You might also like
- SampleDocument28 pagesSampleheartandhandstraining_com100% (6)
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- A Study To Evaluate The Effectiveness of Play Therapy in Reducing Post-Operative Pain Among Children Aged 6-12 Years Admitted in Post-Operative Wards, in A Selected Hospital at BengaluruDocument2 pagesA Study To Evaluate The Effectiveness of Play Therapy in Reducing Post-Operative Pain Among Children Aged 6-12 Years Admitted in Post-Operative Wards, in A Selected Hospital at BengaluruInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chemical Peels For The Aging Faces of All Skin TypesDocument12 pagesChemical Peels For The Aging Faces of All Skin TypesGulsher Ahmed100% (2)
- Wound DressingDocument23 pagesWound DressingKryztalGhail Llanora100% (1)
- Week 1 MCQ VMPFDocument25 pagesWeek 1 MCQ VMPFZainab_Wajih_2544100% (1)
- Cohen McqsDocument69 pagesCohen McqsSAEED67% (12)
- Dr. Gopika Solved.Document171 pagesDr. Gopika Solved.Subhajit Saha100% (1)
- Pediatric RehabilitationDocument19 pagesPediatric RehabilitationJustine Rochelle CruzNo ratings yet
- Caring For Your Central LineDocument20 pagesCaring For Your Central Lineapi-311857882No ratings yet
- Piis0002939418302228 PDFDocument9 pagesPiis0002939418302228 PDFadistimayaNo ratings yet
- Jurnal EED 3Document10 pagesJurnal EED 3Garsa GarnolNo ratings yet
- Difluprednato EC U S JOPT 2010 26 5 475 FosterDocument11 pagesDifluprednato EC U S JOPT 2010 26 5 475 FosterMartin MauadNo ratings yet
- UveitisDocument7 pagesUveitissrihandayaniakbarNo ratings yet
- Inter-Grader Agreement in The Diabetic Retinopathy Screening Program in Palestine-IJMBS-2018.Document6 pagesInter-Grader Agreement in The Diabetic Retinopathy Screening Program in Palestine-IJMBS-2018.Riyad BanayotNo ratings yet
- Nejmoa 1310422Document11 pagesNejmoa 1310422mz zumrodinNo ratings yet
- Treating adenoviral conjunctivitis with povidone-iodine and dexamethasoneDocument7 pagesTreating adenoviral conjunctivitis with povidone-iodine and dexamethasoneKurnia22No ratings yet
- Jurnal Andi CitraDocument10 pagesJurnal Andi Citrayusti aisyahNo ratings yet
- International Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsDocument9 pagesInternational Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsPujiNo ratings yet
- Ranibizumab Versus Verteporfin Photodynamic Therapy in Asian Patients With Myopic Choroidal NeovascularizationDocument10 pagesRanibizumab Versus Verteporfin Photodynamic Therapy in Asian Patients With Myopic Choroidal Neovascularizationmeris dindaNo ratings yet
- Prospective, Randomized Clinical Trial ofDocument10 pagesProspective, Randomized Clinical Trial ofFarhan RezaNo ratings yet
- Desprendimiento de RetinaDocument8 pagesDesprendimiento de RetinaDiana Carolina RodríguezNo ratings yet
- Telaah Kritis Jurnal Oftalmologi - Povidone Iodine + DeksamethasoneDocument4 pagesTelaah Kritis Jurnal Oftalmologi - Povidone Iodine + DeksamethasoneKurnia22No ratings yet
- Jurnal EED 6Document10 pagesJurnal EED 6Garsa GarnolNo ratings yet
- Povidone-Iodine vs Antibiotics for Bacterial KeratitisDocument22 pagesPovidone-Iodine vs Antibiotics for Bacterial Keratitisbenefits35No ratings yet
- MataDocument16 pagesMataIslah NadilaNo ratings yet
