You might also like
- Delayed Coker Safety During ShutdownsDocument38 pagesDelayed Coker Safety During ShutdownsMIGUELONOFRENo ratings yet
- Blasting Painting Report (Example)Document1 pageBlasting Painting Report (Example)DoddyNo ratings yet
- Corrective Action Log TemplateDocument20 pagesCorrective Action Log Templatendayiragije JMVNo ratings yet
- Lecture 3 - Process SafetyDocument79 pagesLecture 3 - Process SafetyDivyashini MohanNo ratings yet
- Training Plan Including On-The-Job Training of NigeriansDocument5 pagesTraining Plan Including On-The-Job Training of NigeriansLaohoria YamallahNo ratings yet
- JSA Installation of Platform and Guard Rails On Crawler CraneDocument5 pagesJSA Installation of Platform and Guard Rails On Crawler CraneDann TanNo ratings yet
- Activity - Communication PlanDocument5 pagesActivity - Communication Planwaqeeh arshadNo ratings yet
- ChecklistDocument10 pagesChecklistbharat ghantaNo ratings yet
- Blanking and Blinding PracticeDocument8 pagesBlanking and Blinding PracticeBabyface888100% (1)
- Workplace Hazard Inspection ChecklistDocument3 pagesWorkplace Hazard Inspection ChecklistWisnu KertaningnagoroNo ratings yet
- Dust and EmissionsDocument112 pagesDust and Emissions0808276kNo ratings yet
- Director Manager Environmental Health Safety in Nashville TN Resume Neil SchwartzDocument2 pagesDirector Manager Environmental Health Safety in Nashville TN Resume Neil SchwartzNeilSchwartzNo ratings yet
- 508 Access Fullbook Industrial PSM Training Ed. 2.0 January 2014 PDFDocument235 pages508 Access Fullbook Industrial PSM Training Ed. 2.0 January 2014 PDFwaheed2286No ratings yet
- Saferad LTD: Health, Safety and Environmental Targets - 2016 2018Document3 pagesSaferad LTD: Health, Safety and Environmental Targets - 2016 2018AkhilNo ratings yet
- Observation Card ReportDocument32 pagesObservation Card Reportob8y100% (1)
- Regular Board Meeting Agenda Package - April 7, 2020Document29 pagesRegular Board Meeting Agenda Package - April 7, 2020Jess PetersNo ratings yet
- EGA SETP TT-CSM 13 Prequal Questionnaire v2.00Document6 pagesEGA SETP TT-CSM 13 Prequal Questionnaire v2.00shijadNo ratings yet
- REGDOC2 1 2 Safety Culture Final EngDocument31 pagesREGDOC2 1 2 Safety Culture Final Engnagatopein6No ratings yet
- FY12 New Comp PlanDocument6 pagesFY12 New Comp PlanhousingworksNo ratings yet
- Central EHS meeting performance highlightsDocument4 pagesCentral EHS meeting performance highlightsakshay aryaNo ratings yet
- Procedure For OffloadingDocument10 pagesProcedure For OffloadingStansilous Tatenda Nyagomo100% (1)
- Solar Permitting GuidelinesDocument12 pagesSolar Permitting GuidelinesDanielNo ratings yet
- Section 942-BR Area Coating GIIDocument31 pagesSection 942-BR Area Coating GIIchristian gordonNo ratings yet
- SWP 03 Heavy EquipmentDocument7 pagesSWP 03 Heavy Equipmentমমিন মানব100% (1)
- JHA 001 Welding OperationsDocument3 pagesJHA 001 Welding OperationsAhmad alwaelyNo ratings yet
