Professional Documents
Culture Documents
Inspection and Preventif Maintenance Ecri PDF
Inspection and Preventif Maintenance Ecri PDF
Uploaded by
fitri nurOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Inspection and Preventif Maintenance Ecri PDF
Inspection and Preventif Maintenance Ecri PDF
Uploaded by
fitri nurCopyright:
Available Formats
IPM Procedures
Inspection and Preventive Maintenance
Procedures
Procedure No. Procedure No.
Anesthesia Unit Vaporizers . . . . . . . 436-0595 Infant Incubators . . . . . . . . . . . . . 415-0595
Anesthesia Unit Ventilators . . . . . . . 461-0595 Infusion Devices . . . . . . . . . . . . . 416-0595
Anesthesia Units . . . . . . . . . . . . . 400-0595 Intra-Aortic Balloon Pumps . . . . . . . 432-0595
Apnea Monitors . . . . . . . . . . . . . . 420-0595 Isolated Power Systems . . . . . . . . . 439-0595
Argon Surgical Lasers . . . . . . . . . . 462-0595 Laparoscopic Insufflators . . . . . . . . . 466-0595
Aspirators . . . . . . . . . . . . . . . . . 433-0595 Mammography Units . . . . . . . . . . . 467-0595
Autotransfusion Units . . . . . . . . . . 449-0595 Medical Gas/Vacuum Systems . . . . . . 440-0595
Beds, Electric . . . . . . . . . . . . . . . 402-0595 Mobile C-arms . . . . . . . . . . . . . . 463-0595
Blood Pressure Monitors, Electronic Mobile X-ray Units . . . . . . . . . . . . 468-0595
Indirect . . . . . . . . . . . . . . . . . 454-0595 Nd:YAG Surgical Lasers . . . . . . . . . 447-0595
Blood Pressure Monitors, Invasive . . . 434-0595 Oxygen-Air Proportioners . . . . . . . . 444-0595
Blood/Solution Warmers . . . . . . . . . 445-0595 Oxygen Analyzers . . . . . . . . . . . . . 417-0595
Capnometers and Multiple Medical Pacemakers, External Invasive . . . . . 418-0595
Gas Monitors . . . . . . . . . . . . . . 450-0595 Pacemakers, External Noninvasive . . . 460-0595
Carbon Dioxide Surgical Lasers . . . . . 446-0595 Peritoneal Dialysis Units . . . . . . . . . 455-0595
Cardiac Resuscitators . . . . . . . . . . 421-0595 Phototherapy Units . . . . . . . . . . . . 469-0595
Centrifuges . . . . . . . . . . . . . . . . 456-0595 Physical Therapy Ultrasound Units . . . 470-0595
Circulating-Fluid Pumps . . . . . . . . . 412-0595 Pneumatic Tourniquets . . . . . . . . . . 443-0595
Conductive Furniture and Floors . . . . 441-0595 Portable Ventilators . . . . . . . . . . . 471-0595
Critical Care Ventilators . . . . . . . . . 458-0595 Pressure Transducers . . . . . . . . . . 435-0595
Cryosurgical Units . . . . . . . . . . . . 457-0595 Pulmonary Resuscitators,
Defibrillator/Monitors . . . . . . . . . . 408-0595 Gas-Powered . . . . . . . . . . . . . . 448-0595
Defibrillators . . . . . . . . . . . . . . . 407-0595 Pulmonary Resuscitators, Manual . . . . 422-0595
ECG Monitors . . . . . . . . . . . . . . . 409-0595 Pulse Oximeters . . . . . . . . . . . . . 451-0595
Electrical Receptacles . . . . . . . . . . 437-0595 Radiant Warmers . . . . . . . . . . . . . 419-0595
Electrocardiographs . . . . . . . . . . . 410-0595 Radiographic Units, General-Purpose . . 472-0595
Electrosurgical Units . . . . . . . . . . . 411-0595 Radiographic/Fluoroscopic Units,
Frequency-Doubled Nd:YAG General-Purpose . . . . . . . . . . . . 473-0595
Surgical Lasers . . . . . . . . . . . . 464-0595 Smoke Evacuators . . . . . . . . . . . . 452-0595
General Devices . . . . . . . . . . . . . . 438-0595 Sphygmomanometers . . . . . . . . . . . 424-0595
Heart-Lung Bypass Units . . . . . . . . 430-0595 Suction Regulators . . . . . . . . . . . . 459-0595
Heated Humidifiers . . . . . . . . . . . . 431-0595 Temperature Monitors . . . . . . . . . . 425-0595
Hemodialysis Units . . . . . . . . . . . . 413-0595 Traction Units . . . . . . . . . . . . . . . 427-0595
Ho:YAG Surgical Lasers . . . . . . . . . 465-0595 Transcutaneous O2/CO2 Monitors . . . . 453-0595
Hypo/Hyperthermia Units . . . . . . . . 414-0595 Ultrasound Scanners . . . . . . . . . . . 474-0595
257941 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
456-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Procedure/Checklist 436-0595
Anesthesia Unit Vaporizers
Used For:
Anesthesia Unit Vaporizers [10-144]
Also Called: By trade names (e.g., Fluotec 5, Vapor 19.1, Tec 6), which are registered trademarks and should
be used only when referring to the specific devices
Commonly Used In: Operating rooms, emergency rooms, delivery rooms, trauma rooms, and any areas
requiring the administration of an inhalation agent (with anesthesia units)
Scope: Applies to the various anesthesia vaporizers used to deliver a known concentration of vaporized liquid
anesthetic
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval* By Hospital Time Required
Major 6 months months . hours
Minor NA months . hours
* Additional periodic calibration and preventive maintenance is normally required annually or biannually (see
manufacturer’s recommendation). Only qualified personnel trained and experienced in this function should
perform this additional servicing.
Overview smaller stream, which acts as the carrier gas, passes
through the vaporizing chamber containing the anes-
An anesthesia unit vaporizer is used to vaporize a thetic agent and becomes saturated with agent vapor;
liquid anesthetic agent and deliver a controlled the remainder of the gas bypasses this chamber. A
amount to the patient. wick may be used in the vaporizing chamber to provide
increased surface area for efficient evaporation of the
According to the American Society for Testing and
drug and saturation of the carrier gas. The saturated
Materials (ASTM) standard ASTM F1161-88, anesthetic
carrier gas leaves the chamber and mixes with the
agent vaporizers are required to be concentration cali-
bypass gas. One adjustment is made to set the desired
brated (i.e., a calibrated knob controls the output con-
concentration. This adjustment simultaneously bal-
centration). Older vaporizers, such as the Copper
ances the carrier and bypass flows to produce the blend
Kettle and the Vernitrol, do not have a single control
required for the set concentration. The mixture exits
for selecting the concentration of anesthetic vapor.
the vaporizer and is delivered from the anesthesia
Where possible, these units should be removed from
machine as the fresh gas to be inspired by the patient.
service. Contemporary concentration-calibrated va-
porizers are of two types: variable bypass and heated
blender. Evaporation of the liquid agent contained in the
chamber is driven by heat absorbed from the walls of
Conventional (variable-bypass) vaporizers. In a the vaporizer; consequently, when evaporation is oc-
variable-bypass vaporizer, the total background gas curring, the vaporizer and its contents cool. Because
flow that enters the unit is split into two streams. The the equilibrium vapor pressure of an agent changes
009006 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
436-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
pass vaporizer. As a result, the variable-bypass design
was abandoned for desflurane, and Ohmeda developed
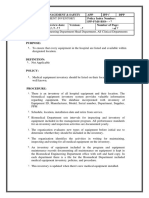
a new vaporizer, the Tec 6, based on a heated-blender
design. Figure 2 shows a schematic of this vaporizer.
A version of the Tec 6 (also manufactured by Oh-
meda) has been adapted for Drager machines and is
compatible with the Drager triple-exclusion interlock
system. As of this writing, neither Drager nor Sie-
mens has developed its own desflurane vaporizer.
A desflurane vaporizer requires electrical power to
heat the agent to a thermostatically controlled 39°C,
producing a stable, saturated vapor pressure of
1,500 mm Hg. No wick is used, and no carrier gas
enters the sump chamber. Instead, a stream of vapor
under pressure flows out of the sump; this stream
blends with the background gas stream, which origi-
nates from the anesthesia machine’s flowmeters, to
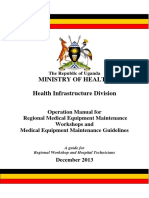
Figure 1. Schematic illustrating the basic elements of a achieve the desired concentration.
vaiable-bypass vaporizer
The background gas stream passes through a fixed-
flow resistor, producing a back pressure upstream of
with temperature, a temperature-sensitive mecha-
this resistor that is proportional to the background gas
nism is used to automatically adjust the carrier and
flow. The desired desflurane concentration is set on the
bypass flows to compensate for temperature changes.
dial of the adjustable metering valve in the vapor
Figure 1 presents a schematic of a variable-bypass
stream; this setting produces a predetermined aper-
vaporizer.
ture. The pressure in the vapor upstream of the aper-
Desflurane (heated-blender) vaporizers. Desflu- ture and the back pressure in the background gas
rane, a volatile inhalation anesthetic marketed by stream are continually sensed by a differential pres-
Ohmeda Pharmaceutical Products Division under the sure transducer. The transducer controls a pressure-
trade name Suprane, has characteristics that differ regulating valve in the vapor stream between the sump
markedly from those currently in use — enflurane, ha-
lothane, and isoflurane; for example, its low solubility
allows rapid induction of and emergence from anesthe-
sia. Thus, by increasing the speed of recovery, desflurane
has the potential to shorten hospital stays (although this
has not yet been consistently demonstrated).
The boiling point of desflurane — 22.9°C at 760 mm
Hg — is just above room temperature; therefore, small
increases in ambient temperature or decreases in atmos-
pheric pressure can cause it to boil. Also, because of
desflurane’s high minimum alveolar concentration, or
MAC (i.e., its low potency), evaporation of sufficient
agent to achieve a given anesthetic effect would require
much more heat absorption from the vaporizer than
occurs with other agents. Furthermore, the change in
vapor pressure of desflurane per change in temperature
is as much as three times that for the other volatile
agents at sea-level atmospheric pressure. These pro-
found effects of temperature and ambient pressure on
the vapor pressure of desflurane make stabilizing the Figure 2. Schematic illustrating the basic elements of the
delivered concentration at a set point extremely difficult Ohmeda Tec 6 vaporizer
in a passive mechanical system, such as a variable-by-
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Anesthesia Unit Vaporizers
and the adjustable metering valve. The pressure-regu- Do not fill a vaporizer with an inhalation agent
lating valve permits only that flow from the sump unless you are qualified to do so. Always use a scav-
necessary to cause the pressure upstream of the ad- enging system or appropriate ventilation when in-
justable metering valve to equal the back pressure in specting vaporizers. For personal safety, when
the background gas stream. In this way, the ratio of inspecting vaporizers alone, notify other personnel of
the adjustable metering valve’s resistance to the resis- your location. Be sure that filler ports are tightly
tance of the fixed-flow resistor determines the ratio of capped before passing gas through the vaporizer.
the flows in each stream, and therefore, the concentra-
tion of vapor in the blended output. If the flow from the Procedure
anesthesia machine’s flowmeters through the vapor- Before beginning an inspection, carefully read this
izer is altered, the flow of vapor from the sump is procedure and the manufacturer’s instruction and serv-
automatically adjusted so that the pressures at the two ice manuals; be sure that you understand how to oper-
monitored points remain equal, the flow ratio does not ate the equipment and the significance of each control
change, and the output concentration continues to and indicator. Also determine whether any special in-
match its setting. spection or preventive maintenance procedures or fre-
The control circuits and heating elements in the quencies are recommended by the manufacturer.
vaporizer are turned on by the act of connecting the Note: This procedure should be done simultaneously
vaporizer to electrical power. The unit then heats to with Anesthesia Units Procedure/Checklist 400,
and remains at operating temperature as long as it where leak testing of the vaporizer has been included
receives power, whether it is delivering agent or is in with the anesthesia unit.
the standby mode. Consequently, it is warm to the
touch while plugged into a live socket. Each vaporizer should have a separate control
number. Inspection documentation for up to three
Citations from Health Devices vaporizers (on one anesthesia unit) can be included on
Avoiding anesthesia mishaps through pre-use checks, one inspection form (record each control number), but
1982 May; 11:210-3. some hospitals may prefer to use a separate form for
each vaporizer.
