You might also like
- ASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Document2 pagesASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Ade Marvira PutriNo ratings yet
- ASIA ISCOS IntlWorksheet 2019Document2 pagesASIA ISCOS IntlWorksheet 2019Anastasia CanahuateNo ratings yet
- ASIA ISCOS IntlWorksheet 2019Document2 pagesASIA ISCOS IntlWorksheet 2019Raquel GomesNo ratings yet
- ASIA ISCOS IntlWorksheet - 2019Document2 pagesASIA ISCOS IntlWorksheet - 2019Luisa CruzNo ratings yet
- Formato Escala ASIADocument2 pagesFormato Escala ASIADavid ParraNo ratings yet
- Isncsci Worksheet 2015 Web PDFDocument2 pagesIsncsci Worksheet 2015 Web PDFDavideNo ratings yet
- UER UEL: R L Zone of Partial Preservation R LDocument2 pagesUER UEL: R L Zone of Partial Preservation R LIridian Berenice Villaseñor XochimitlNo ratings yet
- ASIA International Standards For Neurological Classification of Spinal Cord InjuryDocument2 pagesASIA International Standards For Neurological Classification of Spinal Cord InjuryMicah Tagle100% (1)
- Asia PDFDocument2 pagesAsia PDFIrro Asentista CabelloNo ratings yet
- PDF Datasheet 7432 or PDF - CompressDocument9 pagesPDF Datasheet 7432 or PDF - CompressfurnitureartmabqNo ratings yet
- C134-Westend Mall Extension Framing Layout and Details-A1Document1 pageC134-Westend Mall Extension Framing Layout and Details-A1abhijitkolheNo ratings yet
- Right Totals (Maximum)Document6 pagesRight Totals (Maximum)kaychi zNo ratings yet
- Analisis Niveles de LogroDocument36 pagesAnalisis Niveles de LogroteovibalcNo ratings yet
- Tab Puente 2hp440vcaDocument3 pagesTab Puente 2hp440vcaliliana mercadoNo ratings yet
- Pemeriksaan NeurologisDocument1 pagePemeriksaan NeurologisLuthfi LazuardiNo ratings yet
- Patient Name - Date/Time of Exam - Examiner Name - SignatureDocument1 pagePatient Name - Date/Time of Exam - Examiner Name - SignatureVineeth ReddyNo ratings yet
- Pictorial (Manual & Auto)Document1 pagePictorial (Manual & Auto)gt xNo ratings yet
- (AP0) (AP1) : MCCB 30ADocument1 page(AP0) (AP1) : MCCB 30AMuhammad Bilal FarooqNo ratings yet
- NETTER DermatomDocument1 pageNETTER Dermatomngwinda90100% (1)
- Plano Ramaleo AreasDocument1 pagePlano Ramaleo AreasDiego CampuzanoNo ratings yet
- Column Detail A3Document1 pageColumn Detail A3Hemam PrasantaNo ratings yet
- Schematic Pages From Service Manual ICCDocument65 pagesSchematic Pages From Service Manual ICCKuni KazeNo ratings yet
- MCC Nanjing Fan Damper PlanDocument7 pagesMCC Nanjing Fan Damper PlanNAZIM ŞAHAN ERKALNo ratings yet
- Des - Con: Lighting Outlet Layout Plan Convenience Outlet Layout PlanDocument1 pageDes - Con: Lighting Outlet Layout Plan Convenience Outlet Layout PlanArch Jemil Rose SamosNo ratings yet
- Horloge Geant Kit InstructionsDocument16 pagesHorloge Geant Kit Instructionsthierry.francois.1965No ratings yet
- MR Sarri Bus Myhome Legrand ScsDocument1 pageMR Sarri Bus Myhome Legrand ScsPolo CasdenNo ratings yet
- Capstone v1 BRDDocument1 pageCapstone v1 BRDapi-506962353No ratings yet
- Mancore Project Bit LBP Mocnphase1 Df031Document1 pageMancore Project Bit LBP Mocnphase1 Df031Josua imanuel purbaNo ratings yet
- Memory: by Kriti Sundar Das Mirafra TechnnologiesDocument22 pagesMemory: by Kriti Sundar Das Mirafra Technnologiesamena fahatNo ratings yet
