You might also like
- Renal UltrasoundDocument179 pagesRenal UltrasoundJuhar AhamedNo ratings yet
- Animal Kingdom Mind MapDocument4 pagesAnimal Kingdom Mind MapVedanti Naik100% (1)
- Hypothyroid SymptomsDocument19 pagesHypothyroid Symptomsfatima110100% (2)
- TOPNOTCH Parasitology-Supertable-by-Yns-Pereyra-Cocoy-Calderon-Troy-Soberano-UPDATED-NOVEMBER-2017Document25 pagesTOPNOTCH Parasitology-Supertable-by-Yns-Pereyra-Cocoy-Calderon-Troy-Soberano-UPDATED-NOVEMBER-2017Waiwit KritayakiranaNo ratings yet
- TrematodesDocument9 pagesTrematodesLewis P. SanchezNo ratings yet
- Surpac Drill and Blast TutorialDocument69 pagesSurpac Drill and Blast Tutorialgunawan100% (4)
- How To Paidalajin For Common Symptoms-Final VersionDocument35 pagesHow To Paidalajin For Common Symptoms-Final VersionAndy100% (2)
- Liver Function TestsDocument16 pagesLiver Function TestsAnjali Devi100% (1)
- Physiological Differences Between Children and AdultsDocument17 pagesPhysiological Differences Between Children and AdultsAndrewBeck33% (3)
- Wound Management Guide DigitalDocument48 pagesWound Management Guide DigitalBrian NiuNo ratings yet
- AgniDocument12 pagesAgniAbhishek SharmaNo ratings yet
- DAX Cheat Sheet: Basic Aggregate and Math FunctionsDocument5 pagesDAX Cheat Sheet: Basic Aggregate and Math FunctionsIrvin SamaniegoNo ratings yet
- Introduction To Cestodes and Minor CestodesDocument8 pagesIntroduction To Cestodes and Minor CestodesJustin TayabanNo ratings yet
- Eiriu Eolas Quick GuideDocument7 pagesEiriu Eolas Quick GuidecpuxxxNo ratings yet
- Parasitology-Lec 5 TrematodesDocument5 pagesParasitology-Lec 5 Trematodesapi-3743217100% (2)
- 2 Parasitology Parasitic AmoebasDocument8 pages2 Parasitology Parasitic AmoebasknkjnNo ratings yet
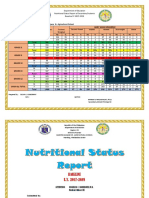
- Nutritional Status Report EndlineDocument3 pagesNutritional Status Report EndlineOliva Cabrales CabornayNo ratings yet
- Surpac DTM Surface TutorialDocument54 pagesSurpac DTM Surface TutorialLohendys Ramirz Kstilla88% (8)
- PROTOZOA (Sarcodina) : ProtozoologyDocument7 pagesPROTOZOA (Sarcodina) : ProtozoologyReyven Niña DyNo ratings yet
- Parasitology-Lec 7 Lung FlukesDocument5 pagesParasitology-Lec 7 Lung Flukesapi-3743217100% (1)
- Patellofemoral Pain SyndromeDocument21 pagesPatellofemoral Pain SyndromeAdvanced Physiotherapy100% (1)
- Medical Technology Assessment Program: Mycology Review NotesDocument6 pagesMedical Technology Assessment Program: Mycology Review NotesMoira Pauline LibroraniaNo ratings yet
- Parasitic Amoebas by Dr. C. J. Castro PDFDocument4 pagesParasitic Amoebas by Dr. C. J. Castro PDFMiguel CuevasNo ratings yet
- HParker (Reconciliation Principles For The Mining Industry) (2014) .PDF ShortcutDocument17 pagesHParker (Reconciliation Principles For The Mining Industry) (2014) .PDF ShortcutGerson Carhuapoma50% (2)
- Free Living AmoebaDocument5 pagesFree Living AmoebaEiveren Mae SutillezaNo ratings yet
- Trematodes: Intestinal SpeciesDocument7 pagesTrematodes: Intestinal SpeciesMica BernardoNo ratings yet
- Amoeba Part 2 NotesDocument8 pagesAmoeba Part 2 Notesjefftuazon01No ratings yet
- P. Falciparum P. Vivax P. Ovale P. MalariaeDocument3 pagesP. Falciparum P. Vivax P. Ovale P. MalariaeLembemNo ratings yet
- (PARA) 1.5 - Blood and Tissue FlagellatesDocument6 pages(PARA) 1.5 - Blood and Tissue FlagellatesGuia De GuzmanNo ratings yet
- Cns - Infections f2022 MeningoencephalitisDocument11 pagesCns - Infections f2022 MeningoencephalitisMadison MillwoodNo ratings yet