- Intravitreal Injections Primary Prevention: A Case-Control StudyDocument6 pagesIntravitreal Injections Primary Prevention: A Case-Control StudyZipippo ZNo ratings yet
- J Ajo 2020 03 018Document24 pagesJ Ajo 2020 03 018koas forensikNo ratings yet
- Posaconazole Therapy for Refractory CoccidioidomycosisDocument7 pagesPosaconazole Therapy for Refractory CoccidioidomycosisJavier Saldaña CamposNo ratings yet
- Association of Treatment Adherence With Real-Life VA Outcomes in AMD, DME, and BRVO PatientsDocument8 pagesAssociation of Treatment Adherence With Real-Life VA Outcomes in AMD, DME, and BRVO PatientsmaleticjNo ratings yet
- PIIS0140673620316056Document10 pagesPIIS0140673620316056Isais NNo ratings yet
- Jcrs 48 1242Document6 pagesJcrs 48 1242ririen refrina sariNo ratings yet
- Nocardia Keratitis Clinical Course and TherapyDocument8 pagesNocardia Keratitis Clinical Course and TherapyAuroraNo ratings yet
- 10 1093@jac@dky192Document8 pages10 1093@jac@dky192Rahmad SyamsulNo ratings yet
- Risk of Cataract Development Among Children With Juvenile Idiopathic Arthritis-Related Uveitis Treated With Topical CorticosteroidsDocument6 pagesRisk of Cataract Development Among Children With Juvenile Idiopathic Arthritis-Related Uveitis Treated With Topical CorticosteroidsAnis RanisNo ratings yet
- Comparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisDocument6 pagesComparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisVisakha VidyadeviNo ratings yet
- The Effect of Bevacizumab Versus Ranibizumab in The Treatment of Corneal NeovascularizationDocument8 pagesThe Effect of Bevacizumab Versus Ranibizumab in The Treatment of Corneal NeovascularizationmestevezfNo ratings yet
- Journal Reading - Dr. Monika AyuningrumDocument12 pagesJournal Reading - Dr. Monika Ayuningrumamka chanNo ratings yet
- Treatment Satisfaction Among Patients Using Anti-In Ammatory Topical Medications For Dry Eye DiseaseDocument9 pagesTreatment Satisfaction Among Patients Using Anti-In Ammatory Topical Medications For Dry Eye DiseaseAndrés QueupumilNo ratings yet
- Prasanna Uday Patil, Supriya Sudhir Pendke, Mousumi Bandyopadhyay, Purban GangulyDocument4 pagesPrasanna Uday Patil, Supriya Sudhir Pendke, Mousumi Bandyopadhyay, Purban GangulyMinh NguyenNo ratings yet
- Reliability and Validity of The Ocular Surface Disease IndexDocument7 pagesReliability and Validity of The Ocular Surface Disease Indexpompoo posmmspNo ratings yet
- Ischemia Modified Albumin As A Useful Marker For Diagnoses and Management of Diabetic RetinopathyDocument5 pagesIschemia Modified Albumin As A Useful Marker For Diagnoses and Management of Diabetic RetinopathyMarcellia AngelinaNo ratings yet
- Periocular corticosteroid injections for uveitis effects risksDocument12 pagesPeriocular corticosteroid injections for uveitis effects riskssrihandayaniakbarNo ratings yet
- Analysis of The Clinical Diagnosis and Treatment of UveitisDocument7 pagesAnalysis of The Clinical Diagnosis and Treatment of UveitisRhysandNo ratings yet
- Azithromycin eye drops for pediatric conjunctivitisDocument7 pagesAzithromycin eye drops for pediatric conjunctivitistrianaamaliaNo ratings yet
- PIIS0161642018333281Document14 pagesPIIS0161642018333281Yekiita QuinteroNo ratings yet
- 14 FullDocument7 pages14 FullalexanderplNo ratings yet
- Treatment Outcomes in The DRy Eye Amniotic MembraneDocument5 pagesTreatment Outcomes in The DRy Eye Amniotic MembraneDiny SuprianaNo ratings yet
