You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Connection ApplicationDocument35 pagesConnection ApplicationLeo KhkNo ratings yet
- Product Catalogue: Atlas Copco Ground Engineering ProductsDocument40 pagesProduct Catalogue: Atlas Copco Ground Engineering ProductshamidNo ratings yet
- Genomic Report MRIN 2015Document15 pagesGenomic Report MRIN 2015Jessica AdhykaNo ratings yet
- Fungal PneumoniaDocument8 pagesFungal PneumoniaJessica AdhykaNo ratings yet
- Murmur: CausesDocument21 pagesMurmur: CausesJessica AdhykaNo ratings yet
- Hirsutism: SymptomsDocument4 pagesHirsutism: SymptomsJessica AdhykaNo ratings yet
- General PharmacologyDocument5 pagesGeneral PharmacologyJessica AdhykaNo ratings yet
- LO Week 4Document6 pagesLO Week 4Jessica AdhykaNo ratings yet
- Wayne'S Index: - Showing The Scoring of Signs and Symptoms For The Diagnosis of HypothyroidismDocument3 pagesWayne'S Index: - Showing The Scoring of Signs and Symptoms For The Diagnosis of HypothyroidismJessica AdhykaNo ratings yet
- Adult Glasgow Coma Scale: Traumatic Brain InjuryDocument5 pagesAdult Glasgow Coma Scale: Traumatic Brain InjuryJessica AdhykaNo ratings yet
- Diplopia (Double Vision) : BackgroundDocument4 pagesDiplopia (Double Vision) : BackgroundJessica AdhykaNo ratings yet
- Anatomy of Hand and Wrist: Cartilage Which Helps MovementDocument10 pagesAnatomy of Hand and Wrist: Cartilage Which Helps MovementJessica AdhykaNo ratings yet
- Bones of The KneeDocument5 pagesBones of The KneeJessica AdhykaNo ratings yet
- Observer Reliability in The Arthroscopic Classification of Osteoarthritis of The KneeDocument1 pageObserver Reliability in The Arthroscopic Classification of Osteoarthritis of The KneeJessica AdhykaNo ratings yet
- Osteoarthtritis Symptoms: Older Age. The Risk of Osteoarthritis Increases With AgeDocument4 pagesOsteoarthtritis Symptoms: Older Age. The Risk of Osteoarthritis Increases With AgeJessica AdhykaNo ratings yet
- Short Stories Present SimpleDocument2 pagesShort Stories Present SimpleDavid TovarNo ratings yet
- Analisis Proses Pelaksanaan Anggaran Dana Bantuan Operasional Kesehatan (Bok) Pada Dinas Kesehatan Kabupaten BuolDocument11 pagesAnalisis Proses Pelaksanaan Anggaran Dana Bantuan Operasional Kesehatan (Bok) Pada Dinas Kesehatan Kabupaten BuolAyunDa RahayuNo ratings yet
- IBM x3850X5 x3950X5 HX5 OverviewDocument118 pagesIBM x3850X5 x3950X5 HX5 OverviewTruong Anh VuNo ratings yet
- Atmel-megaAVR-ATmega48-Learning Centre MCU-Application Notes-Atmel - Application - Notes - 30 PDFDocument4 pagesAtmel-megaAVR-ATmega48-Learning Centre MCU-Application Notes-Atmel - Application - Notes - 30 PDFMaPitufinaNo ratings yet
- Journal of Krishi Vigyan Vol 7 Issue 2Document293 pagesJournal of Krishi Vigyan Vol 7 Issue 2Dr. MANOJ SHARMANo ratings yet
- Comprehension ExamDocument16 pagesComprehension ExamAyanangshu ChakrabartyNo ratings yet
- INTERCHANGE 1 - Units 5-8 Review: Read The Answer. Then Complete The QuestionsDocument4 pagesINTERCHANGE 1 - Units 5-8 Review: Read The Answer. Then Complete The QuestionsLaureano GeraldoNo ratings yet
- Lab 1.5.2 - Basic Router ConfigurationDocument4 pagesLab 1.5.2 - Basic Router Configurationvictor teopezNo ratings yet
- Lesson 4 - The Receptive Skills WritingDocument14 pagesLesson 4 - The Receptive Skills Writingkimgabriel723No ratings yet
- E-Lock: Digital Signature SolutionsDocument4 pagesE-Lock: Digital Signature SolutionsSuchit KumarNo ratings yet
- 3Document24 pages3Iris Bustamante PájaroNo ratings yet
- Suction Strainer Boxes: Standard Specification ForDocument5 pagesSuction Strainer Boxes: Standard Specification ForKevin JosueNo ratings yet
- Efficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic ReviewDocument10 pagesEfficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic ReviewFerryGoNo ratings yet
- Responsibility Accounting: Acc 7 - Management Consultancy Test BankDocument12 pagesResponsibility Accounting: Acc 7 - Management Consultancy Test BankHiraya ManawariNo ratings yet
- Acid Bases and SaltsDocument6 pagesAcid Bases and Saltsasma asifNo ratings yet
- Paradise Datacom Outdoor-Redundant SSPA 209495 RevADocument9 pagesParadise Datacom Outdoor-Redundant SSPA 209495 RevAarzeszutNo ratings yet
- Larkey Ray Dotson ResumeDocument2 pagesLarkey Ray Dotson Resumeapi-510181676No ratings yet
- Hydraulic Hammer Operators Manual: GH Series HammersDocument71 pagesHydraulic Hammer Operators Manual: GH Series HammersmarceloNo ratings yet
- WJGEv 4 I 6Document82 pagesWJGEv 4 I 6Duane BrooksNo ratings yet
- Ii. Functions: Trust?Document6 pagesIi. Functions: Trust?Jeffrey Garcia IlaganNo ratings yet
- Indian Oil Corporation Limited Panipat Refinery & Petrochemical ComplexDocument2 pagesIndian Oil Corporation Limited Panipat Refinery & Petrochemical ComplexSomnath Das YTNo ratings yet
- Business Vocabulary RoundDocument9 pagesBusiness Vocabulary RoundAndrei-Alexandru VasiloviciNo ratings yet
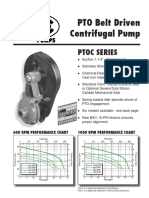
- Ptoc 03-13Document4 pagesPtoc 03-13Matias Contreras KöbrichNo ratings yet
- The Volatile Oil of Ziziphora: HispanicaDocument3 pagesThe Volatile Oil of Ziziphora: HispanicaРусланNo ratings yet
- DESIDOC Journal of Library & Information Technology, Vol. 31, No. 2, March 2011, Pp. 116-120 © 2011, DESIDOCDocument5 pagesDESIDOC Journal of Library & Information Technology, Vol. 31, No. 2, March 2011, Pp. 116-120 © 2011, DESIDOCanon_69363824No ratings yet
- Scentsy Layers Ingrediants ListDocument16 pagesScentsy Layers Ingrediants ListsimonejanesNo ratings yet
- Thesis Topics List PhilippinesDocument5 pagesThesis Topics List Philippinesfc5wsq30100% (2)
- Iec Solar Yaan Merged - CompressedDocument3 pagesIec Solar Yaan Merged - CompressedVINAY ARORANo ratings yet