You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- ACE - Personal Trainer University Curriculum - Lab Manual PDFDocument36 pagesACE - Personal Trainer University Curriculum - Lab Manual PDFdiego100% (2)
- FM 3-20.96Document204 pagesFM 3-20.96csantos1989100% (9)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Numerical Reasoning FormulasDocument7 pagesNumerical Reasoning FormulasRachid HC100% (1)
- Generational CursesDocument5 pagesGenerational Cursesfatima110No ratings yet
- The Nature of ResearchDocument14 pagesThe Nature of ResearchRonnel Aldin FernandoNo ratings yet
- LG DV450 DV452 Reproductor DVD Manual de Servicio PDFDocument73 pagesLG DV450 DV452 Reproductor DVD Manual de Servicio PDFalberto castañoNo ratings yet
- Rogers, Lisa - Movie Review (EPortfolio)Document14 pagesRogers, Lisa - Movie Review (EPortfolio)Lisa RogersNo ratings yet
- S3651323 - A3 - Governance Research EssayDocument7 pagesS3651323 - A3 - Governance Research EssayTai LuongNo ratings yet
- Western Story MagazineDocument2 pagesWestern Story MagazineFelipe NicastroNo ratings yet
- Nacsport Scout Plus Manual enDocument131 pagesNacsport Scout Plus Manual enKoall Tchang LindienNo ratings yet
- Imsart-SA-33 Walkthrought Metal Detector by ZAMTAS - 2Document4 pagesImsart-SA-33 Walkthrought Metal Detector by ZAMTAS - 2anasNo ratings yet
- Natural OrderDocument5 pagesNatural OrderMicah Santon100% (1)
- Export Meaning, Significance and Methods in IndiaDocument9 pagesExport Meaning, Significance and Methods in IndiaPayal AroraNo ratings yet
- Unit 2 Lesson 2 Honors ApplyDocument3 pagesUnit 2 Lesson 2 Honors ApplyJohn SynchrosNo ratings yet
- Art and MusicDocument92 pagesArt and MusicKiên KiênNo ratings yet
- Maths Apptitude QUES ANSDocument382 pagesMaths Apptitude QUES ANSd_narnoliaNo ratings yet
- Project Assignment DAMDocument2 pagesProject Assignment DAMPrimax DiagnosticsNo ratings yet
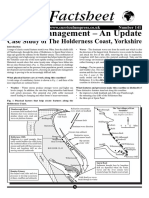
- Coastal Managemtn Holderness 2Document5 pagesCoastal Managemtn Holderness 2Grand OverallNo ratings yet
- Project Report ON Advance Atm Security SystemDocument7 pagesProject Report ON Advance Atm Security SystemAnil BatraNo ratings yet
- Test Bank For Macroeconomics 8e by Andrew B Abel 0133407926Document3 pagesTest Bank For Macroeconomics 8e by Andrew B Abel 0133407926Marvin Patterson100% (37)
- Tn-Fee Structure 2022 - 28.05.2022Document1 pageTn-Fee Structure 2022 - 28.05.2022MSPET TrustNo ratings yet
- SugarDocument4 pagesSugarabiramanNo ratings yet
- Indoor Unit/Outdoor Unit: Split Type Air ConditionerDocument23 pagesIndoor Unit/Outdoor Unit: Split Type Air ConditionerMuhamad PriyatnaNo ratings yet
- McWilliams Center For Counseling, Inc. Community Support Office - 438Document2 pagesMcWilliams Center For Counseling, Inc. Community Support Office - 438James BennettNo ratings yet
- Coastal Nursing Tourism To Improve Tourist Safety in Tourist AttractionDocument10 pagesCoastal Nursing Tourism To Improve Tourist Safety in Tourist AttractionihwanNo ratings yet
- GenBio AnswersDocument8 pagesGenBio AnswersRiza CatubigNo ratings yet
- Debre Birhan University C0Llege of Business & EconomicsDocument20 pagesDebre Birhan University C0Llege of Business & Economicsይንገስ ጎጃም አድማስ100% (1)
- Reflection On Written AssignmentDocument3 pagesReflection On Written Assignmentapi-302720012No ratings yet
- Lecture 9 (Dirk Mohr, ETH, Rate-Dependent Plasticity and Fracture) PDFDocument52 pagesLecture 9 (Dirk Mohr, ETH, Rate-Dependent Plasticity and Fracture) PDFชัยรัตน์ ตันตืไพบูลย์วุฒิNo ratings yet
- 2017 - YEAR5 - BI - Paper1 - 1st PRODocument13 pages2017 - YEAR5 - BI - Paper1 - 1st PRORani ArumugamNo ratings yet