- Job Safety Analysis Sheet: FacilityDocument1 pageJob Safety Analysis Sheet: FacilityHelza RahmanniaNo ratings yet
- Cold Work PermitDocument1 pageCold Work PermitherdianNo ratings yet
- SWP-07 For Office Safety and Health DaimanDocument1 pageSWP-07 For Office Safety and Health DaimanHassan AbdullahNo ratings yet
- Qcs 2010 Section 11 Part 2.3.11 She Procedures - Permit To Work SysteDocument20 pagesQcs 2010 Section 11 Part 2.3.11 She Procedures - Permit To Work Systebryanpastor106No ratings yet
- Annual Training Calender Eti 12Document1 pageAnnual Training Calender Eti 12anand shankarNo ratings yet
- PT BUMI MOROWALI UTAMA HSE Monthly ReportDocument9 pagesPT BUMI MOROWALI UTAMA HSE Monthly ReportHifni GhazaliNo ratings yet
- Ho 89Document1 pageHo 89Shanmugam AnnamalaiNo ratings yet
- IAEA PPE SpecificationDocument4 pagesIAEA PPE SpecificationRoberto CarlosNo ratings yet
- Part Submission WarrantDocument4 pagesPart Submission WarrantSam AnuNo ratings yet
- EOHSMS-02-F06 Hot Work PermitDocument2 pagesEOHSMS-02-F06 Hot Work PermitHassan AbdullahNo ratings yet
- Welding Workshop Layout GuideDocument1 pageWelding Workshop Layout GuideAna Rosel Olaran AtonNo ratings yet
- LCAM Whitepaper 204 PDFDocument7 pagesLCAM Whitepaper 204 PDFShashank JainNo ratings yet
- Fall Protection Equipment Inspection ChecklistDocument2 pagesFall Protection Equipment Inspection ChecklistCristinaNo ratings yet
- What Is PSMDocument2 pagesWhat Is PSMChawki Zerrouki100% (1)
- SOP 4 - Coal Bed Leveling in PGPDocument18 pagesSOP 4 - Coal Bed Leveling in PGPfaraz ahmedNo ratings yet
- Lab Design Guide ChecklistDocument9 pagesLab Design Guide ChecklistTanveer AzizNo ratings yet
- Blasting & Painting Report: Surface PreparationDocument1 pageBlasting & Painting Report: Surface PreparationSandra SandersNo ratings yet
- Job Safety Analysis: JSA Basic DataDocument5 pagesJob Safety Analysis: JSA Basic DataPrabhu DivakaranNo ratings yet
- Complacency - Safety Toolbox Talks Meeting TopicsDocument2 pagesComplacency - Safety Toolbox Talks Meeting TopicsqhseNo ratings yet
- Activity-Based Risk Assessment BesmarDocument9 pagesActivity-Based Risk Assessment Besmardwi_6188No ratings yet
- HSE Inspection Checklist: 1 Safety PromotionDocument4 pagesHSE Inspection Checklist: 1 Safety PromotionRanjan PrNo ratings yet
- HSE Safety Permit to Work ProcedureDocument32 pagesHSE Safety Permit to Work Proceduregobi100% (1)
- Audit ChecklistDocument25 pagesAudit ChecklistMaria Luciana GusmãoNo ratings yet
- EHS 2-F8 PTW LiftingDocument2 pagesEHS 2-F8 PTW LiftingLee Xiao YuNo ratings yet
- Augustine - O - Olumoye - 16 - Yrs Oil Gas - HSE MANAGERDocument4 pagesAugustine - O - Olumoye - 16 - Yrs Oil Gas - HSE MANAGERTheophilus Muyiwa100% (1)
- IGN 07 Working at Height and Working at Height Rescue PlanDocument75 pagesIGN 07 Working at Height and Working at Height Rescue Planin123No ratings yet
- TPIP ManualDocument53 pagesTPIP ManualMurugananthamParamasivamNo ratings yet
