
Electrolytes Notes PDF
Electrolytes Notes PDF
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
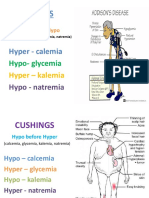
- Addison's Disease vs. Cushing SyndromeDocument2 pagesAddison's Disease vs. Cushing Syndromedecsag06100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pathology - Chapter 4Document9 pagesPathology - Chapter 4Cory GrayNo ratings yet
- Emergency and Disaster NursingDocument144 pagesEmergency and Disaster Nursingdecsag06No ratings yet
- Exit and NCLEX Examination Study Guide PDFDocument158 pagesExit and NCLEX Examination Study Guide PDFdecsag06100% (4)
- 160 Nursing Bullets - Medical Surgical NursingDocument7 pages160 Nursing Bullets - Medical Surgical Nursingdecsag06No ratings yet
- A Case Presentation of An Adult With Gestational Diabetes Mellitus FinalDocument59 pagesA Case Presentation of An Adult With Gestational Diabetes Mellitus FinalJM PunzalanNo ratings yet
- Respiratory SystemDocument32 pagesRespiratory Systemapi-202513022No ratings yet
- Cardiovascular System Acronyms and MnemonicsDocument18 pagesCardiovascular System Acronyms and Mnemonicsdecsag06No ratings yet
- Common Diseases in NCLEXDocument15 pagesCommon Diseases in NCLEXdecsag06No ratings yet
- Cheat Sheet - Growth and DevelopmentDocument4 pagesCheat Sheet - Growth and Developmentdecsag06No ratings yet
- Burn Stage I - PathophysiologyDocument1 pageBurn Stage I - Pathophysiologydecsag06No ratings yet
- Menopause: District I ACOG Medical Student Education Module 2009Document10 pagesMenopause: District I ACOG Medical Student Education Module 2009decsag06No ratings yet
- Pediatric Nursing NotesDocument21 pagesPediatric Nursing NotesFaye Nervanna Alecha AlferezNo ratings yet
- A Maternal and Child's Nurses Quest Towards ExcellenceDocument78 pagesA Maternal and Child's Nurses Quest Towards Excellencedecsag06No ratings yet
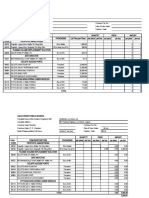
- Item Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item CodeDocument3 pagesItem Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item Codedecsag06No ratings yet
- Item Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item CodeDocument3 pagesItem Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item Codedecsag06No ratings yet
- Midterms - Nervous SystemDocument6 pagesMidterms - Nervous SystemStella Maris PenetranteNo ratings yet
- Horizontal Jaw RelationDocument101 pagesHorizontal Jaw Relationruchika0% (1)
- Infant of Diabetic MotherDocument14 pagesInfant of Diabetic MothersreekalaNo ratings yet
- Edexcel A2 IAL Biology: Topic 8 - Grey MatterDocument24 pagesEdexcel A2 IAL Biology: Topic 8 - Grey MatterErin100% (1)
- Meristematic TissueDocument10 pagesMeristematic TissueSangam G.CNo ratings yet
- Regulating Growth and Development The Plant HormonesDocument30 pagesRegulating Growth and Development The Plant HormonesMoath EnnabNo ratings yet
- General Biology 2 Reproductive SystemDocument4 pagesGeneral Biology 2 Reproductive SystemAnjhiene Camba100% (1)
- Neusci 302 Oral Presentation - Briana Katie LizzyDocument16 pagesNeusci 302 Oral Presentation - Briana Katie Lizzyapi-340131743No ratings yet
- Kuliah 8. Safety Handling of Infusion ProductDocument63 pagesKuliah 8. Safety Handling of Infusion ProductElva SorumbaNo ratings yet
- Lecture 6 Special Senses Part 1-VisionDocument47 pagesLecture 6 Special Senses Part 1-VisionMoses Jr KazevuNo ratings yet
- Case Study On Meninomyocele (Repaired) PDocument29 pagesCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Importance of Proteins in Living OrganismsDocument2 pagesImportance of Proteins in Living OrganismsChris Wills0% (1)
