You might also like
- ASIA ISCOS IntlWorksheet 2019Document2 pagesASIA ISCOS IntlWorksheet 2019Raquel GomesNo ratings yet
- ASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Document2 pagesASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Ade Marvira PutriNo ratings yet
- ASIA ISCOS IntlWorksheet - 2019Document2 pagesASIA ISCOS IntlWorksheet - 2019Luisa CruzNo ratings yet
- International standards for neurological classification of spinal cord injuryDocument2 pagesInternational standards for neurological classification of spinal cord injuryDavid ParraNo ratings yet
- International standards for neurological classification of spinal cord injuryDocument2 pagesInternational standards for neurological classification of spinal cord injuryGiieeeNo ratings yet
- Sensory exam of upper extremitiesDocument2 pagesSensory exam of upper extremitiesDavideNo ratings yet
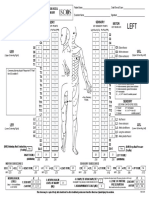
- UER UEL: R L Zone of Partial Preservation R LDocument2 pagesUER UEL: R L Zone of Partial Preservation R LIridian Berenice Villaseñor XochimitlNo ratings yet
- ASIA International Standards For Neurological Classification of Spinal Cord InjuryDocument2 pagesASIA International Standards For Neurological Classification of Spinal Cord InjuryMicah Tagle100% (1)
- Asia PDFDocument2 pagesAsia PDFIrro Asentista CabelloNo ratings yet
- Right Totals (Maximum)Document6 pagesRight Totals (Maximum)kaychi zNo ratings yet
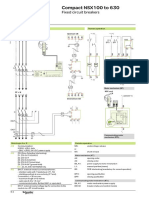
- Compact NSX100 To 630: Fixed Circuit BreakersDocument1 pageCompact NSX100 To 630: Fixed Circuit BreakersJose Manuel GpNo ratings yet
- Noise Filter Circuit AnalysisDocument9 pagesNoise Filter Circuit AnalysisДенис БородинNo ratings yet
- C8 C1-C11 Corners/Curves track map for Madras Motor Sports Club short courseDocument1 pageC8 C1-C11 Corners/Curves track map for Madras Motor Sports Club short courseVishnu GopzzNo ratings yet
- Patient Name - Date/Time of Exam - Examiner Name - SignatureDocument1 pagePatient Name - Date/Time of Exam - Examiner Name - SignatureVineeth ReddyNo ratings yet
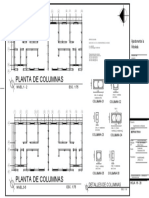
- Column Detail A3Document1 pageColumn Detail A3Hemam PrasantaNo ratings yet
- Schita Arctic - EliDocument1 pageSchita Arctic - EliAlexandru PopaNo ratings yet
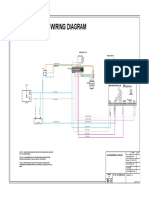
- Typical wiring diagram emergency stop circuitDocument1 pageTypical wiring diagram emergency stop circuitzeshanjamilNo ratings yet
- Single Line Wiring Diagram 275M 250kva PDFDocument1 pageSingle Line Wiring Diagram 275M 250kva PDFzeshanjamilNo ratings yet
- TMS370Cx5x 8-Bit Microcontroller: FN / FZ Package (Top View)Document75 pagesTMS370Cx5x 8-Bit Microcontroller: FN / FZ Package (Top View)Carlos Luis ColmenaresNo ratings yet
- 1650L Hydraulic SchematicDocument1 page1650L Hydraulic SchematicCarlos PinedaNo ratings yet
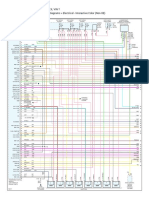
- Ecu Chevrolet S10 1998 2.2Document4 pagesEcu Chevrolet S10 1998 2.2AUTOMOTRIZ TIPO SPCA100% (2)
- Ignition System Circuit GuideDocument10 pagesIgnition System Circuit GuideCarlos Awo OsaureNo ratings yet
- Des - Con: Lighting Outlet Layout Plan Convenience Outlet Layout PlanDocument1 pageDes - Con: Lighting Outlet Layout Plan Convenience Outlet Layout PlanArch Jemil Rose SamosNo ratings yet
- APT Rectrofitting 24-03-2018-Model PDFDocument1 pageAPT Rectrofitting 24-03-2018-Model PDFAnonymous ddAndJNo ratings yet
- Centre line plan for columnsDocument1 pageCentre line plan for columnsHusen GhoriNo ratings yet
- MCC Nanjing Fan Damper PlanDocument7 pagesMCC Nanjing Fan Damper PlanNAZIM ŞAHAN ERKALNo ratings yet
- HC04a PCB Top ViewDocument1 pageHC04a PCB Top ViewAitorNo ratings yet