- Habits of Effective Safety ManagersDocument7 pagesHabits of Effective Safety ManagersNiraNo ratings yet
- Installer Instructions: WWW - Etnice.co - ZaDocument20 pagesInstaller Instructions: WWW - Etnice.co - ZaJack SmithNo ratings yet
- Electric Arc Welder Risk ManagementDocument9 pagesElectric Arc Welder Risk ManagementpankajNo ratings yet
- Welding Shop Environmental PolicyDocument1 pageWelding Shop Environmental PolicyMuhammad UmarNo ratings yet
- PSI Inspection SheetDocument9 pagesPSI Inspection SheetSalman BankariNo ratings yet
- SWP - 21!06!2019 (Demolish Existing Ceiling & Raised Floor)Document4 pagesSWP - 21!06!2019 (Demolish Existing Ceiling & Raised Floor)Jhon Luther PNo ratings yet
- Safety Pre-Task AssignmentDocument2 pagesSafety Pre-Task AssignmentSathiya SeelanNo ratings yet
- 08C Supbook STADocument2 pages08C Supbook STAMohammed MinhajNo ratings yet
- Weekly Repot 20 Juli - 26 JuliDocument6 pagesWeekly Repot 20 Juli - 26 JuliJhon Luther PNo ratings yet
- Weather Report: Month: May-22 Project: AAJ - Marunda Location: Marunda - Jakarta UtaraDocument1 pageWeather Report: Month: May-22 Project: AAJ - Marunda Location: Marunda - Jakarta UtaraJhon Luther PNo ratings yet
- Weather Report: Month: Apr-22 Project: AAJ - Marunda Location: Marunda - Jakarta UtaraDocument1 pageWeather Report: Month: Apr-22 Project: AAJ - Marunda Location: Marunda - Jakarta UtaraJhon Luther PNo ratings yet
- Weekly - Report - HSE - 5 JULI-12 - JuLI - 2019Document9 pagesWeekly - Report - HSE - 5 JULI-12 - JuLI - 2019Jhon Luther PNo ratings yet
- Hse Workplace Condition Inspection (Wci) Hazard / Non-Conformance FormDocument9 pagesHse Workplace Condition Inspection (Wci) Hazard / Non-Conformance FormJhon Luther PNo ratings yet
- HDL 1 September 2019Document1 pageHDL 1 September 2019Jhon Luther PNo ratings yet
- Office door installation notesDocument1 pageOffice door installation notesJhon Luther PNo ratings yet
- 7 September 2019 Attendance ListDocument2 pages7 September 2019 Attendance ListJhon Luther PNo ratings yet
- HDL 3 Agustus 2019Document3 pagesHDL 3 Agustus 2019Jhon Luther PNo ratings yet
- SWP - 21!06!2019 (Demolish Existing Ceiling & Raised Floor)Document4 pagesSWP - 21!06!2019 (Demolish Existing Ceiling & Raised Floor)Jhon Luther PNo ratings yet
- Weekly Repot 20 Juli - 26 JuliDocument6 pagesWeekly Repot 20 Juli - 26 JuliJhon Luther PNo ratings yet
- Weekly Repot 20 Juli - 26 JuliDocument6 pagesWeekly Repot 20 Juli - 26 JuliJhon Luther PNo ratings yet
- Absensi Juni & Juli 2019: JL Pejompongan Dalam No. 16 Bendungan Hilir, Tanah Abang TLP 021 57901232 Fax 021 52906772Document1 pageAbsensi Juni & Juli 2019: JL Pejompongan Dalam No. 16 Bendungan Hilir, Tanah Abang TLP 021 57901232 Fax 021 52906772Jhon Luther PNo ratings yet
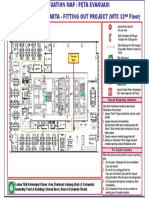
- EVACUATION MAPDocument1 pageEVACUATION MAPJhon Luther PNo ratings yet
- Boll Filter Protection System ProgramDocument38 pagesBoll Filter Protection System ProgramsridarNo ratings yet