- Development and Evaluation of A Measure of Patient-Reported Symptoms of BlepharitisDocument6 pagesDevelopment and Evaluation of A Measure of Patient-Reported Symptoms of BlepharitisYulia MagdalenaNo ratings yet
- Research Article 'S Disease: Severity of Ocular: Vision-Threatening Behcet Involvement PredictorsDocument7 pagesResearch Article 'S Disease: Severity of Ocular: Vision-Threatening Behcet Involvement PredictorsdeswitrigintaNo ratings yet
- Peritonitis in Children On Peritoneal Dialysis: 12 Years of Tertiary Center ExperienceDocument7 pagesPeritonitis in Children On Peritoneal Dialysis: 12 Years of Tertiary Center ExperienceMarselya GaniNo ratings yet
- Efficacy of Second-Course Intra-Arterial Chemo-Therapy in Children For Advanced Retinoblastoma Recurrence After Intra-Arterial ChemotherapyDocument4 pagesEfficacy of Second-Course Intra-Arterial Chemo-Therapy in Children For Advanced Retinoblastoma Recurrence After Intra-Arterial ChemotherapyilhamNo ratings yet
- Visual Acuity Recovery Following Traumatic Hyphema in A Pediatric PopulationDocument4 pagesVisual Acuity Recovery Following Traumatic Hyphema in A Pediatric PopulationDian Putri NingsihNo ratings yet
- Remdesivir - BeigelDocument14 pagesRemdesivir - BeigelMaureen KoesnadiNo ratings yet
- Long-Term Outcomes of Pediatric Penetrating Keratoplasty For Herpes Simplex Virus KeratitisDocument6 pagesLong-Term Outcomes of Pediatric Penetrating Keratoplasty For Herpes Simplex Virus KeratitisgallaNo ratings yet
- Figus2020 Article AqueousHumourConcentrationsAftDocument9 pagesFigus2020 Article AqueousHumourConcentrationsAftBK RegulatoryNo ratings yet
- Re-Appraisal of Topical 1% Voriconazole and 5% Natamycin in The Treatment of Fungal KeratitisDocument7 pagesRe-Appraisal of Topical 1% Voriconazole and 5% Natamycin in The Treatment of Fungal KeratitisD.E.P.HNo ratings yet
- Matsuura 2020Document8 pagesMatsuura 2020Ghufrani RismawantiNo ratings yet
- Corneal UlcerDocument6 pagesCorneal UlcerChanifah SitiNo ratings yet
- Rem Desi VirDocument14 pagesRem Desi VirSusanyi ErvinNo ratings yet
- Critical Appraisal Therapy Study (Randomized Controlled Trial)Document7 pagesCritical Appraisal Therapy Study (Randomized Controlled Trial)Putri Dwi KartiniNo ratings yet
- The Effects of Povidone Iodine (PH 4.2) On Patients With Adenoviral ConjunctivitisDocument3 pagesThe Effects of Povidone Iodine (PH 4.2) On Patients With Adenoviral ConjunctivitisShari' Si WahyuNo ratings yet
- Abrar - Anterior Chamber Angle in Aniridia With and Whout GloucomaDocument5 pagesAbrar - Anterior Chamber Angle in Aniridia With and Whout Gloucomabudi haryadiNo ratings yet
- Acyclovir in Pityriasis Rosea: An Observer Blind, Randomized Controlled Trial of Effectiveness, Safety and TolerabilityDocument4 pagesAcyclovir in Pityriasis Rosea: An Observer Blind, Randomized Controlled Trial of Effectiveness, Safety and TolerabilityAyyub ParkovicNo ratings yet
- Easy Pharyngeal Anesthesia with Lidocaine LozengesDocument6 pagesEasy Pharyngeal Anesthesia with Lidocaine LozengespaulaNo ratings yet
- Results of Dexamethasone Intravitreal Implant (Ozurdex) in Diabetic Macular Edema Patients: Early Versus Late SwitchDocument11 pagesResults of Dexamethasone Intravitreal Implant (Ozurdex) in Diabetic Macular Edema Patients: Early Versus Late SwitchPutri kartiniNo ratings yet
