You might also like
- Pain (MS)Document4 pagesPain (MS)Lezel LaracasNo ratings yet
- LMN Disease - DiagnosisDocument6 pagesLMN Disease - DiagnosisIqi Siti RizkiahNo ratings yet
- Rheumatoid Arthritis ReportDocument3 pagesRheumatoid Arthritis ReportHeloise DiamanteNo ratings yet
- Neurology in TableDocument93 pagesNeurology in TableHassan Bani SaeidNo ratings yet
- Reflex Sympathetic Dystrophy andDocument37 pagesReflex Sympathetic Dystrophy andHarinderNo ratings yet
- AnnexIII DifferentialDiagnosis FromNLEP India PDFDocument3 pagesAnnexIII DifferentialDiagnosis FromNLEP India PDFAegirine RafilahNo ratings yet
- MRAT 211 - Ankle & Foot TRANSDocument8 pagesMRAT 211 - Ankle & Foot TRANSLovely GopezNo ratings yet
- Pathophysiology of Pain in BiliodigestiDocument19 pagesPathophysiology of Pain in Biliodigestiprabowoaji12No ratings yet
- Pathophysiology of Pain in BiliodigestiDocument19 pagesPathophysiology of Pain in Biliodigestiprabowoaji12No ratings yet
- QuizletDocument37 pagesQuizletnaimNo ratings yet
- Chronic Pain: - Painful Conditions. - Far Exceeds The Expected Duration - of Motor FunctionDocument7 pagesChronic Pain: - Painful Conditions. - Far Exceeds The Expected Duration - of Motor FunctionCalaena SardothienNo ratings yet
- TRANS - Somatic SensationsDocument10 pagesTRANS - Somatic SensationsCaesar Anthony Dequito SamsonNo ratings yet
- TRANS PAIN W NotesDocument6 pagesTRANS PAIN W NotesjoanneNo ratings yet
- p12-13 Touch and PainDocument41 pagesp12-13 Touch and PainBob SmithNo ratings yet
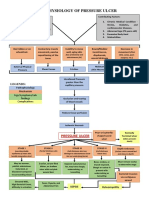
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- Diseases of The Pns Rosales, MD: Peripheral Nervous SystemDocument9 pagesDiseases of The Pns Rosales, MD: Peripheral Nervous SystemJanina AndreaNo ratings yet
- The Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis UniversityDocument53 pagesThe Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis Universitymonica ortizNo ratings yet
- Hierarchy of Response To SensationDocument18 pagesHierarchy of Response To SensationnictitateNo ratings yet
- 111 Peripheral NeuropathyDocument17 pages111 Peripheral NeuropathyjassbhanguNo ratings yet
- DIAGNOSIS AND TREATMENT NN Fino-2017Document46 pagesDIAGNOSIS AND TREATMENT NN Fino-2017siti rumaisaNo ratings yet
- Pathophysiology and Managemement of Pain: Dr. Subodh Kumar Mahto, Dept. of Medicine Pgimer, DR - RML Hospital. NEW DelhiDocument86 pagesPathophysiology and Managemement of Pain: Dr. Subodh Kumar Mahto, Dept. of Medicine Pgimer, DR - RML Hospital. NEW DelhiMarcelo GutiérrezNo ratings yet
- Physiology of Pain Pathways and Its Modulation: DR HassanDocument79 pagesPhysiology of Pain Pathways and Its Modulation: DR HassanvaishnaviNo ratings yet
- Sensory DisturbancesDocument4 pagesSensory DisturbancesNicNo ratings yet
- Reflex Sympathetic DystrophyDocument13 pagesReflex Sympathetic Dystrophynaman shahNo ratings yet
- Lecture 37-Diseases of The Spine and Spinal Cord-Dr. Yudiyanta, SP.S (K) (2018)Document44 pagesLecture 37-Diseases of The Spine and Spinal Cord-Dr. Yudiyanta, SP.S (K) (2018)Chairul AmriNo ratings yet
- Management Acute PainDocument110 pagesManagement Acute PainjohannesNo ratings yet
- Pathophysiology Carpal Tunnel Syndrome: Due To Etiological FactorsDocument1 pagePathophysiology Carpal Tunnel Syndrome: Due To Etiological FactorsLeslie Lagat PaguioNo ratings yet
- SensesDocument6 pagesSensesNicole FinuliarNo ratings yet
- Block of InformationDocument19 pagesBlock of InformationALok KumarNo ratings yet
- Dr. Dioszeghy Peter MononeuropathiesDocument52 pagesDr. Dioszeghy Peter MononeuropathiesAhmad abu-dayyehNo ratings yet
- 001 - DM - ComplicationsDocument23 pages001 - DM - ComplicationsLucas Victor AlmeidaNo ratings yet