Water in halothane vaporizers [Hazard], 1985 Aug;
14:326. Be sure that the anesthesia system is level and
secure. Check that all hoses and fittings are tight.
Anesthesia units with a flowmeter-controlled vapor-
izer [Hazard], 1986 Dec; 15:336. 1. Qualitative tests
Vaporizer leak with Mapleson breathing circuits [Haz- 1.1 Chassis/Housing. Examine the exterior of the
ard], 1986 Dec; 15:344-5. unit for cleanliness and general physical condi-
tion. Be sure that housings are intact, that all
Concentration calibrated vaporizers [Hazard], 1987 assembly hardware is present and tight, and
Mar-Apr; 16:112-3. that there are no signs of spilled liquids or other
Pre-use anesthesia check fails to find faults [Hazard], serious abuse.
1988 Sep; 17:274-6. 1.2 Mount/Fasteners. Check security of mounts or
Desflurane (Suprane): Considerations for introduc- support mechanisms. Verify that the vaporizer
ing the new inhalation anesthetic agent into clinical is firmly mounted on the anesthesia unit.
practice [Guidance article], 1994 Apr; 23:131-42. 1.4 AC Plug. If the unit is so equipped, examine the
AC power plug for damage. Attempt to wiggle
Test apparatus and supplies the blades to determine that they are secure.
Halogenated anesthetics analyzer Shake the plug and listen for rattles that could
Hoses and adapters indicate loose screws. If any damage is sus-
pected, open the plug and inspect it.
Special precautions 1.5 Line Cord. Inspect the cord, if so equipped, for
As a general precaution, a vaporizer containing an signs of damage. If damaged, replace the entire
anesthetic agent should not be tipped. If such tipping cord, or if the damage is near one end, cut out the
occurs, notify the user and follow the manufacturer’s defective portion. Be sure to wire a new power cord
recommended procedures for airing or drying the unit. or plug with the same polarity as the old one.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
1.6 Strain Reliefs. Examine the strain reliefs at manual or automatic) against the manufac-
both ends of the line cord, if so equipped. Be sure turer’s specifications. Check that the vaporizer
that they hold the cord securely. interlock allows activation of only one vaporizer
at a time.
1.7 Circuit Breaker/Fuse. If the device has a
switch-type circuit breaker, check that it moves 1.21 Audible Signals. Operate the device in such a
freely. If the device is protected by an external way as to activate any audible signals. Confirm
fuse, check its value and type against that appropriate volume, as well as the operation of
marked on the chassis, and ensure that a spare a volume control, if so equipped.
fuse is provided.
1.22 Labeling. Check that all necessary placards, la-
1.8 Tubes/Hoses. Check the condition of all tubing bels, conversion charts, and instruction cards
and hoses. Be sure that they are not cracked, are present and legible.
kinked, or dirty.
1.24 Site Glass, O-Rings, Keyed Filler Mechanism. Ex-
1.10 Fittings/Connectors. Examine all gas and liq- amine the physical condition of the site glass,
uid fittings and connectors for general condition. O-rings, and keyed filler mechanism, if so
Be sure all fittings are tight. equipped.
1.13 Controls. Before moving any controls, check 2. Quantitative tests
their positions. If any of them appear inordinate
2.1 Grounding Resistance. If the unit is electrically
or are left in the on position, consider the possi-
powered, use an ohmmeter, electrical safety ana-
bility of inappropriate clinical use or of incipient
lyzer, or multimeter with good resolution of frac-
device failure.
tional ohms to measure and record the
Examine all controls for physical condition, resistance between the grounding pin of the
secure mounting, and correct motion. Where a power cord and exposed (unpainted and not ano-
control should operate against fixed-limit stops, dized) metal of the chassis. We recommend a
check for proper alignment, as well as positive maximum of 0.5 Ω
stopping. During the course of the inspection, be
2.2 Leakage Current. For electrically powered
sure to check that each control performs its
units, measure chassis leakage current to the
proper function. Return all controls to the off
chassis of the device with the grounding conduc-
position following the test.
tor of plug-connected equipment temporarily
1.16 Fluid Levels. Check all fluid levels. If the fluid opened. Operate the device in all normal modes,
level is zero, we recommend that you have a including On, Standby, and Off, and record the
qualified user fill the sump with anesthetic maximum leakage current. Leakage current
agent to continue the inspection. should not exceed 300 µA.
1.17 Battery. Inspect the physical condition of the 2.10 Concentration Check. Data for up to three va-
battery and battery connectors, if so equipped porizers can be recorded as Items 2.10, 2.11, and
and readily accessible. Operate the battery-pow- 2.12. Record the type and control number of the
ered functions of the unit for several minutes to vaporizer being tested under each item.
check that the battery has an adequate charge.
2.11 See Item 2.10
Check remaining battery capacity by activating
the battery test function or measuring the out- 2.12 See Item 2.10
put voltage. If it is necessary to replace a battery,
label it with the date. Because there are various types of halogen-
ated anesthetic analyzers, follow the manufac-
1.18 Indicators/Displays. During the course of the turer’s procedure for setup and use of the
inspection, confirm the operation of all indica- analyzer.
tors and visual displays on the unit, if so
equipped. Vaporizers should usually be tested with an
oxygen flow of 4 to 5 L/min (nitrous oxide may
1.20 Alarms/Interlocks. Operate the device in such affect the readings of some vapor analyzers).
a way as to activate each audible and visual Test the vaporizers at low, medium, and high
alarm, if so equipped. If the device has an alarm- concentration settings in the normal clinical use
silence feature, check the method of reset (i.e., range (e.g., 0.5%, 1.0%, and 3.0% for halothane).
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Anesthesia Unit Vaporizers
At one concentration setting (e.g., 1.0% for ha- 3.2 Replace the battery, if so equipped (battery
lothane, 10% for desflurane), test the vaporizer should be replaced at least once annually).
at another flow (e.g., 1 L/min). We recommend
that the concentration be ±0.3% vapor or ±10% 4. Acceptance tests
of the measured value, whichever is greater. If
errors in concentration are observed, allow the Conduct major inspection tests for incoming vapor-
vaporizer to operate for a minute or two and izers and, if a vaporizer is position sensitive, any time
recheck the unit. Some units may require a it is demounted from an anesthesia unit.
short stabilization period.
Before returning to use
3. Preventive maintenance Return all controls to the off position, level and
3.1 Clean the exterior. secure the unit, and tighten all fittings and tubing.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure Checklist 461-0595
Anesthesia Unit Ventilators
Used For:
Anesthesia Unit Ventilators [10-145]
Commonly Used In: Delivery rooms and operating rooms
Scope: Applies to ventilators used to deliver inhalation anesthetic agents during surgical procedures that
require general anesthesia
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 6 months* months . hours
Minor NA months . hours
* Inspection and preventive maintenance intervals should be scheduled according to the manufacturer’s
recommendations. However, units should have a major inspection at least every six months. Pre-use checks
should be performed before each case by the anesthetist who will be operating the equipment.
Overview In general, an anesthesia ventilator is less sophisti-
cated than a critical care ventilator, having only a
Patients undergoing surgery under general anesthesia control mode of operation, with time cycling. (However,
are routinely paralyzed with muscle relaxants to sta- there is at least one ICU-type ventilator that can be
bilize the surgical field. Consequently, they are unable used to administer inhalation anesthetics.) A pressure
to breathe on their own and must be mechanically limit prevents exposure of the lungs to excessive pres-
ventilated either manually by the anesthetist, who sure. Several other breathing waveshape parameters
squeezes a reservoir bag in the breathing circuit, or (e.g., inspiratory:expiratory [I:E] ratio, tidal volume,
automatically by an anesthesia ventilator. A switch minute volume, flow) are settable by the operator and
valve allows the choice of the method by which venti- controlled by the ventilator. Ventilators designed
lation is to be supported. The anesthesia ventilator is solely for anesthetic administration typically do not
typically turned on and off independently of the switch- have compressors.
ing between manual and automatic ventilation.
During extended procedures and procedures involv-
Anesthesia ventilators use positive pressure to in- ing open breathing circuit configurations, a humidifier
flate a patient’s lungs and deliver a prescribed mixture may be included in the breathing circuit. Otherwise, a
of gases and vapors to them. This mixture is produced circle system with an absorber, along with one-way
by the anesthesia machine. The ventilator can be built inspiratory and expiratory valves, is used, typically
into the anesthesia machine or can be a stand-alone without a humidifier. The ventilator’s pressure-relief
unit connected to the machine by gas tubing and, and limit valve(s) should be connected to a waste gas
perhaps, sensor cables. Some anesthesia ventilators scavenging system.
have built-in displays and alarms; others rely on the
sensors, displays, and alarms of the anesthesia ma- Citations from Health Devices
chine to monitor their performance. Anesthesia systems [Evaluation], 1988 Jan; 17:3.
238369 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
461-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Who should service anesthesia equipment [User Expe- use by outside vendors can be produced to ensure that
rience NetworkTM], 1988 Feb; 17:70. those items agreed upon are performed by the vendor.
Barotrauma from anesthesia ventilators [Hazard], The following framework should be supplemented
1988 Nov; 17:354. by the manufacturer’s recommended preventive main-
tenance procedures for mechanical ventilators.
Damage to elastic components from Loctite [Hazard],
1989 Jul-Aug; 18:288. 1. Qualitative tests
Risk of barotrauma and/or lack of ventilation with 1.1 Chassis/Housing. Examine the exterior of the
ventilatorless anesthesia machines [Hazard], 1994 unit for cleanliness and general physical condition.
Jan-Feb; 23:54. Be sure that plastic housings are intact, that all
hardware is present and tight, and that there are
Test apparatus and supplies no signs of spilled liquids or other serious abuse.
Lung simulator with adjustable compliance or ven- 1.2 Mount/Fasteners. Check that ventilators
tilator tester mounted in anesthesia machines are properly
Pressure gauge or meter with 2 cm H2O resolution installed. If the device is mounted on a stand or
from -20 to +120 cm H2O cart, examine the condition of the mount. If it is
attached to a wall or rests on a shelf, check the
Various breathing circuit adapters security of this attachment. Check the mounting
Leakage current meter or electrical safety analyzer security of all components.
