You might also like
- Post BSC I YearDocument3 pagesPost BSC I Yearkuruvagadda sagarNo ratings yet
- Annual Report - Year 2018-2019Document24 pagesAnnual Report - Year 2018-2019baby100% (1)
- Mharashtra Nursing Council Inspection FormatDocument15 pagesMharashtra Nursing Council Inspection FormatRavindra Puranik Msc Nursing100% (2)
- M.SC 2nd Year Obg Clinical Rotation PlanDocument1 pageM.SC 2nd Year Obg Clinical Rotation PlanSanthu Su67% (3)
- Ambaji School of Nursing Ganeshpura DIST - MEHSANA (382705) : Cumulative RecordDocument6 pagesAmbaji School of Nursing Ganeshpura DIST - MEHSANA (382705) : Cumulative RecordNeha Pandey Sharma100% (1)
- Evaluation Criteria MSC NursingDocument15 pagesEvaluation Criteria MSC NursingAnish VeettiyankalNo ratings yet
- Midwifery Lab Equipment & ArticlesDocument3 pagesMidwifery Lab Equipment & Articlesravi002480% (10)
- Resume for Selma Alvan ZacchaeusDocument6 pagesResume for Selma Alvan ZacchaeusSri HariNo ratings yet
- Lab Articles As Per IncDocument29 pagesLab Articles As Per IncMukesh Kashyap100% (2)
- Pediatric Nursing Lab ArticlesDocument6 pagesPediatric Nursing Lab ArticlesPrincipal Principal100% (1)
- Cumulative Record of General Nursing and MidwiferyDocument4 pagesCumulative Record of General Nursing and MidwiferyVinod Kumaar58% (12)
- Child Health Nursing (Pediatric) LabDocument1 pageChild Health Nursing (Pediatric) LabChakrapani Chaturvedi50% (2)
- Inspection ProformaDocument21 pagesInspection ProformaArunachala VijayNo ratings yet
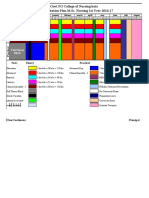
- New Clinical Rotation Balaji 2016 2017Document22 pagesNew Clinical Rotation Balaji 2016 2017rama joy100% (1)
- ROTATION PLAN M.Sc. 1sr YRDocument1 pageROTATION PLAN M.Sc. 1sr YRRuchika KaushalNo ratings yet
- OBG Lab InstrumentsDocument6 pagesOBG Lab InstrumentsChellapandyaNo ratings yet
- Clinical Rotation Plan BSC 1ST YearDocument4 pagesClinical Rotation Plan BSC 1ST YearMeenakshi Antil0% (1)
- Visit ReportDocument14 pagesVisit Reportjoeti100% (2)
- A Descriptive Study To Assess The Knowledge and Practice Regarding Adverse Effects of Excessive Use of Mobile Phones Among Nursing Students of Selected Nursing College of BagalkotDocument8 pagesA Descriptive Study To Assess The Knowledge and Practice Regarding Adverse Effects of Excessive Use of Mobile Phones Among Nursing Students of Selected Nursing College of BagalkotAnonymous izrFWiQNo ratings yet
- Cumulative-record-For BSC Nursing IstDocument11 pagesCumulative-record-For BSC Nursing IstJUHI PRAKASH100% (1)
- 4 TH Management SyllabusDocument37 pages4 TH Management SyllabusDIANANo ratings yet
- CHC VisitDocument48 pagesCHC VisitRamyasree BadeNo ratings yet
- Patna ANM Training School Master Rotation PlanDocument6 pagesPatna ANM Training School Master Rotation PlanBijayalaxmi SinghNo ratings yet
- B.SC Nursing 2018 Question Papers First Year English FR 2Document2 pagesB.SC Nursing 2018 Question Papers First Year English FR 2Himanshu0% (1)
- Annotated Bibliography of Nursing Education:: 1. Elakkuvana Bhaskara Raj and Nima Bhaskar (2015), "A Textbook ofDocument4 pagesAnnotated Bibliography of Nursing Education:: 1. Elakkuvana Bhaskara Raj and Nima Bhaskar (2015), "A Textbook ofKaku Manisha100% (1)
- 10.master Rotation Plan M. Sc. Nursing 1st YearDocument4 pages10.master Rotation Plan M. Sc. Nursing 1st YearNaresh JeengarNo ratings yet
- Nursing Lab Articles & Advance Skill Labs For GNM As Per Inc - DSDDocument5 pagesNursing Lab Articles & Advance Skill Labs For GNM As Per Inc - DSDRahul Kashyap100% (1)
