You might also like
- Vince McMahon's Testimony To Waxman CommitteeDocument122 pagesVince McMahon's Testimony To Waxman Committeeestannard100% (2)
- Herbal Formula Ratios and Instructions by Puijo Anyujuliot Juurilattu (DIY Herbs For Detoxification and Regeneration Facebook Group)Document6 pagesHerbal Formula Ratios and Instructions by Puijo Anyujuliot Juurilattu (DIY Herbs For Detoxification and Regeneration Facebook Group)Ioanna Daskalaki100% (3)
- Somatic TherapiesDocument170 pagesSomatic TherapiesDelyn Gamutan Millan100% (2)
- Reiki Tips You Haven T Thought ofDocument35 pagesReiki Tips You Haven T Thought ofAnonymous 3gHvQv100% (3)
- Herbal Materia Medica 5th Ed. by Michael MooreDocument57 pagesHerbal Materia Medica 5th Ed. by Michael MooreIreneRains100% (3)
- D5050Document2 pagesD5050Emilie Jane Canilang100% (2)
- VasectomyDocument60 pagesVasectomyVlad ValentinNo ratings yet
- Dimenhydrinate PDFDocument2 pagesDimenhydrinate PDFWindy SengiNo ratings yet
- Reading Jahshan Oet CollectionDocument398 pagesReading Jahshan Oet CollectionMaria del CarmenNo ratings yet
- Brain Tumors A Pocket Guide Mohile 1 Ed 2023Document289 pagesBrain Tumors A Pocket Guide Mohile 1 Ed 2023martinus.urbanusNo ratings yet
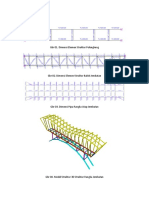
- Hitungan Struktur JembatanDocument51 pagesHitungan Struktur JembatanWindy SengiNo ratings yet
- Hitungan Struktur JembatanDocument51 pagesHitungan Struktur JembatanWindy SengiNo ratings yet
- Hitungan Struktur JembatanDocument51 pagesHitungan Struktur JembatanWindy SengiNo ratings yet
- Hitungan Struktur JembatanDocument51 pagesHitungan Struktur JembatanWindy SengiNo ratings yet
- Hitungan Struktur JembatanDocument51 pagesHitungan Struktur JembatanWindy SengiNo ratings yet
- 1r70omiDocument6 pages1r70omiKartini tenNo ratings yet
- Intrathymic Plasmablasts Are Affected in Patients With Myasthenia Gravis With Active DiseaseDocument10 pagesIntrathymic Plasmablasts Are Affected in Patients With Myasthenia Gravis With Active DiseaseValeria KuchkaryanNo ratings yet
- Thymo-Thyroid Associations Clinical and Pathological AspectsDocument46 pagesThymo-Thyroid Associations Clinical and Pathological AspectsRahmani Sofi726No ratings yet
- Review Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentDocument6 pagesReview Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentHeru SigitNo ratings yet
- Surgery in Hymoma and MGDocument11 pagesSurgery in Hymoma and MGHeru SigitNo ratings yet
- TiroDocument10 pagesTiroIoana CreangaNo ratings yet
- HEGI Et Al., 2005 - A1Document7 pagesHEGI Et Al., 2005 - A1Silvio OrtolanNo ratings yet
- Radio-Contrast Agent-Induced Hyperthyroidism: Case Report and Review of The LiteratureDocument3 pagesRadio-Contrast Agent-Induced Hyperthyroidism: Case Report and Review of The LiteratureIwan SaputeraNo ratings yet
- Successful Management of Granulocytic Sarcoma With Co - 2016 - Pediatric HematolDocument2 pagesSuccessful Management of Granulocytic Sarcoma With Co - 2016 - Pediatric HematolHawin NurdianaNo ratings yet
- A Case of Multiple Myeloma Misdiagnosed As Seronegative ARDocument6 pagesA Case of Multiple Myeloma Misdiagnosed As Seronegative ARRaíla SoaresNo ratings yet
- Art:10.1007/s00595 009 4134 2Document6 pagesArt:10.1007/s00595 009 4134 2Helen SobczykNo ratings yet
- Journal of Oral Science MGDocument9 pagesJournal of Oral Science MGVincia PaulNo ratings yet
- Acute Myeloid LeukemiaDocument33 pagesAcute Myeloid LeukemiardLuis1No ratings yet
