You might also like
- A Stepwise Approach To Acid Base Disorders in ICUDocument71 pagesA Stepwise Approach To Acid Base Disorders in ICUVishal Prabhu100% (3)
- Acid-Base DisorderDocument68 pagesAcid-Base DisorderPrafulla Paudel100% (3)
- Emergency MedicineDocument42 pagesEmergency Medicinedrliza75% (8)
- Acid Base BalanceDocument6 pagesAcid Base BalanceRahul Mehta100% (2)
- Picu NotesDocument65 pagesPicu NotesAhmed Mohammed100% (2)
- Arterial Blood Gas Interpretation – A case study approachFrom EverandArterial Blood Gas Interpretation – A case study approachRating: 1 out of 5 stars1/5 (1)
- Albumin prescribing guide for volume deficitsDocument14 pagesAlbumin prescribing guide for volume deficitsMaria Chona Penillos HularNo ratings yet
- Stan Checketts DocumentationDocument2 pagesStan Checketts Documentationnikdolly50% (4)
- Vasopressors and InotropesDocument31 pagesVasopressors and InotropesReza Prakosa SedyatamaNo ratings yet
- Acid-Base Balance ExplainedDocument8 pagesAcid-Base Balance ExplainedNicole TangcoNo ratings yet
- PALS Study GuideDocument25 pagesPALS Study GuideVitor Hugo G CorreiaNo ratings yet
- AbgDocument52 pagesAbgm07wwpNo ratings yet
- Clinical Guidelines in PediatricsDocument267 pagesClinical Guidelines in PediatricsDrshaukat N PanjawaniNo ratings yet
- Pals CasesDocument24 pagesPals CasesPaíto San Martín100% (16)
- Shock: Classification and PathophysiologyDocument15 pagesShock: Classification and PathophysiologyAishwaray KohliNo ratings yet
- Acid-Base DisordersDocument11 pagesAcid-Base DisordersShia LevyNo ratings yet
- ITLS Advanced Pre-Test PDFDocument8 pagesITLS Advanced Pre-Test PDFmorne9ferreira100% (1)
- Acid Base DisordersDocument11 pagesAcid Base DisordersS100% (1)
- Acid Base HomeostasisDocument11 pagesAcid Base HomeostasisOrion JohnNo ratings yet
- Algo StrokeDocument2 pagesAlgo StrokeLocomotorica FK Uki100% (1)
- The Kidneys Role in Maintaining Acid-Base HomeostasisDocument17 pagesThe Kidneys Role in Maintaining Acid-Base HomeostasisMaggieLocke100% (1)
- Renal-Acid Base BalanceDocument31 pagesRenal-Acid Base BalanceMai Kutin KoakNo ratings yet
- Cardio RenalDocument11 pagesCardio RenalAgung WistaraNo ratings yet
- Maintaining Normal PH Through BuffersDocument40 pagesMaintaining Normal PH Through BuffersRJ Noor JanNo ratings yet
- (Final) ACID BASE BALANCEDocument68 pages(Final) ACID BASE BALANCEPauline SalvadorNo ratings yet
- Acid Secretion by The KidneyDocument37 pagesAcid Secretion by The KidneyHakimah K. Suhaimi100% (1)
- 9 - (D) Acid Base Balance Dec 4.17Document61 pages9 - (D) Acid Base Balance Dec 4.17khaledNo ratings yet
- Physiological Buffers and Maintaining EquilibriumDocument12 pagesPhysiological Buffers and Maintaining EquilibriumLuke ShantiNo ratings yet
- Understanding Acid-Base BalanceDocument43 pagesUnderstanding Acid-Base Balanceanju KvNo ratings yet
- Acid-Base Homeostasis: Clin J Am Soc Nephrol. 10.2215/CJN.07400715 26597304Document18 pagesAcid-Base Homeostasis: Clin J Am Soc Nephrol. 10.2215/CJN.07400715 26597304Christine SiraitNo ratings yet
- Seminar Presentatio Lamin KDocument17 pagesSeminar Presentatio Lamin KAl-amin KanyiNo ratings yet
- Clinical BiochemistryDocument11 pagesClinical BiochemistryKrushna SaiNo ratings yet
- Acid - Base BalanceDocument13 pagesAcid - Base Balanceadam yassineNo ratings yet
