You might also like
- Pathophysiology of Cholera PDFDocument1 pagePathophysiology of Cholera PDFRameshKrishnanNo ratings yet
- Endocrine DisordersDocument2 pagesEndocrine DisordersRalph Elvin MacanlalayNo ratings yet
- Tropical SprueDocument3 pagesTropical SprueAVINASH PvkNo ratings yet
- Path o PhysiologyDocument9 pagesPath o PhysiologyKyle Ü D. CunanersNo ratings yet
- Choler A: Prepared By: Angelou Mortos John Radley SantosDocument11 pagesCholer A: Prepared By: Angelou Mortos John Radley SantosAdhaNo ratings yet
- A) Schematic Diagram (Pathophysiology) - Book Based: Direct Contact, Through Sexual ContactDocument6 pagesA) Schematic Diagram (Pathophysiology) - Book Based: Direct Contact, Through Sexual ContactCyrus Christian CanlasNo ratings yet
- Concept Map MarwahDocument5 pagesConcept Map MarwahAsniah Hadjiadatu AbdullahNo ratings yet
- Type 2 DM PathoDocument5 pagesType 2 DM PathoPearl JuntillaNo ratings yet
- WOC DiareDocument3 pagesWOC DiarenawangNo ratings yet
- Pathophysiology CKD - DrawioDocument54 pagesPathophysiology CKD - DrawioGwyneth CiriloNo ratings yet
- Pathophy - Nephrotic SyndromeedDocument1 pagePathophy - Nephrotic Syndromeedianecunar100% (1)
- Primary Defect: Proteinuria Tertiary Spiral: Compensatory Salt RetentionDocument4 pagesPrimary Defect: Proteinuria Tertiary Spiral: Compensatory Salt RetentionCici Novelia ManurungNo ratings yet
- Adrenal GlandDocument1 pageAdrenal GlandAfiera MurpiNo ratings yet
- Fournier's Gangrene PathophysiologyDocument5 pagesFournier's Gangrene PathophysiologyKAYCEENo ratings yet
- Final - CholeraDocument12 pagesFinal - CholeraCassey Cureg100% (1)
- Pathophysiology of Diabetes Mellitus Type 2Document7 pagesPathophysiology of Diabetes Mellitus Type 2jnrue_aerith96% (28)
- Disease Patho Manifestations Assessment Labs Other Notes DKA Used To Suppress Ketogenesis, Gluconeogenesis NOT Just To Lower BGDocument1 pageDisease Patho Manifestations Assessment Labs Other Notes DKA Used To Suppress Ketogenesis, Gluconeogenesis NOT Just To Lower BGSara SabraNo ratings yet
- Nursing Care Plan Diabetes 2Document3 pagesNursing Care Plan Diabetes 2Ysun Espino100% (1)
- Kelompok Bhs Inggrtios .Id - enDocument16 pagesKelompok Bhs Inggrtios .Id - enAgustinusNo ratings yet
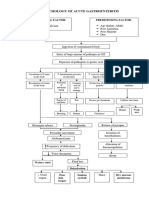
- Pathophysiology of Acute GastroenteritisDocument2 pagesPathophysiology of Acute GastroenteritisIra Velle ViosNo ratings yet
- English of NursingDocument1 pageEnglish of NursingyustiNo ratings yet
- Pa Tho Physiology GastroenteritisDocument2 pagesPa Tho Physiology Gastroenteritisjeneva029No ratings yet
- Ward Class: Acute GastroenteritisDocument4 pagesWard Class: Acute GastroenteritisKate Penelope Dalid100% (1)
- BACTERIADocument1 pageBACTERIAKumkum MahajanNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Primary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Document6 pagesPrimary: Congenital Disease 2. Finnish Nephrotic Syndrome (Inherited) 3. Nephrotic Syndrome Minimal Change (The Most Common Type)Cici Novelia ManurungNo ratings yet
- Assessment Using Functional Health Patterns: AppendixDocument16 pagesAssessment Using Functional Health Patterns: AppendixNalzaro Emyril89% (19)
- Anti - Diarrheal DrugsDocument5 pagesAnti - Diarrheal DrugsFitri NurullahNo ratings yet
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaNo ratings yet
- University of Cebu at Pardo and Talisay, IncDocument4 pagesUniversity of Cebu at Pardo and Talisay, IncMary louicita canadaNo ratings yet
- Drug StudyDocument2 pagesDrug StudyAUBREY GARATENo ratings yet
- Chronic Kidney DiseaseDocument4 pagesChronic Kidney DiseaseImnot YouNo ratings yet
- Diabetes Mellitus Is A Condition in Which A Person Has A High Blood SugarDocument4 pagesDiabetes Mellitus Is A Condition in Which A Person Has A High Blood SugarisonkutonNo ratings yet
- VII. Pathophysiology of PUDDocument1 pageVII. Pathophysiology of PUDJehmima Gloriani100% (1)