- Thymoma: A Case Report and Review of The LiteratureDocument6 pagesThymoma: A Case Report and Review of The LiteratureArja' WaasNo ratings yet
- Current and Emerging Targets in ImmunotherapyDocument9 pagesCurrent and Emerging Targets in ImmunotherapyTika wahyuNo ratings yet
- Diferenças Neoplasia de Timo e Benignos Na TomografiaDocument21 pagesDiferenças Neoplasia de Timo e Benignos Na TomografiaJesus DecepcionadoNo ratings yet
- Tid 13506Document5 pagesTid 13506Jenny Mundaca QuirozNo ratings yet
- Myasthenic Crisis As A Side Effect of Methimazole Therapy: Case ReportDocument5 pagesMyasthenic Crisis As A Side Effect of Methimazole Therapy: Case ReportThein Htun NaungNo ratings yet
- Pi Is 0923753419453180Document2 pagesPi Is 0923753419453180alu0100537680No ratings yet
- Phase III trial of chemoradiotherapy with temozolomide plus nivolumab or placebo for newly diagnosed glioblastoma with methylated MGMT promoterDocument15 pagesPhase III trial of chemoradiotherapy with temozolomide plus nivolumab or placebo for newly diagnosed glioblastoma with methylated MGMT promoterCher IshNo ratings yet
- JurnalDocument8 pagesJurnalRyanNo ratings yet
- RT+TMZ JepangDocument6 pagesRT+TMZ JepangFaris HidayatNo ratings yet
- Hipotiroidismo Após Tireoidectomia ParcialDocument3 pagesHipotiroidismo Após Tireoidectomia ParcialporsanimedNo ratings yet
- MYELITISDocument8 pagesMYELITISFebrina RamadhaniNo ratings yet
- Evidence-Based Guideline: Clinical Evaluation and Treatment of Transverse MyelitisDocument8 pagesEvidence-Based Guideline: Clinical Evaluation and Treatment of Transverse MyelitisAnonymous V5l8nmcSxbNo ratings yet
- Immune Function in Children Under Chemotherapy For Standard Risk Acute Lymphoblastic Leukaemia - A Prospective Study of 20 Paediatric PatientsDocument11 pagesImmune Function in Children Under Chemotherapy For Standard Risk Acute Lymphoblastic Leukaemia - A Prospective Study of 20 Paediatric PatientsJOSE PORTILLONo ratings yet
- Struma Nodosa 2Document10 pagesStruma Nodosa 2dewi rositaNo ratings yet
- Tratament of Miastenia GravisDocument9 pagesTratament of Miastenia GravisAndres MardonesNo ratings yet
- 2011 Guias ClinicasDocument5 pages2011 Guias ClinicasJavier VegaNo ratings yet
- Successful MethotrexateDocument6 pagesSuccessful MethotrexateWinda HaeriyokoNo ratings yet
- Radiotherapy combined with nivolumab or temozolomide for newly diagnosed glioblastoma with unmethylated MGMT promoter- An international randomized phase III trialDocument12 pagesRadiotherapy combined with nivolumab or temozolomide for newly diagnosed glioblastoma with unmethylated MGMT promoter- An international randomized phase III trialCher IshNo ratings yet
- Tumor Microenvironment and Immune-Related Therapies of Head and Neck Squamous Cell CarcinomaDocument10 pagesTumor Microenvironment and Immune-Related Therapies of Head and Neck Squamous Cell CarcinomaSpore FluxNo ratings yet
- 2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRDocument2 pages2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRPoljarLijanNo ratings yet
- Grupo 5el TimoDocument11 pagesGrupo 5el TimoSantos Pardo GomezNo ratings yet
- Abnormal Memory T Cells Linked to Bone Marrow Failure in Aplastic AnemiaDocument11 pagesAbnormal Memory T Cells Linked to Bone Marrow Failure in Aplastic AnemiaArie kusuma WijayaNo ratings yet
- WWW - Kup.at/ Journals/eano/index - HTML: Systemic Treatment of Recurrent MeningiomaDocument8 pagesWWW - Kup.at/ Journals/eano/index - HTML: Systemic Treatment of Recurrent MeningiomaAnonymous KKqrboTNo ratings yet