Ground resistance ohmmeter 1.3 Casters/Brakes. If the device moves on casters,
Additional items as required for specific manufac- check their condition. Verify that they turn and
turers’ procedures swivel, as appropriate, and look for accumula-
tions of lint and thread around the casters.
Check the operation of brakes and swivel locks,
Procedure if the unit is so equipped.
Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and 1.4 AC Plug. Examine the AC power plug for dam-
service manuals; be sure that you understand how to age, if so equipped. Attempt to wiggle the blades
operate the equipment, the significance of each control to check that they are secure. Shake the plug and
and indicator, and the alarm capabilities. Also deter- listen for rattles that could indicate loose screws.
mine whether any special inspection or preventive If any damage is suspected, open the plug and
maintenance procedures or frequencies are recom- inspect it.
mended by the manufacturer.
1.5 Line Cord. Inspect the cord for signs of damage,
Manufacturers’ recommended procedures for in- if so equipped. If damaged, replace the entire
spection and preventive maintenance of mechanical cord or, if the damage is near one end, cut out the
anesthesia ventilators vary in both methods and re- defective portion. Be sure to wire a new power
quired accuracy. In addition, ventilator controls can cord or plug with the correct polarity. Also check
vary greatly among manufacturers and models. This line cords of battery chargers.
procedure provides the basic framework for complete 1.6 Strain Reliefs. Examine the strain reliefs at
ventilator inspection and preventive maintenance. both ends of the line cord, if so equipped. Be sure
Manufacturers’ recommended procedures should be that they hold the cord securely.
added where appropriate. References to specific pages
of the manufacturer’s manual should be added to the 1.7 Circuit Breaker/Fuse. If the device has a switch-
checklist. (The checklist includes blank spaces for the type circuit breaker, check that it moves freely. If
insertion of these reference numbers.) the device is protected by an external fuse, check
its value and type against that marked on the
IPM Task ManagerTM, the software component of the chassis, and ensure that a spare is provided.
Inspection and Preventive Maintenance System, en-
ables easy production of customized procedures and 1.8 Tubes/Hoses. Check the condition of all tubing
checklists for specific ventilator models and clinical and hoses. Be sure that they are not cracked,
needs. Items performed by outside vendors can be kinked, or dirty. Check that they are connected
excluded from the checklist; a separate checklist for to the correct locations.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Anesthesia Unit Ventilators
1.9 Cables. Inspect any cables (e.g., for sensors) and 1.17 Battery/Charger. Inspect the physical condition
their strain reliefs for general condition. Care- of batteries and battery connectors, if so equipped
fully examine cables to detect breaks in the in- and if readily accessible. Check operation of
sulation and to ensure that they are securely battery-operated power-loss alarms, if so
gripped in the connectors at each end, which will equipped. Operate the unit on battery power for
prevent rotation or other strain. Where appro- several minutes to check that the battery is
priate, verify that there are no intermittent charged and can hold a charge. (The inspection
faults by flexing cables near each end and look- can be carried out on battery power to help
ing for erratic operation or by using an ohmme- confirm adequate battery capacity.) Check bat-
ter. tery condition by activating the battery test func-
tion or measuring the output voltage; for
1.10 Fittings/Connectors. Examine all gas fittings lead-acid batteries, measure the specific gravity
and connectors for general condition. Gas fit- and check the fluid level. Check the condition of
tings should be tight and should not leak. Verify the battery charger and, to the extent possible,
that keyed connectors (e.g., pin-indexed gas con- confirm that it does, in fact, charge the battery.
nectors) are used where appropriate, that all Be sure that the battery is recharged or charging
pins are in place and secure, and that keying is when the inspection is complete. When it is nec-
correct. Connectors to hospital central piped essary to replace a battery, label it with the date.
medical gas systems should have the appropri-
ate DISS or quick-connect fitting to eliminate the 1.18 Indicators/Displays. During the course of the
need for adapters. inspection, confirm the operation of all lights,
indicators, meters, gauges, and visual displays
1.12 Filters. Check the condition of gas filters, if in- on the unit and charger (if so equipped). Be sure
cluded in the unit. Check for corrosion residue that all segments of a digital display function.
indicative of liquid, gaseous, or solid particle Record the reading of an hour meter, if present.
contaminants in the gas supply; if found, notify
1.20 Alarms/Interlocks. Induce alarm conditions to ac-
appropriate personnel. Clean or replace if appro-
tivate audible and visual alarms. Check that any
priate, and indicate this on Lines 3.1 and 3.4 of
associated interlocks function. If the unit has an
the inspection form.
alarm-silence feature, check the method of reset
(i.e., manual, automatic) against the manufac-
1.13 Controls/Switches. Before changing any con-
turer’s specifications. It may not be possible to
trols or alarm limits, check their positions. If any
check out all alarms at this time since some may
settings appear inordinate (e.g., alarm limits at
require special conditions that must be established
the ends of their range), consider the possibility
according to the manufacturer’s recommenda-
of inappropriate clinical use or of incipient device
tions; include these in Item 2.4. Verify that any
failure. Record the settings of those controls that
remote alarm indicator (e.g., within the main-
should be returned to their original positions
frame anesthesia unit) functions properly.
following the inspection.
1.22 Labeling. Check that all necessary placards, la-
Examine all controls and switches for physical bels, and instruction cards are present and legible.
condition, secure mounting, and correct motion.
Check that control knobs have not slipped on 1.23 Accessories. Confirm the presence and condition
their shafts. Where a control should operate of accessories. Check the condition of reusable
against fixed-limit stops, check for proper align- Bain circuit and adapters, if available.
ment, as well as positive stopping. Check mem-
1.24 Bellows. Check the physical condition and
brane switches for damage (e.g., from
proper operation of the bellows.
fingernails, pens). During the inspection, be sure
to check that each control and switch performs 2. Quantitative tests
its proper function.
2.1 Grounding Resistance. Using an ohmmeter, elec-
1.15 Fan. Check physical condition and proper op- trical safety analyzer, or multimeter with good
eration, if so equipped. Clean and lubricate if resolution of fractional ohms, measure and record
required, according to the manufacturer’s in- the resistance between the grounding pin of the
structions, and note this on Lines 3.1 and 3.2 of power cord and exposed (unpainted and not ano-
the form. dized) metal on the chassis of the ventilator or of
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
the system in which the ventilator is mounted. Volume (e.g., tidal volume, minute volume,
We recommend a maximum of 0.5 Ω. If the apnea)
ventilator is a component within an anesthesia Fraction of inspired oxygen (FIO2; see Oxygen
unit, grounding and leakage current measure- Analyzers Procedure/Checklist 417)
ments can be referenced to that unit.
Alarm settings (e.g., high PIP, low MAP, low
2.2 Leakage Current. Measure chassis leakage cur- pressure, low FIO2) should be inspected for
rent to ground with the grounding conductor of proper and accurate activation.
plug-connected equipment temporarily opened.
Operate the device in all normal modes, includ- 2.5 Gas Supply.
ing on, standby, and off, and record the maxi-
Pneumatic lines (including air filters). Verify
mum leakage current.
that appropriate gas-specific connectors are
Measure chassis leakage current with all ac- used. Check gas filters, if so equipped and
cessories normally powered from the same line accessible.
cord connected and turned on and off. This in- Gas cylinders (and gauges and regulators, if so
cludes other equipment that is plugged into the equipped). Verify that these are present, se-
primary device’s accessory receptacles, as well as curely mounted, and in good condition and
equipment plugged into a multiple-outlet strip that there is an adequate gas supply. Verify
(“Waber strip”) so that all are grounded through that one and only one washer is used to seal
a single line or extension cord. the tank to its yoke. Verify that all index pins
Chassis leakage current to ground should not are present and protruding to the proper
exceed 300 µA. length to engage the hole in the tank valve
stem and in the correct positions for the gas to
2.3 Modes and Settings. Anesthesia ventilators are be supplied through the yoke.
usually equipped only with a control mode. How-
ever, specialized units may have additional 2.6 Patient Circuit.
modes such as assist/control and pressure sup- Breathing circuit (including filters). Verify that
port. Adjustable positive end-expiratory pres- these components are compatible with the ven-
sure (PEEP) may also be available. The function tilator according to the manufacturer’s recom-
of these modes should be inspected and verified mendations (see Health Devices 1988 Apr;
for proper operation. Check the operation and 17:109). Check for leaks, the absence of obstruc-
accuracy of ventilation controls, which may in- tions, and proper flow direction in the breathing
clude tidal volume, breath rate, inspiratory time, circuit, ensuring the proper assembly and func-
expiratory time, I:E ratio, pressure limit, or flow. tion of fittings, adapters, the CO2 absorber, in-
Typically, these tests are performed by attaching spiratory and expiratory valves and PEEP
the ventilator to a lung simulator or ventilator valves, the APL valve, the scavenger, and other
tester and comparing measured values to set- components. With the ventilator connected to
tings on the ventilator. The manufacturer should the anesthesia system, check for leaks in the
recommend the appropriate ventilator settings entire system, including the breathing circuit.
(e.g., tidal volume, rate, inspiratory time) to ver- This does not have to be duplicated if done as
ify proper operation and accuracy (generally part of the Anesthesia Units procedure (see
within 10%). Procedure/Checklist 400).
2.4 Monitors and Alarms. The following breathing Humidifiers. See Heated Humidifiers Proce-
circuit parameters may be monitored by the ven- dure/Checklist 431.
tilator or by the system in which the ventilator
is mounted. They should be inspected for accu- Pressure-Relief Mechanism. Check the proper
racy (generally within 10%) according to the operation of the pressure-relief mechanism by
manufacturer’s specifications: occluding the breathing circuit and measuring
the resulting peak pressure on the pressure
Breathing rate gauge. Verify that pressure is vented in the
Inspiratory time breathing circuit.
Airway pressure (e.g., PIP, PEEP, MAP, ap- Absorber. See Anesthesia Units Proce-
nea) dure/Checklist 400.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Anesthesia Unit Ventilators
3. Preventive maintenance Before returning to use
3.1 Clean the exterior and interior, if needed. Ensure that all controls are set properly. Set alarms
loud enough to alert personnel in the area in which the
3.3 Calibrate according to manufacturer’s instructions.
device will be used. Other controls should be in their
3.4 Replace components according to the manufac- normal pre-use positions.
turer’s instructions.
Attach a Caution tag in a prominent position so that
4. Acceptance tests the user will be aware that control settings may have
been changed.