- Panel Pju Perumahan Polinema A4: KeteranganDocument1 pagePanel Pju Perumahan Polinema A4: KeteranganFerdiNo ratings yet
- Noise Filter: Secondary PrimaryDocument9 pagesNoise Filter: Secondary PrimaryДенис БородинNo ratings yet
- 08/01/2019 09:38 P. M. F 2.20 C:/Users/Luis SADG/Documents/ITESHU/PENDIENTE/CTRL/INVERSOR/EAGLE/POTENCIA - PARTE - 1 - V8.brdDocument1 page08/01/2019 09:38 P. M. F 2.20 C:/Users/Luis SADG/Documents/ITESHU/PENDIENTE/CTRL/INVERSOR/EAGLE/POTENCIA - PARTE - 1 - V8.brdLuis Alberto SDNo ratings yet
- Ig Toyota TeriosDocument10 pagesIg Toyota TeriosCarlos Awo OsaureNo ratings yet
- 3KW DC DC Power - RevBDocument1 page3KW DC DC Power - RevBKornélIllyésNo ratings yet
- E2 34Document1 pageE2 34Jamaica BandinNo ratings yet
- TecnicoDocument2 pagesTecnicoAbulonNo ratings yet
- APT Rectrofitting 24-03-2018-Model PDFDocument1 pageAPT Rectrofitting 24-03-2018-Model PDFAnonymous ddAndJNo ratings yet
- Destroyer SoundTech S375WR & PSM1200 IC8 M65831 PDFDocument2 pagesDestroyer SoundTech S375WR & PSM1200 IC8 M65831 PDFSandro José100% (1)
- CH01 Sample PDFDocument32 pagesCH01 Sample PDFDilah RahmaNo ratings yet
- Power Wirring)Document1 pagePower Wirring)HamedNo ratings yet
- HS35 5Document2 pagesHS35 5dgalvan.keisergroupNo ratings yet
- Aida MMP 80T 2Document8 pagesAida MMP 80T 2Salsabila IkbalNo ratings yet
- Tpa 3116Document1 pageTpa 3116Edi KurniawanNo ratings yet
- Tpa3116 PDFDocument1 pageTpa3116 PDFNICONo ratings yet
- Low Cost Digital Panel Meter Designs and Complete Instructions For LCD and LED KitsDocument9 pagesLow Cost Digital Panel Meter Designs and Complete Instructions For LCD and LED KitsLucía MitchellNo ratings yet
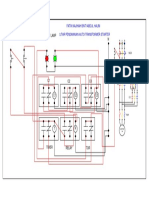
- Litar Pendawaian Auto-Transformer StarterDocument1 pageLitar Pendawaian Auto-Transformer StarterFatinHalim67% (6)
- Calles y Vias - Sector 3Document1 pageCalles y Vias - Sector 3Ana Paula Villanueva PalominoNo ratings yet
- Waveshare Sound Sensor SchematicDocument1 pageWaveshare Sound Sensor SchematicNishant Kumar KashyapNo ratings yet
- Swich TransferDocument13 pagesSwich TransferFikre shameboNo ratings yet
- Eguiron, Carlo - Ee06lab - Activity No.3Document1 pageEguiron, Carlo - Ee06lab - Activity No.3Carlo EguieronNo ratings yet
- RG 88Document1 pageRG 88api-3711045100% (2)
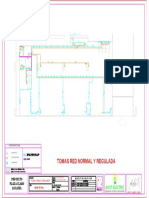
- Plano Tomas y Red ReguladaDocument1 pagePlano Tomas y Red Reguladaasist electricNo ratings yet
- Dotplot of C1, C2, C3, C4, C5, C6, C7, C8, ... : C16 C15 C14 C13 C12 C11 C10 C9 C8 VariableDocument1 pageDotplot of C1, C2, C3, C4, C5, C6, C7, C8, ... : C16 C15 C14 C13 C12 C11 C10 C9 C8 VariableJoseph HalfordNo ratings yet
- Untitled PDFDocument1 pageUntitled PDFBajak LautNo ratings yet
- 13TR T4DDocument1 page13TR T4Dfox7878No ratings yet
- Diagrama Yag II Plus No.2Document1 pageDiagrama Yag II Plus No.2eduardoquijada100% (1)
- Schematic Keypad 2023-04-10Document1 pageSchematic Keypad 2023-04-10Alfredo Meurer JuniorNo ratings yet
- TMOD1 - EN - v1.0.2018 PARTIAL HANDDocument2 pagesTMOD1 - EN - v1.0.2018 PARTIAL HANDEsaRidho SambadaNo ratings yet
- Unit 3 Forensic AnthropologyDocument32 pagesUnit 3 Forensic AnthropologyTina SharmaNo ratings yet
- Low Thoracic and Lumbar Burst Fractures - Radiographic and Functional OutcomesDocument10 pagesLow Thoracic and Lumbar Burst Fractures - Radiographic and Functional Outcomesmuhammad bayu wicaksonoNo ratings yet
