You might also like
- Central Nervous System MetastasesFrom EverandCentral Nervous System MetastasesManmeet AhluwaliaNo ratings yet
- Jurnal KedokteranDocument9 pagesJurnal KedokteranannisanoviaNo ratings yet
- Adults Brain Tumor in Cipto Mangunkusumo General Hospital A Descriptive EpidemiologyDocument5 pagesAdults Brain Tumor in Cipto Mangunkusumo General Hospital A Descriptive EpidemiologyHarun NANo ratings yet
- 1.masas en CuelloDocument3 pages1.masas en CuelloIsaac TellezNo ratings yet
- Cpho023 01 03Document11 pagesCpho023 01 03Kyung-Nam KohNo ratings yet
- Natural course of low risk neuroblastoma in Thai childrenDocument5 pagesNatural course of low risk neuroblastoma in Thai childrenvalentina rojasNo ratings yet
- Intra-Ventricular Tumors and Their Expression With Immunohistochemistry (IHC) Markers - Original ArticleDocument9 pagesIntra-Ventricular Tumors and Their Expression With Immunohistochemistry (IHC) Markers - Original ArticleVenansius Ratno KurniawanNo ratings yet
- Epidemiological Patterns of Paediatric Brain Tumors in CoimbatoreDocument6 pagesEpidemiological Patterns of Paediatric Brain Tumors in CoimbatoreIJAR JOURNALNo ratings yet
- Prostate Cancer Brain Metastases: A Single-Institution ExperienceDocument5 pagesProstate Cancer Brain Metastases: A Single-Institution ExperienceGabriel ŞarguNo ratings yet
- Triple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesDocument10 pagesTriple Negative Breast Cancer, Experience of Military Hospital Rabat: About 52 CasesIJAR JOURNALNo ratings yet
- Granulosa Tumors: About 10 CasesDocument7 pagesGranulosa Tumors: About 10 CasesIJAR JOURNALNo ratings yet
- Perilongo 1997Document7 pagesPerilongo 1997Gustav RSRNo ratings yet
- 6279 17690 1 SMDocument14 pages6279 17690 1 SMvistaNo ratings yet
- Mri Evaluation of Medulloblastoma With Histopahtological CorrelationDocument5 pagesMri Evaluation of Medulloblastoma With Histopahtological CorrelationVidinikusumaNo ratings yet
- HN 04-2011 Sublingual Gland Tumors PDFDocument6 pagesHN 04-2011 Sublingual Gland Tumors PDFHafiz FatmarNo ratings yet
- 21 Srilakshmi Et AlDocument5 pages21 Srilakshmi Et AleditorijmrhsNo ratings yet
- Ependymoma: Evaluation and Management UpdatesDocument9 pagesEpendymoma: Evaluation and Management UpdatesIsaac Bacasehua InzunzaNo ratings yet
- Tumores Malignos de Anexos CutáneosDocument7 pagesTumores Malignos de Anexos CutáneostisadermaNo ratings yet
- Primary Tracheal Tumors: Review of 37 CasesDocument4 pagesPrimary Tracheal Tumors: Review of 37 CasesGordana PuzovicNo ratings yet
- Ijss Jan Oa08Document7 pagesIjss Jan Oa08IvanDwiKurniawanNo ratings yet
- 3454-Article Text-11501-1-10-20200318Document4 pages3454-Article Text-11501-1-10-20200318NuruljannahNo ratings yet
- Original ArticleDocument7 pagesOriginal ArticleDain 2IronfootNo ratings yet
- Metastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyDocument7 pagesMetastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyJafet Gonzalez EstradaNo ratings yet
- Ijss Nov Oa28Document5 pagesIjss Nov Oa28Irsanti sasmitaNo ratings yet
