You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PDF DocumentDocument10 pagesPDF DocumentNIKHIL DASARINo ratings yet
- Trainer Activity: All Adrift!Document6 pagesTrainer Activity: All Adrift!DollyNo ratings yet
- Ho'oponopono ! - The Power of ForgivenessDocument6 pagesHo'oponopono ! - The Power of ForgivenessParainNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- m5 Mage The AscensionDocument20 pagesm5 Mage The AscensionQuentin Agnes0% (1)
- Odontogenic InfectionsDocument27 pagesOdontogenic InfectionsEmad Hussien Haj-Abdulla100% (2)
- Anesthesia For Paediatric DentistryDocument18 pagesAnesthesia For Paediatric DentistryErfiadi Nur FahmiNo ratings yet
- DNA Discoveries Reveal Human DNA as a Biological InternetDocument7 pagesDNA Discoveries Reveal Human DNA as a Biological InternetUmbrielNo ratings yet
- WellBeing I193 2021Document164 pagesWellBeing I193 2021lan tranNo ratings yet
- Lesson Plan For Demonstration (COT) : School Grade Level Teacher Learning Area Teaching Dates and Time QuarterDocument6 pagesLesson Plan For Demonstration (COT) : School Grade Level Teacher Learning Area Teaching Dates and Time Quartermaritel dawaNo ratings yet
- EBM On Harm - Dentistry 2010Document16 pagesEBM On Harm - Dentistry 2010Erfiadi Nur FahmiNo ratings yet
- ABC of Oral Health Dental EmergenciesDocument5 pagesABC of Oral Health Dental EmergenciesErfiadi Nur FahmiNo ratings yet
- Bru X Is M Consensus 2018Document9 pagesBru X Is M Consensus 2018Erfiadi Nur FahmiNo ratings yet
- Journal of Oral and Maxillofacial Surgery Volume Issue 2017 (Doi 10.1016/j.joms.2017.04.045) Best, Adrian D. de Silva, R.K. Thomson, W.M. Tong, Darryl C. - The Efficacy of Codeine When Added To PDFDocument24 pagesJournal of Oral and Maxillofacial Surgery Volume Issue 2017 (Doi 10.1016/j.joms.2017.04.045) Best, Adrian D. de Silva, R.K. Thomson, W.M. Tong, Darryl C. - The Efficacy of Codeine When Added To PDFErfiadi Nur FahmiNo ratings yet
- ElevatorDocument2 pagesElevatorErfiadi Nur FahmiNo ratings yet
- Hubungan Pola Asuh Orang Tua Dengan Status Kebersihan Gigi Dan Mulut Siswa Tuna Netra Kelas V Dan VI SDLB A YPAB Surabaya Isnanto Dwi Rahayu Poltekkes SurabayaDocument8 pagesHubungan Pola Asuh Orang Tua Dengan Status Kebersihan Gigi Dan Mulut Siswa Tuna Netra Kelas V Dan VI SDLB A YPAB Surabaya Isnanto Dwi Rahayu Poltekkes SurabayaErfiadi Nur FahmiNo ratings yet
- PEP 604 Research Methods GuideDocument13 pagesPEP 604 Research Methods Guidea1savedNo ratings yet
- 152 1394 2 PB PDFDocument2 pages152 1394 2 PB PDFErfiadi Nur FahmiNo ratings yet
- Pregnancy Oral HealthcareDocument2 pagesPregnancy Oral HealthcareErfiadi Nur FahmiNo ratings yet
- Odontogenicinfection 130303003840 Phpapp02Document141 pagesOdontogenicinfection 130303003840 Phpapp02Erfiadi Nur FahmiNo ratings yet
- Pregnancy Oral HealthcareDocument2 pagesPregnancy Oral HealthcareErfiadi Nur FahmiNo ratings yet
- Heart Diseases Dental TreatmentDocument2 pagesHeart Diseases Dental TreatmentErfiadi Nur FahmiNo ratings yet
- Use of Passive VoiceDocument13 pagesUse of Passive VoiceLuciana DicieroNo ratings yet
- Resume-Mariam Abdul AzizDocument2 pagesResume-Mariam Abdul Azizmaryam cookNo ratings yet
- Vessel and Conveyors - VPDDocument4 pagesVessel and Conveyors - VPDAntonio Mizraim Magallon SantanaNo ratings yet
- Review of Dr. Mark Cheng's "Prehab-Rehab 101" SeriesDocument6 pagesReview of Dr. Mark Cheng's "Prehab-Rehab 101" SeriesWilliam TortorielloNo ratings yet
- Flygt 4660 EnglishDocument2 pagesFlygt 4660 EnglishVictor Manuel Lachira YarlequeNo ratings yet
- National Capital Region Schools Division Office Novaliches High School MAPEH Department Definitive Budget of Work for Blended Learning Modality Quarter 1 Grade 10Document9 pagesNational Capital Region Schools Division Office Novaliches High School MAPEH Department Definitive Budget of Work for Blended Learning Modality Quarter 1 Grade 10Ma. Cristina Angenel RamosNo ratings yet
- Medical Services Recruitment Board (MRB)Document20 pagesMedical Services Recruitment Board (MRB)durai PandiNo ratings yet
- PreceptronDocument17 pagesPreceptroneng_kmmNo ratings yet
- ST Patrick Lodge 199 BibleDocument5 pagesST Patrick Lodge 199 Bibletofique_fatehiNo ratings yet
- ENGLISH CONTENT UNIT 4 2022 5tos.Document9 pagesENGLISH CONTENT UNIT 4 2022 5tos.Dylan QuiñónezNo ratings yet
- Siwarex Cs-En v12Document15 pagesSiwarex Cs-En v12Diego CanoNo ratings yet
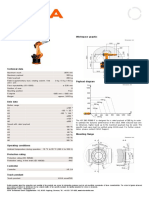
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet
- Enquiries: 1. Enquiry From A Retailer To A Foreign ManufacturerDocument7 pagesEnquiries: 1. Enquiry From A Retailer To A Foreign ManufacturerNhi Hoàng Lê NguyễnNo ratings yet
- Seagate WD Hard Drive Price List From Billion HoDocument4 pagesSeagate WD Hard Drive Price List From Billion HoALi RAzaNo ratings yet
- WRBS Quarter 1 Modules WEEK-1-8Document32 pagesWRBS Quarter 1 Modules WEEK-1-8Sir Kindred VillaruzNo ratings yet
- Journal of Materials Processing Technology: Jun Cao, Michael A. Gharghouri, Philip NashDocument11 pagesJournal of Materials Processing Technology: Jun Cao, Michael A. Gharghouri, Philip NashJesus Ismael Jimenez GarciaNo ratings yet
- DOE V Rhodes College Ammended Motion For TRODocument19 pagesDOE V Rhodes College Ammended Motion For TROSouwesterdocs100% (1)
- Flared Separable FittingDocument9 pagesFlared Separable FittingbenNo ratings yet
- Vergara, Valerie G. Drug Study (Ma'Am Dean)Document3 pagesVergara, Valerie G. Drug Study (Ma'Am Dean)Valerie VergaraNo ratings yet
- Intersecting Lines Intersecting Lines Parallel Lines Same LineDocument7 pagesIntersecting Lines Intersecting Lines Parallel Lines Same Lineapi-438357152No ratings yet
- A Review Paper On Rice Quality Analysis Using Image Processing TechniqueDocument5 pagesA Review Paper On Rice Quality Analysis Using Image Processing TechniqueIJRASETPublicationsNo ratings yet
- Rabbani Env 3Document298 pagesRabbani Env 3Arnob SarkerNo ratings yet