- Cestodes (Tapeworm) : Diphyllobotium Latum - 20 Yrs Life SpanDocument4 pagesCestodes (Tapeworm) : Diphyllobotium Latum - 20 Yrs Life SpanMicael Andrei MendozaNo ratings yet
- 1.3 Hemoflagellates and Ciliates (Limpin)Document4 pages1.3 Hemoflagellates and Ciliates (Limpin)arvinkennethdelacruzNo ratings yet
- Disease Causing OrganismsDocument4 pagesDisease Causing OrganismsANKITA GAYENNo ratings yet
- Trematodes: 2. MiracidiaDocument3 pagesTrematodes: 2. MiracidiaBikram ChohanNo ratings yet
- Enperiment For Spotting-3Document18 pagesEnperiment For Spotting-3Debayan Bhattacharyya class:- 11-ANo ratings yet
- Nematodes-Reviewer (Revised)Document4 pagesNematodes-Reviewer (Revised)Primo GeorgeNo ratings yet
- MBP Lab ReviewerDocument9 pagesMBP Lab ReviewerTrisha PaolaNo ratings yet
- Protista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Document6 pagesProtista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Primo GeorgeNo ratings yet
- Week 6 Blood and Tissue FlagellatesDocument7 pagesWeek 6 Blood and Tissue FlagellatesaemancarpioNo ratings yet
- Cnidaria SummaryDocument12 pagesCnidaria SummaryJose ArroyoNo ratings yet
- Parasites by Apple TanDocument16 pagesParasites by Apple TanOlivia LimNo ratings yet
- Amoeba: Ms. Helga SyDocument7 pagesAmoeba: Ms. Helga Syanti romantic txtNo ratings yet
- Parasites High YoieldDocument4 pagesParasites High Yoieldnreena aslamNo ratings yet
- 6.2 2021para ReviewlocalwactsDocument35 pages6.2 2021para ReviewlocalwactsHeyzel joy FabianNo ratings yet
- Trematodes LECDocument2 pagesTrematodes LECAki SuzumeNo ratings yet
- 1590 - Invented Primitive Microscope 1665 - 1665-1676 Cell Theory - Complete Cell TheoryDocument4 pages1590 - Invented Primitive Microscope 1665 - 1665-1676 Cell Theory - Complete Cell TheoryjaysparklesNo ratings yet
- Comparative Anatomy - Protochordates and The Origin of CraniatesDocument16 pagesComparative Anatomy - Protochordates and The Origin of CraniatesjeannegiananNo ratings yet
- Para - Amoeba TabulatedDocument1 pagePara - Amoeba TabulatedKaoriMarieSembranoNo ratings yet
- Protozoa: Free Living ParasitesDocument18 pagesProtozoa: Free Living Parasitesصفا رياض محمد /مسائيNo ratings yet
- Cestodes EditedDocument7 pagesCestodes EditedPrimo GeorgeNo ratings yet
- Pro Bef Ore Karyotic Nucleus: BloodDocument5 pagesPro Bef Ore Karyotic Nucleus: BloodDanielle Anne Zamora-Matillosa LambanNo ratings yet
- Amoeba paraDocument9 pagesAmoeba paraHANNA CASANDRA GARCIANo ratings yet
- Reviewer On EukaryotesDocument6 pagesReviewer On EukaryotesAlaica Joice B. JaboneteNo ratings yet
- Plus 2 PracticalDocument16 pagesPlus 2 Practicaljayantaroy783360No ratings yet
- OkieDocument3 pagesOkieFebeval CastilloNo ratings yet
- Chapter 6 IntegumentaryDocument3 pagesChapter 6 IntegumentaryLiane LomioNo ratings yet
- Phylum PlatyhelminthesDocument4 pagesPhylum PlatyhelminthesRenz GarciaNo ratings yet
- Week 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesDocument4 pagesWeek 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesHannah Beatrice Adame TamayoNo ratings yet
- Amoeba Notes 2015Document6 pagesAmoeba Notes 2015Ivy FlorentinoNo ratings yet
- Intro Medical Mycology Part 1Document1 pageIntro Medical Mycology Part 1pammcakeghzNo ratings yet
- Intestinal and Schistosoma FlukesDocument3 pagesIntestinal and Schistosoma FlukesKervy Jay AgraviadorNo ratings yet
- Parasitology Review On FlagellatesDocument2 pagesParasitology Review On FlagellatesKaoriMarieSembranoNo ratings yet
- ECHINOCOCCUSDocument5 pagesECHINOCOCCUSGhina RizwanNo ratings yet