- Acid-Base BalanceDocument6 pagesAcid-Base BalanceStanley OdiraNo ratings yet
- ABG Analysis in Clinical SettingDocument5 pagesABG Analysis in Clinical SettingLord GrimmNo ratings yet
- Blood Gases, PH and Buffer Systems: DefinitionsDocument4 pagesBlood Gases, PH and Buffer Systems: DefinitionsMj TizonNo ratings yet
- Clinical BiochemistryDocument73 pagesClinical BiochemistryEslam NassarNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasLal NandaniNo ratings yet
- Acid-Base Balance ABGs InterpretationDocument30 pagesAcid-Base Balance ABGs InterpretationQusai IbraheemNo ratings yet
- Acid Base Balance 11Document37 pagesAcid Base Balance 11Mustafa KhandgawiNo ratings yet
- O.M.O - Acid Base Balance and DisordersDocument50 pagesO.M.O - Acid Base Balance and DisordersIiiNo ratings yet
- Mechanisms of Acid-Base BalanceDocument23 pagesMechanisms of Acid-Base BalancedvgNo ratings yet
- Acid-Base Disturbances Acid-Base Disturbances Are CommonlyDocument18 pagesAcid-Base Disturbances Acid-Base Disturbances Are CommonlyDAEVINNA FELIZ GALBIZONo ratings yet
- Chapter 1 Acid-Base Regulation: Lesser Amounts of Organic Acid Derive From The FollowingDocument52 pagesChapter 1 Acid-Base Regulation: Lesser Amounts of Organic Acid Derive From The FollowingMarwa RagabNo ratings yet
- Acid Base PhysiologyDocument1 pageAcid Base PhysiologyPrabjot SehmiNo ratings yet
- BCH 201 ModuleDocument15 pagesBCH 201 ModuleJoyNo ratings yet
- Acid Base BalanceDocument35 pagesAcid Base BalanceDhanasvi Dessai100% (1)
- Acid Base PhysiologyDocument54 pagesAcid Base PhysiologyDiana AyónNo ratings yet
- 835 Regulation of Acid Base Balance 2019Document26 pages835 Regulation of Acid Base Balance 2019sanofazal786No ratings yet
- Buffer System: Danica Alyssa C. Cruz, RMTDocument27 pagesBuffer System: Danica Alyssa C. Cruz, RMTDanica Alyssa CruzNo ratings yet
- Module 4 - MARCHMIDTERMfinalmodule Biochemwithpages2021-22Document5 pagesModule 4 - MARCHMIDTERMfinalmodule Biochemwithpages2021-22Maden betoNo ratings yet
- Acid Base Balance Buffers PHDocument12 pagesAcid Base Balance Buffers PHdeepaNo ratings yet
- Other Buffers: The Phosphate Buffer System Is NOT An Important Blood Buffer As Its Concentration Is Too LowDocument3 pagesOther Buffers: The Phosphate Buffer System Is NOT An Important Blood Buffer As Its Concentration Is Too LowtidesenNo ratings yet
- Acid-Base HomeostasisDocument12 pagesAcid-Base Homeostasisuriel1No ratings yet
- Role of Kidney in Acid Base BalanceDocument1 pageRole of Kidney in Acid Base BalanceSumit GaonkerNo ratings yet
- Acid-Base Balance Regulation and DisordersDocument37 pagesAcid-Base Balance Regulation and DisordersSittie RamosNo ratings yet
- Acid Base Im Balance-2a - 3.05.2021Document75 pagesAcid Base Im Balance-2a - 3.05.2021Kavya FouzdarNo ratings yet
- Alkalosis AcidosisDocument13 pagesAlkalosis Acidosismultika80No ratings yet
- Bibliografía PDFDocument13 pagesBibliografía PDFHelio GrullónNo ratings yet
- Acid Base BalanceDocument21 pagesAcid Base BalancevampirekawaiiNo ratings yet
- BASIC CONCEPT OF ACID-BASEDocument30 pagesBASIC CONCEPT OF ACID-BASEYaniNo ratings yet
- Blood Buffer SystemDocument10 pagesBlood Buffer Systemmd hasib munsiNo ratings yet
- Mtap421 BloodgasesDocument11 pagesMtap421 BloodgasesNhelomar ManlinconNo ratings yet