- Litar Pendawaian Auto-Transformer StarterDocument1 pageLitar Pendawaian Auto-Transformer StarterFatinHalim67% (6)
- Star DeltaDocument1 pageStar DeltaVERY YOGA MARULI TUA SIHOMBING TBANo ratings yet
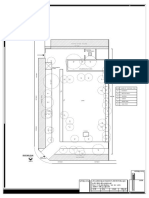
- Plano Ramaleo AreasDocument1 pagePlano Ramaleo AreasDiego CampuzanoNo ratings yet
- Existing PlanDocument1 pageExisting Plankanad kumbharNo ratings yet
- Screenshot 2021-11-19 at 10.37.25Document56 pagesScreenshot 2021-11-19 at 10.37.25TIMOTHY DIPONo ratings yet
- Genset 50SLD Golf Cart Shed 20220131-DB1 UPSDocument1 pageGenset 50SLD Golf Cart Shed 20220131-DB1 UPSGem RNo ratings yet
- Circuit diagrams and PCB layouts for ICC 200, 300, 350 CPUsDocument65 pagesCircuit diagrams and PCB layouts for ICC 200, 300, 350 CPUsKuni KazeNo ratings yet
- HS35 5Document2 pagesHS35 5dgalvan.keisergroupNo ratings yet
- Destroyer SoundTech S375WR & PSM1200 IC8 M65831 PDFDocument2 pagesDestroyer SoundTech S375WR & PSM1200 IC8 M65831 PDFSandro José100% (1)
- TMOD1 - EN - v1.0.2018 PARTIAL HANDDocument2 pagesTMOD1 - EN - v1.0.2018 PARTIAL HANDEsaRidho SambadaNo ratings yet
- Mancore Project Bit LBP Mocnphase1 Df031Document1 pageMancore Project Bit LBP Mocnphase1 Df031Josua imanuel purbaNo ratings yet
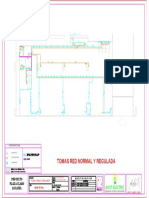
- Plano Tomas y Red ReguladaDocument1 pagePlano Tomas y Red Reguladaasist electricNo ratings yet
- (AP0) (AP1) : MCCB 30ADocument1 page(AP0) (AP1) : MCCB 30AMuhammad Bilal FarooqNo ratings yet
- Compact NSX Wiring Diagrams Under 40 CharactersDocument9 pagesCompact NSX Wiring Diagrams Under 40 CharactersBojan KitanovskiNo ratings yet
- Frma 2 SRD C v2 Standing Desk InstructionsDocument16 pagesFrma 2 SRD C v2 Standing Desk InstructionsrickNo ratings yet
- Planificación urbana y clasificación vialDocument1 pagePlanificación urbana y clasificación vialAna Paula Villanueva PalominoNo ratings yet
- Transmissions - A - T Circuit (Transmission and Drivetrain) - ALLDATA RepairDocument2 pagesTransmissions - A - T Circuit (Transmission and Drivetrain) - ALLDATA RepairManuel AyalaNo ratings yet
- C134-Westend Mall Extension Framing Layout and Details-A1Document1 pageC134-Westend Mall Extension Framing Layout and Details-A1abhijitkolheNo ratings yet
- Ovaj dokument iz tvrtke OMIKODocument1 pageOvaj dokument iz tvrtke OMIKOZdenko NagyNo ratings yet
- Daihatsu Type k3 Engine Service Manual No9737 No9332 No 9237 Ignition SystemDocument10 pagesDaihatsu Type k3 Engine Service Manual No9737 No9332 No 9237 Ignition SystemJoko Mardiyanto100% (1)
- TRANSMISSION - Pontiac Grand Prix GTP 1997 - SYSTEM WIRING DIAGRAMS PDFDocument3 pagesTRANSMISSION - Pontiac Grand Prix GTP 1997 - SYSTEM WIRING DIAGRAMS PDFRicardo Alejandro Castro HernándezNo ratings yet
- An9hdbft 5m8cseeizlte40yr4hgi76irdktufpi6ubsvnj62umxxarspztpu Ohxcvqfbs Nrrkzcde Gexu1uw9vbadgbkvpqkzuhck3kkcj6nbes8kf4vigoi5zoDocument1 pageAn9hdbft 5m8cseeizlte40yr4hgi76irdktufpi6ubsvnj62umxxarspztpu Ohxcvqfbs Nrrkzcde Gexu1uw9vbadgbkvpqkzuhck3kkcj6nbes8kf4vigoi5zopaul.fernandez2No ratings yet
- Planta de Columnas: Apartamentos La ArboledaDocument1 pagePlanta de Columnas: Apartamentos La ArboledaSusy CifuentesNo ratings yet
- Dermatome Map OverviewDocument1 pageDermatome Map Overviewngwinda90100% (1)
- 543 RM Relay Module ENDocument1 page543 RM Relay Module ENEricks PérezNo ratings yet
- Socket For 5-Pin RelaysDocument4 pagesSocket For 5-Pin RelaysLikabeus EirlNo ratings yet
- 2003 Chevy Truck K Tahoe 4WD V8-5.3L VIN TDocument5 pages2003 Chevy Truck K Tahoe 4WD V8-5.3L VIN Tluis leonNo ratings yet
