You might also like
- WWW - Kup.at/ Journals/eano/index - HTML: Systemic Treatment of Recurrent MeningiomaDocument8 pagesWWW - Kup.at/ Journals/eano/index - HTML: Systemic Treatment of Recurrent MeningiomaAnonymous KKqrboTNo ratings yet
- Central Nervous System MetastasesFrom EverandCentral Nervous System MetastasesManmeet AhluwaliaNo ratings yet
- Multiple Myeloma and Other Plasma Cell NeoplasmsFrom EverandMultiple Myeloma and Other Plasma Cell NeoplasmsMeletios A. DimopoulosNo ratings yet
- Journal Current Treatment Options For MeningiomaDocument10 pagesJournal Current Treatment Options For MeningiomaNEUROUNSRAT XVIIINo ratings yet
- Jurnal KedokteranDocument9 pagesJurnal KedokteranannisanoviaNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- An Overview of Meningiomas: ReviewDocument18 pagesAn Overview of Meningiomas: ReviewMuhammad Naqvi Al FarisiNo ratings yet
- Neuroblastoma Origin and Therapeutic Targets For IDocument26 pagesNeuroblastoma Origin and Therapeutic Targets For IRokia GhariebNo ratings yet
- Lancet NeDocument10 pagesLancet NeKrisTianz OkaNo ratings yet
- Brain Tumors in ChildrenFrom EverandBrain Tumors in ChildrenAmar GajjarNo ratings yet
- Biomedicines: Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future DirectionsDocument23 pagesBiomedicines: Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future DirectionsAlfian_Dwi_SNo ratings yet
- Molecular Biomarkers in Sinonasal Cancers: New Frontiers in Diagnosis and TreatmentDocument13 pagesMolecular Biomarkers in Sinonasal Cancers: New Frontiers in Diagnosis and TreatmentventyperdanasariNo ratings yet
- Pathophysiology of Meningiomas 2003Document18 pagesPathophysiology of Meningiomas 2003Klinik medan DeliNo ratings yet
- Therapeutic Options in Neuro-Oncology: Molecular SciencesDocument34 pagesTherapeutic Options in Neuro-Oncology: Molecular SciencesAhana MukherjeeNo ratings yet
- Extracranial Metastases of Anaplastic Meningioma: Case ReportDocument6 pagesExtracranial Metastases of Anaplastic Meningioma: Case ReportRizky AdriansahNo ratings yet
- Follow UpDocument6 pagesFollow UpWinda HaeriyokoNo ratings yet
- Clinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDocument9 pagesClinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpSiva SubramaniamNo ratings yet
- Cpho023 01 03Document11 pagesCpho023 01 03Kyung-Nam KohNo ratings yet
- Soft Tissue Tumors: A Practical and Comprehensive Guide to Sarcomas and Benign NeoplasmsFrom EverandSoft Tissue Tumors: A Practical and Comprehensive Guide to Sarcomas and Benign NeoplasmsNo ratings yet
- 6279 17690 1 SMDocument14 pages6279 17690 1 SMvistaNo ratings yet
- Biomedicines: Emerging Medical Treatments For Meningioma in The Molecular EraDocument21 pagesBiomedicines: Emerging Medical Treatments For Meningioma in The Molecular EraNorAmalinaNo ratings yet
- Clinical Endocrinology - 2022 - Coopmans - Molecular Genetic Testing in The Management of Pituitary DiseaseDocument12 pagesClinical Endocrinology - 2022 - Coopmans - Molecular Genetic Testing in The Management of Pituitary DiseasegarrobosNo ratings yet
- Tumors of The Nervous SystemDocument45 pagesTumors of The Nervous SystemIsaac MwangiNo ratings yet
- Neuro Oncol 2014Document9 pagesNeuro Oncol 2014quirinalNo ratings yet
- Atlas of Clinical Cases on Brain Tumor ImagingFrom EverandAtlas of Clinical Cases on Brain Tumor ImagingYelda ÖzsunarNo ratings yet
- Olfactory Groove MeningiomaDocument16 pagesOlfactory Groove Meningiomaclaudio RivasNo ratings yet