- Use of Ergonomics Risk Assessment Tools On Construction SiteDocument4 pagesUse of Ergonomics Risk Assessment Tools On Construction SiteVIVA-TECH IJRINo ratings yet
- Mediastinum and Its ContentsDocument11 pagesMediastinum and Its ContentsPap YeeNo ratings yet
- D FTP Media Manuals 330175 ManualDocument53 pagesD FTP Media Manuals 330175 ManualPETER LOCKNo ratings yet
- Ortho HO Exam NS AnswerDocument33 pagesOrtho HO Exam NS Answersarvesswara muniandyNo ratings yet
- Safe Work Method Statement Gangra Kilometre 8 Phase 2 ProjectDocument3 pagesSafe Work Method Statement Gangra Kilometre 8 Phase 2 ProjectMark GarmondehNo ratings yet
- Siegelman Online Advantage 1.1 PDFDocument39 pagesSiegelman Online Advantage 1.1 PDFDana Ysabelle Ibarra100% (1)
- Civil Appeal 7 of 2019Document22 pagesCivil Appeal 7 of 2019William Mungai KariukiNo ratings yet
- 1971 Manson CrashDocument2 pages1971 Manson CrashAlban RileyNo ratings yet
- GadgetsDocument5 pagesGadgetsJewell EstiokoNo ratings yet
- 01 Bones of The Upper Limb by DR Derek NgabiranoDocument31 pages01 Bones of The Upper Limb by DR Derek NgabiranoYIKI ISAACNo ratings yet
- CRS - Sonia Pradepta - G1a219096 (Wound - Dr. Amran)Document27 pagesCRS - Sonia Pradepta - G1a219096 (Wound - Dr. Amran)heta aprianaNo ratings yet
- Stretch Reflex and Muscle ToneDocument14 pagesStretch Reflex and Muscle Toneiman ferganiNo ratings yet
- Prof. DavidWound Care Guidelines 2020 - CompressedDocument33 pagesProf. DavidWound Care Guidelines 2020 - CompressedPUSKESMAS KECAMATAN KEPULAUAN SERIBU UTARANo ratings yet
- Adler 2007Document11 pagesAdler 2007Anand KarnawatNo ratings yet
- Sports Science Gcse CourseworkDocument8 pagesSports Science Gcse Courseworkafjwduenevzdaa100% (2)
- Head Trauma - Dr. Affan Priyambodo, SPBS (K)Document32 pagesHead Trauma - Dr. Affan Priyambodo, SPBS (K)Verty SalleNo ratings yet
- Midterm - Pe 2ndDocument3 pagesMidterm - Pe 2ndRoseann EnriquezNo ratings yet
- LG lfd22786st User ManualDocument43 pagesLG lfd22786st User ManualFrankieNo ratings yet
- Disability History Month - Was Tamerlane Disabled - BBC NewsDocument3 pagesDisability History Month - Was Tamerlane Disabled - BBC NewsAnonymous xo7GDeQNo ratings yet
- Handling Tourist's Special NeedsDocument21 pagesHandling Tourist's Special NeedsZara LuminaNo ratings yet
- Open Pelvic Fracture: The Killing Fracture?Document8 pagesOpen Pelvic Fracture: The Killing Fracture?odyNo ratings yet
- NPTE Sullivan Exam ADocument130 pagesNPTE Sullivan Exam AMarilia Farensena100% (1)
- KE-430F BE-438F: Electronic Direct Drive Lockstitch Bar Tacker Electronic Direct Drive Lockstitch Button SewerDocument184 pagesKE-430F BE-438F: Electronic Direct Drive Lockstitch Bar Tacker Electronic Direct Drive Lockstitch Button SewerFrankNo ratings yet
- The Health Sector in Mass Casualty IncidentsDocument47 pagesThe Health Sector in Mass Casualty IncidentsLorenz SmallNo ratings yet
- Aer Conditionat LGDocument22 pagesAer Conditionat LGcasiloNo ratings yet
- Musculoskeletal Assessment ChecklistDocument2 pagesMusculoskeletal Assessment ChecklistThe Blue and Gold RvdNo ratings yet
- Femoral Neck FractureDocument32 pagesFemoral Neck FractureAndi Karwana Cipta100% (1)
- Surgical Stent and C-Arm Guided Reduction andDocument5 pagesSurgical Stent and C-Arm Guided Reduction andkityamuwesiNo ratings yet