Conduct major inspection tests for this procedure
and the appropriate tests in the General Devices Pro- Recharge battery-powered devices, or equip them
cedure/Checklist 438. with fresh batteries, if needed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 400-0595
Anesthesia Units
Used For:
Anesthesia Units [10-134]
Also Called: Anesthesia machines, anesthesia workstations
Commonly Used In: Operating rooms, emergency departments, trauma rooms, delivery rooms, any areas
where anesthetic agents are used
Scope: Applies to anesthesia units; includes leak testing of vaporizers and should be used in conjunction with
Anesthesia Unit Vaporizers Procedure/Checklist 436 (in the very rare case where an anesthesia unit may still
use flammable anesthetic agents, refer to Conductive Furniture and Floors Procedure/Form 441); does not
apply to oxygen monitors with an alarm, spirometers, other monitors, or ventilators that might be part of the
breathing system (see Anesthesia Unit Ventilators Procedure/Checklist 461)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 6 months months . hours
Minor NA months . hours
Overview a health hazard to chronically exposed OR personnel
and unborn children. Inadvertent switching of gas
Most surgical procedures are performed while the pa- supplies, failure of an alarm to respond to an exces-
tient is under general anesthesia. Usually, the patient sively low oxygen pressure, and misconnected or im-
is anesthetized by a narcotic or barbiturate injection properly calibrated flowmeters have also caused
followed by administration of an inspired gas mixture anesthesia-related accidents.
of oxygen, nitrous oxide, and the vapor of a volatile
Because mishandling and mistakes can have severe
liquid anesthetic, typically a halogenated hydrocar-
consequences, life-support devices such as anesthesia
bon. The anesthesia unit administers this mixture of
units should be operated and inspected only by quali-
anesthetic gases and life-sustaining oxygen, varying
fied personnel who have a thorough knowledge of the
the proportions to control the patient’s level of con-
units and their functions. If you are unsure of any
sciousness. If respiratory assist is necessary (e.g., in
aspect of the procedure, consult the manufacturer be-
cases of muscular blockade), a ventilator may be con-
fore inspecting an anesthesia unit.
nected to the patient breathing system to force the gas
mixture into the patient’s lungs. The anesthesia unit consists of four systems: the gas
supply system, the gas control system, the vaporizers,
Improperly modified or inadequately maintained and the breathing system.
anesthesia units have injured and killed patients
and hospital personnel. Gas leaks can adversely Gas supply. This system delivers a variety of gases
affect the accuracy of gas delivery to the patient, as to the patient. Cylinders containing oxygen and other
well as add anesthetic agents to the OR atmosphere. gases at high pressure (see Table 1) are connected to
Trace levels of anesthetics have been implicated as the high-pressure system of the anesthesia unit by
009005 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
400-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
TABLE 1. Gases Used in Anesthesia Machines
Gas Chemical Color Code: Color Code: Service Pressure,
Formula U.S. International psi 21°C, Full Cylinder
Oxygen O2 Green White 1,800-2,400*
Carbon Dioxide CO2 Gray Gray 838
Nitrous Oxide N2O Blue Blue 745
Helium He Brown Brown 1,600-2,000*
Air Yellow White and Black 1,800
* Depends on cylinder size.
yoke fittings that comply with the Compressed Gas normally attached to the anesthesia unit as a reserve
Association (CGA) pin-index safety system (see Figure source if the central supply fails or if central supply
1). Unique placements of pins and mating holes on the outlets are not available.
pin-index fittings prevent connection of a gas cylinder
to the wrong inlet. Inside the unit, each high-pressure Centrally supplied gases are delivered directly to the
gas flows through a filter, a check valve (for one-way intermediate-pressure gas control system at approxi-
flow), and a regulator that reduces the pressure to mately 50 psi through low-pressure hoses and connec-
approximately 45 psi. tors. These connectors may not comply with a universal
standard safety system, but each is designed to prevent
Because oxygen and nitrous oxide are used in rela- mismating the gas supply and the machine inlet.
tively large quantities, they are usually drawn from
the hospital’s central gas supplies, which are more Some units may provide an oxygen power outlet to
convenient and economical than compressed-gas cyl- drive auxiliary devices (e.g., a ventilator).
inders. However, cylinders of these gases are also Gas control. This system regulates gas flow rates so
that the gases can be mixed and delivered under accu-
rate, constantly metered control. The operator must
be able to adjust the ratios or make rapid gross changes
in flow rates without inducing system interactions that
cause temporary delivery of undesirable mixtures.
The flow of each gas is controlled by a valve and
indicated by a glass-tube flowmeter. After gases pass
the control valve and enter the low-pressure system,
they can be administered to the patient.
A fail-safe provision in many anesthesia units pro-
tects the patient against a fall in pressure of life-sus-
taining oxygen. If the oxygen pressure drops below
about 25 to 30 psi, some units shut off the flow of all
other gases, while others reduce all gas flow rates in
proportion to the drop in oxygen pressure. Newer
anesthesia machines have additional safety systems
that provide a minimum percent of oxygen (around
25%) and/or deliver a minimum flow of oxygen (usually
CGA Connector 150 to 250 mL/min) (see Item 2.11).
Gas Index Pins Number
Oxygen 2-5 870 Vaporizers. These devices add the vapor of a volatile
Nitrous Oxide 3-5 910 liquid anesthetic (e.g., halothane, isoflurane, enflurane,
O2 - CO2 (CO2<7%) 2-6 880
O2 - CO2 (CO2>7%) 1-6 940 sevoflurane, desflurane) to the gas mixture, when de-
O2 - HE (He > 80%) 4-6 930 sired, and aid in controlling the vapor concentration.
O2 - HE (He < 80%) 2-4 890
Air 1-5 950 According to the American Society for Testing and
Materials (ASTM) standard ASTM F1161-88, anes-
Figure 1. Pin-index safety system thetic agent vaporizers are required to be concentra-
tion calibrated (i.e., a calibrated knob controls the
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Anesthesia Units
output concentration). Older vaporizers, such as the patient who cannot breathe spontaneously, as well as
Copper Kettle and the Vernitrol, do not have a single positive end-expiratory pressure (PEEP), if required.
control for selecting the concentration of anesthetic The breathing system typically includes a scavenging
vapor. Where possible, these units should be removed system to remove waste gases.
from service. Contemporary concentration-calibrated
vaporizers are of two types: variable bypass and heated Two types of breathing systems are used to deliver
blender. the anesthetic mixture from the unit to the patient,
although they may assume a variety of configurations.
The variable-bypass (conventional) vaporizer is
used for most volatile agents (e.g., halothane, isoflu- The T-piece or open system may be a nonrebreath-
rane, enflurane, sevoflurane). The total background ing system consisting of a reservoir bag and a gas-de-
gas flow that enters the unit is split into two streams. livery hose connected through a nonrebreathing
The smaller stream, which acts as the carrier gas, (one-way) valve to the face mask or endotracheal tube.
passes through the vaporizing chamber containing the The patient breathes the anesthetic mixture directly
anesthetic agent and becomes saturated with agent from the machine, and exhaled gas is vented out of the
vapor; the remainder of the gas bypasses this chamber. system. T-piece systems that do not include the nonre-
A wick may be used in the vaporizing chamber to breathing valve may allow partial rebreathing, de-
provide increased surface area for efficient evapora- pending on the inflow of fresh gas.
tion of the drug and saturation of the carrier gas. The
The circle or closed system is a continuous loop in
saturated carrier gas leaves the chamber and mixes
which check valves allow gas to flow in only one direc-
with the bypass gas. One adjustment is made to set the
tion. The patient inhales from and exhales into the
desired concentration. This adjustment simultane-
system. Fresh gases from the anesthesia machine
ously balances the carrier and bypass flows to produce
enter at one point, mix with previously exhaled gases,
the blend required for the set concentration. The mix-
and pass to the patient, who inhales the mixture.
ture exits the vaporizer and is delivered from the
Newly exhaled gases are channeled to a carbon dioxide
anesthesia machine as the fresh gas to be inspired by
absorber, which removes almost all the carbon dioxide
the patient.
produced by body metabolism and routes the scrubbed
A heated-blender vaporizer is used only for desflu- gases back toward the patient. En route, the scrubbed
rane. It requires electrical power to heat the agent gases become mixed with fresh machine gases.
to a thermostatically controlled 39°C, producing a
A scavenging system should be included to remove
stable, saturated vapor pressure of 1,500 mm Hg. No
waste gas from the vent port of a T-piece breathing
wick is used, and no carrier gas enters the sump
system or from the adjustable pressure-limiting (APL)
chamber. Instead, a stream of vapor under pressure
valve and relief valve of a ventilator of a circle system
flows out of the sump; this stream blends with the
to reduce the quantity of gas that escapes into the
background gas stream, which originates from the
operating room. Such a scavenging system is neces-
anesthesia machine’s flowmeters, to achieve the de-
sary because trace levels of anesthetics are believed to
sired concentration.
cause an increased incidence of spontaneous abortion,
(Desflurane, a volatile inhalation anesthetic mar- congenital anomalies in offspring, and neoplastic dis-
keted by Ohmeda Pharmaceutical Products Division ease and may affect the mental and physical abilities
under the trade name Suprane, and sevoflurane, of exposed personnel. The breathing system should be
marketed by Abbott under the trade name Ultane, checked before each use for leaking gases. It is also
have characteristics that differ markedly from those recommended that the concentration of waste anes-
currently in use — enflurane, halothane, and isoflu- thetic gas in the operating room be surveyed quarterly.
rane. For example, their low solubilities allow rapid The scavenging system must include pressure-relief
induction of and emergence from anesthesia. Thus, mechanisms so that abnormal pressures cannot de-
by increasing the speed of recovery, desflurane and velop in the scavenging system and interfere with
sevoflurane have the potential to shorten hospital operation of the breathing system.
stays, although this has not yet been consistently
demonstrated.) Anesthesia units either come with physiological
monitors integrated into the unit or provide shelving
Breathing system. Although it is designed primar- to support such monitors. Most also provide mounting
ily for sustained, efficient gas delivery to the patient, for a suction regulator and canister and other accesso-
the breathing system may also remove carbon dioxide ries, along with storage for drugs, supplies, and related
and provide mechanical or manual ventilation of a paraphernalia.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
Citations from Health Devices have a minimum pressure of 745 psi for nitrous
oxide and 1,000 psi for oxygen
Anesthesia units with a flowmeter-controlled vapor-
izer [Hazard], 1986 Dec; 15:336-7. Nondisposable corrugated breathing hose (dispos-
able tubing may not provide reliable connections)
Vaporizer leak with Mapleson breathing systems
Test lung (reservoir bag with 3 or 5 L capacity)
[Hazard], 1986 Dec; 15:344-5.
Sphygmomanometer bulb with tubing and adapter
Concentration calibrated vaporizers [Hazard], 1987
Leak-detecting solution
Mar-Apr; 16:112-3.
Conductive lubricant for conductive casters (e.g.,
Pre-use testing prevents “helpful” reconstruction of Dow No. 41, graphited oil)
anesthesia components [Hazard], 1987 May;
16:178-9. Trichloroethylene cleaning solvent or solvent rec-
ommended by the manufacturer (be sure to review
Anesthesia systems [Evaluation], 1988 Jan; 17:3-34. the manufacturer’s Material Safety Data Sheet and
see the special precautions below)
Who should service anesthesia equipment [User Expe-
rience NetworkTM], 1988 Feb; 17:70-1. Lubricant as specified by manufacturer
Pre-use anesthesia check fails to find faults [Hazard], Special precautions
1988 Sep; 17:274-6. (Contains pre-use checklist for
ECRI is aware of a number of incidents in which
anesthesia units.)
improperly serviced ventilation or anesthesia equip-
Anesthesia systems [Evaluation Update], 1988 Dec; ment was implicated in patient injury or death. Do not
17:366-7. perform any procedures, adjustments, repairs, or
modifications unless you thoroughly understand the
Anesthesia units and breathing systems [Standard], device and have verified the appropriateness of the
1989 Oct; 18:363. intended actions. Resolve any questions or uncertain-
Monitoring and anesthesia systems: integration and a ties with the manufacturer, the anesthetist, or ECRI
new option, 1991 Mar-Apr; 20:131-2. before placing a unit into use.