- Epidemiology, Natural History, Pathology and Management of Medulloblastoma in ChildrenDocument48 pagesEpidemiology, Natural History, Pathology and Management of Medulloblastoma in ChildrenSam OlukaNo ratings yet
- New WHO Classification of Pituitary Adenomas (4th Edition) : Assessment of Pituitary Transcription Factors and The Prognostic Histological FactorsDocument5 pagesNew WHO Classification of Pituitary Adenomas (4th Edition) : Assessment of Pituitary Transcription Factors and The Prognostic Histological FactorscristianescNo ratings yet
- Brain TumorDocument15 pagesBrain TumorA Farid WajdyNo ratings yet
- Diagnosis and Treatment of Pineal Region Tumors in AdultsDocument21 pagesDiagnosis and Treatment of Pineal Region Tumors in AdultsJames E. WalkerNo ratings yet
- Embryonal CnsDocument13 pagesEmbryonal CnsPoly EdayanalNo ratings yet
- The Basics of Cancer ImmunotherapyFrom EverandThe Basics of Cancer ImmunotherapyHaidong DongNo ratings yet
- Ni Hms 278458Document8 pagesNi Hms 278458VidinikusumaNo ratings yet
- NIH Public Access: Author ManuscriptDocument22 pagesNIH Public Access: Author ManuscriptHumberto QuimeNo ratings yet
- Ependymoma: Evaluation and Management UpdatesDocument9 pagesEpendymoma: Evaluation and Management UpdatesIsaac Bacasehua InzunzaNo ratings yet
- Tumor Immune Microenvironment in Cancer Progression and Cancer TherapyFrom EverandTumor Immune Microenvironment in Cancer Progression and Cancer TherapyPawel KalinskiNo ratings yet
- (10920684 - Neurosurgical Focus) Clinical Potential of Meningioma Genomic Insights - A Practical Review For NeurosurgeonsDocument7 pages(10920684 - Neurosurgical Focus) Clinical Potential of Meningioma Genomic Insights - A Practical Review For Neurosurgeonsgasosa cNo ratings yet
- 3870 51441 2 PBDocument18 pages3870 51441 2 PBApriyanto LatiefNo ratings yet
- 07 Central Nervous System TumorsDocument25 pages07 Central Nervous System TumorsRolando Rocha AtenciaNo ratings yet
- Department of Internal Medicine,: Prof WBP Matuja Muhas/MnhDocument31 pagesDepartment of Internal Medicine,: Prof WBP Matuja Muhas/MnhDanyu KibuguluNo ratings yet
- Brain CancerDocument7 pagesBrain Cancerbanteng wibisonoNo ratings yet
- Neuro Oncol 2artigo012 Rudà Iv55 64Document10 pagesNeuro Oncol 2artigo012 Rudà Iv55 64Glauce L TrevisanNo ratings yet
- Materials and MethodsDocument2 pagesMaterials and MethodsRedigo RahmadhaniNo ratings yet
- 10.1007@s00270 019 02259 WDocument7 pages10.1007@s00270 019 02259 WJuan Daniel Serrano GuerreroNo ratings yet
- Tratamiento de Los Gliomas - En.esDocument15 pagesTratamiento de Los Gliomas - En.esAndrea Viviana Galvis MolinaNo ratings yet
- Pediatric Neuro-Oncology: Understanding Brain Tumors in ChildrenDocument17 pagesPediatric Neuro-Oncology: Understanding Brain Tumors in ChildrenRandy UlloaNo ratings yet
- Recent Advances in Radiological and Radionuclide Imaging and Therapy of Neuroendocrine TumoursDocument14 pagesRecent Advances in Radiological and Radionuclide Imaging and Therapy of Neuroendocrine TumoursrevanthNo ratings yet
- NeuroblastomaDocument19 pagesNeuroblastomaTri Andhika Dessy WahyuniNo ratings yet
- Cancer-5 (HSS 2305) - F2022Document10 pagesCancer-5 (HSS 2305) - F2022zahra.lalani14No ratings yet
- Seizures, Headaches, and Right Hemiparesis: MeningiomaDocument2 pagesSeizures, Headaches, and Right Hemiparesis: MeningiomacazecageNo ratings yet
- Maris 2007Document15 pagesMaris 2007asialoren74No ratings yet
- Tumores CerebralesDocument24 pagesTumores CerebralesRocio LedesmaNo ratings yet
