You might also like
- The Characterisation of Overweight and Obese Women Who Are Under Reporting Energy Intake During PregnancyDocument10 pagesThe Characterisation of Overweight and Obese Women Who Are Under Reporting Energy Intake During PregnancyDheaNo ratings yet
- Physical Activity For Antenatal and Postnatal Depression in Women Attempting To Quit Smoking: Randomised Controlled TrialDocument10 pagesPhysical Activity For Antenatal and Postnatal Depression in Women Attempting To Quit Smoking: Randomised Controlled TrialDheaNo ratings yet
- The Characterisation of Overweight and Obese Women Who Are Under Reporting Energy Intake During PregnancyDocument10 pagesThe Characterisation of Overweight and Obese Women Who Are Under Reporting Energy Intake During PregnancyDheaNo ratings yet
- Risk Factors For Peripartum Hysterectomy Among Women With Postpartum Haemorrhage: Analysis of Data From The WOMAN TrialDocument8 pagesRisk Factors For Peripartum Hysterectomy Among Women With Postpartum Haemorrhage: Analysis of Data From The WOMAN TrialDheaNo ratings yet
- Jurnal MaternitasDocument10 pagesJurnal Maternitasamelia henitasariNo ratings yet
- JurnalDocument7 pagesJurnalDheaNo ratings yet
- Successful Use of An Artificial Placenta To Support Extremely Preterm Ovine Fetuses at The Border of ViabilityDocument17 pagesSuccessful Use of An Artificial Placenta To Support Extremely Preterm Ovine Fetuses at The Border of ViabilityDheaNo ratings yet
- Sexual & Reproductive Healthcare: SciencedirectDocument6 pagesSexual & Reproductive Healthcare: SciencedirectDheaNo ratings yet
- Patient Education and CounselingDocument6 pagesPatient Education and CounselingDheaNo ratings yet
- BMJ j3448 Full PDFDocument13 pagesBMJ j3448 Full PDFDheaNo ratings yet
- BMJ j1710 Full (1148)Document10 pagesBMJ j1710 Full (1148)DheaNo ratings yet
- BMJ j2856 Full PDFDocument15 pagesBMJ j2856 Full PDFdhea handyaraNo ratings yet
- BMJ k96 FullDocument9 pagesBMJ k96 FullDheaNo ratings yet
- BMJ k1675 Full PDFDocument11 pagesBMJ k1675 Full PDFDheaNo ratings yet
- BMJ j1710 Full (1148)Document10 pagesBMJ j1710 Full (1148)DheaNo ratings yet
- BMJ l1778 FullDocument10 pagesBMJ l1778 FullDheaNo ratings yet
- BAB 2 Penelitian9 IKAKOMDocument51 pagesBAB 2 Penelitian9 IKAKOMDheaNo ratings yet
- Penyuluhan PpokDocument7 pagesPenyuluhan PpokDhea100% (1)
- ID None PDFDocument11 pagesID None PDFDheaNo ratings yet
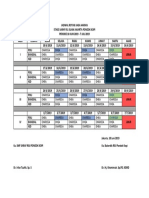
- Jadwal Rotasi Jaga Harian Stase SarafDocument1 pageJadwal Rotasi Jaga Harian Stase SarafDheaNo ratings yet
- BMJ j1710 Full (1148)Document10 pagesBMJ j1710 Full (1148)DheaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Rafiki MapDocument72 pagesThe Rafiki MapAnonymous Y2qwEuANo ratings yet
- Lecture Notes-Growth Kinetics - Growth PhasesDocument24 pagesLecture Notes-Growth Kinetics - Growth Phasesbioenviron100% (1)
- Acls QuestionsDocument28 pagesAcls QuestionsDsd100% (1)
- Buku Ident KepitingDocument111 pagesBuku Ident KepitingihsanNo ratings yet
- Heat Related Injuries-IllnessesDocument46 pagesHeat Related Injuries-IllnessesMusa D'anfieldNo ratings yet