- Drug Study D5LRDocument2 pagesDrug Study D5LRCarissa Mae Tapec EstradaNo ratings yet
- MS-2 GallbladderDocument2 pagesMS-2 Gallbladderelijahdale.guillergan-05No ratings yet
- Increased Serum Glucose Level (Hyperglycemia) 278.14 MG/DL (Normal: 70-100 MG/DL)Document3 pagesIncreased Serum Glucose Level (Hyperglycemia) 278.14 MG/DL (Normal: 70-100 MG/DL)Angel FiloteoNo ratings yet
- Pathophysiology of GastroenteritisDocument1 pagePathophysiology of GastroenteritisNathaniel SupanNo ratings yet
- Sodium Bicarbonate Drug StudyDocument3 pagesSodium Bicarbonate Drug StudyShaira Suzane SabidoNo ratings yet
- Pathophysiology of Diabetes Insipidus: DX: Serum ADHDocument3 pagesPathophysiology of Diabetes Insipidus: DX: Serum ADHkristian markus delos santosNo ratings yet
- Acute Diarrhea: MicroorganismDocument5 pagesAcute Diarrhea: MicroorganismAhmed almahdiNo ratings yet
- Pathophysiology of Acute GastroenteritisDocument1 pagePathophysiology of Acute GastroenteritisMay RodeoNo ratings yet
- Gastrointestinal TractDocument63 pagesGastrointestinal Tractsachin pandaoNo ratings yet
- Electrolytes TableDocument4 pagesElectrolytes TableMeg NoriegaNo ratings yet
- Name Classificatio N Action Indication Contraindicati ON Adverse Effect Nursing Responsibilities Generic: Captopril MIDocument4 pagesName Classificatio N Action Indication Contraindicati ON Adverse Effect Nursing Responsibilities Generic: Captopril MIHarvey BanagNo ratings yet
- Case Analysis DehydrationDocument6 pagesCase Analysis DehydrationDayan CabrigaNo ratings yet
- Drug StudyDocument1 pageDrug Studyjasper pachingelNo ratings yet
- Respiratory Disorders of Pediatric Clients-1Document10 pagesRespiratory Disorders of Pediatric Clients-1Genalyn PenuagaNo ratings yet
- SdadsaDocument2 pagesSdadsaDalo ZeronNo ratings yet
- Anatomy of The Pancreas: Regulate Blood Glucose - The Fuel ThatDocument2 pagesAnatomy of The Pancreas: Regulate Blood Glucose - The Fuel ThatSkyerex100% (1)
- Esrd Diagram PathophysiologyDocument3 pagesEsrd Diagram PathophysiologySTEPHANIE JOSUE100% (1)
- 4 Diabetes MellitusDocument26 pages4 Diabetes MellitusnomiskemalNo ratings yet
- Aldosterone: International Series of Monographs in Pure and Applied BiologyFrom EverandAldosterone: International Series of Monographs in Pure and Applied BiologyNo ratings yet
- Fast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentFrom EverandFast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentNo ratings yet
- Arterial Blood Gas Analysis: Ram E. RajagopalanDocument26 pagesArterial Blood Gas Analysis: Ram E. RajagopalanRameshKrishnanNo ratings yet
- QP Code: 101501 Reg. No.: D.M. (Cardiology) Degree Regular/Supplementary Examinations September 2020Document1 pageQP Code: 101501 Reg. No.: D.M. (Cardiology) Degree Regular/Supplementary Examinations September 2020RameshKrishnanNo ratings yet
- Biologic Therapies: What and When?: ReviewDocument10 pagesBiologic Therapies: What and When?: ReviewRameshKrishnanNo ratings yet
- Multiple MyelomaDocument23 pagesMultiple MyelomaRameshKrishnanNo ratings yet
- Poster Ramesh MMDocument5 pagesPoster Ramesh MMRameshKrishnanNo ratings yet
- Multiple Myeloma Presenting As Oral Cavity Lesion: Stand Life SciencesDocument2 pagesMultiple Myeloma Presenting As Oral Cavity Lesion: Stand Life SciencesRameshKrishnanNo ratings yet
- 0 - New Doc 2019-09-26 07.59.08 - 1Document1 page0 - New Doc 2019-09-26 07.59.08 - 1RameshKrishnanNo ratings yet
- Notice For DNB Post MBBS 2020Document1 pageNotice For DNB Post MBBS 2020RameshKrishnanNo ratings yet
- DNB (Post MBBS) January 2019 Counseling (Final Round) - Participation Letter PDFDocument1 pageDNB (Post MBBS) January 2019 Counseling (Final Round) - Participation Letter PDFRameshKrishnanNo ratings yet
- Epicura Hornu: Informed ConsentDocument5 pagesEpicura Hornu: Informed ConsentRameshKrishnanNo ratings yet
- 0 - New Doc 2019-09-26 21.48.53 - 2Document1 page0 - New Doc 2019-09-26 21.48.53 - 2RameshKrishnanNo ratings yet