- Imun PDFDocument4 pagesImun PDFLeyni SabatiniNo ratings yet
- Zhao 2020Document7 pagesZhao 2020asialoren74No ratings yet
- Neuropathologic Features of Central Nervous System HemangioblastomaDocument11 pagesNeuropathologic Features of Central Nervous System HemangioblastomaDavid Camilo GomezNo ratings yet
- Whole Exome and Transcriptome Analyses Integrated With Microenvironmental Immune Signatures of Lung Squamous Cell CarcinomaDocument13 pagesWhole Exome and Transcriptome Analyses Integrated With Microenvironmental Immune Signatures of Lung Squamous Cell CarcinomaRubens BegajNo ratings yet
- Brain TumorsDocument12 pagesBrain Tumors36Kushal saNdHuNo ratings yet
- RetinoblastomaDocument16 pagesRetinoblastomaDiego Joaquín RiveraNo ratings yet
- PDF TJP 2175Document5 pagesPDF TJP 2175husna fitriaNo ratings yet
- Clinical Outcome of Tetanus Based On Dakar Tetanus Severity Score in Paediatric Intensive Care Unit of ADocument5 pagesClinical Outcome of Tetanus Based On Dakar Tetanus Severity Score in Paediatric Intensive Care Unit of Ahusna fitriaNo ratings yet
- Fped 09 591052Document6 pagesFped 09 591052husna fitriaNo ratings yet
- RISK FACTORS FOR HEARING LOSSDocument11 pagesRISK FACTORS FOR HEARING LOSShusna fitriaNo ratings yet
- Tetanus Neonatorum: Its Associated Risk Factors and Mortality Rate in Khyber PakhtunkhwaDocument3 pagesTetanus Neonatorum: Its Associated Risk Factors and Mortality Rate in Khyber Pakhtunkhwahusna fitriaNo ratings yet
- Jurnal Fix Faktor Risiko Peningkatan Ambang Dengar Pada Pekerja PengelasanDocument8 pagesJurnal Fix Faktor Risiko Peningkatan Ambang Dengar Pada Pekerja Pengelasanhusna fitriaNo ratings yet
- Faktor Yang Berhubungan Dengan GG Pendengaran Pada Pekerja Aircrew 2021Document11 pagesFaktor Yang Berhubungan Dengan GG Pendengaran Pada Pekerja Aircrew 2021husna fitriaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Keluhan Pendengaran Pada Pekerja Di Bagian Produksi Di PT. Hervenia Kampar LestariDocument14 pagesFaktor-Faktor Yang Berhubungan Dengan Keluhan Pendengaran Pada Pekerja Di Bagian Produksi Di PT. Hervenia Kampar Lestarihusna fitriaNo ratings yet
- Pneumonia Treatment and DiagnosisDocument5 pagesPneumonia Treatment and Diagnosishusna fitriaNo ratings yet
- Jurnal Tambahan 1Document13 pagesJurnal Tambahan 1husna fitriaNo ratings yet
- Ginsberg 1996Document10 pagesGinsberg 1996husna fitriaNo ratings yet
- A Case Series, Experience of Using 20% Potassium Hydroxide Solution To Treat Adult Sexually Transmitted Molluscum ContangiosumDocument6 pagesA Case Series, Experience of Using 20% Potassium Hydroxide Solution To Treat Adult Sexually Transmitted Molluscum Contangiosumhusna fitriaNo ratings yet
- Biomedicines: Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future DirectionsDocument23 pagesBiomedicines: Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future DirectionsAlfian_Dwi_SNo ratings yet
- Emergency Procedures Masterclass: Siamak Moayedi, MDDocument23 pagesEmergency Procedures Masterclass: Siamak Moayedi, MDCoding NinjaNo ratings yet
- Model Test PapersDocument2 pagesModel Test Papersprofarmah6150No ratings yet
- Ultrasound Imaging of The NeckDocument25 pagesUltrasound Imaging of The Neckmark jacob dela rosaNo ratings yet
- Diagnostic Laparoscopy: Reason For VisitDocument4 pagesDiagnostic Laparoscopy: Reason For Visitdrnareshkumar3281No ratings yet
- Urinary SystemDocument66 pagesUrinary SystemJustine Vens G. AgustinNo ratings yet
