You might also like
- Pathology WebsitesDocument7 pagesPathology WebsitesrubinnewNo ratings yet
- Solar Turbine ModelDocument58 pagesSolar Turbine Modelarmin heidariNo ratings yet
- 52 Ways To Increase Testosterone Levels Naturally PDFDocument74 pages52 Ways To Increase Testosterone Levels Naturally PDFItzikRazonNo ratings yet
- CPQ Design and Maintenance: Managing Organizational Growth With Long-Term FlexibilityDocument28 pagesCPQ Design and Maintenance: Managing Organizational Growth With Long-Term Flexibilityarmin heidari50% (2)
- Function Test Procedure1Document6 pagesFunction Test Procedure1armin heidari100% (1)
- Actuator & Test Procedure1Document11 pagesActuator & Test Procedure1armin heidariNo ratings yet
- Fenugreek On DiabetesDocument3 pagesFenugreek On DiabetesDr Dushyant Kamal DhariNo ratings yet
- George Miller Beard. (1879) - The Psychology of Spiritism. The North American Review, Vol. 129, No. 272, Pp. 65-80Document17 pagesGeorge Miller Beard. (1879) - The Psychology of Spiritism. The North American Review, Vol. 129, No. 272, Pp. 65-80GustavonNo ratings yet
- KapalbhatipptDocument17 pagesKapalbhatipptAmrinder Singh100% (2)
- Step 2 CS AdviceDocument14 pagesStep 2 CS AdviceHnia Usman100% (1)
- San Diego Lean 6 Sigma Solar Turbines PDFDocument91 pagesSan Diego Lean 6 Sigma Solar Turbines PDFarmin heidariNo ratings yet
- Ex Ophtalmo Eng 1Document4 pagesEx Ophtalmo Eng 1Roxana PascalNo ratings yet
- Jurnal 2Document8 pagesJurnal 2radiyNo ratings yet
- Guidelines of The International Writing Group On The Diabetic Foot On DiagnosisDocument12 pagesGuidelines of The International Writing Group On The Diabetic Foot On DiagnosisHan's OfficialNo ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- ASNJ-Volume 9-Issue 24.0 - Page 170-181 PDFDocument12 pagesASNJ-Volume 9-Issue 24.0 - Page 170-181 PDFMayasumita Wijayana05No ratings yet
- Manejo Del ResangradoDocument13 pagesManejo Del ResangradoRudy J CoradoNo ratings yet
- Grip Et Al-2018-British Journal of SurgeryDocument9 pagesGrip Et Al-2018-British Journal of SurgeryIrma SihotangNo ratings yet
- Clinical Examination and NonDocument23 pagesClinical Examination and NonMiguel SalesNo ratings yet
- SMJ 56 626Document6 pagesSMJ 56 626Andy HongNo ratings yet
- Passive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational StudyDocument9 pagesPassive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational Studycardionerd101No ratings yet
- The Efficacy of Topical Royal Jelly On Diabetic Foot Ulcers Healing: A Case SeriesDocument7 pagesThe Efficacy of Topical Royal Jelly On Diabetic Foot Ulcers Healing: A Case SeriesnatchredNo ratings yet
- Diabetes and Ulceration of The Foot 2011Document2 pagesDiabetes and Ulceration of The Foot 2011alex1973maNo ratings yet
- Ying Li 2016Document8 pagesYing Li 2016Bogdan TrandafirNo ratings yet
- Endoscopic Treatment of Esophageal Varices in Patients With Liver CirrhosisDocument13 pagesEndoscopic Treatment of Esophageal Varices in Patients With Liver CirrhosisAuliaNo ratings yet
- Outcome of Patients Undergoing Amputation For Diabetic Foot UlcerDocument4 pagesOutcome of Patients Undergoing Amputation For Diabetic Foot UlcerrischaNo ratings yet
- BasilDocument10 pagesBasilDavid FlynnNo ratings yet
- Eci 12222Document9 pagesEci 12222Andikaputra Brahma WidiantoroNo ratings yet
- Research Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionDocument9 pagesResearch Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionmikeNo ratings yet