- Bacteriology 1: - Non MotileDocument27 pagesBacteriology 1: - Non MotileYeshaa MiraniNo ratings yet
- Balantidum Coli: EBON, SISON - 2017Document5 pagesBalantidum Coli: EBON, SISON - 2017Abcd ReyesNo ratings yet
- Bot 3 2 Lec Exam Reviewer: I. Euglenophyta Chlorophyceae Ulvophyceae Charophyceae Iii. BryophytesDocument4 pagesBot 3 2 Lec Exam Reviewer: I. Euglenophyta Chlorophyceae Ulvophyceae Charophyceae Iii. BryophytesXearis SangalangNo ratings yet
- Trematode SDocument5 pagesTrematode SAUDREY VERONICA PEREZ100% (1)
- Parasitology - TrematodesDocument16 pagesParasitology - TrematodesMarlex SuanNo ratings yet
- Gurumantra of Zoology Final File)Document65 pagesGurumantra of Zoology Final File)Shivam GuptaNo ratings yet
- Biological: ClassificationDocument4 pagesBiological: ClassificationRiya BhardwajNo ratings yet
- Biodiversity Part 2/2Document25 pagesBiodiversity Part 2/2Kim Say Chun / Sc.KIMNo ratings yet
- Phasmids 4: Angiostrongylus CantonensisDocument5 pagesPhasmids 4: Angiostrongylus CantonensisJack Ortega PuruggananNo ratings yet
- Camp's Zoology by the Numbers: A comprehensive study guide in outline form for advanced biology courses, including AP, IB, DE, and college courses.From EverandCamp's Zoology by the Numbers: A comprehensive study guide in outline form for advanced biology courses, including AP, IB, DE, and college courses.No ratings yet
- 002 Power-BI-Masterclass-beginners-to-advanced-formulasDocument2 pages002 Power-BI-Masterclass-beginners-to-advanced-formulasIrvin SamaniegoNo ratings yet
- Geological Logging Look Up Tables: Gansu Longjin Mining Resources CompanyDocument4 pagesGeological Logging Look Up Tables: Gansu Longjin Mining Resources CompanyIrvin SamaniegoNo ratings yet
- Splitter DimensionDocument2 pagesSplitter DimensionIrvin SamaniegoNo ratings yet
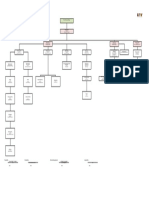
- Table of Organization 2020: Title: Department: Mine Department YearDocument1 pageTable of Organization 2020: Title: Department: Mine Department YearIrvin SamaniegoNo ratings yet
- Tbltrip Table DefinitionDocument7 pagesTbltrip Table DefinitionIrvin SamaniegoNo ratings yet
- EdT GCA Dossier PDFDocument1 pageEdT GCA Dossier PDFIrvin SamaniegoNo ratings yet
- MinerecDocument3 pagesMinerecIrvin SamaniegoNo ratings yet
- Database Exercise: Primary KEY Field Name Data TypeDocument3 pagesDatabase Exercise: Primary KEY Field Name Data TypeIrvin SamaniegoNo ratings yet
- SimonSezIT MovieRentalActorImportDocument1 pageSimonSezIT MovieRentalActorImportIrvin SamaniegoNo ratings yet
- SurpacDocument2 pagesSurpacIrvin SamaniegoNo ratings yet
- Dec2021 - Land Use MapDocument1 pageDec2021 - Land Use MapIrvin SamaniegoNo ratings yet
- Leapfrog Geo Release NotesDocument16 pagesLeapfrog Geo Release NotesrodrigoxtremNo ratings yet
- Disturbed Area Monitoring - 26dec21Document9 pagesDisturbed Area Monitoring - 26dec21Irvin SamaniegoNo ratings yet
- Ore Dilution Estimation Model in Tanzania Southern Highland Zone: A Case of New Luika Gold MineDocument6 pagesOre Dilution Estimation Model in Tanzania Southern Highland Zone: A Case of New Luika Gold MineIrvin SamaniegoNo ratings yet
- Covid-19 Test Result Summary: Sars-Cov-2 Viral Rna - Not DetectedDocument1 pageCovid-19 Test Result Summary: Sars-Cov-2 Viral Rna - Not DetectedIrvin SamaniegoNo ratings yet
- Q4 PaperDeni IJEEDocument8 pagesQ4 PaperDeni IJEEIrvin SamaniegoNo ratings yet
- Database Exercise: Primary KEY Field Name Data TypeDocument3 pagesDatabase Exercise: Primary KEY Field Name Data TypeIrvin SamaniegoNo ratings yet