- Incidence and Management of Symptomatic Dry Eye Related To Lasik For Myopia, With Topical Cyclosporine ADocument8 pagesIncidence and Management of Symptomatic Dry Eye Related To Lasik For Myopia, With Topical Cyclosporine Aamirah sinumNo ratings yet
- Clinical Outcomes of Esophagogastroduodenoscopy In.27Document6 pagesClinical Outcomes of Esophagogastroduodenoscopy In.27Agung KaryawinaraNo ratings yet
- Jurnal Ci BangkalanDocument7 pagesJurnal Ci BangkalanLidwina DewiNo ratings yet
- Jurnal Labor and DeliveryDocument9 pagesJurnal Labor and DeliveryLidwina DewiNo ratings yet
- Clinical Characteristics and Psychosocial Impact of Different Reflux Time in Gastroesophageal Reflux Disease PatientsDocument6 pagesClinical Characteristics and Psychosocial Impact of Different Reflux Time in Gastroesophageal Reflux Disease PatientsLidwina DewiNo ratings yet
- Living Alone (Depression)Document10 pagesLiving Alone (Depression)Lidwina DewiNo ratings yet
- Highlights: 2017 G P, D, e M H B P ADocument2 pagesHighlights: 2017 G P, D, e M H B P AJamie LittleNo ratings yet
- The Beneficial Effect of Physical Exercise On Cognitive Function in A Non-Dementia Aging Chinese PopulationDocument8 pagesThe Beneficial Effect of Physical Exercise On Cognitive Function in A Non-Dementia Aging Chinese PopulationLidwina DewiNo ratings yet
- The Ef Cacy and Safety of Clotrimazole Vaginal Tablet vs. Oral Fuconazole in Treating Severe Vulvovaginal CandidiasisDocument10 pagesThe Ef Cacy and Safety of Clotrimazole Vaginal Tablet vs. Oral Fuconazole in Treating Severe Vulvovaginal CandidiasisLidwina DewiNo ratings yet
- 2019 Article 1175 PDFDocument14 pages2019 Article 1175 PDFLidwina DewiNo ratings yet
- Konjungtivitis VirusDocument9 pagesKonjungtivitis VirusLidwina DewiNo ratings yet
- Duration of Oral Tetracycline-Class Antibiotic Therapy and Use of Topical Retinoids For The Treatment of Acne Among General Practitioners (GP) : A Retrospective Cohort StudyDocument10 pagesDuration of Oral Tetracycline-Class Antibiotic Therapy and Use of Topical Retinoids For The Treatment of Acne Among General Practitioners (GP) : A Retrospective Cohort StudySalomo Galih NugrohoNo ratings yet
- Vitiligo ObatDocument6 pagesVitiligo ObatLidwina DewiNo ratings yet
- 1Document12 pages1Lidwina DewiNo ratings yet
- Nefrologi 6 GgapgkDocument20 pagesNefrologi 6 GgapgkAry ChendrianyNo ratings yet
- 1Document12 pages1Lidwina DewiNo ratings yet
- CamScanner document scansDocument34 pagesCamScanner document scansLidwina DewiNo ratings yet
- The Effectiveness of Levocetirizine and Desloratadine in Up To 4 Times Conventional Doses in Difficult-To-Treat UrticariaDocument7 pagesThe Effectiveness of Levocetirizine and Desloratadine in Up To 4 Times Conventional Doses in Difficult-To-Treat UrticariaLidwina DewiNo ratings yet
- Journal of Autoimmunity: SciencedirectDocument18 pagesJournal of Autoimmunity: SciencedirectLidwina DewiNo ratings yet
- Highlights: 2017 G P, D, e M H B P ADocument2 pagesHighlights: 2017 G P, D, e M H B P AJamie LittleNo ratings yet
- 127488-Jurnal 11Document11 pages127488-Jurnal 11Lidwina DewiNo ratings yet
- New Discoveries in The Pathogenesis and Classification of VitiligoDocument13 pagesNew Discoveries in The Pathogenesis and Classification of VitiligoLidwina DewiNo ratings yet
