You might also like
- Essential Physical Therapy Terminology: Navigating Physical Therapy LanguageFrom EverandEssential Physical Therapy Terminology: Navigating Physical Therapy LanguageNo ratings yet
- Description of Physical Therapy WCPTDocument12 pagesDescription of Physical Therapy WCPTHadassah Salinas de FerroNo ratings yet
- WCPT Description of Physical Therapy-Sep07-Rev 2Document7 pagesWCPT Description of Physical Therapy-Sep07-Rev 2Mark JayNo ratings yet
- Description of Physical Therapy: Policy StatementDocument10 pagesDescription of Physical Therapy: Policy StatementBenny WirawanNo ratings yet
- Guide Apta 3.0 - English PDFDocument144 pagesGuide Apta 3.0 - English PDFEveliin DaYana43% (7)
- Professional Conduct ETHICSDocument16 pagesProfessional Conduct ETHICSAman hussainNo ratings yet
- 2.introduction To The Guide To Physical Therapist Practice - Guide To PhysDocument11 pages2.introduction To The Guide To Physical Therapist Practice - Guide To Physalejandra rengifoNo ratings yet
- Guide to Physical Therapist Practice: IntroductionDocument98 pagesGuide to Physical Therapist Practice: IntroductionKana AmesNo ratings yet
- Physiotherapy Scope of Practice-Article PDFDocument3 pagesPhysiotherapy Scope of Practice-Article PDFeins_mptNo ratings yet
- PT in CBRDocument3 pagesPT in CBRAkshay BadoreNo ratings yet
- History and Definition of Physical TherapyDocument50 pagesHistory and Definition of Physical TherapyJiggs LimNo ratings yet
- Code of Ethics For The Physical TherapistDocument5 pagesCode of Ethics For The Physical TherapistdanielgriffinotherNo ratings yet
- Role of a Physical TherapistDocument8 pagesRole of a Physical TherapistNestor BalboaNo ratings yet
- Vision Statement For The Physical Therapy Profession and Guiding Principles To Achieve The VisionDocument3 pagesVision Statement For The Physical Therapy Profession and Guiding Principles To Achieve The VisionJánosNo ratings yet
- The Federation of State Boards of Physical Therapy Standards of CompetenceDocument9 pagesThe Federation of State Boards of Physical Therapy Standards of CompetenceAlexaNo ratings yet
- 2-Contemporary Practice IssuesDocument39 pages2-Contemporary Practice IssuesAyesha AsifNo ratings yet
- Module 6 THE HEALTH CARE PROVIDERDocument8 pagesModule 6 THE HEALTH CARE PROVIDERColeen TanNo ratings yet
- Physiotherapy Is One of The Main Health Professions Involved in RehabilitationDocument1 pagePhysiotherapy Is One of The Main Health Professions Involved in RehabilitationDeepak SomanNo ratings yet
- RehabilitationDocument18 pagesRehabilitationpoulami mukherjeeNo ratings yet
- Apta StandardsDocument3 pagesApta Standardsapi-306297846No ratings yet
- Contamproary Practice IssuesDocument22 pagesContamproary Practice Issuespihabo3594No ratings yet
- Code of EthicsDocument2 pagesCode of EthicsmilananandNo ratings yet
- Code of EthicsDocument6 pagesCode of EthicsHemant WelfareNo ratings yet
- Competences of Advanced NursingDocument8 pagesCompetences of Advanced NursingNatukunda DianahNo ratings yet
- Conceptual Framework For Clinical PracticeDocument19 pagesConceptual Framework For Clinical PracticeFisher LeeNo ratings yet
- مقدمة و متطلباتDocument9 pagesمقدمة و متطلباتseedhassan686No ratings yet
- Code of Ethics in PhysiotherapyDocument7 pagesCode of Ethics in PhysiotherapyRex RaiNo ratings yet
- Role of Physical TherapistsDocument4 pagesRole of Physical TherapistsdrhalwagyNo ratings yet
- Code of Ethics For The Physical Therapist: HOD S06-20-28-25Document3 pagesCode of Ethics For The Physical Therapist: HOD S06-20-28-25Ankit1402No ratings yet
- Ethical PrinciplesDocument6 pagesEthical PrinciplesmilananandNo ratings yet
- PediatricAPTA FactSheet PhysicalTherapistsPractitionerofChoice - 2020Document5 pagesPediatricAPTA FactSheet PhysicalTherapistsPractitionerofChoice - 2020Juan Ignacio Gómez IruretagoyenaNo ratings yet
- Code of EthicsDocument3 pagesCode of EthicsMaged BashaNo ratings yet