- Materials and MethodsDocument2 pagesMaterials and MethodsRedigo RahmadhaniNo ratings yet
- Shifts in The Proportion of Colorectal CancerDocument8 pagesShifts in The Proportion of Colorectal CancerprimaNo ratings yet
- MicroRNA-based Risk Scoring System To Identify EarDocument14 pagesMicroRNA-based Risk Scoring System To Identify EarDavidNo ratings yet
- A Study of Histopathological Spectrum of Breast Lesions in A Tertiary Care Hospital PDFDocument5 pagesA Study of Histopathological Spectrum of Breast Lesions in A Tertiary Care Hospital PDFravimalagundlaNo ratings yet
- As Trocito MaDocument10 pagesAs Trocito Majeimy_carolina4163No ratings yet
- Pmid DreamDocument12 pagesPmid DreamwurtziteblendeNo ratings yet
- Medi 96 E6799Document8 pagesMedi 96 E6799Utami DewiNo ratings yet
- Maris 2007Document15 pagesMaris 2007asialoren74No ratings yet
- Brainstem Gliomas in Adults: Prognostic Factors and ClassificationDocument12 pagesBrainstem Gliomas in Adults: Prognostic Factors and ClassificationIsabel PereiraNo ratings yet
- Albayrak 2016Document7 pagesAlbayrak 2016DavorIvanićNo ratings yet
- Meningiomas A Clinicopathological Study PDFDocument5 pagesMeningiomas A Clinicopathological Study PDFIcha IchaNo ratings yet
- CONTRIBUTION OF COMPUTED TOMOGRAPHY IN THE ASSESSMENT OF THE EXTENT OF BLADDER CANCER AT THE MOTHER-CHILD UNIVERSITY HOSPITAL CENTER LE LUXEMBOURGDocument14 pagesCONTRIBUTION OF COMPUTED TOMOGRAPHY IN THE ASSESSMENT OF THE EXTENT OF BLADDER CANCER AT THE MOTHER-CHILD UNIVERSITY HOSPITAL CENTER LE LUXEMBOURGIJAR JOURNALNo ratings yet
- (14796821 - Endocrine-Related Cancer) Neoplastic Metastases To The Endocrine GlandsDocument20 pages(14796821 - Endocrine-Related Cancer) Neoplastic Metastases To The Endocrine GlandsMihai MarinescuNo ratings yet
- 17 Iajps17102017 PDFDocument3 pages17 Iajps17102017 PDFBaru Chandrasekhar RaoNo ratings yet
- NIH Public Access: Author ManuscriptDocument22 pagesNIH Public Access: Author ManuscriptHumberto QuimeNo ratings yet
- EANO Guideline On The Diagnosis and Management ofDocument14 pagesEANO Guideline On The Diagnosis and Management ofJames E. WalkerNo ratings yet
- An Overview of Meningiomas: ReviewDocument18 pagesAn Overview of Meningiomas: ReviewMuhammad Naqvi Al FarisiNo ratings yet
- Cancer-5 (HSS 2305) - F2022Document10 pagesCancer-5 (HSS 2305) - F2022zahra.lalani14No ratings yet
- Brain Tumor Thesis StatementDocument8 pagesBrain Tumor Thesis Statementchristinamartinspringfield100% (2)
- Ory 2022Document16 pagesOry 2022Fabián Chávez EcosNo ratings yet
- Ovaire EndometreDocument2 pagesOvaire Endometresafa HADFINo ratings yet
- Focus: Brain Metastases: The HER2 ParadigmDocument8 pagesFocus: Brain Metastases: The HER2 Paradigmferas_oskan781No ratings yet
- The Epidemiology of Lung MetastasesDocument12 pagesThe Epidemiology of Lung MetastasesAlexandra RobuNo ratings yet
- Brain Tumors: Epidemiology and Current Trends in Treatment: September 2015Document22 pagesBrain Tumors: Epidemiology and Current Trends in Treatment: September 2015lameck phiriNo ratings yet