- 2013 Renal Tubular AcidosisDocument13 pages2013 Renal Tubular AcidosisLUIS FRANCISCO GUERRERO MARTÍNEZNo ratings yet
- Acid Base Balance: Acid: A Molecule That Contributes HDocument16 pagesAcid Base Balance: Acid: A Molecule That Contributes HOsama MohamedNo ratings yet
- ACID BASE BALANCE and disordersDocument47 pagesACID BASE BALANCE and disordersShivanand MaliNo ratings yet
- Kesetimbangan Asam BasaDocument49 pagesKesetimbangan Asam BasadindaaputriaNo ratings yet
- School of Physiology: University of The Witwatersrand, JohannesburgDocument19 pagesSchool of Physiology: University of The Witwatersrand, JohannesburgJoel AmoniNo ratings yet
- Acid Base Disturbance - Mpath 1Document30 pagesAcid Base Disturbance - Mpath 1Nadzirah YusofNo ratings yet
- Acid-Base BalanceDocument7 pagesAcid-Base BalanceMichelle Mae JulianaNo ratings yet
- Acid Base PhysiologyDocument12 pagesAcid Base PhysiologyaequNo ratings yet
- Two-Year Outcome After Endovascular Treatment For Acute Ischemic StrokeDocument9 pagesTwo-Year Outcome After Endovascular Treatment For Acute Ischemic Strokedoni anandaNo ratings yet
- Chronic Heart Failure in Adults Diagnosis and Management PDF 66141541311685Document37 pagesChronic Heart Failure in Adults Diagnosis and Management PDF 66141541311685Peter Ivan HadiprajitnoNo ratings yet
- Pembagian JadwalDocument1 pagePembagian JadwalM Fathur Arief KurniawanNo ratings yet
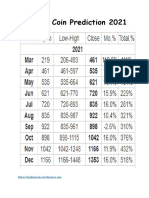
- Prediksi CryptocurrencyDocument4 pagesPrediksi CryptocurrencyM Fathur Arief KurniawanNo ratings yet
- Guidelines For The Management of Spontaneous Intracerebral HemorrhageDocument30 pagesGuidelines For The Management of Spontaneous Intracerebral HemorrhageM Fathur Arief KurniawanNo ratings yet
- Antioxidants & Redox SignalingDocument40 pagesAntioxidants & Redox SignalingM Fathur Arief KurniawanNo ratings yet
- The Effect of Physical Training Upon The Mechanical and Metabolic Performance of The Rat HeartDocument10 pagesThe Effect of Physical Training Upon The Mechanical and Metabolic Performance of The Rat HeartM Fathur Arief KurniawanNo ratings yet
- SC Heuer 1977Document31 pagesSC Heuer 1977M Fathur Arief KurniawanNo ratings yet
- SC Heuer 1977Document31 pagesSC Heuer 1977M Fathur Arief KurniawanNo ratings yet
- Reference AkuDocument5 pagesReference AkuArfiska Ridha Fausa 'ucha'No ratings yet
- Cadiac LDH SerumDocument6 pagesCadiac LDH SerumM Fathur Arief KurniawanNo ratings yet
- Chronobiology of Acid-Base Balance Under General A PDFDocument39 pagesChronobiology of Acid-Base Balance Under General A PDFM Fathur Arief KurniawanNo ratings yet
- The Lactate Aerobic MetabolismDocument9 pagesThe Lactate Aerobic MetabolismM Fathur Arief KurniawanNo ratings yet
- What Is Pseudomonas Aeruginosa?Document4 pagesWhat Is Pseudomonas Aeruginosa?M Fathur Arief KurniawanNo ratings yet
- Chronobiology of Acid-Base Balance Under General ADocument39 pagesChronobiology of Acid-Base Balance Under General AM Fathur Arief KurniawanNo ratings yet
- Asam Basa BahanDocument4 pagesAsam Basa BahanM Fathur Arief KurniawanNo ratings yet
- Nama Samaran KelompokDocument10 pagesNama Samaran KelompokM Fathur Arief KurniawanNo ratings yet
- Asam Basa BahanDocument39 pagesAsam Basa BahanM Fathur Arief KurniawanNo ratings yet
- Asam Basa BahanDocument7 pagesAsam Basa BahanM Fathur Arief KurniawanNo ratings yet