Use of inadequate (old) anesthesia scavenger inter- To avoid the adverse effects of exposure to anes-
faces [Hazard], 1993 Dec; 22:592. thetic gases, all testing should be done with an operat-
ing scavenging system in place or an alternative means
Anesthesia systems [Evaluation]. To be published in to vent excess gases from the vicinity of inspecting
1996. personnel. If a flammable anesthetic is used, be sure
all traces of the gas are cleared away before performing
Test apparatus and supplies any electrical tests. Check that all valves, including
Pressure gauge or meter, -10 to +80 cm H2O (accu- the gas cylinder stem valves, are turned off at the
racy ±5 cm H2O at 30 cm H2O) beginning of the inspection. Turn all valves off again
when the inspection is complete.
Flowmeters with ranges of approximately 0.1 to 1.0
L/min and 1 to 10 L/min, ±2% accuracy, calibrated When testing cyclopropane flowmeters, observe
separately for each of the gases used with the anes- noted procedures to avoid a buildup of explosive levels
thesia machine, and one flowmeter for 10 to 100 of cyclopropane.
L/min (±10% of reading)
Trichloroethylene is a common solvent particularly
Stopwatch or watch with a second hand recommended for cleaning oxygen fittings because it
Hoses and adapters for connecting pressure gauges does not leave a residue that is flammable in high-con-
or meters and flowmeters to equipment being in- centration oxygen. However, this solvent reacts with
spected the soda lime used in carbon dioxide absorbers to form
several poisonous gases, including phosgene. Al-
Cylinder of each type of gas used with the unit though concentrations may not be lethal, the presence
being inspected; each cylinder on a unit that is of these gases to any degree is highly undesirable.
ready for use should be more than half full if the
gas is normally stored in gaseous form (e.g., oxy- To prevent the generation of these gases, make sure
gen) and should contain some liquid if the gas is that equipment recently cleaned with trichlo-
normally liquefied for storage; cylinders should roethylene is completely dry before using. When clean-
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Anesthesia Units
ing parts of the anesthesia unit with this solvent, first 1.6 Strain Reliefs. Examine the strain reliefs at
disconnect the line to the carbon dioxide absorber. both ends of the line cord. Be sure that they hold
After cleaning, allow time for the solvent to evaporate. the cord securely.
When the parts appear dry, take the added precaution
of briefly flushing them with a high oxygen flow rate. 1.7 Circuit Breaker/Fuse. If the device has a
switch-type circuit breaker, check that it moves
Procedure freely. If the device is protected by an external
fuse, check its value and type against that
Before beginning an inspection, carefully read this marked on the chassis, and ensure that a spare
procedure and the manufacturer’s instruction and is provided.
service manuals; be sure that you understand how to
operate the equipment, the significance of each control 1.8 Tubes/Hoses. Check the condition of all tubing
and indicator, and the alarm capabilities. Also deter- and hoses. Be sure that they are not cracked,
mine whether any special inspection or preventive kinked, or dirty.
maintenance procedures or frequencies are recom-
mended by the manufacturer. 1.9 Cables. Inspect the cables (e.g., sensor, elec-
trode) and their strain reliefs for general condi-
1. Qualitative tests tion. Examine cables carefully to detect breaks
1.1 Chassis/Housing. Examine the exterior of the in the insulation and to ensure that they are
unit for cleanliness and general physical condi- gripped securely in the connectors of each end to
tion. Be sure that plastic housings are intact, prevent rotation or other strain.
that all assembly hardware is present and tight,
1.10 Fittings/Connectors. Examine all gas and liq-
and that there are no signs of spilled liquids or
uid fittings and connectors, as well as all electri-
other serious abuse.
cal cable connectors and sockets, for general
1.2 Mount. Check any shelves, brackets, or sup- condition. Electrical contact pins or surfaces
porting structures. Check the security of the should be straight, clean, and bright. Check that
attachments. pins used with the pin-index safety system com-
ply (location and length of protrusion) and are
1.3 Casters/Brakes. If the device moves on casters, intact. Check the yoke clamping screw and
check their condition. Look for accumulations of make sure empty yokes have plugs. Check that
lint and thread around the casters, and be sure appropriate keyed or indexed fittings are being
that they turn and swivel as appropriate. Check used with corresponding gases.
the operation of brakes and swivel locks, if the
unit is so equipped. Check that gas hoses do not 1.12 Filters. Check the condition of all compressed-
lie on the floor or loop near the casters. gas filters. Clean or replace as needed, and indi-
cate this on Line 3.1 or 3.4 of the inspection form.
1.4 AC Plug/Receptacles. Examine the AC power
plug for damage. Attempt to wiggle the blades 1.13 Controls/Switches. Before moving any controls
to determine that they are secure. Shake the and alarm limits, check their positions. If any of
plug and listen for rattles that could indicate them appear inordinate (e.g., a pressure alarm
loose screws. If any damage is suspected, open control at maximum, alarm limits at the ends of
the plug and inspect it. their range), consider the possibility of inappro-
If the device has electrical receptacles for ac- priate clinical use or of incipient device failure.
cessories, insert an AC plug into each and check Record the settings of those controls that should
that it is held firmly. If accessories are plugged be returned to their original positions following
and unplugged often, consider a full inspection the inspection.
of the receptacle.
Examine all controls and switches for physical
1.5 Line Cord. Inspect the cord for signs of damage. condition, secure mounting, and correct motion.
If damaged, replace the entire cord or, if the Where a control should operate against fixed-
damage is near one end, cut out the defective limit stops, check for proper alignment, as well
portion. Be sure to wire a new power cord or plug as positive stopping. During the course of the
with the correct polarity. Also check line cords of inspection, be sure to check that each control and
battery chargers. switch performs its proper function.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
Check that the concentration dial on each of pressure on the pressure gauge. Watch for any
vaporizer moves freely and that only one vapor- inflation of the flattened bag as a sign of expira-
izer can be on at a time. Observe the float motion tory valve leakage.
as its flow control valve is turned on. The valve
should turn smoothly with only slight drag. Reconnect the bag to the bag mount and the
Each valve should have a definite shutoff posi- hose to the inhalation port. With your hand oc-
tion at which the float should be motionless at cluding the expiratory port, use a test lung to
its zero level. Check for free play in the control again generate about 5 cm H2O of pressure and
valve by pushing, pulling, and gently rocking the check for inspiratory valve leakage by watching
stem from side to side without rotation. The stem for any inflation of the bag.
should feel firm, and the flowmeter float should 1.20 Alarms/Interlocks. Operate the device in such a
not move. The control valve knob should require way as to activate each audible and visual alarm.
turning through at least 90° to change the flow Check that any associated interlocks function
rate from 10% to 100% of full scale. (Note: All (particularly the vaporizer interlocks, which
recent anesthesia units should now have differ- should allow activation of only one vaporizer at a
ent sized and shaped knobs for oxygen and ni- time). If the device has an alarm-silence feature,
trous oxide to aid in differentiating between the check the method of reset (i.e., manual or auto-
two controls.) matic) against the manufacturer’s specifications.
1.17 Battery/Charger. Inspect the physical condi- 1.21 Audible Signals. Operate the device in such a
tion of batteries and battery connectors, if read- way as to activate all audible signals. Confirm
ily accessible. Check the battery-operated appropriate volume, as well as the operation of
power-loss alarms on AC and pneumatic devices, a volume control, if so equipped. Check that the
if so equipped. Operate the unit on battery power audible signals are appropriate for the test con-
for several minutes to check that the battery has ditions used.
an adequate charge. Check remaining battery
capacity by activating battery test function or 1.22 Labeling. Check that all necessary placards, la-
measuring the output voltage. If appropriate, bels, conversion charts, and instruction cards
check the condition of the battery charger and, are present and legible. Check for proper color
to the extent possible, confirm that it does, in coding for corresponding parts (e.g., green for
fact, charge the battery. When it is necessary to oxygen, blue for nitrous oxide).
replace a battery, label it with the date.
1.23 Accessories. Verify accuracy and function of any
1.18 Indicators/Displays. During the course of the accessories (e.g., spirometer, sphygmomanome-
inspection, confirm the operation of all lights, ter gauge). (Inspect ventilators, vaporizers, and
indicators, meters, gauges, and visual displays oxygen monitors separately using the appropri-
on the unit and charger, if so equipped. Be sure ate procedures, and record on separate forms.)
that all segments of a digital display function.
1.24 Fail-Safe Oxygen Valves and Alarms. Close all
1.19 Directional Valves. Check that directional control valves. Open all cylinder stem valves
valves are free from cracks and chips and fit and external gas source valves. Connect gas
smoothly against the valve seats. Check for free scavenging or other evacuation system to com-
movement by shaking or lightly squeezing the mon gas outlet. Turn on the main gas control,
hose connecting the two valves. The valves and open the flow control valves until the flow-
should flutter up and down and should not stick meter for each gas reads midscale. Then discon-
to their seats. nect or turn off all oxygen sources. The flow of
other gases should fall or stop as the oxygen flow
Check for the possibility of reverse flow decreases to half its previous level. All gas flow
through directional valves by removing the should cease when the oxygen flow reaches zero.
breathing hoses from the absorber and attach- (Cyclopropane flow rate normally falls more
ing a thin disposable reservoir bag to the exha- slowly than the others.)
lation port. Attach a piece of hose to the bag
mount, set the control for manual mode, close In addition to the automatic shutoff or reduc-
the APL valve, and occlude the inspiratory port tion of gas flow, audible or visual alarms signify-
with the palm of your hand. Then, connect a test ing low oxygen pressure should have been
lung to the hose and generate about 5 cm H2O activated, if the unit is so equipped. Silence the
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Anesthesia Units
alarm by raising the oxygen pressure above the Measure chassis leakage current with all ac-
preset alarm limit. If the unit has an alarm that cessories normally powered from the same line
does not respond, check for exhausted batteries cord connected and turned on and off. This in-
or other source of the malfunction. cludes other equipment that is plugged into the
primary device’s accessory receptacles, as well as
1.25 Common Outlet Back-Pressure Check Valve. equipment plugged into a multiple-outlet strip
Most anesthesia units manufactured after 1968 (“Waber strip”) so that all are grounded through
with mounted bubble-through vaporizers have a a single line or extension cord.
check valve in the gas delivery system to prevent
pressures at the outlet (e.g., produced by a ven- Leakage current should not exceed 300 µA.
tilator) from being transmitted to other parts of
2.3 Oxygen Flush Valve. Attach the 100 L/min flow-
the unit where they could affect the accuracy of
meter to the common outlet. Set the oxygen flow
gas delivery and the concentration of anesthetic
rate to a 2 L/min indication on the machine’s
gases.
oxygen flowmeter and actuate the oxygen flush
To test this check valve, attach the -10 to +80 control. The rate should rise to between 35 and
cm H2O pressure gauge or meter to the common 75 L/min. The machine flowmeter indication
gas outlet. Turn off all vaporizers, either filled should remain near 2 L/min unless the manufac-
or empty. Adjust the oxygen flow control valve to turer’s specification shows otherwise. If it falls
maintain an outlet pressure of 30 cm H2O. Turn more than 1 L/min, check for an inadequate
on the vaporizer flow, and readjust, if necessary, oxygen supply, a partially occluded oxygen line
to maintain 30 cm H2O. Carefully open the in the machine, or a dirty oxygen inlet filter.
vaporizer filler cap (to prevent a sudden flow of Cycle the flush control slowly several times; it
oxygen into the vaporizer) and observe the outlet should move smoothly and not have a tendency
gauge pressure. A sudden pressure drop sug- to stick. Check that the oxygen flow returns to
gests a leaky check valve. If the check valve is 2 L/min within 2 sec each time the flush valve is
missing or defective, replace it or alert appropri- closed.
ate personnel to replace the valve to avoid a
possible hazardous buildup of vapor. Note: This 2.4 High-Pressure Leaks. Close all flow control
test may not be possible on newer machines that valves on the machine. Open all cylinder stem
always maintain a minimum flow of oxygen. On valves one full turn, noting any motion of the
such devices, follow the manufacturer’s instruc- flowmeter floats. Float movement indicates a
tions for testing the common outlet back-pres- leaky flowmeter valve. Record pressure gauge or
sure check valve. meter readings, verifying that they are close to
the service pressure values listed in Table 1.