- Myasthenia Gravis ReferenceDocument19 pagesMyasthenia Gravis ReferenceIka Wulan PermataNo ratings yet
- Triplet Chemotherapy For Malignant Pericardial Mesothelioma: A Case ReportDocument4 pagesTriplet Chemotherapy For Malignant Pericardial Mesothelioma: A Case ReportjamesyuNo ratings yet
- ANG2_Angiopoietin-2-dependent spatial vascular destabilization promotes T cell exclusion and limits immunotherapy in melanomaDocument51 pagesANG2_Angiopoietin-2-dependent spatial vascular destabilization promotes T cell exclusion and limits immunotherapy in melanomaCher IshNo ratings yet
- Myasthenia GravisDocument3 pagesMyasthenia GravisZakia AjaNo ratings yet
- Ni 05007Document4 pagesNi 05007crownesyaNo ratings yet
- Graves' Disease: Causes, Diagnosis and TreatmentDocument34 pagesGraves' Disease: Causes, Diagnosis and TreatmenthaidzarfathinNo ratings yet
- Jurnal Tiroid 5Document6 pagesJurnal Tiroid 5Faradilla NovaNo ratings yet
- Follow UpDocument6 pagesFollow UpWinda HaeriyokoNo ratings yet
- 77 FullDocument7 pages77 FulldjebrutNo ratings yet
- T Cell Lymphomas 2022 SlidesDocument62 pagesT Cell Lymphomas 2022 SlidesИван НегарэNo ratings yet
- Extracranial Metastases of Anaplastic Meningioma: Case ReportDocument6 pagesExtracranial Metastases of Anaplastic Meningioma: Case ReportRizky AdriansahNo ratings yet
- CLINICS 2019 - Adoptive T-Cell Therapy For Solid MalignanciesDocument15 pagesCLINICS 2019 - Adoptive T-Cell Therapy For Solid MalignanciesWilverCarbonelLuyoNo ratings yet
- Mesothelioma Environment Comprises Cytokines and T-Regulatory Cells That Suppress Immune ResponsesDocument10 pagesMesothelioma Environment Comprises Cytokines and T-Regulatory Cells That Suppress Immune ResponseshariompriyNo ratings yet
- Otomycosis Clinical Features, Predisposing Factors and Treatment ImplicationsDocument14 pagesOtomycosis Clinical Features, Predisposing Factors and Treatment ImplicationsVela NazarNo ratings yet
- Myasthenia GravisDocument47 pagesMyasthenia Gravismirabel IvanaliNo ratings yet
- 1299-2. Article Text - Manuscript-16811-2-10-20211031Document9 pages1299-2. Article Text - Manuscript-16811-2-10-20211031Syaputri SogenNo ratings yet
- Original Articles Gestational Trophoblastic Disease Following Complete Hydatidi-Form Mole in Mulago Hospital, Kampala, UgandaDocument5 pagesOriginal Articles Gestational Trophoblastic Disease Following Complete Hydatidi-Form Mole in Mulago Hospital, Kampala, UgandadianaristinugraheniNo ratings yet
- Tormenta Tiroidea: Una Urgencia Endocrinológica: Thyroid Storm: An Endocrinological UrgencyDocument4 pagesTormenta Tiroidea: Una Urgencia Endocrinológica: Thyroid Storm: An Endocrinological UrgencyConstanza Moraga HerreraNo ratings yet
- CML Treatment Outcomes in Trakya UniversityDocument5 pagesCML Treatment Outcomes in Trakya UniversityÇağlaNo ratings yet
- Frequent TERT Promoter Mutations in Ocular Surface Squamous NeoplasiaDocument8 pagesFrequent TERT Promoter Mutations in Ocular Surface Squamous NeoplasiaGlauce L TrevisanNo ratings yet
- Guidelines EuromyastheniaDocument4 pagesGuidelines Euromyastheniadokter mudaNo ratings yet
- A3 FullDocument2 pagesA3 FullApotik ApotekNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Hospital Design Considerations: Hurricane Katrina: The Public Health and Medical Response, Examined TheDocument32 pagesHospital Design Considerations: Hurricane Katrina: The Public Health and Medical Response, Examined ThePhorum PatelNo ratings yet