- APTA Vision 2020 PDFDocument2 pagesAPTA Vision 2020 PDFHasan RahmanNo ratings yet
- CPI CriteriaDocument8 pagesCPI CriteriaMichael KoernerNo ratings yet
- APTA Guide For Professional Conduct: PurposeDocument8 pagesAPTA Guide For Professional Conduct: PurposeJIA YUET NG100% (1)
- Prelim Exam 22Document2 pagesPrelim Exam 22Zgama AbdulrahmanNo ratings yet
- Roles and Responsibilitiesof A Professional NurseDocument94 pagesRoles and Responsibilitiesof A Professional Nursecassandraolson.kya07No ratings yet
- GERIATRICE HEALTH CARE TEAM-FinalDocument6 pagesGERIATRICE HEALTH CARE TEAM-Finalcamile buhangin100% (2)
- PT in CanadaDocument27 pagesPT in CanadaAna CáceresNo ratings yet
- APTA Guide For Professional ConductDocument4 pagesAPTA Guide For Professional ConductdanielgriffinotherNo ratings yet
- PT Job Description PowerbackDocument3 pagesPT Job Description Powerbackdk15janNo ratings yet
- Guidelines To Physical Therapist Practice APTADocument1,006 pagesGuidelines To Physical Therapist Practice APTAGustavo Cabanas82% (11)
- Planning For A: Healt H Caree RDocument46 pagesPlanning For A: Healt H Caree RJanette Anne Reyes MacaraigNo ratings yet
- OT Code of EthicsDocument8 pagesOT Code of Ethicsxarae23No ratings yet
- Legal and Ethical Issues FinalDocument8 pagesLegal and Ethical Issues FinalmandykalerNo ratings yet
- Philosophy and Theoretical Framework of Community Health NursingDocument9 pagesPhilosophy and Theoretical Framework of Community Health Nursingᜀᜇᜒᜐ᜔ ᜇᜒᜎ ᜃ᜔ᜇᜓᜐ᜔No ratings yet
- 200-CQDN-666574-ND - Job Description and Person SpecificationDocument6 pages200-CQDN-666574-ND - Job Description and Person Specificationsachin_sawant1985No ratings yet
- Code and Ethics Standards 2010Document11 pagesCode and Ethics Standards 2010bsdeepuNo ratings yet
- European Core Standards of Physiotherapy PracticeDocument43 pagesEuropean Core Standards of Physiotherapy Practicerambabs369No ratings yet
- RehabilitationDocument5 pagesRehabilitationMOHAMMED ABUBACKER SIDDIQ ANo ratings yet
- Role of The Doctor Consensus StatementDocument3 pagesRole of The Doctor Consensus StatementMaxNo ratings yet
- CSP Core Standards 2005 0Document68 pagesCSP Core Standards 2005 0Irina MafteiNo ratings yet
- Professional Adjustment Final 2Document41 pagesProfessional Adjustment Final 2lielani_martinezNo ratings yet
- CBT for Psychological Well-Being in Cancer: A Skills Training Manual Integrating DBT, ACT, Behavioral Activation and Motivational InterviewingFrom EverandCBT for Psychological Well-Being in Cancer: A Skills Training Manual Integrating DBT, ACT, Behavioral Activation and Motivational InterviewingNo ratings yet
- Public Health Nursing: Scope and Standards of PracticeFrom EverandPublic Health Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (1)
- Food Counselling. How To Motivate People To Change Eating HabitsFrom EverandFood Counselling. How To Motivate People To Change Eating HabitsNo ratings yet
- Essentials of Para-Medical Terminology: Mastering the Para-Medical LanguageFrom EverandEssentials of Para-Medical Terminology: Mastering the Para-Medical LanguageNo ratings yet
- BAC814: Management Accounting: Discussion QuestionsDocument3 pagesBAC814: Management Accounting: Discussion QuestionsJotham MunalaNo ratings yet
- The African Academy of Sciences: Job Application FormDocument5 pagesThe African Academy of Sciences: Job Application FormJotham MunalaNo ratings yet
- Classification of FQE Papers 2016Document3 pagesClassification of FQE Papers 2016Jotham MunalaNo ratings yet
- Office of The President Department of Civil Registration Application For A Birth CertificateDocument1 pageOffice of The President Department of Civil Registration Application For A Birth CertificateJotham MunalaNo ratings yet
- Pharmacy practical exam requirements under $50,000Document18 pagesPharmacy practical exam requirements under $50,000Jotham MunalaNo ratings yet
- TCC 2017Document1 pageTCC 2017Jotham MunalaNo ratings yet