- Diabetic Foot Ulcer : Risk Factors Stratification in Patients. A Study of 150 PatientsDocument6 pagesDiabetic Foot Ulcer : Risk Factors Stratification in Patients. A Study of 150 PatientsAnanda WulandariNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open Reconstructiontmarrero00No ratings yet
- A Comparative Study Between Platelet Rich Plasma and ConventionalDocument6 pagesA Comparative Study Between Platelet Rich Plasma and ConventionalAziir 'arNo ratings yet
- Original Research PaperDocument4 pagesOriginal Research PaperFernando SilalahiNo ratings yet
- Ari Cendani Prabawati (17.321.2658)Document12 pagesAri Cendani Prabawati (17.321.2658)yuna pratiwiNo ratings yet
- Foot & Ankle International: Minimal Incision Surgery For Tibiotalocalcaneal ArthrodesisDocument14 pagesFoot & Ankle International: Minimal Incision Surgery For Tibiotalocalcaneal Arthrodesisapi-241264935No ratings yet
- On-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyDocument8 pagesOn-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyGono GenieNo ratings yet
- ACG Ulcer Bleeding Guideline SummaryDocument6 pagesACG Ulcer Bleeding Guideline SummaryElison J PanggaloNo ratings yet
- Sys Rev TT of Intermittent ClaudicationDocument20 pagesSys Rev TT of Intermittent ClaudicationMaria PopNo ratings yet
- 10 5114@pdia 2016 62415Document6 pages10 5114@pdia 2016 62415senkonenNo ratings yet
- Late Results After Splenectomy in Adult Idiopathic Thrombocytopenic PurpuraDocument7 pagesLate Results After Splenectomy in Adult Idiopathic Thrombocytopenic PurpuraBogdan TrandafirNo ratings yet
- Goal-Directed Haemodynamic Therapy and Gastrointestinal Complications in Major Surgery: A Meta-Analysis of Randomized Controlled TrialsDocument10 pagesGoal-Directed Haemodynamic Therapy and Gastrointestinal Complications in Major Surgery: A Meta-Analysis of Randomized Controlled TrialsMateoZuluagaGomezNo ratings yet
- Cilostazol Prevents Foot Ulcers in Diabetic Patients With Peripheral Vascular DiseaseDocument4 pagesCilostazol Prevents Foot Ulcers in Diabetic Patients With Peripheral Vascular DiseaseOcha24 TupamahuNo ratings yet
- Articulo PatologiaDocument8 pagesArticulo PatologiaAlex C. GutierrezNo ratings yet
- Umapathy 2017Document11 pagesUmapathy 2017Karinaayu SerinNo ratings yet
- Hemodynamic Response To Pharmacological Treatment of Portal Hypertension and Long-Term Prognosis of CirrhosisDocument7 pagesHemodynamic Response To Pharmacological Treatment of Portal Hypertension and Long-Term Prognosis of CirrhosisBarbara Sakura RiawanNo ratings yet
- J CPM 2019 02 010Document13 pagesJ CPM 2019 02 010Mohamed GoudaNo ratings yet
- MIMS Doctor August 2016 RGDocument43 pagesMIMS Doctor August 2016 RGDeddy SupriyadiNo ratings yet
- AbiDocument11 pagesAbiMiftahul JannahNo ratings yet
- Intraabdominal HypertensionDocument23 pagesIntraabdominal Hypertensionflorinmd333No ratings yet
- Nej Mo A 2303706Document11 pagesNej Mo A 2303706xivydpndNo ratings yet
- Calder 2016 - Meta Analysis and Suggested Guidelines For Prevention of Venous Thromboembolism (VTE) in Foot and Ankle SurgeryDocument12 pagesCalder 2016 - Meta Analysis and Suggested Guidelines For Prevention of Venous Thromboembolism (VTE) in Foot and Ankle SurgeryNoel Yongshen LeeNo ratings yet
- Subglottic Stenosis in Granulomatosis With Polyangiitis: The Role of Laryngotracheal ResectionDocument5 pagesSubglottic Stenosis in Granulomatosis With Polyangiitis: The Role of Laryngotracheal ResectionSamNo ratings yet
- TyG VascularagingDocument8 pagesTyG VascularagingSNo ratings yet
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocument9 pagesSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Atm 08 23 1626Document12 pagesAtm 08 23 1626Susana MalleaNo ratings yet