- Critical Evaluation GNMDocument7 pagesCritical Evaluation GNMManisha Samson100% (2)
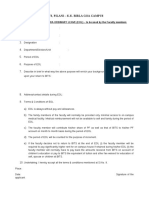
- Nursing Foundation Written Assignment Evaluation FormatDocument2 pagesNursing Foundation Written Assignment Evaluation Formatsubi50% (2)
- MSc. Nursing Log BookDocument42 pagesMSc. Nursing Log Booksumanjali Joshua100% (1)
- OBG Nursing Lab Equipment & Skills TrainingDocument2 pagesOBG Nursing Lab Equipment & Skills TrainingChakrapani Chaturvedi0% (1)
- Intranatal Assessment FormatDocument10 pagesIntranatal Assessment FormatAnnapurna Dangeti100% (1)
- Master Rotation Plan-3Rd Year Basic-Bsc Nursing: Indira Gandhi College of NursingDocument5 pagesMaster Rotation Plan-3Rd Year Basic-Bsc Nursing: Indira Gandhi College of Nursingkuruvagadda sagarNo ratings yet
- Nursing Lab Articles As Per Indian Nursing CouncilDocument40 pagesNursing Lab Articles As Per Indian Nursing CouncilRahul Kashyap100% (1)
- Revised Proforma Guidelines Internal Assessment II PBBSC 011007Document58 pagesRevised Proforma Guidelines Internal Assessment II PBBSC 011007mljg30100% (2)
- Cumulative Report For GNMDocument7 pagesCumulative Report For GNMPatel Amee100% (4)
- Clinical Rotation Basic B.sc.Document7 pagesClinical Rotation Basic B.sc.bijoNo ratings yet
- Master Rotation Plan For GNMDocument2 pagesMaster Rotation Plan For GNMkuruvagadda sagar100% (2)
- College Nursing Tips Master Rotation PlanDocument4 pagesCollege Nursing Tips Master Rotation PlanBisakha DeyNo ratings yet
- Rotation Plan GNM 2ND YearDocument10 pagesRotation Plan GNM 2ND Yearamritanshu chanchalNo ratings yet
- Clinical Rotation Plan BSCDocument10 pagesClinical Rotation Plan BSCBabita DhruwNo ratings yet
- Clinical rotation plan for MSc Nursing studentsDocument2 pagesClinical rotation plan for MSc Nursing studentsPriyaNo ratings yet
- Clinical Evaluation Format and HEALTH TALK BSC JIMSHDocument3 pagesClinical Evaluation Format and HEALTH TALK BSC JIMSHKiran Mini RaviNo ratings yet
- History Collection and Physical Examination Kardex Nurses NotesDocument41 pagesHistory Collection and Physical Examination Kardex Nurses Notessubi86% (7)
- Community health nursing lab inventory checklistDocument2 pagesCommunity health nursing lab inventory checklistshalini7575% (4)
- Principles of Nursing EducationDocument15 pagesPrinciples of Nursing Educationsrinivasana100% (2)
- Educational Institution PoliciesDocument4 pagesEducational Institution PoliciesDeepak patel50% (2)
- Synopsis PresentationDocument24 pagesSynopsis PresentationAnkita Sarma86% (7)
- A Study To Assess The Effectiveness of Hot and Cold Application On Arthritic Pain and Mobility Status Among Clients With Osteoarthritis in Selected Hospitals at Kolar District.Document31 pagesA Study To Assess The Effectiveness of Hot and Cold Application On Arthritic Pain and Mobility Status Among Clients With Osteoarthritis in Selected Hospitals at Kolar District.Lambert Winston67% (6)
- Nursing Rotation Plan by Month, Week and BlockDocument2 pagesNursing Rotation Plan by Month, Week and BlockpriyankaNo ratings yet
- B. SC Nursing Syllabus INC PDFDocument183 pagesB. SC Nursing Syllabus INC PDFSathya Palanisamy75% (28)
- Final Problem Statement EctDocument2 pagesFinal Problem Statement EctRahul DamorNo ratings yet
- Master Rotation Plan For Anm EditDocument9 pagesMaster Rotation Plan For Anm EditAnil Kumar100% (5)
- Netaji Subhash College of Nursing, Palampur: MASTER ROTATION PLAN 2022-2023 (B.SC Nursing 3rd Semester)Document2 pagesNetaji Subhash College of Nursing, Palampur: MASTER ROTATION PLAN 2022-2023 (B.SC Nursing 3rd Semester)Priya100% (5)