- Impetigo ScabiesDocument7 pagesImpetigo ScabiesLidwina DewiNo ratings yet
- AcneDocument4 pagesAcneLidwina DewiNo ratings yet
- Intravenous Thrombolysis For Acute Ischemic Stroke Due To Cervical Internal Carotid Artery OcclusionDocument7 pagesIntravenous Thrombolysis For Acute Ischemic Stroke Due To Cervical Internal Carotid Artery OcclusionLidwina DewiNo ratings yet
- Failure To Thrive: SECTION 3 Gastrointestinal DisordersDocument20 pagesFailure To Thrive: SECTION 3 Gastrointestinal DisordersLidwina DewiNo ratings yet
- Journal of Dermatological ScienceDocument6 pagesJournal of Dermatological ScienceLidwina DewiNo ratings yet
- 127488-Jurnal 11Document11 pages127488-Jurnal 11Lidwina DewiNo ratings yet
- Jurnal AnakDocument7 pagesJurnal AnakLidwina DewiNo ratings yet
- AcneDocument4 pagesAcneLidwina DewiNo ratings yet
- Youth at Risk Screening QuestionnaireDocument2 pagesYouth at Risk Screening Questionnaireapi-234873915100% (1)
- Regimental TherapyDocument39 pagesRegimental Therapyafira khanamNo ratings yet
- Pharmacy Daily 29th Nov 2023Document2 pagesPharmacy Daily 29th Nov 2023Marinero CzarNo ratings yet
- Chapter II FinalDocument7 pagesChapter II FinalBianca MelendresNo ratings yet
- Tele rehab OA 2Document11 pagesTele rehab OA 2Kavya MittalNo ratings yet
- Ovarian Germ Cell Tumors TreatmentDocument6 pagesOvarian Germ Cell Tumors TreatmentSoleh SundawaNo ratings yet
- Ayurveda JournalsDocument4 pagesAyurveda JournalsHarish Ayu LNo ratings yet
- Effects of Cold Therapy On Pain and Breathing Exercises Among Median Sternotomy PatientsDocument10 pagesEffects of Cold Therapy On Pain and Breathing Exercises Among Median Sternotomy PatientsMedhia IqlimaNo ratings yet
- Academic Stress and Mental Health Among Students' LearningDocument11 pagesAcademic Stress and Mental Health Among Students' LearningPat0% (1)
- Essay AssignmentDocument3 pagesEssay AssignmentJoshua Casas100% (1)
- Mark Richardson PHD Risk Assessment of Two Dental MaterialsDocument32 pagesMark Richardson PHD Risk Assessment of Two Dental MaterialsMercury ExposureNo ratings yet
- HalitosisDocument6 pagesHalitosispratyusha vallamNo ratings yet
- Anterograde AmnesiaDocument3 pagesAnterograde AmnesiaKavin RagawanNo ratings yet
- Tinea PedisDocument4 pagesTinea PediskirustagyNo ratings yet
- Caries Risk Assessment Form (Age 6) : Contributing Conditions Check or Circle The Conditions That ApplyDocument2 pagesCaries Risk Assessment Form (Age 6) : Contributing Conditions Check or Circle The Conditions That ApplysayacitraNo ratings yet
- OA Case #Q1Document6 pagesOA Case #Q1Asma AlfaouriNo ratings yet
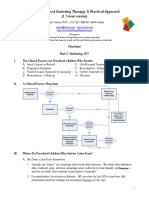
- Early Childhood Stuttering Therapy: A Practical Approach: (1.5-Hour Version)Document12 pagesEarly Childhood Stuttering Therapy: A Practical Approach: (1.5-Hour Version)Sobia HumairaNo ratings yet
- Ithihasa&AbbreviationsDocument17 pagesIthihasa&AbbreviationsSree DivyaNo ratings yet
- Parkinson: Nursing Care ManagementDocument44 pagesParkinson: Nursing Care ManagementPIPIT0% (1)
- 5 Plantarfasciitis Exercises1Document2 pages5 Plantarfasciitis Exercises1Fahmi Nur SuwandiNo ratings yet
- 10 Scientifically Proven Health Benefits of Taking A BathDocument6 pages10 Scientifically Proven Health Benefits of Taking A BathKiara Isabel Dela VegaNo ratings yet