2. Quantitative tests Close the cylinder stem valves. The pressure
drop over 30 sec should be negligible. Excess
2.1 Grounding Resistance. Use an ohmmeter, elec- pressure drop indicates an unacceptable leak
trical safety analyzer, or multimeter with good that should be located and repaired.
resolution of fractional ohms to measure and
record the resistance between the grounding pin 2.5 Intermediate Pressure System. Close all flow
of the power cord and exposed (unpainted and control valves on the anesthesia unit. Connect
not anodized) metal on the chassis. We recom- the hoses to the external pipeline gas source and
mend a maximum of 0.5 Ω. test the supply line hoses with leak-detecting
solution. Note the pressure on the pipeline/cen-
If the device has an accessory outlet, check its tral gas supply pressure gauge. (Most machines
grounding to the main power cord. should have such a gauge. If not, contact the
manufacturer for instructions for testing the in-
2.2 Leakage Current. Measure chassis and patient
termediate pressure system.) Disconnect the gas
lead leakage current to the chassis of the device
supply line hose from the machine, and check
with the grounding conductor of plug-connected
that the pressure drop in 30 sec is negligible.
equipment temporarily opened. Operate the de-
Excessive pressure drop indicates an unaccept-
vice in all normal modes, including on, standby,
able leak that should be located and repaired.
and off, with all monitors and accessories con-
nected to the unit’s accessory power receptacle(s), 2.6 Low-Pressure Leaks. Attach the -10 to +80 cm
and record the maximum leakage current. H2O pressure gauge or meter to the unit’s common
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
gas outlet and pressurize the outlet section, in- steady 30 cm H2O, indicated on both the test
cluding vaporizers, to approximately 30 cm H2O gauge or meter and the pressure gauge in the
by opening the oxygen flow control valve slightly breathing system, and verify that both gauges
(this is about three times the average working have the same readings. The oxygen flow rate
pressure). Now reduce the flow rate to 30 should be less than 150 mL/min above the leak
mL/min. (Connect a flowmeter to the common measured in Item 2.6.
gas outlet if necessary.) If the gauge or meter
pressure continues to rise, the leak rate is less For anesthesia systems with minimum oxy-
than 30 mL/min at 30 cm H2O (10 mL/min at 10 gen flow, turn the anesthesia machine off and
cm H2O), which is acceptable. If the pressure connect the -10 to +80 cm H2O pressure gauge or
falls, the leakage rate is excessive. Locate the meter to a piece of breathing system tubing that
leak by shutting off all vaporizers and repeating is connected to the inspiratory and expiratory
the test with each vaporizer added in turn. valve outlets. Close the APL valve. Remove the
manual reservoir bag. In its place, connect a
For anesthesia units for which low flow rates stopper with a fitting for a sphygmomanometer
cannot be generated (units that deliver mini- squeeze bulb. Use the bulb to pressurize the
mum flows of oxygen), the low-pressure system breathing system to 50 cm H2O. It should take
can be tested in combination with the breathing at least 30 sec for the pressure to drop from 50
system. Connect the -10 to +80 cm H2O pressure to 30 cm H2O. Less time indicates a leak in the
gauge or meter to a piece of breathing system breathing system that should be corrected.
tubing that is connected to the inspiratory and
expiratory valve outlets. Occlude the outlet to Open the moisture-relief valve. (Note: Due to
the manual reservoir bag and close the APL dust and moisture, some of these valves on older
valve. Turn on the minimum flow of oxygen. units will not turn and might break when force
The pressure gauge or meter should read at least is applied.) The pressure should drop immedi-
30 cm H2O. A reading of less than 30 indicates ately. If the pressure does not drop, clean the
an unacceptable leak that should be corrected. valve of dried soda lime, repeat the pressuriza-
Proceed to Item 2.7 to identify whether the tion, and open the relief valve again.
breathing system is the major source of the leak. 2.8 APL Valve. Leave the setup as in Item 2.7 but
Alternatively, follow the manufacturer’s recom- remove the pressure gauge or meter, replacing it
mendations for testing for low-pressure leaks. with the breathing bag, and restore the normal
2.7 Breathing System. Check the carbon dioxide ab- pressure-limiting valve setting.
sorber housing for cracks or broken edges in the If the APL valve is not the bleeding type,
glass or plastic canister and in the check valve squeeze the bag and verify that the valve holds
domes. pressure until a specific level is exceeded, and
Remove the canister from its holder, without that it then opens. Check that the opening pres-
inverting it, and inspect the gaskets for any sure is adjustable from approximately 1 to at
absorbent dust and wear. Remove any dust from least 30 cm H2O. Other valves, such as the
the bottom of the absorber. If the amount of dust Georgia and Drager valves, may operate in a
seems excessive or if the canister appears seri- completely different manner and at a higher
ously pitted, check for dust in the inspiratory pressure and should be tested according to the
valve and piping, and report the condition to manufacturer’s specified procedure.
department personnel. 2.9 Scavenging System. Insert the pressure gauge or
Check the absorber-elevating mechanism and meter between the APL valve or exhaust port and
clamps for proper operation. the scavenging system intake. Leave the setup as
in Item 2.8, with the APL valve closed or in its
For anesthesia systems without minimum minimum-flow condition. With the scavenging
oxygen flows, connect a breathing hose from the system operating at maximum suction, the pres-
patient inspiration valve to the patient expiration sure gauge or meter reading should be between
valve of the absorber. Close the pressure-limit- -0.5 and 0 cm H2O. Partially open the APL valve,
ing valve. Remove the reservoir bag, and replace and set a 10 L/min oxygen flow rate. With the
it with a -10 to +80 cm H2O pressure gauge or scavenging system at the minimum vacuum, the
meter. Pressurize the system with oxygen to a gauge reading should be near ambient.
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Anesthesia Units
Repeat the last measurement with the APL stipulated by the manufacturer (usually 100 to
valve fully open while occluding the vacuum hose 250mL/min).
and activating the flush valve for 5 sec. The
pressure should remain at less than 10 cm H2O. Set the flow of oxygen to around 200 mL/min.
Turn off the flow of nitrous oxide. Using an
2.10 Flowmeters. The following procedure applies to oxygen monitor, verify that at least the mini-
each flowmeter on the anesthesia unit. Record mum percent of oxygen (stipulated by the manu-
the data on Line 2.10 (i.e., oxygen, nitrous oxide, facturer) is delivered as the flow of nitrous oxide
and air). If other flowmeters are provided (e.g., is increased.
helium, carbon dioxide), make similar checks
and enter data on the back of the form. 2.12 PEEP Valve. Set up the breathing system with
a test lung. Use the -10 to +80 cm H2O pressure
Examine flowmeters for signs of damage or gauge or meter to measure the airway pressure
abuse (e.g., internal nicks, scratches, cracks, at the test lung. Manually ventilate the test lung
condensation, debris). with the PEEP valve set to deliver 0 cm H2O
water pressure. The end-exhalation pressure in
For each flowmeter, observe the float motion
the breathing system should be less than 1 cm
as the associated valve is turned. The float
H2O, although this depends on the fresh gas flow
should rise and fall freely as the flow is raised or
and APL valve setting.
lowered. At maximum flow, the float should still
be visible at the top of the flow tube. If the PEEP valve is calibrated, set it to deliver
5 and 10 cm H2O water pressure. The pressure
Connect one of the calibrated flowmeters to
in the breathing system at the end of exhalation
the common gas outlet with its discharge di-
should be within 1.5 cm H2O of the set value.
rected into the scavenging or other gas evacu-
ation system. Level the flowmeter. For each gas 3. Preventive maintenance
in turn, set the flow rates at a high and low
setting for each flowmeter that lies within the 3.1 Clean any excess leak-detection solution from
range of the calibrated flowmeter. Record the the exterior and interior of the unit; clean all
readings of both the machine and the calibrated compressed-gas filters, if needed.
flowmeters. Repeat the tests with the second
3.2 Lubricate per the manufacturer’s specifications.
calibrated flowmeter and the second group of
flow rates. 3.4 Replace compressed-gas filters and alarm bat-
teries, if needed.
The readings on the unit’s flowmeters should
agree with those on the calibrated flowmeters to 4. Acceptance tests
within 10% of set values or the manufacturer’s
specifications. If the error is excessive, check for Conduct major inspection tests for this procedure
damaged, inverted, or interchanged flowmeter and the appropriate tests in the General Devices Pro-
tubes, condensation, or damaged floats. cedure/Checklist 438.
2.11 Minimum Oxygen Flow and Percent. The follow- Before returning to use
ing procedure applies to those systems that pro-
Depressurize external gas supply; return all flow-
vide a minimum flow of oxygen or a minimum
meters to zero position; turn all vaporizers to off posi-
percent of oxygen.
tion; and reconnect all tubing (e.g., main common gas
Close the valve to the anesthesia unit’s oxy- outlet tubing). Return all controls to pre-use settings.
gen flowmeter. Connect the 0.1 to 1.0 L/min Attach a Caution tag in a prominent position so the
oxygen flowmeter to the common gas outlet. user is aware that control settings may have been
The flowmeter should read the minimum flow changed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Procedure/Checklist 420-0595
Apnea Monitors
Used For:
Apnea Monitors [12-575]
Apnea Monitors, Recording [17-885]
Impedance Pneumograph Monitors [12-621]
Respiration Monitors [12-662]
Also Called: Cardiorespiratory monitors, apnea alarms and respiration monitors, ventilatory effort monitors,
apnea detectors
Commonly Used In: Pediatric departments, homes, critical care units, nurseries, delivery rooms, ambulances
Scope: Applies to apnea monitors, which alarm if a patient stops breathing, and respiration rate monitors,
which display the patient’s breathing rate and alarm when previously selected high or low limits are exceeded;
applies to adult and infant monitoring units or modules, as well as impedance-, motion-, thermistor-, and
airway-pressure-type monitors; does not apply to other types of monitors with respiration monitoring functions
(e.g., capnometers, pulse oximeters); some apnea monitors also include other monitoring capabilities (e.g.,
ECG and blood pressure), which should be checked using the appropriate procedure/checklist unless the
function is very limited (e.g., heart rate alarm without other ECG features)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 3 months * months . hours
* Minor interval applies only to units used for home care.