- Orthopedic RheumatologyDocument9 pagesOrthopedic RheumatologyAngelinaNo ratings yet
- Iapc November 2016 Pain PathophysiologyDocument45 pagesIapc November 2016 Pain PathophysiologypradeepNo ratings yet
- Manajemen Nyeri: Nella Harisa NovianiDocument30 pagesManajemen Nyeri: Nella Harisa NovianiCitra AnggrainiNo ratings yet
- Manajemen NyeriDocument30 pagesManajemen NyericlvpratamaNo ratings yet
- Acne, Physical Dermatoses, Bacterial InfectiosDocument35 pagesAcne, Physical Dermatoses, Bacterial InfectiosRiena Austine Leonor NarcillaNo ratings yet
- Clinical Significance of Demyelinating Lesions of The CNSDocument5 pagesClinical Significance of Demyelinating Lesions of The CNSTransverse Myelitis AssociationNo ratings yet
- 05b-Sensory FunctionDocument57 pages05b-Sensory FunctionUntung Edi PurwantoNo ratings yet
- Mono ParesisDocument2 pagesMono ParesisYulyani PratiwiNo ratings yet
- Presented By-Dr. Vijaya Laxmi Murty 1 Year Postgraduate StudenDocument60 pagesPresented By-Dr. Vijaya Laxmi Murty 1 Year Postgraduate StudenRAANUNo ratings yet
- Management of Acute PainDocument76 pagesManagement of Acute PainAnonymous nruHyuwtJ100% (1)
- Comparison of Rheumatoid and OsteoarthritisDocument4 pagesComparison of Rheumatoid and OsteoarthritisWaseem Khan AfridiNo ratings yet
- Localisation in NeurologyDocument19 pagesLocalisation in NeurologyArnav GuptaNo ratings yet
- Localisation in NeurologyDocument19 pagesLocalisation in NeurologyArnav GuptaNo ratings yet
- Pain PathwayDocument17 pagesPain PathwaySalsabila Al-BasheerNo ratings yet
- Acute Flaccid Paralysis-1Document20 pagesAcute Flaccid Paralysis-1Peterson Wachira HscNo ratings yet
- Peripheral Neuropathies PathoDocument2 pagesPeripheral Neuropathies PathoSOLEIL LOUISE LACSON MARBASNo ratings yet
- Peripheral Neuropathy AidaDocument36 pagesPeripheral Neuropathy AidaAdlina ArifinNo ratings yet
- Management of Chronic Pain With Interventional TechniqueDocument40 pagesManagement of Chronic Pain With Interventional TechniqueRovika RovikaNo ratings yet
- REFERAT Koass Neurologi - Carpal Tunnel SyndromeDocument34 pagesREFERAT Koass Neurologi - Carpal Tunnel SyndromeVindhita RatiputriNo ratings yet
- P and C Cont - VdsDocument4 pagesP and C Cont - VdsAchilles YbarraNo ratings yet
- Sensory ExaminationDocument4 pagesSensory ExaminationAthena BorjaNo ratings yet
- AP06 SensesDocument15 pagesAP06 SensesLyn YmiNo ratings yet
- 2012-04-24 FK PainDocument49 pages2012-04-24 FK PainYanis Widhiya NingrumNo ratings yet
- Physiology of Pain: DR M Madhavi LathaDocument23 pagesPhysiology of Pain: DR M Madhavi Lathanico diangeloNo ratings yet
- Pathophysiology of Pressure UlcersDocument1 pagePathophysiology of Pressure UlcersSTORAGE FILENo ratings yet
- 5.3... Screening For Hip, Thigh, Leg PainDocument2 pages5.3... Screening For Hip, Thigh, Leg PainAyesha HabibNo ratings yet
- Acute Scrotal Pain in Adults and Adolescents - Approach To The Patient - DynaMedDocument66 pagesAcute Scrotal Pain in Adults and Adolescents - Approach To The Patient - DynaMedSebastian ChavesNo ratings yet
- W7 CTSDocument4 pagesW7 CTSStevanie SesiliaNo ratings yet
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Used As A Guide in Formulating PT DiagnosisDocument1 pageUsed As A Guide in Formulating PT DiagnosisAlyssa BatasNo ratings yet
- 10 Cardiac PDFDocument11 pages10 Cardiac PDFAlyssa BatasNo ratings yet
- Thesis Proposal For Erc 1bDocument15 pagesThesis Proposal For Erc 1bAlyssa BatasNo ratings yet
- Rheumatoid Arthritis: InflammatoryDocument6 pagesRheumatoid Arthritis: InflammatoryAlyssa BatasNo ratings yet
- Rheumatoid Arthritis: InflammatoryDocument6 pagesRheumatoid Arthritis: InflammatoryAlyssa BatasNo ratings yet
- Painful Hip SyndromesDocument2 pagesPainful Hip SyndromesAlyssa BatasNo ratings yet
