewRodrigo Bittencourt100% (3)
- Otitis MediaDocument11 pagesOtitis MediajessyNo ratings yet
- 12 Otitis MediaDocument19 pages12 Otitis MediaCabdiNo ratings yet
- Nursing Management of Children With Respiratory System DysfunctionsDocument27 pagesNursing Management of Children With Respiratory System DysfunctionsDody ZainNo ratings yet
- Resp System KoleyaDocument96 pagesResp System KoleyaAlberto MeroNo ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- ChestDocument46 pagesChestNokatNo ratings yet
- Respiratory Tract Infection PDFDocument64 pagesRespiratory Tract Infection PDFMaretah TaufahNo ratings yet
- Acute Respiratory InfectionDocument9 pagesAcute Respiratory InfectionStephen FoxNo ratings yet
- Pediatric Airway Disorders and Parenchymal Lung DiseaseDocument10 pagesPediatric Airway Disorders and Parenchymal Lung DiseasePuma ChanNo ratings yet
- Acute Respiratory InfectionsDocument50 pagesAcute Respiratory InfectionsLinus PuleNo ratings yet
- Respiratory System of ChildrenDocument39 pagesRespiratory System of Childrenzoro4631No ratings yet
- NRSG 364 - Respiratory DisordersDocument65 pagesNRSG 364 - Respiratory DisordersJoanNo ratings yet
- Disorders of Thhe Lower Respiratory TractDocument18 pagesDisorders of Thhe Lower Respiratory TractLiecel ValdezNo ratings yet
- Nursing care for respiratory infections in children at Suez Canal University HospitalDocument20 pagesNursing care for respiratory infections in children at Suez Canal University HospitalAhmed SanadNo ratings yet
- Respiratory System DisordersDocument9 pagesRespiratory System Disordersasop06No ratings yet
- Acute CoughDocument14 pagesAcute CoughMerna MahrousNo ratings yet
- URI-ppt 03Document111 pagesURI-ppt 03tinsjohnNo ratings yet
- Treat Acute Chronic Ear InfectionsDocument32 pagesTreat Acute Chronic Ear InfectionsAndrew KaumbaNo ratings yet
- ASTHMA IN CHILDRENDocument5 pagesASTHMA IN CHILDRENRenjie ElizardeNo ratings yet
- عرض تقديميDocument19 pagesعرض تقديميJust muhannad AlharbiNo ratings yet
- Otitis Media I. Overview/DefinitionDocument10 pagesOtitis Media I. Overview/DefinitionBiancaGabatinoAbarcaNo ratings yet
- ALRI Control ProgrammeDocument20 pagesALRI Control ProgrammeDr.G.Bhanu PrakashNo ratings yet
- Acute Respiratory Infections in ChildrenDocument4 pagesAcute Respiratory Infections in ChildrenAxmeg YmapNo ratings yet
- Otitis Media: Prepared By: - Priyanka ThapaDocument38 pagesOtitis Media: Prepared By: - Priyanka ThapaKalo kajiNo ratings yet
- أطفال نظري 7Document23 pagesأطفال نظري 7حسين علي سلطانNo ratings yet
- Respi SDG Cluster3Document45 pagesRespi SDG Cluster3faye kimNo ratings yet
- Lesson Notes On UrtiDocument9 pagesLesson Notes On UrtiNeethupaulNo ratings yet
- MK BronchiolitisDocument6 pagesMK BronchiolitisMoses Jr Kazevu100% (1)
- Pubdoc 4 14280 150Document6 pagesPubdoc 4 14280 150jadarcNo ratings yet
- Alvin M. Hernandez, RN, RM, MSN, Man Faculty, School of NursingDocument37 pagesAlvin M. Hernandez, RN, RM, MSN, Man Faculty, School of NursingkathnlscNo ratings yet
- Online Learning ModuleDocument38 pagesOnline Learning ModuleMani SainiNo ratings yet
- File 18585Document15 pagesFile 18585Mohammed MuthanaNo ratings yet
- Bronchiolitis - Dr. IonescuDocument30 pagesBronchiolitis - Dr. IonescuArleen MatincaNo ratings yet
- Whooping Cough: Dr. MwendwaDocument39 pagesWhooping Cough: Dr. MwendwaAlvin OmondiNo ratings yet
- Wheezy Chest: Causes of Acute Respiratory Distress in An InfantDocument17 pagesWheezy Chest: Causes of Acute Respiratory Distress in An InfantMerna MahrousNo ratings yet
- Pneumonia 10Document13 pagesPneumonia 10Dina M Elbakary100% (1)
- SEO-Optimized Title for Febrile Seizures and Ear Infection DocumentDocument6 pagesSEO-Optimized Title for Febrile Seizures and Ear Infection DocumentKirstin del CarmenNo ratings yet
- Path o Physiology TablesDocument4 pagesPath o Physiology TablesRose Athena SibalaNo ratings yet
- SinusitisDocument23 pagesSinusitisMumin Alamin AllaminNo ratings yet
- PneumoniaDocument22 pagesPneumoniaNyakie MotlalaneNo ratings yet
- P 3 The Upper Respiratory Tract 2Document61 pagesP 3 The Upper Respiratory Tract 2Christelle CilliersNo ratings yet
- Jordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryDocument11 pagesJordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryJordan Abosama MamalumpongNo ratings yet
- Upper Airway Obstruction Causes and TreatmentDocument5 pagesUpper Airway Obstruction Causes and TreatmentAli Abd AlrezaqNo ratings yet
- Nursing Care for Ear, Nose and Throat InfectionsDocument8 pagesNursing Care for Ear, Nose and Throat Infectionsمحمد سعد طه احمدNo ratings yet
- Pneumonia in ChildrenDocument11 pagesPneumonia in ChildrenReni April AnaNo ratings yet
- Headaches & TMJ: Ari SudarsonoDocument160 pagesHeadaches & TMJ: Ari SudarsonoIsnaenyEraKartikaNo ratings yet
- Recurrent Wheeze in Pre-School Children: Respiratory MedicineDocument5 pagesRecurrent Wheeze in Pre-School Children: Respiratory MedicinejprakashjjNo ratings yet
- Care Plan FaringitisDocument63 pagesCare Plan FaringitisEnerolisa ParedesNo ratings yet
- Basog - ReportTonsillitis and EpistaxisDocument4 pagesBasog - ReportTonsillitis and EpistaxisclaribelleNo ratings yet
- Respiratory System 2017 PDFDocument158 pagesRespiratory System 2017 PDFdarla ryanNo ratings yet
- Diseases of Upper Respiratory System (URTI) : DR Sarwar Hussain, Assistant Professor Department of Pediatrics, NBUDocument36 pagesDiseases of Upper Respiratory System (URTI) : DR Sarwar Hussain, Assistant Professor Department of Pediatrics, NBUخالد مطرNo ratings yet
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- Week 15 - ONCO COURSE TASK - Breast Cancer DetectionDocument3 pagesWeek 15 - ONCO COURSE TASK - Breast Cancer DetectionGelo AlonzoNo ratings yet
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet
- Ultrasound-Guided Lumbar Central Neuraxial Block 2016Document8 pagesUltrasound-Guided Lumbar Central Neuraxial Block 2016drkis20100% (1)
- Persuasive Speech TextDocument2 pagesPersuasive Speech TextAnindya Azzahra0% (1)
- List of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atDocument2 pagesList of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atAdegokeNo ratings yet
- 4) Skema Set 1Document10 pages4) Skema Set 1Raymond Cheang Chee-CheongNo ratings yet
- Preface: Color Profile: Disabled Composite Default ScreenDocument2 pagesPreface: Color Profile: Disabled Composite Default ScreenCláudio CastroNo ratings yet
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- Psychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyDocument69 pagesPsychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyGokushimakNo ratings yet
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
- Apply teacher short leaveDocument1 pageApply teacher short leaveJean Claudine MandayNo ratings yet
- Affidavit of Accident Dominador Rosario BagamaspadDocument2 pagesAffidavit of Accident Dominador Rosario BagamaspadJaime GonzalesNo ratings yet
- OSHA Illness Injury Incidence RatesDocument2 pagesOSHA Illness Injury Incidence RatesGebshet WoldetsadikNo ratings yet
- Travel Guide to Thailand in 2021Document14 pagesTravel Guide to Thailand in 2021Russell KhanNo ratings yet
- CIS ParentDocument2 pagesCIS ParentAbegail (Abby) MirandaNo ratings yet
- PDF Biaya MaternityDocument2 pagesPDF Biaya MaternityKurnia Yuliyanti RahayuNo ratings yet
- DISC2-14071 AppealLetter PublicCommentsDocument17 pagesDISC2-14071 AppealLetter PublicCommentsJames ParsonsNo ratings yet
- The30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Document17 pagesThe30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Alexander OrzocoNo ratings yet
- Avulsi Dan Degloving Injury Dr. LuthfiDocument26 pagesAvulsi Dan Degloving Injury Dr. Luthfimutiara firdausyNo ratings yet
- The Northern Ireland Sport and Physical Activity Survey 2010 (SAPAS)Document178 pagesThe Northern Ireland Sport and Physical Activity Survey 2010 (SAPAS)sportniNo ratings yet
- MSDS for Feldspar PowderDocument7 pagesMSDS for Feldspar PowderRıdvan SürmeliNo ratings yet
- Grain Legumes/Pulses Introduction and ImportanceDocument5 pagesGrain Legumes/Pulses Introduction and ImportancesumandhakalNo ratings yet
- Young InfantDocument69 pagesYoung InfantAurora Doris BatagaNo ratings yet
- 2023 AHAR: PIT Estimates of Homelessness in The U.S.Document117 pages2023 AHAR: PIT Estimates of Homelessness in The U.S.Santiago Adolfo OspitalNo ratings yet