Overview manual and the Health Devices evaluations cited below
for specific information.
Our evaluations of infant apnea monitors have
stressed that apnea monitoring is still an imperfect
science. An ECRI poster (Poster HD 602-980) warned
of the susceptibility of these monitors to artifact and Some apnea monitors have documentation capabili-
ties that typically can record two or more channels of
provided succinct reminders and hints for clinical per-
sonnel. An additional poster (Poster HD 625-290) and patient event data ranging from several hours to sev-
warning notice (Health Devices 1990 Apr; 19:142-5) eral months, depending on the amount and format of
data and the parameters stored. Recorded data are
provide guidance for apnea monitors used in the home.
available in two categories: patient (respiratory rate,
When inspecting these monitors, in addition to heart rate) and equipment (power on/off, low battery).
making a qualitative and quantitative inspection of Patient data can be recorded and printed as either
the monitor itself, be alert to indications of incorrect tabular data or waveforms. These data can be used to
equipment usage and misapplication. Confirm that ensure that the monitor is being used properly, to
users are aware of proper monitoring techniques and distinguish true from false alarms, and to troubleshoot
the monitor’s limitations. See the device’s operating equipment problems.
009007 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
420-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Activation of memory waveform recording can be to 5,000 Ω, variable respiration resistance change
automatic or continuous. Automatic activation is trig- amplitude from 0.1 to 1 Ω, and an apnea function;
gered when an event occurs that exceeds preset moni- simulators with fewer capabilities may be used for
tor limits. In the continuous mode, all data from the inspection, but additional equipment may be required
selected channels are recorded for a specific duration. to supplement missing functions
The data stored in the memory can be managed one of
ECG simulator with variable rate may be required
three ways. Some units overwrite the old data with
(may be part of the respiration simulator or may be
more recent events; others keep the data that satisfy
a separate unit)
specific criteria based on the duration of the events;
and some documentation monitors stop storing data Memory interface and documentation hardware
when the memory is filled. and software (where applicable)
Citations from Health Devices Procedure
Infant apnea monitors [Evaluation], 1980 Aug-Sep; Before beginning an inspection, carefully read this
9:247-83. procedure and the manufacturer’s instruction and
service manuals; be sure that you understand how to
Connection of electrode lead wires to line power [Haz- operate the equipment, the significance of each control
ard], 1987 Feb; 16:44-6. and indicator, and the alarm capabilities. If the monitor
Infant apnea monitors [Evaluation], 1987 Mar-Apr; has memory and documentation capabilities, make sure
16:79-88. the memory contents have been successfully downloaded
and documented. Also, determine whether any special
Infant home apnea monitors [Evaluation update], inspection or preventive maintenance procedures or
1987 Dec; 16:385-7. frequencies are recommended by the manufacturer.
Infant home apnea monitors: Essential safety fea- Do not test the monitor while it is in use. If a
tures and practices, 1990 Apr; 19:142-5. substitute monitor is not available, ask the nursing
Infant home apnea documentation monitors [Evalu- staff whether the patient can be temporarily removed
ation], 1992 Oct; 21(10):342-79. from the unit. It may be necessary for someone to
watch the patient in the interim. Alternatively, ar-
Air-Shields System V Model HRRM71-2 heart rate and range to be notified when the monitor is available.
respiration monitor [User Experience NetworkTM],
1992 Oct; 21(10):383. 1. Qualitative tests
Risk of electric shock from patient monitoring cables When performing IPM on apnea monitors with mem-
and electrode lead wires [Hazard], 1993 May-Jun; ory and documentation capabilities, a log identifying the
22(5-6):301-3. order, type, and duration of patient and equipment
alarms and events should be recorded (e.g., using the
Infant home apnea documentation monitors [Evalu- IPM checklist). At the end of the procedure, the memory
ation update], 1993 Dec; 22(12):564-5. contents should be compared to the log contents.
Infant home apnea monitors: Essential safety features 1.1 Chassis/Housing. Examine the exterior of the
and practices [Hazard update], 1993 Dec; unit for cleanliness and general physical condi-
22(12):598-601. tion. Be sure that plastic housings are intact,
Loose-lead alarms resulting from dried-out disposable that necessary assembly hardware is present
electrodes [User Experience NetworkTM], 1994 Jul; and tight, and that there are no signs of spilled
23(7):309-10. liquids or other serious abuse. If there are signs
of fluid spills, inspect the interior of the monitor
Test apparatus and supplies for intrusion of fluids into electronic circuitry.
The monitor top should not be used as a storage
Leakage current meter or electrical safety analyzer area for other material (e.g., formula).
Ground resistance ohmmeter
1.2 Mount. If the unit is mounted on a stand or cart,
Stopwatch or watch with a second hand check the mount’s condition. Be sure that all
Respiration simulator (needed for impedance-type fasteners are tight and that the mount is sturdy.
monitors only) that includes controls to vary the Apnea monitors should not be placed on top of
respiration rate, variable base impedance from 100 incubators where they can be easily dislodged
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Apnea Monitors
or obscure the view of an infant. A wall-sup- For monitors using belts, bands, a thermistor,
ported shelf or bracket dedicated to the monitor a mattress pad, or other sensor, connect the
is recommended. sensor to the monitor, turn on the monitor, and
jiggle the sensor cable, being careful not to dis-
1.4 AC Plug/Receptacles. Examine the AC power turb the sensor in such a way as to simulate a
plug for damage. Attempt to wiggle the blades breath. Observe the monitor for artifacts that
to determine that they are secure. Shake the would indicate a defective cable or connector.
plug and listen for rattles that could indicate
loose screws. If any damage is suspected, open 1.10 Fittings/Connectors. Examine all fittings and
the plug and inspect it. If the device has electri- connectors, including electrical cable connectors,
cal receptacles for accessories, insert an AC plug for general condition. Electrical contact pins or
into each and check that it is held firmly. If surfaces should be straight, clean, and bright.
accessories are plugged and unplugged often,
1.11 Electrodes/Transducers. Confirm that any nec-
consider a full inspection of the receptacle.
essary electrodes and/or transducers are on hand
and check their physical condition. If disposable
1.5 Line Cord. Inspect the cord for signs of damage.
electrodes are used, be sure an adequate supply
If damaged, either replace the entire cord or, if
is on hand.
the damage is near one end, cut out the defective
portion. Be sure to wire the new power cord or Verify that the insulation on thermistor sen-
plug with the same polarity as the old one. Also, sors is intact. Check that air mattresses are free
check battery charger line cords. of leaks and that the tubing that connects the
segments of the mattress to the manifold fits
1.6 Strain Reliefs. Examine the strain reliefs at both well, without the use of tape. Keep spare tubing
ends of the line cord. Be sure that they hold the on hand to make necessary repairs. Carefully
cord securely. If the line cord is detachable (by examine sensor belts, bands, or pads (magnetic,
the user), affix the cord to the unit so that it capacitive, or pressure transducer) for intact in-
cannot be removed by the operator. (See Health sulation. If there are cracks or defects in the
Devices 1993 May-Jun; 22[5-6]:301-3.) insulation, remove the sensor from service.
1.7 Circuit Breaker/Fuse. If the device has a 1.13 Controls/Switches. Before moving any controls
switch-type circuit breaker, check that it moves and alarm limits, check their positions. If any
freely. If the device is protected by an external appear inordinate (e.g., a gain control at maxi-
fuse, check its value and type against that mum, alarm limits at the ends of their range),
marked on the chassis, and ensure that a spare consider the possibility of inappropriate clinical
fuse is provided. use or of incipient device failure. Investigate
questionable control settings on a home care
1.9 Cables. Inspect the cables (e.g., patient sensor, monitor. Consult with the patient’s physician to
remote alarm) and their strain reliefs for general determine correct settings. The parents should
condition. Examine cables carefully to detect receive additional training if required. Record
breaks in the insulation and to ensure that they the settings of those controls that should be
are gripped securely in the connectors of each returned to their original positions following the
end to prevent rotation or other strain. Elec- inspection. Examine all controls and switches
trode leads and cables are often fragile and may for physical condition, secure mounting, and cor-
lack adequate strain relief; intermittent contact rect motion. Where a control should operate
can provide false indications. against fixed-limit stops, check for proper align-
ment, as well as positive stopping. Check mem-
The lead-electrode connector should be of the brane switches for membrane damage (e.g., from
type that cannot be inadvertently plugged into a fingernails, pens). During the course of the in-
115 VAC outlet or power cord. Attach a pair of spection, be sure to check that each control and
electrodes to the patient cable and hold the RA and switch performs its proper function.
LA electrodes face to face. Connect the patient
cable to the monitor, turn the unit on at maximum 1.17 Battery/Charger. Inspect the physical condi-
sensitivity, and jiggle the leads. If either breaths tion of batteries and battery connectors, if read-
or lead faults are indicated, suspect damaged ca- ily accessible. Check operation of
bles or weak contact with the electrodes. battery-operated power-loss alarms, if so
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
equipped. Operate the unit on battery power for dized) metal on the chassis with an ohmmeter,
several minutes to check that the battery is electrical safety analyzer, or multimeter with
charged and can hold a charge. Check the condi- good resolution of fractional ohms. We recom-
tion of the battery charger and, to the extent pos- mend a maximum of 0.5 Ω.
sible, confirm that it does, in fact, charge the
battery. When it is necessary to replace a battery, If the device has an accessory outlet, check its
label it with the date. grounding to the main power cord.
1.18 Indicators/Displays. During the course of the 2.2 Leakage Current. Measure chassis leakage cur-
inspection, confirm the operation of all lights, rent with the grounding conductor of plug-con-
indicators, and visual displays on the unit and nected equipment temporarily opened. Operate
charger, if so equipped. Be sure that all seg- the device in all normal modes, including on,
ments of a digital display function. standby, and off.
1.19 User Calibration. Confirm that the calibration Chassis leakage current to ground should not
or test function operates. exceed 300 µA.
1.20 Alarms/Interlocks. Operate the device in such If a bedside or central station monitor is
a way as to activate each audible and visual grounded through system interconnections in
alarm. Check that any associated interlocks addition to power line grounding and is only used
function. If the device has an alarm-silence fea- in this configuration, then do not disconnect the
ture, check the method of reset (i.e., manual or monitor from the system to measure leakage
automatic) against the manufacturer’s specifica- current during routine inspections. Verifying
tions. Some apnea alarms that reset automat- low grounding resistance is adequate.
ically when breathing resumes have a separate 2.3 Open Electrode Indicator. This check is for im-
indication that an apneic episode has occurred; pedance-type monitors only. Connect the moni-
this reminds clinical personnel that the patient tor to the respiration simulator. Vary the base
needs closer attention. To verify that this indica- impedance and determine the resistance value
tor functions properly, halt simulated respira- at which the unit first indicates an electrode
tion until the apnea alarm sounds, then resume fault. This is usually in the range of 1,000 to
the simulated respiration. Check that the reset 2,000 Ω.
control functions. If the unit is used with a
remote alarm indicator, verify its function. 2.4 Sensitivity.