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptAndriawan BramNo ratings yet
- Randomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseDocument9 pagesRandomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseTommy WidjayaNo ratings yet
- General Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueDocument3 pagesGeneral Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueRahul SinghNo ratings yet
- Intermittent Claudication-: ReconstructionDocument10 pagesIntermittent Claudication-: ReconstructionVlad ConstantinNo ratings yet
- PMR 2022 0017 PDFDocument7 pagesPMR 2022 0017 PDFStory WA DokterNo ratings yet
- AnemiaDocument10 pagesAnemiaRamesh VaradharajanNo ratings yet
- Portal Vein Thrombosis, Risk Factors, Clinical Presentation, and TreatmentDocument6 pagesPortal Vein Thrombosis, Risk Factors, Clinical Presentation, and TreatmentAdiNo ratings yet
- Effects DMCEA01Document11 pagesEffects DMCEA01milmrch523No ratings yet
- GI Bleeding (Text)Document11 pagesGI Bleeding (Text)Hart ElettNo ratings yet
- Turkjmedsci 50 706Document7 pagesTurkjmedsci 50 706Dave Miiranda KenedyNo ratings yet
- PeripheralDocument7 pagesPeripheralerdynNo ratings yet
- 2017 - Bansal - Corelation of HbA1c Levels and Duration of Diabetes With PADDocument4 pages2017 - Bansal - Corelation of HbA1c Levels and Duration of Diabetes With PADbuat nugas28No ratings yet
- Gallbladder Perforation: Clinical Presentation, Predisposing Factors, and Surgical Outcomes of 46 PatientsDocument8 pagesGallbladder Perforation: Clinical Presentation, Predisposing Factors, and Surgical Outcomes of 46 Patientsmudasir61No ratings yet
- Riesgo Quirurgico en Cirrosis, Clin Gast 2010Document7 pagesRiesgo Quirurgico en Cirrosis, Clin Gast 2010Diana Anguita IbarraNo ratings yet
- Management of Suspected Anastomotic Leak After Bariatric Laparoscopic Roux-en-Y Gastric BypassDocument7 pagesManagement of Suspected Anastomotic Leak After Bariatric Laparoscopic Roux-en-Y Gastric BypassJOTACENo ratings yet
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianNo ratings yet
- Home Blood Pressure MonitoringFrom EverandHome Blood Pressure MonitoringGeorge S. StergiouNo ratings yet
- AST Our CatalogDocument5 pagesAST Our Catalogarmin heidariNo ratings yet
- Kamat - Pressure Relief Valve-AssemblyDocument9 pagesKamat - Pressure Relief Valve-Assemblyarmin heidariNo ratings yet
- Leader in Superabrasive Finishing Systems: Pad Applications We Offer A Full Line of Hyprez® ProductsDocument2 pagesLeader in Superabrasive Finishing Systems: Pad Applications We Offer A Full Line of Hyprez® Productsarmin heidariNo ratings yet
- Production Map: Control Valve Production FlowchartDocument1 pageProduction Map: Control Valve Production Flowchartarmin heidariNo ratings yet
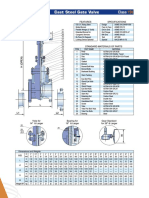
- C.S Gate ValveDocument4 pagesC.S Gate Valvearmin heidariNo ratings yet
- Actuators and Actuated Valve Packages: Product DefinitionDocument4 pagesActuators and Actuated Valve Packages: Product Definitionarmin heidariNo ratings yet
- Understanding Lambplan Maternal AsbvsDocument1 pageUnderstanding Lambplan Maternal Asbvsarmin heidariNo ratings yet
- Cladding & Nace 1Document21 pagesCladding & Nace 1armin heidariNo ratings yet
- 8 Inch Model 380/381 Control Valves: Technical Sales BulletinDocument12 pages8 Inch Model 380/381 Control Valves: Technical Sales Bulletinarmin heidariNo ratings yet
- GRP Pipeline ProjectDocument43 pagesGRP Pipeline Projectarmin heidariNo ratings yet