- Physiology of Bone: Dr. Ross G. Cooper Senior Lecturer Division of Physiology School of Health & Policy StudiesDocument70 pagesPhysiology of Bone: Dr. Ross G. Cooper Senior Lecturer Division of Physiology School of Health & Policy StudiesnannaraNo ratings yet
- Bait Cycle Location Fish Benign Infested Tumor Ferment BladderDocument3 pagesBait Cycle Location Fish Benign Infested Tumor Ferment BladderClaude HaynesNo ratings yet
- How It Works Book of The Human Body (Kalinel - Du)Document180 pagesHow It Works Book of The Human Body (Kalinel - Du)AMFA100% (4)
- Catalase TestDocument29 pagesCatalase TestmaleehaNo ratings yet
- Untitled 2Document6 pagesUntitled 2Dr Prashant ChauhanNo ratings yet
- Bronchiolitis A Practical Approach For The General RadiologistDocument42 pagesBronchiolitis A Practical Approach For The General RadiologistTara NareswariNo ratings yet
- Coagulation DisordersDocument40 pagesCoagulation DisordersDr. Shatdal Chaudhary100% (6)
- Formula Guide NewestDocument60 pagesFormula Guide Newesteran76No ratings yet
- The Role of Emotions in Marketing: Richard P. BagozziDocument23 pagesThe Role of Emotions in Marketing: Richard P. BagozziEngin OzsahinNo ratings yet
- Guide To Clerking 2014Document24 pagesGuide To Clerking 2014Ridhwan Amid100% (1)
- Dynamic Correspondance of Rowing To WeighliftingDocument6 pagesDynamic Correspondance of Rowing To WeighliftingSajeel Chaudhry100% (1)
- Module 2 - Cell Structure & Function (Student Guide)Document24 pagesModule 2 - Cell Structure & Function (Student Guide)greggcllam619076100% (7)
- Transitional EpitheliumDocument7 pagesTransitional EpitheliumsakuraleeshaoranNo ratings yet
- Material Downloaded From - 1 / 8Document8 pagesMaterial Downloaded From - 1 / 8HARSH PahwaNo ratings yet
- Alingatong Plants?Document3 pagesAlingatong Plants?nancy urrizaNo ratings yet
- DD PresentationDocument13 pagesDD PresentationM Burhan BajwaNo ratings yet
- Effect of A High-Protein Diet Versus Standard-Protein Diet On Weight Loss and Biomarkers of Metabolic Syndrome A Randomized Clinical TrialDocument14 pagesEffect of A High-Protein Diet Versus Standard-Protein Diet On Weight Loss and Biomarkers of Metabolic Syndrome A Randomized Clinical TrialReni WulansariNo ratings yet
- Nursing Care Plan2 CVADocument4 pagesNursing Care Plan2 CVAhermesdave1No ratings yet
- Chapter - 6: TissuesDocument20 pagesChapter - 6: Tissueskrista leeNo ratings yet
- Hyper Kale Mia Case ReviewDocument4 pagesHyper Kale Mia Case ReviewSamina AhmadNo ratings yet
- Major Topic Abbreviation: RadiologyDocument105 pagesMajor Topic Abbreviation: Radiologycontrolpane100% (2)
- DAVIS MedSurg Notes Nurse S Clinical Pocket Guide FA Davis 2007Document242 pagesDAVIS MedSurg Notes Nurse S Clinical Pocket Guide FA Davis 2007amaliea234100% (1)
- Fun Facts About Anatomy and Physiology 2Document22 pagesFun Facts About Anatomy and Physiology 2Theodore Liwongan0% (1)
- CHEM14LAB - Experiment 1Document10 pagesCHEM14LAB - Experiment 1Lemon AdeNo ratings yet
- Biology Research PaperDocument5 pagesBiology Research Paperapi-240098584No ratings yet