- Mine Value Chain Reconciliation - Demonstrating VaDocument15 pagesMine Value Chain Reconciliation - Demonstrating VaIrvin SamaniegoNo ratings yet
- EdT GCA Dossier PDFDocument1 pageEdT GCA Dossier PDFIrvin SamaniegoNo ratings yet
- International Journal of Mining Science and TechnologyDocument6 pagesInternational Journal of Mining Science and TechnologyIrvin SamaniegoNo ratings yet
- LifeDocument4 pagesLifeIrvin SamaniegoNo ratings yet
- Tbltrip Table DefinitionDocument7 pagesTbltrip Table DefinitionIrvin SamaniegoNo ratings yet
- Esprit de Tour - Our Current Tours: Monday, May 30, 2016 Page 1 of 14Document14 pagesEsprit de Tour - Our Current Tours: Monday, May 30, 2016 Page 1 of 14Irvin SamaniegoNo ratings yet
- Esprit de Tour Trip ImportDocument2 pagesEsprit de Tour Trip ImportIrvin SamaniegoNo ratings yet
- Esprit de Tour Trip ImportDocument6 pagesEsprit de Tour Trip ImportIrvin SamaniegoNo ratings yet
- SimonSezIT NightMoviesMovieImportDocument1 pageSimonSezIT NightMoviesMovieImportIrvin SamaniegoNo ratings yet
- Slide Chronic Pain-Rudy Hidayat-Iai PDFDocument30 pagesSlide Chronic Pain-Rudy Hidayat-Iai PDFAsri ArrachmanNo ratings yet
- Notable Articles of 2023Document77 pagesNotable Articles of 2023Maria Angelica BocoliNo ratings yet
- Nutritional Content and Health Benefits of EggplantDocument6 pagesNutritional Content and Health Benefits of Eggplantdhanashri pawarNo ratings yet
- Personal Appearance and UniformDocument6 pagesPersonal Appearance and UniformmunyekiNo ratings yet
- Cheklist For Pre-Employment Medical Checkup For HeightDocument2 pagesCheklist For Pre-Employment Medical Checkup For HeightShad Siddiqui100% (1)
- The Effect of Age On Distribution and Symptomatology of Craniomandibular DysfunctionDocument5 pagesThe Effect of Age On Distribution and Symptomatology of Craniomandibular DysfunctionwalentinafroNo ratings yet
- IJPN 24 March With DOIDocument252 pagesIJPN 24 March With DOIShrutiMarwahNo ratings yet
- ExamDocument7 pagesExamAneesa AnserNo ratings yet
- Human Development and Human BehaviorDocument11 pagesHuman Development and Human BehaviormirtchNo ratings yet
- Bezold AbscessDocument2 pagesBezold AbscessSamuel anNo ratings yet
- Dermatitis Atopica Niños - Ingles PDFDocument10 pagesDermatitis Atopica Niños - Ingles PDFESTEPHANY PAMELA GAMBINI ACOSTANo ratings yet
- Is Agt The New Gene For Muscle Performance An Analysis of Agt Actn3 Ppara and Igf2 On Athletic Performance Muscle Size and Body Fa Z1yrDocument6 pagesIs Agt The New Gene For Muscle Performance An Analysis of Agt Actn3 Ppara and Igf2 On Athletic Performance Muscle Size and Body Fa Z1yrLeticia GasparNo ratings yet
- Test IntegumentaryDocument2 pagesTest IntegumentaryRoshann_Larano_48No ratings yet
- Covid Report: Mr. Rakesh SharmaDocument1 pageCovid Report: Mr. Rakesh Sharmavishal sharmaNo ratings yet
- Journal of The ACP in Womens HealthDocument108 pagesJournal of The ACP in Womens HealthRobert SandeepNo ratings yet
- HNR Paper 2Document10 pagesHNR Paper 2api-657392252No ratings yet
- ESC Guidelines On The Diagnosis and Treatment of Peripheral Artery DiseasesDocument56 pagesESC Guidelines On The Diagnosis and Treatment of Peripheral Artery DiseasesJuan José Ruiz CastilloNo ratings yet
- ALT (Alanine Aminotransferase) Test - Purpose, Procedure, and Results PDFDocument5 pagesALT (Alanine Aminotransferase) Test - Purpose, Procedure, and Results PDFMARIUS BACIUNo ratings yet
- CRIM ExemptingDocument88 pagesCRIM ExemptingKara LorejoNo ratings yet
- ProtozoaDocument132 pagesProtozoaAb AbNo ratings yet