- P PIPING - Hydrotest - Procedure PDFDocument12 pagesP PIPING - Hydrotest - Procedure PDFarmin heidariNo ratings yet
- CM20160503 40917 61336Document24 pagesCM20160503 40917 61336armin heidariNo ratings yet
- MEJ Volume 50 Issue 1 Pages 103-112-2Document4 pagesMEJ Volume 50 Issue 1 Pages 103-112-2armin heidariNo ratings yet
- V04 Neu090608 PDFDocument15 pagesV04 Neu090608 PDFarmin heidariNo ratings yet
- EES Volume 5 Issue 1 Pages 71-83Document13 pagesEES Volume 5 Issue 1 Pages 71-83armin heidariNo ratings yet
- Amozesh Gas TurbineDocument114 pagesAmozesh Gas Turbinearmin heidari100% (1)
- DrawingDocument86 pagesDrawingarmin heidariNo ratings yet
- Peripheral Arterial DseDocument2 pagesPeripheral Arterial Dsemiss RNNo ratings yet
- Ph. Arthropoda: Subphylum Myriapoda: (Centipedes, Millipedes, and Their Kin)Document51 pagesPh. Arthropoda: Subphylum Myriapoda: (Centipedes, Millipedes, and Their Kin)PabloDarlanNo ratings yet
- Musculoskeletal SystemDocument210 pagesMusculoskeletal SystemDr. Serin KuriakoseNo ratings yet
- Summary of Human Digestive SystemDocument4 pagesSummary of Human Digestive SystemNurullina FajriNo ratings yet
- Hypothalamus: By: Ma. Athena C. Del Rosario-Rebulado MD September 10, 2021Document45 pagesHypothalamus: By: Ma. Athena C. Del Rosario-Rebulado MD September 10, 2021AthenaNo ratings yet
- Course SyllabusDocument12 pagesCourse SyllabusCamille Honeyleith Lanuza FernandoNo ratings yet
- Anatomy and Physiology of Peptic UlcerDocument16 pagesAnatomy and Physiology of Peptic UlcerDrNarayan KR100% (8)
- Humoral and Intra Cardiac Mechanism of Heart' RegulationDocument23 pagesHumoral and Intra Cardiac Mechanism of Heart' RegulationAman singhNo ratings yet
- Thesis Statement and OutlinesDocument3 pagesThesis Statement and OutlinesShane DistorNo ratings yet
- Oral Mucous Membrane: by - Arindam MondalDocument92 pagesOral Mucous Membrane: by - Arindam MondalMohammed hisham khanNo ratings yet
- Buckel2018-Flavin Based ElectronDocument24 pagesBuckel2018-Flavin Based ElectronmonicNo ratings yet
- Principles of Osteoarthritis - Its Definition, Character, Derivation (Etc.,) - B. Rothschild (Intech, 2012) WWDocument602 pagesPrinciples of Osteoarthritis - Its Definition, Character, Derivation (Etc.,) - B. Rothschild (Intech, 2012) WWSilvia AlexandraNo ratings yet
- NITROGLYCERIN IN DEXTROSE-nitroglycerin Injection Baxter Healthcare CompanyDocument18 pagesNITROGLYCERIN IN DEXTROSE-nitroglycerin Injection Baxter Healthcare CompanyAinunZamiraNo ratings yet
- Obstetric Hemorrhage AnestDocument9 pagesObstetric Hemorrhage AnestjefeNo ratings yet
- Skin and Body MembranesDocument10 pagesSkin and Body MembranesChromagrafx100% (1)
- Fits, Faints and Funny Turns in Children - Mark MackayDocument6 pagesFits, Faints and Funny Turns in Children - Mark MackayOwais Khan100% (1)
- EnterobakterDocument36 pagesEnterobakterUttari DalemNo ratings yet
- I. ConclusionDocument1 pageI. ConclusionJARISSA DIZON GALLAZANo ratings yet
- Adult IV Therapy Course (Seventh Edition, 2018) : ©consortium of New Jersey Nurse EducatorsDocument144 pagesAdult IV Therapy Course (Seventh Edition, 2018) : ©consortium of New Jersey Nurse EducatorsAriana BlumNo ratings yet
- Tmp1a96 TMPDocument80 pagesTmp1a96 TMPFrontiersNo ratings yet
- S2-OB-Maternal Physio PDFDocument14 pagesS2-OB-Maternal Physio PDFSheena PasionNo ratings yet
- Nursing Practice Threesoko Na Ito Cgena... Kainis 1Document16 pagesNursing Practice Threesoko Na Ito Cgena... Kainis 1JayCesarNo ratings yet
- Principles of Nonunion Management State of The.12Document6 pagesPrinciples of Nonunion Management State of The.12marcoselverdinNo ratings yet