- Neuro Oncol 2014Document9 pagesNeuro Oncol 2014quirinalNo ratings yet
- Cervical Cancer With Brain MetastasesDocument7 pagesCervical Cancer With Brain MetastasesTataru RaduNo ratings yet
- Tumores CerebralesDocument24 pagesTumores CerebralesRocio LedesmaNo ratings yet
- En - 0120 9957 RCG 33 02 00134 PDFDocument10 pagesEn - 0120 9957 RCG 33 02 00134 PDFbernardo04061993No ratings yet
- Clinical and Cytopathological Aspects in Phyllodes Tumors of The BreastDocument7 pagesClinical and Cytopathological Aspects in Phyllodes Tumors of The Breastreeves_coolNo ratings yet
- Abdollahi Et AlDocument5 pagesAbdollahi Et AlMarc DaouNo ratings yet
- Klasifikasi MeningiomaDocument8 pagesKlasifikasi Meningiomahusna fitriaNo ratings yet
- AsianJNeurosurg10150-2524489 070044 PDFDocument4 pagesAsianJNeurosurg10150-2524489 070044 PDFSucipto HartonoNo ratings yet
- (2018) Aggresiveness of Solid Pseudopapillary Neoplasm Literature Review and MetanalysisDocument7 pages(2018) Aggresiveness of Solid Pseudopapillary Neoplasm Literature Review and MetanalysispengadaanNo ratings yet
- Brain Tumors: Epidemiology and Current Trends in Treatment: September 2015Document22 pagesBrain Tumors: Epidemiology and Current Trends in Treatment: September 2015Desty PurnamasariNo ratings yet
- Low and High Grade Gliom in MRSDocument8 pagesLow and High Grade Gliom in MRSHuyen NguyenNo ratings yet
- Pancreatic NETsDocument37 pagesPancreatic NETseztouch12No ratings yet
- GOLD 2021 Teaching Slide Set v102 12nov2020Document58 pagesGOLD 2021 Teaching Slide Set v102 12nov2020banteng wibisonoNo ratings yet
- Acute Respiratory Distress Syndrome: David SweetDocument204 pagesAcute Respiratory Distress Syndrome: David SweetJelenaNo ratings yet
- (14796805 - Journal of Endocrinology) Corticosteroid-Insensitive Asthma - Molecular Mechanisms PDFDocument9 pages(14796805 - Journal of Endocrinology) Corticosteroid-Insensitive Asthma - Molecular Mechanisms PDFTu DangNo ratings yet
- TNF-alpha Levels in Serum and Mononuclear Cell Lysate of Nigerian Tuberculosis Patients at DiagnosisDocument5 pagesTNF-alpha Levels in Serum and Mononuclear Cell Lysate of Nigerian Tuberculosis Patients at Diagnosisbanteng wibisonoNo ratings yet
- TripodDocument1 pageTripodbanteng wibisonoNo ratings yet
- Kawasaki-Like Disease - Emerging Complication During The COVID-19 Pandemic - TheDocument11 pagesKawasaki-Like Disease - Emerging Complication During The COVID-19 Pandemic - Thebanteng wibisonoNo ratings yet
- Kawasaki-Like Disease - Emerging Complication During The COVID-19 Pandemic - TheDocument11 pagesKawasaki-Like Disease - Emerging Complication During The COVID-19 Pandemic - Thebanteng wibisonoNo ratings yet
- GOLD 2021 COPD Teaching SlidesDocument58 pagesGOLD 2021 COPD Teaching Slideshendra ritongaNo ratings yet
- Coccidioidomycosis Idsa Guidelines 2016 PDFDocument35 pagesCoccidioidomycosis Idsa Guidelines 2016 PDFAtanta WahyuNo ratings yet
- Γ And Tnf-Α Levels: Ir - Perpustakaan Universitas AirlanggaDocument1 pageΓ And Tnf-Α Levels: Ir - Perpustakaan Universitas Airlanggabanteng wibisonoNo ratings yet