- Electromagnetic FieldDocument2 pagesElectromagnetic FieldAlyssa BatasNo ratings yet
- CHAPTER 1: Cardiac Anatomy and PhysiologyDocument7 pagesCHAPTER 1: Cardiac Anatomy and PhysiologyAlyssa BatasNo ratings yet
- Hiv/ Aids: General Medical BackgroundDocument4 pagesHiv/ Aids: General Medical BackgroundAlyssa BatasNo ratings yet
- Superficial Heating ModalitiesDocument3 pagesSuperficial Heating ModalitiesAlyssa BatasNo ratings yet
- Plano de Treino CrossfitDocument8 pagesPlano de Treino Crossfitmari_kundera19No ratings yet
- Electrode Placement ChartDocument34 pagesElectrode Placement ChartFranklin Hall86% (7)
- Geriatric Emt QuizDocument6 pagesGeriatric Emt QuizRebecca Lau0% (1)
- Pain ManagementDocument11 pagesPain Managementenam professorNo ratings yet
- Gap Year, Aurelien SchmittDocument3 pagesGap Year, Aurelien SchmittAurelNo ratings yet
- Effects of Lumbar Stabilization and Muscular Stretchingon Pain, Disabilities, Postural Control and Muscleactivation in Pregnant Woman With Low Back PainDocument10 pagesEffects of Lumbar Stabilization and Muscular Stretchingon Pain, Disabilities, Postural Control and Muscleactivation in Pregnant Woman With Low Back PainVincentius Michael WilliantoNo ratings yet
- Tuning Forks For Healing Therapy by Alan SalesDocument10 pagesTuning Forks For Healing Therapy by Alan SalesMargot Granado100% (4)
- Head INJURIES SruthyDocument27 pagesHead INJURIES SruthySreenath SukumaranNo ratings yet
- Brochure HC Sito IngleseDocument34 pagesBrochure HC Sito Inglesefail mürsəloğluNo ratings yet
- ShaylaDocument3 pagesShaylaapi-530728661No ratings yet
- Potts Disease NCPDocument6 pagesPotts Disease NCPDyanne BautistaNo ratings yet
- Otitis Media NCPDocument3 pagesOtitis Media NCPJames AbendanNo ratings yet
- Pace University End of Life Simulation State 2 Pain ManagementDocument4 pagesPace University End of Life Simulation State 2 Pain Managementapi-414017065No ratings yet
- Euthanasia - Brock CallahanDocument8 pagesEuthanasia - Brock CallahanAzraelDHVRNo ratings yet
- Principles of Balanced AnesthesiaDocument2 pagesPrinciples of Balanced AnesthesiaZahra ZakiyyahNo ratings yet
- 500 Item Free Nursing Board Exam ReviewerDocument149 pages500 Item Free Nursing Board Exam ReviewerMichael Montaño100% (3)
- Health ProblemsDocument3 pagesHealth Problemseduardo orellanaNo ratings yet
- Out of Your Mind and Into Your Life WorkbookDocument28 pagesOut of Your Mind and Into Your Life WorkbookAmy Rowan Hartin100% (9)
- Mirror Therapy - Practical Protocol For Stroke Rehabilitation, 2013Document25 pagesMirror Therapy - Practical Protocol For Stroke Rehabilitation, 2013Nacho Castro Izquierdo75% (4)
- Mr. Emmanuel J. Sombilon: Department of AnesthesiologyDocument3 pagesMr. Emmanuel J. Sombilon: Department of AnesthesiologyPaul Rizel LedesmaNo ratings yet
- SEMINAR On PainDocument36 pagesSEMINAR On PainGuna50% (2)
- Pain Management: Dr. Bambang Rahardjo, DR, Spog-KDocument32 pagesPain Management: Dr. Bambang Rahardjo, DR, Spog-KmeldaNo ratings yet
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 pagesColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care PlanCatherine Joy VillapandoNo ratings yet
- Local AnesthesiaDocument40 pagesLocal AnesthesiaKY HoNo ratings yet
- Psychological Aspect of PainDocument23 pagesPsychological Aspect of PainAndi RifkyNo ratings yet
- Preview 15031 Greene Treatment of TmdsDocument24 pagesPreview 15031 Greene Treatment of TmdsManuel CastilloNo ratings yet
- ELECTROTHERAPYDocument62 pagesELECTROTHERAPYXavier ZamudioNo ratings yet
- Official Lima Allen County Visitors Guide 2012Document47 pagesOfficial Lima Allen County Visitors Guide 2012The Lima News0% (1)
- NCP Post Op PainDocument2 pagesNCP Post Op PainLiz Liwag0% (1)