100% found this document useful (1 vote)
7K views1 pagePPN Hospital Declaration Form
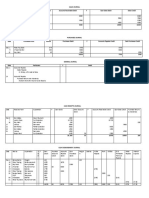
This document contains a declaration by a patient or patient's attendant regarding their insurance policy and treatment options at a hospital. It includes sections for declaring whether the patient has an insurance policy or not. If they do have a policy, it requests the policy number and insurance company. It also asks if the patient has opted for the eligible room category under their policy. Finally, it contains a declaration where the patient agrees to pay for any additional facilities, procedures, or treatments not covered by their insurance policy.
Uploaded by
Anup SrivastavaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
100% found this document useful (1 vote)
7K views1 pagePPN Hospital Declaration Form
This document contains a declaration by a patient or patient's attendant regarding their insurance policy and treatment options at a hospital. It includes sections for declaring whether the patient has an insurance policy or not. If they do have a policy, it requests the policy number and insurance company. It also asks if the patient has opted for the eligible room category under their policy. Finally, it contains a declaration where the patient agrees to pay for any additional facilities, procedures, or treatments not covered by their insurance policy.
Uploaded by
Anup SrivastavaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
- PPN Network Declaration Form