- An Approach To Interpreting SpirometryDocument8 pagesAn Approach To Interpreting Spirometrylisa_hayesNo ratings yet
- dst15030 1277 1282Document6 pagesdst15030 1277 1282banteng wibisonoNo ratings yet
- Kawasaki-Like Disease - Emerging Complication During The COVID-19 Pandemic - TheDocument11 pagesKawasaki-Like Disease - Emerging Complication During The COVID-19 Pandemic - Thebanteng wibisonoNo ratings yet
- Γ And Tnf-Α Levels: Ir - Perpustakaan Universitas AirlanggaDocument1 pageΓ And Tnf-Α Levels: Ir - Perpustakaan Universitas Airlanggabanteng wibisonoNo ratings yet
- Pathogenesis of Fungal InfectionsDocument70 pagesPathogenesis of Fungal Infectionsማላያላም ማላያላም100% (15)
- MycologyDocument117 pagesMycologybanteng wibisonoNo ratings yet
- A13v12n3 PDFDocument8 pagesA13v12n3 PDFbanteng wibisonoNo ratings yet
- TripodDocument1 pageTripodbanteng wibisonoNo ratings yet
- Idsa GuidelineDocument50 pagesIdsa GuidelinenilnaNo ratings yet
- Human Anatomy and Physiology SyllabusDocument5 pagesHuman Anatomy and Physiology Syllabusbanteng wibisonoNo ratings yet
- Fungi MedicalDocument25 pagesFungi Medicalbanteng wibisono100% (1)
- TripodDocument1 pageTripodbanteng wibisonoNo ratings yet
- Fungi ZugerDocument27 pagesFungi Zugerbanteng wibisonoNo ratings yet
- Role of Echinocandins in Invasive Fungal InfectionsDocument63 pagesRole of Echinocandins in Invasive Fungal Infectionsbanteng wibisonoNo ratings yet
- Idsa GuidelineDocument50 pagesIdsa GuidelinenilnaNo ratings yet
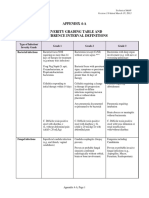
- Severity Grading - Recurrence IntervalDocument5 pagesSeverity Grading - Recurrence Intervalbanteng wibisonoNo ratings yet
- Therapeutic Guidelines in Systemic Fungal Infection 3edDocument127 pagesTherapeutic Guidelines in Systemic Fungal Infection 3eddohuutri66No ratings yet
- Pathogenic Fungal Infection in The Lung: Zhi Li, Gen Lu and Guangxun MengDocument20 pagesPathogenic Fungal Infection in The Lung: Zhi Li, Gen Lu and Guangxun Mengbanteng wibisonoNo ratings yet
- Dimorphic Fungi: Prabin Shah BSCMLT, MSC (Biochemistry)Document49 pagesDimorphic Fungi: Prabin Shah BSCMLT, MSC (Biochemistry)banteng wibisonoNo ratings yet
- Psychology Notes - Cognitive PsychologyDocument17 pagesPsychology Notes - Cognitive PsychologyNikita YapariNo ratings yet
- Inducing Lucid Dreaming: Main Points Minor DetailsDocument2 pagesInducing Lucid Dreaming: Main Points Minor DetailsHarren Asia BueraNo ratings yet
- Soft Tissue DysfunctionDocument8 pagesSoft Tissue DysfunctionphysioaliNo ratings yet
- Script When Presenting About Listening and HearingDocument3 pagesScript When Presenting About Listening and HearingGladyss PunzalanNo ratings yet
- Basal GangliaDocument32 pagesBasal GangliaManisanthosh Kumar100% (2)
- Physiology MCQ - CNSDocument5 pagesPhysiology MCQ - CNSKamaluddin KhanNo ratings yet
- Treatment and Prognosis of Febrile Seizures - UpToDateDocument14 pagesTreatment and Prognosis of Febrile Seizures - UpToDateDinointernosNo ratings yet
- Executive Functions and Their Disorders PDFDocument11 pagesExecutive Functions and Their Disorders PDFLauren SerafiniNo ratings yet