- Negative Pressure Wound Therapy The Experience of Our Surgery DepartmentDocument10 pagesNegative Pressure Wound Therapy The Experience of Our Surgery DepartmentAthenaeum Scientific PublishersNo ratings yet
- ASRA Guidelines Regional Anaesthesia in Anticoagulated PatientDocument10 pagesASRA Guidelines Regional Anaesthesia in Anticoagulated PatientRizg AlamriNo ratings yet
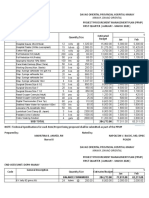
- DOPH-MANAY Procurement Plan for Medical SuppliesDocument16 pagesDOPH-MANAY Procurement Plan for Medical SuppliesJan Oneille Y. VallesNo ratings yet
- Catheter Complication: Managing Pitfalls in IV Therapy: Perawat Hebat - Perawat TangguhDocument37 pagesCatheter Complication: Managing Pitfalls in IV Therapy: Perawat Hebat - Perawat TangguhAdi SullivanNo ratings yet
- Ocular EmergencyDocument25 pagesOcular EmergencyJo AnneNo ratings yet
- PDF TextDocument2 pagesPDF TextJaiprakash GuptaNo ratings yet
- Endodontic SurgeryDocument16 pagesEndodontic SurgeryauntymayaNo ratings yet
- 2018 NJAASC Member RosterDocument15 pages2018 NJAASC Member Rostersatish vermaNo ratings yet
- Zygoma Fixture in The Management of Advanced Atrophy of The Maxilla Technique and Long Term ResultsDocument17 pagesZygoma Fixture in The Management of Advanced Atrophy of The Maxilla Technique and Long Term ResultspedroNo ratings yet
- Guide to miscarriage diagnosis and careDocument22 pagesGuide to miscarriage diagnosis and careherryNo ratings yet
- AO - Trans Obturator Technique Versus Suburethral Tape PDFDocument15 pagesAO - Trans Obturator Technique Versus Suburethral Tape PDFGustavo flores quispeNo ratings yet
- Medical Surgical Nursing Module 10Document34 pagesMedical Surgical Nursing Module 10weissNo ratings yet
- Hemodynamic MonitoringDocument37 pagesHemodynamic MonitoringStephy Sojan50% (2)
- Accreditation Audit - RAFT Task 1Document13 pagesAccreditation Audit - RAFT Task 1janesdarren_16310790100% (1)
- Balanco 2021Document4 pagesBalanco 2021HllerdNo ratings yet
- SARP (Skin Anesthesia Radiology Psychiatry) Review 2010Document4 pagesSARP (Skin Anesthesia Radiology Psychiatry) Review 2010QworldNo ratings yet
- The Circulatory System of AmphibiansDocument3 pagesThe Circulatory System of AmphibiansNathaniel FelicianoNo ratings yet
- Download ebook Greens Operative Hand Surgery 2 Volume Set Pdf full chapter pdfDocument67 pagesDownload ebook Greens Operative Hand Surgery 2 Volume Set Pdf full chapter pdfkathleen.lloyd406100% (22)
- Preoperative Care Guide for SurgeonsDocument33 pagesPreoperative Care Guide for SurgeonsPrincewill SeiyefaNo ratings yet
- Basic Life SupportDocument31 pagesBasic Life SupportNHUXUANNo ratings yet
- Closed Vs Open SuctionDocument5 pagesClosed Vs Open SuctionKhushboo DurejaNo ratings yet
- Shunt Calculation, NICVDDocument31 pagesShunt Calculation, NICVDNavojit ChowdhuryNo ratings yet
- Spinal Subdural Hematoma Responsible For A Syndrome of The Tail of A Horse About A Case in The University Hospital Center of Guadeloupe and Review of LiteratureDocument4 pagesSpinal Subdural Hematoma Responsible For A Syndrome of The Tail of A Horse About A Case in The University Hospital Center of Guadeloupe and Review of LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Z-Plasty Technique On The Frenectomy ApproachDocument5 pagesThe Z-Plasty Technique On The Frenectomy ApproachVineet ArunNo ratings yet
- Prevention of Dialysis Acces Cath Related InfectionDocument33 pagesPrevention of Dialysis Acces Cath Related Infectionbarkah04No ratings yet