You might also like
- FDA Guidance Target Product ProfileDocument25 pagesFDA Guidance Target Product Profileisoasp100% (1)
- Sedation of Patients in ICUDocument9 pagesSedation of Patients in ICUAlfrin AntonyNo ratings yet
- Dosages and CalculationDocument107 pagesDosages and CalculationNomi Waqas GulNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol 2mg-ml DropsDocument15 pagesHaloperidol 2mg-ml Dropsddandan_2No ratings yet
- Health Canada - HaloperidolDocument25 pagesHealth Canada - HaloperidolIndrie LestarieNo ratings yet
- Haloperidol Drug StudyDocument3 pagesHaloperidol Drug StudyAysaaa DCNo ratings yet
- HaloperidolDocument4 pagesHaloperidolNickol BaylonNo ratings yet
- Haldol 5mg: (Haloperidol)Document17 pagesHaldol 5mg: (Haloperidol)ddandan_2No ratings yet
- Haldol DecanoasDocument8 pagesHaldol Decanoastatih_meilaniNo ratings yet
- Drug Study HaldolDocument2 pagesDrug Study HaldolGracia EvangelistaNo ratings yet
- Halcion Triazolam Tablets, USP CIV: DescriptionDocument14 pagesHalcion Triazolam Tablets, USP CIV: DescriptionAlberto JaramilloNo ratings yet
- HaloperidolDocument9 pagesHaloperidolteguh aminNo ratings yet
- Clinical Medications WorksheetsDocument3 pagesClinical Medications WorksheetsVinz OñoNo ratings yet
- AntipsychoticsDocument24 pagesAntipsychoticsSashin DissanayakeNo ratings yet
- Drug StudyDocument12 pagesDrug StudyAngeli A EstilloreNo ratings yet
- DonepezilDocument8 pagesDonepezilhabi_smNo ratings yet
- Drug Study 2019Document14 pagesDrug Study 2019Aubrey Unique Evangelista100% (1)
- Obat-Obat Psychiatry - 1 2018Document104 pagesObat-Obat Psychiatry - 1 2018Christo LimbongNo ratings yet
- Furosemide HaloperidolDocument6 pagesFurosemide HaloperidolLady Lou ArmadaNo ratings yet
- Aripiprazol in Delirium La Pacientii VarstniciDocument10 pagesAripiprazol in Delirium La Pacientii VarstniciRobert MovileanuNo ratings yet
- Drug PresentationDocument32 pagesDrug PresentationManisha ShakyaNo ratings yet
- PHARMACOLOGY OF PSYCHOSIS AND MANIADocument53 pagesPHARMACOLOGY OF PSYCHOSIS AND MANIAlavanyakakarlaNo ratings yet
- Ativan CIV Tablets: R OnlyDocument8 pagesAtivan CIV Tablets: R OnlyP KasikrishnarajaNo ratings yet
- Centrally Acting Alpha Agonist Lowers BP & HRDocument4 pagesCentrally Acting Alpha Agonist Lowers BP & HRAriadne MangondatoNo ratings yet
- Antipsychotics,-WPS OfficeDocument7 pagesAntipsychotics,-WPS Officermconvidhya sri2015No ratings yet
- Psychia Drug StudyDocument11 pagesPsychia Drug StudyJustin 葉志明 Yap Delapaz100% (1)
- Side Effects.: Aripiprazole (Abilify)Document3 pagesSide Effects.: Aripiprazole (Abilify)Vera El Sammah SiagianNo ratings yet
- QuetiapineDocument3 pagesQuetiapineMichael KuzbytNo ratings yet
- Side Effects:: AtropineDocument7 pagesSide Effects:: AtropinekletadaNo ratings yet
- Drug Study of SchizophreniaDocument17 pagesDrug Study of SchizophreniaCLOYD MARVINNo ratings yet
- Metoclopromide Drug StudyDocument4 pagesMetoclopromide Drug Studymarklesterdeguzman087No ratings yet
- Anti Psychotic DrugDocument25 pagesAnti Psychotic DrugANI SAMNo ratings yet
- Drug StudyDocument7 pagesDrug StudyJohn Paulo MataNo ratings yet
- Clozapine, Quetiapine, Biperiden, and Fluphenazine Drug StudyDocument6 pagesClozapine, Quetiapine, Biperiden, and Fluphenazine Drug StudyRegine Lorenzana Mey-AngNo ratings yet
- Drug Mechanism of Action Indication Nursing ResponsibilitiesDocument5 pagesDrug Mechanism of Action Indication Nursing ResponsibilitiesShara SampangNo ratings yet
- Ospolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)Document7 pagesOspolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)ddandan_2No ratings yet
- Drug StudyDocument12 pagesDrug StudyMeraflor BahonsuaNo ratings yet
- Seroquel (Quetiapine)Document3 pagesSeroquel (Quetiapine)E100% (1)
- Psychopharmacology in PsychiatryDocument94 pagesPsychopharmacology in PsychiatryOslo SaputraNo ratings yet
- Module 8Document5 pagesModule 8Yuki Xairah TunayNo ratings yet
- Therapeutics II - 1Document9 pagesTherapeutics II - 1shukranamer2No ratings yet
- HaloperidolDocument15 pagesHaloperidolfachsyarNo ratings yet
- Soumya Mary 1 Year MSC (N)Document24 pagesSoumya Mary 1 Year MSC (N)Salman HabeebNo ratings yet
- Anti Psychotic DrugsDocument6 pagesAnti Psychotic DrugsJoseph NyirongoNo ratings yet
- Nortriptyline Tablets Prescribing InformationDocument10 pagesNortriptyline Tablets Prescribing InformationMirza MarufNo ratings yet
- Drug StudyDocument7 pagesDrug StudyMariCris CaronanNo ratings yet
- Antipsychotic Drugs - Wafa Bin ShamlanDocument8 pagesAntipsychotic Drugs - Wafa Bin ShamlanSara AbdoNo ratings yet
- Antipsychotic Drugs DESKTOP MHAO1SHDocument17 pagesAntipsychotic Drugs DESKTOP MHAO1SHjanemwanza003No ratings yet
- Drug Study-Grand Case PresDocument8 pagesDrug Study-Grand Case PresLorina Lynne ApelacioNo ratings yet
- Delirium: An Acute Fluctuating DisturbanceDocument22 pagesDelirium: An Acute Fluctuating DisturbanceJose AndinoNo ratings yet
- Antipsychotic Drugs: Eduviere A.TDocument19 pagesAntipsychotic Drugs: Eduviere A.TOmaraye JoshuaNo ratings yet
- Antipsychotics 2017Document57 pagesAntipsychotics 2017bakhtawar shaikhNo ratings yet
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcFrom EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcNo ratings yet
- SULPYCO Method: A New Quantum and Integrative Approach to DepressionFrom EverandSULPYCO Method: A New Quantum and Integrative Approach to DepressionNo ratings yet
- Chemical Activity of AntipsychoticsDocument3 pagesChemical Activity of Antipsychoticsteguh aminNo ratings yet
- NEUROTRANSMITTER AND PharmacologyDocument36 pagesNEUROTRANSMITTER AND Pharmacologyteguh aminNo ratings yet
- NEUROTRANSMITTER AND PharmacologyDocument36 pagesNEUROTRANSMITTER AND Pharmacologyteguh aminNo ratings yet
- IELTS Assessment Criteria - SPEAKING - Band DescriptorsDocument1 pageIELTS Assessment Criteria - SPEAKING - Band DescriptorsIbrahim Babatunde OladapoNo ratings yet
- HaloperidolDocument9 pagesHaloperidolteguh aminNo ratings yet
- Trihexyphenidyl: PronunciationDocument4 pagesTrihexyphenidyl: Pronunciationteguh aminNo ratings yet
- Trihexyphenidyl 2Document4 pagesTrihexyphenidyl 2teguh aminNo ratings yet
- Faktor Kekambuhan Pasien SkizoDocument6 pagesFaktor Kekambuhan Pasien SkizoFadlan ADima AdriantaNo ratings yet
- Chlorpromazine: Why Is This Medication Prescribed?Document3 pagesChlorpromazine: Why Is This Medication Prescribed?teguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Word Cara Baca Meaning Hafal CentangDocument15 pagesWord Cara Baca Meaning Hafal Centangteguh aminNo ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Chemical Activity of AntipsychoticsDocument3 pagesChemical Activity of Antipsychoticsteguh aminNo ratings yet
- Band Descriptors for IELTS Writing TasksDocument2 pagesBand Descriptors for IELTS Writing TasksChortle2099No ratings yet
- Haloperidol: Brand Name: HaldolDocument15 pagesHaloperidol: Brand Name: Haldolteguh aminNo ratings yet