- Chronobiology of Acid-Base Balance Under General A PDFDocument39 pagesChronobiology of Acid-Base Balance Under General A PDFM Fathur Arief KurniawanNo ratings yet
- Acid Base Physiology Anesthesia PDFDocument9 pagesAcid Base Physiology Anesthesia PDFM Fathur Arief KurniawanNo ratings yet
- Acid Base Physiology Anesthesia PDFDocument9 pagesAcid Base Physiology Anesthesia PDFM Fathur Arief KurniawanNo ratings yet
- Asam Basa BahanDocument6 pagesAsam Basa BahanM Fathur Arief KurniawanNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaHassan MuhammadNo ratings yet
- A B P A: IntroductionsDocument10 pagesA B P A: IntroductionsM Fathur Arief KurniawanNo ratings yet
- Distúrbios Ácido Básicos Revisão NEJM 2014-1Document12 pagesDistúrbios Ácido Básicos Revisão NEJM 2014-1sabrinamgrNo ratings yet
- Epilepsy Knowledge SourcesDocument2 pagesEpilepsy Knowledge SourcesMahadian Ismail NasutionNo ratings yet
- Hypovolemic Shock in ChildrenDocument5 pagesHypovolemic Shock in ChildrenSussy ListiarsasihNo ratings yet
- Basic First Aid 2018Document36 pagesBasic First Aid 2018Mohamad AzharNo ratings yet
- Guía Manejo Del Shock 2023Document67 pagesGuía Manejo Del Shock 2023Alvaro ArriagadaNo ratings yet
- 11.initial Assesment & Stabilization of Poly Trauma PatientsDocument7 pages11.initial Assesment & Stabilization of Poly Trauma PatientsmyscribeNo ratings yet
- Prayer For Defense ThesisDocument8 pagesPrayer For Defense Thesismkdswzgig100% (2)
- Basic First Aid - FuturelearnDocument11 pagesBasic First Aid - FuturelearnSuhaib SghaireenNo ratings yet
- Fccs Course Administration: Licensed Activities PortalDocument8 pagesFccs Course Administration: Licensed Activities PortalRizki Baiti OktaviyaniNo ratings yet
- ShockDocument124 pagesShockRahman Mukti AjiNo ratings yet
- Cardio Intensive ReviewDocument40 pagesCardio Intensive ReviewAchilles YbarraNo ratings yet
- Cardiogenic ShockDocument9 pagesCardiogenic Shockrio kharismaNo ratings yet
- Anaphylactic ShockDocument14 pagesAnaphylactic ShockAuliya AndiNo ratings yet
- Postoperative Care: ACS/ASE Medical Student Core Curriculum Postoperative CareDocument26 pagesPostoperative Care: ACS/ASE Medical Student Core Curriculum Postoperative CareNataraj ThambiNo ratings yet
- Thesis On Biomedical Waste ManagementDocument8 pagesThesis On Biomedical Waste Managementtinawilliamsjackson100% (2)
- Pediatric Surgery Report 091118 FinalDocument33 pagesPediatric Surgery Report 091118 FinalYuanico LiraukaNo ratings yet
- Shock AssessmentDocument36 pagesShock AssessmentAlyssandra LucenoNo ratings yet
- Shock - Classification and Pathophysiological Principles of TherapeuticsDocument12 pagesShock - Classification and Pathophysiological Principles of TherapeuticsLuis ChancusigNo ratings yet
- DM General Surgery CurriculumDocument45 pagesDM General Surgery CurriculumGiovanni HenryNo ratings yet
- Noninvasive Hemodynamic Monitoring in The Intensive Care UnitDocument18 pagesNoninvasive Hemodynamic Monitoring in The Intensive Care UnitmegaNo ratings yet
- Thesis Topics For MD Respiratory MedicineDocument7 pagesThesis Topics For MD Respiratory Medicinelindseyriverakansascity100% (2)
- Nursing Care Paln of Mrs Richard (Clinical Scenario-3)Document20 pagesNursing Care Paln of Mrs Richard (Clinical Scenario-3)Axsa AlexNo ratings yet