- General Medicine: Part BDocument1 pageGeneral Medicine: Part BRameshKrishnanNo ratings yet
- General Medicine: Part ADocument1 pageGeneral Medicine: Part ARameshKrishnanNo ratings yet
- 0 - New Doc 2019-09-26 21.48.53 - 1Document1 page0 - New Doc 2019-09-26 21.48.53 - 1RameshKrishnanNo ratings yet
- Topic 5 - Market Forces - SupplyDocument5 pagesTopic 5 - Market Forces - Supplysherryl caoNo ratings yet
- Cs-Stan Issue 4Document180 pagesCs-Stan Issue 4Jan JíchaNo ratings yet
- Rksi NewDocument38 pagesRksi NewFiq OblivioNo ratings yet
- Hammer Group SeptDec 2023Document5 pagesHammer Group SeptDec 2023Adilah AzamNo ratings yet
- IELTS Writing Task 2 Essay SamplesDocument20 pagesIELTS Writing Task 2 Essay Samples27. Minh PhươngNo ratings yet
- Detailed Lesson Plan in TLEDocument7 pagesDetailed Lesson Plan in TLEma kathrine cecille macapagalNo ratings yet
- NEW HOLLAND - Trucks, Tractor & Forklift Manual PDDocument14 pagesNEW HOLLAND - Trucks, Tractor & Forklift Manual PDAjjaakka0% (2)
- Ucsp LM PDFDocument124 pagesUcsp LM PDFAivonny Peñaranda CorbitaNo ratings yet
- Experimentation, Orgasms, and The Rise of Anal Sex. - by William Saletan - SDocument13 pagesExperimentation, Orgasms, and The Rise of Anal Sex. - by William Saletan - Saweawerwerwe100% (1)
- First Degree Price DiscriminationDocument19 pagesFirst Degree Price DiscriminationRavi KiranNo ratings yet
- Pleadings Extrajudicial ConfessionDocument2 pagesPleadings Extrajudicial ConfessionEdcel AndesNo ratings yet
- Rules and Reminders For Online Classes 2Document14 pagesRules and Reminders For Online Classes 2api-220703221No ratings yet
- Tinynet (Mytyvm) : Creating Virtual MachinesDocument38 pagesTinynet (Mytyvm) : Creating Virtual MachinesSayyam ChNo ratings yet
- Cia Rubric For Portfolio Project Submission 2017Document2 pagesCia Rubric For Portfolio Project Submission 2017FRANKLIN.FRANCIS 1640408No ratings yet
- Predestination Vs Free WillDocument4 pagesPredestination Vs Free WillFrancis Heckman100% (2)
- Umali V EstanislaoDocument2 pagesUmali V EstanislaoVian O.No ratings yet
- C-Line Drives Engineering Guide 11-2006-EnDocument568 pagesC-Line Drives Engineering Guide 11-2006-EnysaadanyNo ratings yet
- Random Puzzle Questions PDF For Ibps RRB Clerk Prelims ExamDocument22 pagesRandom Puzzle Questions PDF For Ibps RRB Clerk Prelims ExamApyrvaNo ratings yet
- Spectra of ComplexesDocument41 pagesSpectra of ComplexesSheena GagarinNo ratings yet
- Chowdhury Fatima Rokon Tuli Former Manager Training & Development. Mobile:880-01615769895 Website: Address:483/1, Shewrapara, Mirpur, Dhaka-1216Document4 pagesChowdhury Fatima Rokon Tuli Former Manager Training & Development. Mobile:880-01615769895 Website: Address:483/1, Shewrapara, Mirpur, Dhaka-1216Rabiul AwalNo ratings yet
- The Daily Tar Heel For February 1, 2011Document8 pagesThe Daily Tar Heel For February 1, 2011The Daily Tar HeelNo ratings yet
- CV - Ganis Woro AyuningtyasDocument1 pageCV - Ganis Woro AyuningtyasGanis Woro AyuningtyasNo ratings yet
- Hci - Web Interface DesignDocument54 pagesHci - Web Interface DesigngopivrajanNo ratings yet
- 1power PDFDocument52 pages1power PDFCarlos Alberto Acevedo0% (1)
- Othello JourneyDocument38 pagesOthello Journeyapi-270897909No ratings yet
- Cloning Quiz: Name: Date: ClassDocument1 pageCloning Quiz: Name: Date: ClassPhuong Lien LaiNo ratings yet
- Irjece: Human Computer Interaction Direct ManipulationDocument4 pagesIrjece: Human Computer Interaction Direct ManipulationgigibowonseetNo ratings yet
- An Investigation Into The Use of GAMA Water Tunnel For Visualization of Vortex Breakdown On The Delta WingDocument7 pagesAn Investigation Into The Use of GAMA Water Tunnel For Visualization of Vortex Breakdown On The Delta WingEdy BudimanNo ratings yet
- Desert RoseDocument2 pagesDesert RoseGADAANKITNo ratings yet
- 2 Obstacle Avoiding Robot PDFDocument7 pages2 Obstacle Avoiding Robot PDFRaj AryanNo ratings yet