- Master Rotation Plan of Anm 2ND YearDocument9 pagesMaster Rotation Plan of Anm 2ND Yearkuruvagadda sagar50% (2)
- Advance Skill Lab AS PER INDIAN NURSING COUNCILDocument10 pagesAdvance Skill Lab AS PER INDIAN NURSING COUNCILRahul Kashyap73% (11)
- Unit Plan Obg Sem 6 Unit IVDocument6 pagesUnit Plan Obg Sem 6 Unit IVDelphy VargheseNo ratings yet
- MbbsDocument287 pagesMbbsBHANUNo ratings yet
- PCI Pilot CEP Program for Pharmacy TeachersDocument4 pagesPCI Pilot CEP Program for Pharmacy Teachers16_dev5038No ratings yet
- Campus Eol FormDocument3 pagesCampus Eol FormdeepakpnNo ratings yet
- Prevent Workplace Violence: Strategies to Reduce RisksDocument4 pagesPrevent Workplace Violence: Strategies to Reduce RisksedrinsneNo ratings yet
- Lesson Plan in Water A.N.M 1ST Year (Environmaental SanitationDocument9 pagesLesson Plan in Water A.N.M 1ST Year (Environmaental Sanitationedrinsne100% (2)
- UNIT PLAN Clinical Sp. IIDocument5 pagesUNIT PLAN Clinical Sp. IIedrinsneNo ratings yet
- Fire Safety Procedures in HospitalsDocument10 pagesFire Safety Procedures in Hospitalsedrinsne100% (1)
- Anm SyllabusDocument83 pagesAnm SyllabusPashobikNo ratings yet
- Nursing College Orientation InvitationDocument1 pageNursing College Orientation InvitationedrinsneNo ratings yet
- Digestive System Lesson Plan StomachDocument14 pagesDigestive System Lesson Plan StomachedrinsneNo ratings yet
- Unit 11 Computers in Health CareDocument22 pagesUnit 11 Computers in Health CareedrinsneNo ratings yet
- Child Health NSG Important QuestionsDocument10 pagesChild Health NSG Important Questionsedrinsne100% (2)
- Cold ChainDocument18 pagesCold ChainedrinsneNo ratings yet
- Adolescent AssessmentDocument4 pagesAdolescent AssessmentedrinsneNo ratings yet
- Know How To Help A Choking Victim: MembersDocument1 pageKnow How To Help A Choking Victim: MembersedrinsneNo ratings yet
- General Duty AssistantDocument1 pageGeneral Duty AssistantedrinsneNo ratings yet
- Pediatric Nursing Clinical Objectives.Document2 pagesPediatric Nursing Clinical Objectives.edrinsne100% (4)
- Assessment ToddlerDocument5 pagesAssessment ToddleredrinsneNo ratings yet
- Finding Related To Association of Knowledge Scores Regarding First Aid Care With Socio-Demographic Variables of 11 Students Table - 12Document2 pagesFinding Related To Association of Knowledge Scores Regarding First Aid Care With Socio-Demographic Variables of 11 Students Table - 12edrinsneNo ratings yet
- DDHDocument30 pagesDDHedrinsneNo ratings yet
- Anorectal MalformationsDocument52 pagesAnorectal MalformationsedrinsneNo ratings yet
- Allergy Skin TestDocument14 pagesAllergy Skin Testedrinsne100% (1)
- Anorectal MalformationsDocument52 pagesAnorectal MalformationsedrinsneNo ratings yet
- Adolescent AssessmentDocument4 pagesAdolescent AssessmentedrinsneNo ratings yet
- Resaerch StatisticDocument1 pageResaerch StatisticedrinsneNo ratings yet
- Neuro Exam PDFDocument23 pagesNeuro Exam PDFedrinsneNo ratings yet
- Pedia LabDocument3 pagesPedia LabedrinsneNo ratings yet
- Case StudyDocument1 pageCase StudyedrinsneNo ratings yet
- Likert Scale KMCDocument1 pageLikert Scale KMCedrinsneNo ratings yet
- Allergy Skin TestDocument14 pagesAllergy Skin Testedrinsne100% (1)
- GNM InternDocument11 pagesGNM InternedrinsneNo ratings yet
- Adult vs Child: Key DifferencesDocument37 pagesAdult vs Child: Key Differencesedrinsne100% (2)