- Strength, Muscular Endurance, and Power in Sports: by Tudor O. Bompa, PHDDocument11 pagesStrength, Muscular Endurance, and Power in Sports: by Tudor O. Bompa, PHDWijaya Krisna I NyomanNo ratings yet
- Cycas Leaflet and Rachis 17.05.24Document4 pagesCycas Leaflet and Rachis 17.05.24Atashi MandalNo ratings yet
- BIO2133 NotesDocument20 pagesBIO2133 NotesSammie TdtNo ratings yet
- Exercise Physiologist Sample ResumeDocument2 pagesExercise Physiologist Sample ResumesooriroyNo ratings yet
- Cluster 4 Close Door 2022Document53 pagesCluster 4 Close Door 2022RadTech ReviewerNo ratings yet
- ICSE Board Class VI Biology Sample Paper - 1: Time: 2 Hrs Total Marks: 75 General InstructionsDocument6 pagesICSE Board Class VI Biology Sample Paper - 1: Time: 2 Hrs Total Marks: 75 General InstructionsSubhadip SarkarNo ratings yet
- Devarajan, Dss DGN ArdsDocument4 pagesDevarajan, Dss DGN ArdsrantiadrianiNo ratings yet
- OVEMP en Equipo EclipseDocument2 pagesOVEMP en Equipo EclipsePedro César Saavedra MartínezNo ratings yet
- Nnate Mmune Ecognition: Charles A. Janeway, Jr. and Ruslan MedzhitovDocument22 pagesNnate Mmune Ecognition: Charles A. Janeway, Jr. and Ruslan MedzhitovMaximeNo ratings yet
- What Makes Animal Cells DifferentDocument14 pagesWhat Makes Animal Cells DifferentGian Carlo Angon100% (1)
- Heat and Cold ApplicationDocument5 pagesHeat and Cold ApplicationBern NerquitNo ratings yet
- Become Fearless TrainingDocument35 pagesBecome Fearless TrainingsonyammmmNo ratings yet
- Barium MealDocument3 pagesBarium MealYusra Shafiq AhmedNo ratings yet
- Laporan Praktikum Fisiologi Sistem Muskuloskeletal: Nama:Nursyam NIM:R011211035 Kelompok:04 Asisten:Michael PinartoDocument31 pagesLaporan Praktikum Fisiologi Sistem Muskuloskeletal: Nama:Nursyam NIM:R011211035 Kelompok:04 Asisten:Michael PinartoIcha NursyamNo ratings yet
- Answers & Solutions: For For For For ForDocument19 pagesAnswers & Solutions: For For For For ForAlokSinghNo ratings yet

















































































You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Addison's Disease vs. Cushing SyndromeDocument2 pagesAddison's Disease vs. Cushing Syndromedecsag06100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pathology - Chapter 4Document9 pagesPathology - Chapter 4Cory GrayNo ratings yet
- Emergency and Disaster NursingDocument144 pagesEmergency and Disaster Nursingdecsag06No ratings yet
- Exit and NCLEX Examination Study Guide PDFDocument158 pagesExit and NCLEX Examination Study Guide PDFdecsag06100% (4)
- 160 Nursing Bullets - Medical Surgical NursingDocument7 pages160 Nursing Bullets - Medical Surgical Nursingdecsag06No ratings yet
- A Case Presentation of An Adult With Gestational Diabetes Mellitus FinalDocument59 pagesA Case Presentation of An Adult With Gestational Diabetes Mellitus FinalJM PunzalanNo ratings yet
- Respiratory SystemDocument32 pagesRespiratory Systemapi-202513022No ratings yet
- Cardiovascular System Acronyms and MnemonicsDocument18 pagesCardiovascular System Acronyms and Mnemonicsdecsag06No ratings yet
- Common Diseases in NCLEXDocument15 pagesCommon Diseases in NCLEXdecsag06No ratings yet
- Cheat Sheet - Growth and DevelopmentDocument4 pagesCheat Sheet - Growth and Developmentdecsag06No ratings yet
- Burn Stage I - PathophysiologyDocument1 pageBurn Stage I - Pathophysiologydecsag06No ratings yet
- Menopause: District I ACOG Medical Student Education Module 2009Document10 pagesMenopause: District I ACOG Medical Student Education Module 2009decsag06No ratings yet
- Pediatric Nursing NotesDocument21 pagesPediatric Nursing NotesFaye Nervanna Alecha AlferezNo ratings yet
- A Maternal and Child's Nurses Quest Towards ExcellenceDocument78 pagesA Maternal and Child's Nurses Quest Towards Excellencedecsag06No ratings yet