- Code of EthicsDocument2 pagesCode of EthicsmilananandNo ratings yet
- Coupled Motions of The Lumbar Spine: A Narrative ReviewDocument5 pagesCoupled Motions of The Lumbar Spine: A Narrative Reviewrapannika100% (2)
- Role of AI in PhysiotherapyDocument3 pagesRole of AI in PhysiotherapyAli MansoorNo ratings yet
- Improving Veterans MSK Rehabilitation ServicesDocument58 pagesImproving Veterans MSK Rehabilitation ServicesJason SnapeNo ratings yet
- Evaluation Is Treatment For Low Back PainDocument11 pagesEvaluation Is Treatment For Low Back PainVizaNo ratings yet
- Orthotics Consensus Conference ReportDocument354 pagesOrthotics Consensus Conference ReportAlec joshua RapadaNo ratings yet
- Handbook of Non-Drug InterventionsDocument44 pagesHandbook of Non-Drug InterventionsFadli NugrahaNo ratings yet
- 13 Chapter 7Document19 pages13 Chapter 7Sadam_fasterNo ratings yet
- LK 2015 Dislokasi SendiDocument5 pagesLK 2015 Dislokasi SendiTriaditya KresnaNo ratings yet
- Occupational Therapy's Role in Adult Cognitive DisordersDocument2 pagesOccupational Therapy's Role in Adult Cognitive DisordersThe American Occupational Therapy AssociationNo ratings yet
- FtensidaDocument9 pagesFtensidaMaría FuentesNo ratings yet
- Eportfolio ResumeDocument2 pagesEportfolio Resumeapi-546354429No ratings yet
- Clinical Practice Guidelines Burns Physiotherapy and Occupational TherapyDocument34 pagesClinical Practice Guidelines Burns Physiotherapy and Occupational Therapyfauziafahmi95100% (2)
- Ataxia Coordinative Physiotherapy BroetzDocument12 pagesAtaxia Coordinative Physiotherapy BroetzchristinaNo ratings yet
- Applicaiton For Initial AssessmentDocument10 pagesApplicaiton For Initial AssessmentAditi AngraNo ratings yet
- Deborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDocument5 pagesDeborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDago Angel Prieto PalavecinoNo ratings yet
- Epidimiological ApprochDocument14 pagesEpidimiological ApprochBabita DhruwNo ratings yet
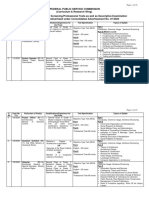
- Syllabus-Combined Ad No 07-2020Document35 pagesSyllabus-Combined Ad No 07-2020Aslam RehmanNo ratings yet
- 1332251810binder2Document33 pages1332251810binder2CoolerAdsNo ratings yet
- Resume 2017Document2 pagesResume 2017api-384685979No ratings yet
- Psthe 1Document111 pagesPsthe 1Angelica RicoNo ratings yet
- Effects of PNF Method For Hemiplegic Patients With Brachial Predominance After Stroke: Controlled and Blinded Clinical TrialDocument6 pagesEffects of PNF Method For Hemiplegic Patients With Brachial Predominance After Stroke: Controlled and Blinded Clinical TrialAperito InternationalNo ratings yet
- A Textbook of Sports and Exercise PhysiologyDocument347 pagesA Textbook of Sports and Exercise PhysiologyPraneeth KumarNo ratings yet
- Grove Music OnlineDocument12 pagesGrove Music OnlineOrleansmusicen EnsemblesNo ratings yet
- Module 1: Psychology of Work PDFDocument16 pagesModule 1: Psychology of Work PDFIRENE MARTINEZ VALENZUELANo ratings yet
- M T TDocument28 pagesM T TAjay Pal NattNo ratings yet
- Akupresure InggrisDocument11 pagesAkupresure InggrisJuniatiNo ratings yet
- Rehabilitation Manual-NHS TrustDocument47 pagesRehabilitation Manual-NHS TrustGleidys NavarroNo ratings yet
- Meuhedet's Complementary Comprehensive Health Insurance PlanDocument16 pagesMeuhedet's Complementary Comprehensive Health Insurance PlanEnglishAccessibilityNo ratings yet
- Cebu Doctors' University College of Rehabilitative Sciences Department of Physical TherapyDocument3 pagesCebu Doctors' University College of Rehabilitative Sciences Department of Physical Therapysss_sarzzzNo ratings yet
- Clinical Study Treatment Effects of Upper Limb Action Observation Therapy and Mirror Therapy On Rehabilitation Outcomes After Subacute Stroke: A Pilot StudyDocument10 pagesClinical Study Treatment Effects of Upper Limb Action Observation Therapy and Mirror Therapy On Rehabilitation Outcomes After Subacute Stroke: A Pilot Studyerfan khanNo ratings yet