- Tab E (Religious Support) To Appendix 2 (Personnel Services Support)Document3 pagesTab E (Religious Support) To Appendix 2 (Personnel Services Support)Stephen SmithNo ratings yet
- Word Perioperative NursingDocument19 pagesWord Perioperative NursingGerald Resubal Oriña100% (1)
- Palliative Care-A Concept AnalysisDocument26 pagesPalliative Care-A Concept Analysiskdavis618100% (3)
- Accenture - Artificial Intelligence - Healthcare's New Nervous SystemDocument8 pagesAccenture - Artificial Intelligence - Healthcare's New Nervous SystemRobert KoverNo ratings yet
- Study On Usage of Self - Medication in MBBS Students in A Teaching HospitalDocument8 pagesStudy On Usage of Self - Medication in MBBS Students in A Teaching HospitalInternational Organization of Scientific Research (IOSR)No ratings yet
- Kendra's Law - New York's Assisted Outpatient Treatment StatuteDocument23 pagesKendra's Law - New York's Assisted Outpatient Treatment StatuteAlexander J. NicasNo ratings yet
- Paulding County Progress May 29, 2013Document16 pagesPaulding County Progress May 29, 2013PauldingProgressNo ratings yet
- BUPA Intl Claim Form PDFDocument4 pagesBUPA Intl Claim Form PDFisabellashNo ratings yet
- CPCDocument32 pagesCPCBaihaqi ReadsNo ratings yet
- Principles of Cancer RehabDocument15 pagesPrinciples of Cancer RehabnoonoonsNo ratings yet
- Bhubaneswar development authority regulationsDocument154 pagesBhubaneswar development authority regulationsVinson IndiaNo ratings yet
- (P) Both Bone Forearm Fracture ORIFDocument3 pages(P) Both Bone Forearm Fracture ORIFkrissh20No ratings yet
- Safe Administrations of Medications (Draft Chapter)Document74 pagesSafe Administrations of Medications (Draft Chapter)Caleb FellowesNo ratings yet
- Lily Grebe Resume 10Document3 pagesLily Grebe Resume 10api-482765948No ratings yet
- Employee Handbook RevisionsDocument82 pagesEmployee Handbook RevisionsRosfaizal Mohamad Zain100% (7)
- 11 Infection Prevention and ControlDocument24 pages11 Infection Prevention and ControlKristian Dave DivaNo ratings yet
- We Care Brochurev3Document14 pagesWe Care Brochurev3Anais IoNo ratings yet
- Act 586 Private Healthcare Facilities and Services Act 1998 PDFDocument84 pagesAct 586 Private Healthcare Facilities and Services Act 1998 PDFAdam Haida & Co100% (1)
- Teu ApalDocument1,219 pagesTeu ApalDanz Adi NNo ratings yet
- Od3 rt01Document4 pagesOd3 rt01Abby GonzalezNo ratings yet
- Knowledge of and Compliance With Standard Precautions Among Nursing StudentsDocument14 pagesKnowledge of and Compliance With Standard Precautions Among Nursing StudentsLeodoro LabragueNo ratings yet
- Drama Script: The GiftDocument9 pagesDrama Script: The GiftHafiz Hanif50% (2)
- Learning Objectives:: Case 6. Epidemic AsthmaDocument13 pagesLearning Objectives:: Case 6. Epidemic AsthmaGaluh Ajeng PangestikaNo ratings yet
- Pediatric Nurse Students' AttitudesDocument8 pagesPediatric Nurse Students' AttitudesBeatrizNo ratings yet
- The Science of Vampires, Zombies, Werewolves, and Other MonstersDocument17 pagesThe Science of Vampires, Zombies, Werewolves, and Other MonstersSimon and Schuster0% (8)
- Grad Day Speech Celebrating Medical School JourneyDocument3 pagesGrad Day Speech Celebrating Medical School JourneyLee Tjen JhungNo ratings yet
- Lobchuk 2020Document44 pagesLobchuk 2020Sigit Nian PrasetyoNo ratings yet
- Informed Consent: DR Sontang Simamora MmededDocument15 pagesInformed Consent: DR Sontang Simamora MmededIcan DoitNo ratings yet
- Modal May Must MightDocument2 pagesModal May Must MightTaniusha Cebotari100% (2)