- Sds - Bengalac Woodprimer - English (Uk) - DubaiDocument5 pagesSds - Bengalac Woodprimer - English (Uk) - DubaiBalasubramanian AnanthNo ratings yet
- Lactarin® DX 2017 Carrageenan - FMC CorporationDocument8 pagesLactarin® DX 2017 Carrageenan - FMC CorporationAna RidaoNo ratings yet
- 3094 User Manual XP KongsbergDocument200 pages3094 User Manual XP KongsbergRadoNo ratings yet
- Isobutanol PDFDocument11 pagesIsobutanol PDFElías VillegasNo ratings yet
- MES-Service-Manual Indeco PDFDocument141 pagesMES-Service-Manual Indeco PDFFastcross Honda100% (2)
- Incident Reporting ProcedureDocument24 pagesIncident Reporting ProcedureAiza Tancinco Bautista100% (1)
- Emergency Contact Information: Your Name Address City, State, Zip Telephone Special DirectionsDocument2 pagesEmergency Contact Information: Your Name Address City, State, Zip Telephone Special DirectionsVictor Hugo Calvanapón SalasNo ratings yet
- 492 MSDSDocument5 pages492 MSDSsrinivignaNo ratings yet
- JSA Mechanical Plant and Machinery SafetyDocument8 pagesJSA Mechanical Plant and Machinery SafetyMazlan AshaariNo ratings yet
- Uniform TCC Final 2024-2025Document31 pagesUniform TCC Final 2024-2025satriaNo ratings yet
- 5 PpeDocument81 pages5 PpeShiella Marie PacturanNo ratings yet
- MTU 2000 M94 OperationDocument153 pagesMTU 2000 M94 OperationDimas Saputro100% (1)
- Sebu7147-05 SDocument19 pagesSebu7147-05 SingjoseosunaNo ratings yet
- MSDS - FlourDocument4 pagesMSDS - FlourMichael RujuwaNo ratings yet
- Workplace Inspection Checklist BlankDocument7 pagesWorkplace Inspection Checklist BlanksifuclenNo ratings yet
- MS-BA400-v3 ENGDocument234 pagesMS-BA400-v3 ENGLabor PrimaNo ratings yet
- File 1416992597Document9 pagesFile 1416992597Roberto BrionesNo ratings yet
- Aircraft Hangar Safety Checklist - Protect Your STDocument8 pagesAircraft Hangar Safety Checklist - Protect Your STMohamad Abu hayyehNo ratings yet
- Twinson Composite Decking InstallationDocument17 pagesTwinson Composite Decking InstallationpbrilhanteNo ratings yet
- JSA-003 Excavation & BackfillingDocument3 pagesJSA-003 Excavation & Backfillingba ratnaparkhe100% (1)
- MSDS - Alkyd Enamel Paint (Cat Avian) PDFDocument11 pagesMSDS - Alkyd Enamel Paint (Cat Avian) PDFbumisetraNo ratings yet
- Rtaf SVX001C en - 11252015Document106 pagesRtaf SVX001C en - 11252015Thiraviam AyyappanNo ratings yet
- POW Montealegre (Final) 3Document131 pagesPOW Montealegre (Final) 3Leah Mamanao100% (1)
- Study Guide for Safety SupervisorsDocument240 pagesStudy Guide for Safety SupervisorsAsif Hussain92% (13)
- DPWHDocument276 pagesDPWHjovitangel100% (4)
- Disaster in Nursing 2Document70 pagesDisaster in Nursing 2wulanNo ratings yet
- Safety MagnalenzDocument29 pagesSafety MagnalenzBruno ThiemeNo ratings yet
- Compact Gas Ramp - Product Manual - enDocument38 pagesCompact Gas Ramp - Product Manual - enSalman Khalid ChauhanNo ratings yet
- Memorandum of Agreement For Work Immersion PartnershipDocument9 pagesMemorandum of Agreement For Work Immersion PartnershipAilene Heramil Ponio100% (5)