- Ardf TX 80m PCB 2013 Mile Kokotov Bd139 Final So Izmeni NajnovDocument1 pageArdf TX 80m PCB 2013 Mile Kokotov Bd139 Final So Izmeni Najnovag1tatorNo ratings yet
- Electrical TWD-110 YuchaiDocument1 pageElectrical TWD-110 YuchaizeshanjamilNo ratings yet
- Conduit LayoutDocument2 pagesConduit LayoutAsif ANo ratings yet
- Raft MezzanineDocument1 pageRaft MezzanineMohanad EldarerNo ratings yet
- Elbow Pain Exercise SheetDocument4 pagesElbow Pain Exercise Sheetmaha AbdulazizNo ratings yet
- Shoulder Joint (MSPT SPT)Document99 pagesShoulder Joint (MSPT SPT)Khushboo IkramNo ratings yet
- The Complete Running and Marathon BookDocument194 pagesThe Complete Running and Marathon Bookozal udaya100% (4)
- Techno Card Us PDFDocument48 pagesTechno Card Us PDFROMEOPUNTO67% (3)
- Postgraduate OrthopaedicsDocument626 pagesPostgraduate OrthopaedicsYau Chun Chong100% (1)
- Muscles Used in RowingDocument4 pagesMuscles Used in RowingCristine EchaveNo ratings yet
- Adductor Tendinopathy - PhysiopediaDocument9 pagesAdductor Tendinopathy - PhysiopediaMikeNo ratings yet
- Ortho - OSCE 1 1Document120 pagesOrtho - OSCE 1 1Santosh DahitNo ratings yet
- ICAO Marshalling Guide LinesDocument1 pageICAO Marshalling Guide LinesSantosh Raj KhanalNo ratings yet
- 11 - Reciprocal InnervationDocument19 pages11 - Reciprocal InnervationGaming ProNo ratings yet
- Muscular System Laboratory Guide: Dissection of The Muscles: See Pages 229-230 in The Lab ManualDocument16 pagesMuscular System Laboratory Guide: Dissection of The Muscles: See Pages 229-230 in The Lab ManualNathaniel CamangonNo ratings yet
- Medial Collateral Ligament Sprains - A Case StudyDocument26 pagesMedial Collateral Ligament Sprains - A Case StudyomboNo ratings yet
- Daftar PustakaDocument3 pagesDaftar Pustakasusi candra winaNo ratings yet
- HeightDocument4 pagesHeightThiện Nhân NguyễnNo ratings yet
- Rehabilitation of Elbow Trauma: Shrikant J. Chinchalkar, Bscot, Otr, CHT, Mike Szekeres, BscotDocument12 pagesRehabilitation of Elbow Trauma: Shrikant J. Chinchalkar, Bscot, Otr, CHT, Mike Szekeres, BscotIoanaCamiiNo ratings yet
- Mobility Training For The Young Athlete.4Document7 pagesMobility Training For The Young Athlete.4Dân NguyễnNo ratings yet
- High Yield MCQsDocument46 pagesHigh Yield MCQsSandareNo ratings yet
- Kamus-ICD-10-ICD-9 DDocument3 pagesKamus-ICD-10-ICD-9 Dnoerrekmed_816409184No ratings yet
- Content ServerDocument9 pagesContent ServerGabriel AguilarNo ratings yet
- Anatomy - Jeopardy Round 2 CompatDocument53 pagesAnatomy - Jeopardy Round 2 Compattaleen_haddadNo ratings yet
- Muscle Coloring BookDocument9 pagesMuscle Coloring Bookjeaves14No ratings yet
- Explaining The Meaning and History of GymnasticsDocument4 pagesExplaining The Meaning and History of GymnasticsJohanna Marie GolinganNo ratings yet
- Mobilizare Pasiva GleznaDocument1 pageMobilizare Pasiva GleznaLuca AnamariaNo ratings yet
- Muscles of the Head, Neck, and TrunkDocument8 pagesMuscles of the Head, Neck, and TrunkJericho CarenaNo ratings yet
- Dynamic Q Angle Is Increased in Patients With Chronic PatellofemoralDocument8 pagesDynamic Q Angle Is Increased in Patients With Chronic PatellofemoralDavids MarinNo ratings yet
- Family Medicine Residents Orthopedic Rotation HandoutDocument18 pagesFamily Medicine Residents Orthopedic Rotation HandoutRuth PoeryNo ratings yet
- Dim Mak Vital Points From Rick ClarkDocument7 pagesDim Mak Vital Points From Rick Clarknakadakaken100% (1)
- Biomechanics of Knee Joint PDFDocument32 pagesBiomechanics of Knee Joint PDFAli NoumanNo ratings yet
- Ortho LMRP 2019Document44 pagesOrtho LMRP 2019skNo ratings yet
- AMPUTATION IN UPPER LIMB (FINaL)Document17 pagesAMPUTATION IN UPPER LIMB (FINaL)Hussain AliNo ratings yet