- Chlorpromazine: Why Is This Medication Prescribed?Document3 pagesChlorpromazine: Why Is This Medication Prescribed?teguh aminNo ratings yet
- KKKDocument3 pagesKKKteguh aminNo ratings yet
- Ipi 432103Document6 pagesIpi 432103Yetty SukmayaniNo ratings yet
- ANALISIS MINAT PENGGUNAAN PROGRAM PENYAKIT KRONISDocument21 pagesANALISIS MINAT PENGGUNAAN PROGRAM PENYAKIT KRONISteguh aminNo ratings yet
- Baygon MSDSDocument9 pagesBaygon MSDSRobert FlorezNo ratings yet
- MDR - Oral Boomer PDFDocument15 pagesMDR - Oral Boomer PDFBandameedi RamuNo ratings yet
- A Geometric Series Is The Sum of The Terms of A Geometric SequenceDocument30 pagesA Geometric Series Is The Sum of The Terms of A Geometric SequenceMary ann GarciaNo ratings yet
- Laboratory Blood Request FormDocument2 pagesLaboratory Blood Request FormIsaac AgbemafleNo ratings yet
- Vice and DrugDocument8 pagesVice and DrugTIPAY, EMELIE L.No ratings yet
- Mango Peel PectinDocument9 pagesMango Peel Pectinjesindha beyatricksNo ratings yet
- Topical Anti-Infectives: Indications, Contraindications, Dosing & Side EffectsDocument12 pagesTopical Anti-Infectives: Indications, Contraindications, Dosing & Side EffectsMabusiNo ratings yet
- PoultryVaccinesGuide Int HDDocument96 pagesPoultryVaccinesGuide Int HDNaumanNo ratings yet
- Xylooligosaccharide - A Valuable Material From Waste To Taste: A ReviewDocument10 pagesXylooligosaccharide - A Valuable Material From Waste To Taste: A ReviewWaqas Bin Niaz AwanNo ratings yet
- Drug Related ProblemsDocument40 pagesDrug Related Problemsfauzul husnaNo ratings yet
- Prelim - DDS Lec TransesDocument5 pagesPrelim - DDS Lec TransesCatherine SsiNo ratings yet
- RS199.S73S29 2018Document212 pagesRS199.S73S29 2018amgranadosvNo ratings yet
- Human longevity plateaus at 114 yearsDocument4 pagesHuman longevity plateaus at 114 yearsNaveenNo ratings yet
- NSTP2 Module 4 AssignmentDocument2 pagesNSTP2 Module 4 AssignmentmikomikomikNo ratings yet
- Mirtazapine Toxicity in CatsDocument7 pagesMirtazapine Toxicity in CatsAllana Valau MoreiraNo ratings yet
- Imci WhoDocument58 pagesImci WhoCarl Elexer Cuyugan Ano67% (3)
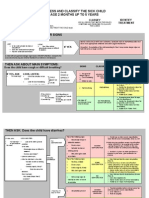
- Assess and Classify The Sick Child Age 2 Months Up To 5 YearsDocument30 pagesAssess and Classify The Sick Child Age 2 Months Up To 5 YearsRommel G. Santiago100% (2)
- Therapeutic Index 18 October 2005Document16 pagesTherapeutic Index 18 October 2005Tabitha JordanNo ratings yet
- TheophyllineDocument6 pagesTheophyllineapi-3797941100% (1)
- Advance in Fish Health ManagementDocument39 pagesAdvance in Fish Health ManagementcrizelbuensucesNo ratings yet
- Permatreat PC-1020T: BenefitsDocument1 pagePermatreat PC-1020T: BenefitsAymen HentatiNo ratings yet
- SE JAN 21 For Sir LouieDocument15 pagesSE JAN 21 For Sir LouieEdna Uneta RoblesNo ratings yet
- Pediatric Case ApproachDocument47 pagesPediatric Case ApproachKenneth NuñezNo ratings yet
- Counseling Tool For PharmacistsDocument3 pagesCounseling Tool For Pharmaciststl drNo ratings yet
- Medical Students Guide to Drug DispensingDocument40 pagesMedical Students Guide to Drug DispensingJIBRIL AHMEDNo ratings yet
- Anthropology AssignmentDocument3 pagesAnthropology AssignmentAhsan AliNo ratings yet
- DRUG NAME: Rituximab: Synonym (S) : Common Trade Name (S) : ClassificationDocument12 pagesDRUG NAME: Rituximab: Synonym (S) : Common Trade Name (S) : ClassificationpmuftiaNo ratings yet
- Pharmacology Exam COHORT 8Document9 pagesPharmacology Exam COHORT 8Lesley Liavoga SandeNo ratings yet