- Sacha Moufarrej Final Term PaperDocument7 pagesSacha Moufarrej Final Term Paperapi-339888853No ratings yet
- Our Lady of La Porteria Academy Senior High School Department Module in Trends, Networks, and Critical Thinking in The 21 Century Culture 12Document7 pagesOur Lady of La Porteria Academy Senior High School Department Module in Trends, Networks, and Critical Thinking in The 21 Century Culture 12Gab ReyesNo ratings yet
- Assessment of Acute and Chronic Pai 2019 Anaesthesia Intensive Care MediciDocument5 pagesAssessment of Acute and Chronic Pai 2019 Anaesthesia Intensive Care MedicipollodearrozNo ratings yet
- Anestesi Lokal Pada Lesi Superfisial: Huntal NapoleonDocument12 pagesAnestesi Lokal Pada Lesi Superfisial: Huntal NapoleonshevinesaNo ratings yet
- F Monostable I) : Ulllted States Patent (19) (11) Patent Number: 6,091,994Document12 pagesF Monostable I) : Ulllted States Patent (19) (11) Patent Number: 6,091,994Mladen CvetkovicNo ratings yet
- Disturbances of ConsciesnessDocument15 pagesDisturbances of ConsciesnessIsak ShatikaNo ratings yet
- Cerebral Contusions and LacerationDocument5 pagesCerebral Contusions and LacerationVithaa'TetaaNo ratings yet
- Cranial Nerve Exam Handout 1Document4 pagesCranial Nerve Exam Handout 1kingpin@mailinatorNo ratings yet
- Hamstring 5Document6 pagesHamstring 5Ardhyan ArdhyanNo ratings yet
- Summary of Clinical Research For LaminineDocument10 pagesSummary of Clinical Research For LaminineDocAxi Maximo Jr AxibalNo ratings yet
- Psychology GeneralDocument73 pagesPsychology GeneralJessmirah LandinginNo ratings yet
- SSC CGL Pre 09 (Eng Sol)Document7 pagesSSC CGL Pre 09 (Eng Sol)Mystic ShivaNo ratings yet
- Imaging For Neuro-Ophthalmic and Orbital Disease - A ReviewDocument24 pagesImaging For Neuro-Ophthalmic and Orbital Disease - A ReviewMashhoor AlfayezNo ratings yet
- Neuro Estudio de Casos Del Dolor Neurologico 2021Document151 pagesNeuro Estudio de Casos Del Dolor Neurologico 2021rogelioNo ratings yet
- Brain Tuner For Cranial Electrotherapy Stimulation (CES)Document9 pagesBrain Tuner For Cranial Electrotherapy Stimulation (CES)Silvano Cardona100% (3)
- Motor Imitation 1-5MDocument1 pageMotor Imitation 1-5MNBNo ratings yet
- Spine Structure and FunctionDocument19 pagesSpine Structure and Functionakhil dattaNo ratings yet
- Theory of First Language Acquisition (Language Acquisition Device) (WEEK 8) Mind MAPDocument7 pagesTheory of First Language Acquisition (Language Acquisition Device) (WEEK 8) Mind MAPlopobhia noobyteNo ratings yet
- Dwnload Full Learning and Memory 2nd Edition Gluck Test Bank PDFDocument35 pagesDwnload Full Learning and Memory 2nd Edition Gluck Test Bank PDFalvacalliopeewc100% (9)
- Code Stroke & Hyperacute Stroke TreatmentDocument35 pagesCode Stroke & Hyperacute Stroke TreatmentSitti Fatwan NisakNo ratings yet
- Rehabilitation AmbulationDocument14 pagesRehabilitation AmbulationDeborah SalinasNo ratings yet
- Approach To A Child With HemiplegiaDocument5 pagesApproach To A Child With HemiplegiaBeenish IqbalNo ratings yet