You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Angina Pectoris & Anti Anginal DrugsDocument46 pagesAngina Pectoris & Anti Anginal DrugsMohammad AliNo ratings yet
- Angina PectorisDocument38 pagesAngina Pectorisekhafagy100% (1)
- A ListaDocument31 pagesA Listaking_petarNo ratings yet
- Kelompok 16 PBL CVSDocument11 pagesKelompok 16 PBL CVSTutde SedanaNo ratings yet
- Shabrina Maharani, Laporan Kasus Seminar, NSTEMIDocument3 pagesShabrina Maharani, Laporan Kasus Seminar, NSTEMIShabrina MaharaniNo ratings yet
- Acut Coronary SyndromeDocument65 pagesAcut Coronary SyndromeArys SetiawanNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- Curriculum VitaeDocument6 pagesCurriculum Vitaejenishajestin755No ratings yet
- Skor Resiko TIMI Untuk UADocument1 pageSkor Resiko TIMI Untuk UAGusnella IswardhaniNo ratings yet
- Unit 2 Pathophysiology Carewell PharmaDocument23 pagesUnit 2 Pathophysiology Carewell Pharmaakshay dhootNo ratings yet
- Cardiac Emergency PDFDocument45 pagesCardiac Emergency PDFnikenNo ratings yet
- Loog Book Kardiologi Khusus-1Document8 pagesLoog Book Kardiologi Khusus-1marjuwarNo ratings yet
- Perhitungan Kuda-Kuda Kayu Bentang 3m - RevisiDocument33 pagesPerhitungan Kuda-Kuda Kayu Bentang 3m - RevisideviNo ratings yet
- Seattle Angina Questionnaire - Google SearchDocument1 pageSeattle Angina Questionnaire - Google SearchAbhishek SikarwarNo ratings yet
- Daftar Diagnosis Dan Kode BPJSDocument18 pagesDaftar Diagnosis Dan Kode BPJSeginagirsangNo ratings yet
- Cardiovascular Disease by SlidesgoDocument32 pagesCardiovascular Disease by SlidesgoIPD STASENo ratings yet
- Angina: CausesDocument12 pagesAngina: CausesM KashifNo ratings yet
- Sensus Icvcu 08.09.2021Document1 pageSensus Icvcu 08.09.2021Raka MahasaduNo ratings yet
- Daftar Pustaka: Universitas Sumatera UtaraDocument2 pagesDaftar Pustaka: Universitas Sumatera UtaraNavisa HaifaNo ratings yet
- Acs - Esc 2023 - BsquangDocument18 pagesAcs - Esc 2023 - BsquangHuy PhạmNo ratings yet
- Daftar Pustaka: Medical Students and Faculty - Edisi Keempat - Baltimore-PhiladelpiaDocument2 pagesDaftar Pustaka: Medical Students and Faculty - Edisi Keempat - Baltimore-PhiladelpiaSylvia PertiwiNo ratings yet
- The Romanian Society of Cardiology BoardDocument4 pagesThe Romanian Society of Cardiology Boardmyreille_mNo ratings yet
- IHDDocument34 pagesIHDElly Msi ProbolinggoNo ratings yet
- Antianginal Drugs: Dr. Jim AmisiDocument11 pagesAntianginal Drugs: Dr. Jim AmisiMike AnnisNo ratings yet
- DR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanDocument50 pagesDR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanHabib Al KahfiNo ratings yet
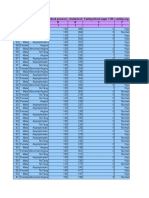
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I IDocument14 pagesAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I Isantu4_1111No ratings yet
- Introducere in Cardiologie: Prof. Maria DOROBANTUDocument33 pagesIntroducere in Cardiologie: Prof. Maria DOROBANTUSolomon VioletaNo ratings yet
- Angina Set #8Document26 pagesAngina Set #8Zaid Al-KadhimiNo ratings yet
- Diagnostik Dan Tatalaksana Stable CAD - CCSDocument38 pagesDiagnostik Dan Tatalaksana Stable CAD - CCSIno HajrinNo ratings yet
- MANIFESTASI KLINIK Penyakit Jantung KoronerDocument4 pagesMANIFESTASI KLINIK Penyakit Jantung KoronerDwitya NoviariNo ratings yet