- Di Men Hydri NateDocument2 pagesDi Men Hydri NateWindy SengiNo ratings yet
- Katalog Obat Apotik RSUD Dr. TC Hillers: No Nama Obat Sediaan Kekuatan 1. Obat Nyeri Dan DemamDocument11 pagesKatalog Obat Apotik RSUD Dr. TC Hillers: No Nama Obat Sediaan Kekuatan 1. Obat Nyeri Dan DemamWindy SengiNo ratings yet
- International Consensus Guidance For Management of Myasthenia GravisDocument8 pagesInternational Consensus Guidance For Management of Myasthenia GravisWindy SengiNo ratings yet
- Myasthenia Gravis Guest LectureDocument43 pagesMyasthenia Gravis Guest LecturePatresya LantanNo ratings yet
- The Role of The Thymus in The Pathogenesis of Myasthenia GravisDocument12 pagesThe Role of The Thymus in The Pathogenesis of Myasthenia GravisWindy SengiNo ratings yet
- Otitis Externa: Continuing Medical EducationDocument12 pagesOtitis Externa: Continuing Medical EducationWindy SengiNo ratings yet
- Book IV Medicine (De Medicina)Document8 pagesBook IV Medicine (De Medicina)Marcus Annaeus LucanusNo ratings yet
- A Proposed Project of Zinbinger Officinale (Ginger) As An Ointment/Vapor Rub For Headache and Nasal CongestionDocument2 pagesA Proposed Project of Zinbinger Officinale (Ginger) As An Ointment/Vapor Rub For Headache and Nasal CongestionKaren PadillaNo ratings yet
- EKG Card 2Document2 pagesEKG Card 2mulyadiNo ratings yet
- Blocking Polyspermy and Pregnancy Tests ExplainedDocument13 pagesBlocking Polyspermy and Pregnancy Tests ExplainedHafizah ZakiahNo ratings yet
- Mania: Caring For A Person ExperiencingDocument6 pagesMania: Caring For A Person ExperiencingGutsy JewelNo ratings yet
- Medical Certificate For AthletesDocument2 pagesMedical Certificate For AthletesCaitlin PeñeraNo ratings yet
- Affidavit Form Medical Clinic Fire SafetyDocument2 pagesAffidavit Form Medical Clinic Fire SafetysrinivasuNo ratings yet
- Albumin Piggyback Procedure ChecklistDocument3 pagesAlbumin Piggyback Procedure ChecklistAljane VistoNo ratings yet
- Pediatric GI Diseases InsightsDocument25 pagesPediatric GI Diseases InsightsSai Kumar KonukuNo ratings yet
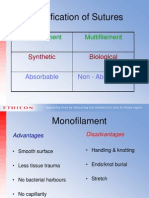
- Classification of Sutures: Monofilament MultifilamentDocument17 pagesClassification of Sutures: Monofilament Multifilamentlina_m354No ratings yet
- Ef310 Unit 08 Client Assessment Matrix Fitt Pros-3Document6 pagesEf310 Unit 08 Client Assessment Matrix Fitt Pros-3api-295146168No ratings yet
- 3 NsaidsDocument23 pages3 NsaidsHagai MagaiNo ratings yet
- 1 Bullets Pain & orDocument7 pages1 Bullets Pain & orAnne Mae PaculaNo ratings yet
- Register Meranti 2018Document178 pagesRegister Meranti 2018Rifat Bow AbdilahNo ratings yet
- Medico-legal aspects of wounds classificationDocument16 pagesMedico-legal aspects of wounds classificationUjjawalShriwastavNo ratings yet
- Inhibitorji Protonske ČrpalkeDocument15 pagesInhibitorji Protonske Črpalkeapi-3814389No ratings yet
- CEPHALOSPORINSDocument18 pagesCEPHALOSPORINSVikas SharmaNo ratings yet
- Forensic MedicineDocument9 pagesForensic Medicinev_vijayakanth7656No ratings yet
- Original Research Article: Journal of Chitwan Medical College 2016 6 (18) : 18-23Document6 pagesOriginal Research Article: Journal of Chitwan Medical College 2016 6 (18) : 18-23malathi kotaNo ratings yet
- Inflammation GuideDocument70 pagesInflammation GuidemikeNo ratings yet
- Chelseyearnhart ProfessionaldevelopmentpttDocument10 pagesChelseyearnhart Professionaldevelopmentpttapi-301343810No ratings yet
- 210-241 UrinaryDocument34 pages210-241 UrinaryYaj Cruzada100% (1)