- Item Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item CodeDocument3 pagesItem Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item Codedecsag06No ratings yet
- Item Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item CodeDocument3 pagesItem Despcription Packaging List Price Per Piece Per Piece Per Box Propofol Anaesthesia Item Codedecsag06No ratings yet
- Midterms - Nervous SystemDocument6 pagesMidterms - Nervous SystemStella Maris PenetranteNo ratings yet
- Horizontal Jaw RelationDocument101 pagesHorizontal Jaw Relationruchika0% (1)
- Infant of Diabetic MotherDocument14 pagesInfant of Diabetic MothersreekalaNo ratings yet
- Edexcel A2 IAL Biology: Topic 8 - Grey MatterDocument24 pagesEdexcel A2 IAL Biology: Topic 8 - Grey MatterErin100% (1)
- Meristematic TissueDocument10 pagesMeristematic TissueSangam G.CNo ratings yet
- Regulating Growth and Development The Plant HormonesDocument30 pagesRegulating Growth and Development The Plant HormonesMoath EnnabNo ratings yet
- General Biology 2 Reproductive SystemDocument4 pagesGeneral Biology 2 Reproductive SystemAnjhiene Camba100% (1)
- Neusci 302 Oral Presentation - Briana Katie LizzyDocument16 pagesNeusci 302 Oral Presentation - Briana Katie Lizzyapi-340131743No ratings yet
- Kuliah 8. Safety Handling of Infusion ProductDocument63 pagesKuliah 8. Safety Handling of Infusion ProductElva SorumbaNo ratings yet
- Lecture 6 Special Senses Part 1-VisionDocument47 pagesLecture 6 Special Senses Part 1-VisionMoses Jr KazevuNo ratings yet
- Case Study On Meninomyocele (Repaired) PDocument29 pagesCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Importance of Proteins in Living OrganismsDocument2 pagesImportance of Proteins in Living OrganismsChris Wills0% (1)
- Strength, Muscular Endurance, and Power in Sports: by Tudor O. Bompa, PHDDocument11 pagesStrength, Muscular Endurance, and Power in Sports: by Tudor O. Bompa, PHDWijaya Krisna I NyomanNo ratings yet
- Cycas Leaflet and Rachis 17.05.24Document4 pagesCycas Leaflet and Rachis 17.05.24Atashi MandalNo ratings yet
- BIO2133 NotesDocument20 pagesBIO2133 NotesSammie TdtNo ratings yet
- Exercise Physiologist Sample ResumeDocument2 pagesExercise Physiologist Sample ResumesooriroyNo ratings yet
- Cluster 4 Close Door 2022Document53 pagesCluster 4 Close Door 2022RadTech ReviewerNo ratings yet
- ICSE Board Class VI Biology Sample Paper - 1: Time: 2 Hrs Total Marks: 75 General InstructionsDocument6 pagesICSE Board Class VI Biology Sample Paper - 1: Time: 2 Hrs Total Marks: 75 General InstructionsSubhadip SarkarNo ratings yet
- Devarajan, Dss DGN ArdsDocument4 pagesDevarajan, Dss DGN ArdsrantiadrianiNo ratings yet
- OVEMP en Equipo EclipseDocument2 pagesOVEMP en Equipo EclipsePedro César Saavedra MartínezNo ratings yet
- Nnate Mmune Ecognition: Charles A. Janeway, Jr. and Ruslan MedzhitovDocument22 pagesNnate Mmune Ecognition: Charles A. Janeway, Jr. and Ruslan MedzhitovMaximeNo ratings yet
- What Makes Animal Cells DifferentDocument14 pagesWhat Makes Animal Cells DifferentGian Carlo Angon100% (1)
- Heat and Cold ApplicationDocument5 pagesHeat and Cold ApplicationBern NerquitNo ratings yet
- Become Fearless TrainingDocument35 pagesBecome Fearless TrainingsonyammmmNo ratings yet
- Barium MealDocument3 pagesBarium MealYusra Shafiq AhmedNo ratings yet
- Laporan Praktikum Fisiologi Sistem Muskuloskeletal: Nama:Nursyam NIM:R011211035 Kelompok:04 Asisten:Michael PinartoDocument31 pagesLaporan Praktikum Fisiologi Sistem Muskuloskeletal: Nama:Nursyam NIM:R011211035 Kelompok:04 Asisten:Michael PinartoIcha NursyamNo ratings yet
- Answers & Solutions: For For For For ForDocument19 pagesAnswers & Solutions: For For For For ForAlokSinghNo ratings yet