1.21 Audible Signals. Operate the device to activate Impedance-type monitors. If the monitor has a
any audible signals. Confirm appropriate vol- manual sensitivity control, set it at maximum
ume, as well as the operation of the volume sensitivity. Connect the respiration simulator
control, if so equipped. and, if adjustable, set it for a base impedance
of 500 Ω, resistance change of 1 Ω, and breath-
1.22 Labeling. Check that all necessary placards, la- ing rate of 30 bpm (15 bpm for an adult moni-
bels, and instruction cards are present and leg- tor). Verify that the monitor detects each
ible. resistance change. Decrease the resistance
change on the simulator and record the mini-
1.23 Accessories. Verify that electrode gel, if used, is
mum value for which breaths are reliably
available.
detected. Most monitors will detect resis-
1.24 CRT Display. If the unit includes a display of tance changes of 0.1 to 0.3 Ω at maximum
respiration waveform, check it for focus, slope, sensitivity.
bow, baseline, position, burn spots, and 60 Hz
Increase the rate to 100 bpm and verify that
interference or other noise. Verify that the dis-
the sensitivity does not change abnormally.
play amplitude increases as the impedance
change setting of the simulator is increased. Discrepancies between similar monitors or
from previous readings greater than 25% sug-
2. Quantitative tests gest significant deterioration of the monitor
and should be investigated.
2.1 Grounding Resistance. Measure and record the
resistance between the grounding pin of the With the monitor set at maximum sensitiv-
power cord and exposed (unpainted and not ano- ity, verify that breaths are not detected when
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Apnea Monitors
the simulator is set to 0 bpm or turned off. activated when the indication falls below 22
Some simulators, when turned off, may pre- bpm. Some monitors have fixed alarm delays;
sent a high base resistance to the monitor that check the instruction manual to determine
can cause extraneous noise pickup. whether this feature is present.
Other types. Only qualitative tests of sensitivity Next, simulate a rate of about 60 bpm, reset
can be made with other types of sensors. any alarms, then increase the simulated rate to
Simulate breaths in the appropriate manner 80 bpm or higher, and verify the operation of the
for each monitor, and observe that the sensi- high-rate alarm.
tivity varies with the control setting. In some
cases, sensitivity will vary with the simulated 3. Preventive maintenance
respiration rate. Confirm the absence of arti-
3.1 Clean the exterior of the unit with a damp cloth,
facts at maximum sensitivity.
if needed.
2.5 ECG Features. If the unit includes ECG and
heart rate monitoring, perform trace quality and 4. Acceptance tests
additional testing as part of a separate ECG In addition to other considerations, every apnea
Monitors procedure. If the unit has limited ECG monitor must include a heartbeat detector (or other
features — such as a heart rate alarm — but no backup mechanism to the primary apnea detection
additional ECG functions, test these as part of function). If battery-powered, the unit must indicate
this procedure. If more extensive ECG tests are whether it is operating on battery power or is being
required, see ECG Monitors Procedure/Check- powered (and charged) from line power. For home use,
list 409. monitors must also include a power-loss alarm (non-
2.10 Apnea Alarm Delay Time. Check the apnea battery-operated unit) and a remote alarm. (See Health
alarm delay by stopping simulated respirations. Devices 1990 Apr; 19:142-5 for further information.)
Time the delay between cessation of respiration Conduct major inspection tests for this procedure
and apnea alarm. Measured times should agree and the appropriate tests in the General Devices Pro-
with indicated times within 20%. Check all cedure/Checklist 438. In addition, perform the follow-
times, if discrete times are available. If the ing tests.
control is continuously variable, check both
shortest and longest times. Check the alarm-si- 4.1 Sensitivity. Testing is similar to that described
lence function, if so equipped. in Item 2.4; however, record the actual sensitiv-
ity at high and low breathing rates (at low,
2.11 Ratemeter Accuracy. Using the respiration medium, and high sensitivity on manual units).
simulator, check the rate display on respiration Also, record the maximum sensitivity at a base
rate monitors at low rate (about 15 bpm for adult impedance of 100 Ω.
units and 30 bpm for infant units) and high rate
(100 bpm). Read the ratemeter when it reaches 4.2 Coincidence Circuit. Some monitors include co-
equilibrium. Indicated rates should be accurate incidence circuitry designed to compare breath-
to within 10%. ing and heart rate signals or data and to reject
detected breaths that may, in fact, be errone-
If the ratemeter is digital, vary the simulated ously detected QRS complexes. If possible, ver-
rate to check for malfunctioning digits. A display ify operation of coincidence circuitry during
of “8” in the tens and units position will check all incoming inspection.
elements of a segmented or dot display; a “1” and
“0” in the hundreds place is all that is needed there. Before returning to use
2.12 Rate Alarm Accuracy. Set the low and high res- Remind clinical personnel of the limitations of the
piration rate alarms at 22 and 78 bpm, respec- monitor and be sure that they understand the operating
tively. Simulate a respiration rate of about 30 principles of that particular unit, since a hospital may
bpm, set the apnea delay to at least 10 sec, and own more than one type of apnea monitor. Also, make
reset any alarms that may have been triggered sure that the audible alarm volume, including remote
during setup. Slow down the simulated respira- alarm if needed, is set so that it can be clearly heard. If
tion rate to about 20 bpm. Observe the rateme- the monitor is being used at home, make sure that the
ter, and verify that the low-rate alarm is controls are set correctly for the patient application.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 462-0595
Argon Surgical Lasers
Used For:
Lasers, Surgical, Argon [16-941]
Also Called: Argon lasers, blue/green lasers, surgical lasers, bronchopulmonary lasers, gastroenterology
lasers, high-power ophthalmic lasers, photocoagulator lasers
Commonly Used In: Operating rooms, short procedure areas, endoscopy laboratories, ophthalmic oper-
ating rooms
Scope: Applies to general-purpose argon surgical lasers that include contact and/or noncontact flexible
fiberoptic delivery systems (either reusable or disposable), emit blue-green visible light energy at 514 and 488
nm, and can provide sufficient power output to coagulate and vaporize tissue; applies to low- and high-power
argon surgical lasers that are typically used for general surgery, gastroenterology, bronchopulmonary,
neurosurgery, gynecology, and ENT surgery procedures; does not apply to ophthalmic argon lasers, which are
typically low power (e.g., below 2 W); however, many of the tests listed herein can be used or modified for
these other lasers
Risk Level: ECRI-recommended, High; Hospital assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview Argon surgical lasers affect tissue by delivering
blue-green visible light energy at a sufficient power
density to cause vaporization and/or coagulation. The
Argon lasers are normally checked before each use by 488/514 nm argon energy is preferentially absorbed by
the laser’s power-on self-test and by user examination pigmented tissue and hemoglobin and is typically ab-
of the aiming beam and the delivery system to be used. sorbed within 3 mm of the tissue surface. Argon surgi-
This minimizes the need for frequent additional peri- cal laser fibers are most often used in contact with or
odic testing. close to tissue to cause coagulation and vaporization.
Moving the fiber tip away from the tissue to lower the
Manufacturers or outside service vendors often power density causes less tissue to be vaporized and
maintain lasers for hospitals. The extent and fre- coagulated.
quency of inspection by hospital personnel should be
coordinated with these outside services. General-purpose argon surgical lasers have a laser
tube containing an argon gas mixture that is caused to
Failure of an argon surgical laser can cause patient emit light energy by an electric field. This energy
or staff injury, abrupt interruption of a surgical proce- leaves the laser tube through a partially reflecting
dure, or damage to the laser system. These lasers must mirror and is typically directed into a flexible optical
be meticulously maintained in order to ensure proper fiber that transmits the laser energy to the tissue. The
and safe operation. fiber may be used with additional devices (e.g., through
230380 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
462-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
an endoscope), with a headpiece and lens, and/or with from the manufacturer or from a qualified alternative
a laser handpiece or a laser micromanipulator (used to training source.
interface the laser with the surgical microscope).
Laser energy can cause serious injury, particularly
These attachments may focus the energy into a small
when the internal interlock is overridden or in any
spot size at a known working distance and/or a specific
other situation in which the energy does not diverge
beam direction to accomplish special tasks (e.g., energy
significantly over long distances. Under some circum-
can be emitted from the surgeon’s headpiece through
stances, the beam may not diverge significantly, even
a handheld lens and focused on the patient’s retina).
a full room length or more away from the laser (and
In addition, argon lasers can emit a single pulse or a
can harm tissue or burn material even at this dis-
train of pulses.
tance). Therefore, exercise great care whenever a laser
Like most lasers, argon lasers are inefficient in beam is accessible. Area security and use of personnel
converting electrical energy into laser energy. As a protective devices and practices should be consistent
result, excess heat is generated in the laser cavity, with hospitalwide laser safety procedures and/or
requiring a cooling system. Most argon lasers use should be approved by the laser safety committee.
water/air cooling systems that are self-contained, con-
In addition, windows should be covered with nonre-
nected to a freestanding chiller system, or connected
flective material to prevent transmission of laser en-
to a water supply and drain.
ergy to other areas.
Citations from Health Devices Wear appropriate laser safety eyewear at all times
Laser use and safety [Guidance article], 1992 Sep; whenever the laser is in the Operating mode. WARN-
21(9):306-10. ING: Do not stare directly into the aiming system beam
or the therapeutic laser beam, even when wearing laser
Surgical lasers [Evaluation], 1991 Jul-Aug; 20(7- safety eyewear. Avoid placing the laser beam path at
8):239-316. eye level (i.e., kneeling, sitting, or standing).
Test apparatus and supplies Do not perform these procedures when a patient is
present or clinical staff is working, and do not aim the
Leakage current meter or electrical safety analyzer
laser across a path that a person might normally use
Ground resistance ohmmeter as a thoroughfare. Furthermore, at minimum, post
New, unused fiber delivery system doors to the room with appropriate laser safety signs
stating that the laser is in use and that it is unsafe to
Black Delrin block 1⁄2″ or more thick, 1″ or more wide,
enter the room without authorization by the service
about 3″ to 4″ long; tongue depressors; or firebrick person performing the procedure. A second person
Laser radiometer (power meter) should be present, especially during procedures of rec-
Laser safety signs ognized risk, to summon help in case of an accident.
Laser safety eyewear specifically designed for use The laser should remain in the off position when not
with argon surgical lasers and of sufficient optical in use. When in use, it should be in the standby/dis-
density to protect the wearer’s eye from laser injury abled mode. Do not switch it to the operating mode
until the procedure is about to begin and the laser and
Vise with padded jaws or ring stand with padded
its delivery system are properly positioned. If the pro-
clamp
cedure must be interrupted, disconnect the laser from
Pressure gauges and coolant system tee fitting line voltage, and remove the laser operation key and
Outlet test fixture (optional) store it in a controlled location.
Insulating gloves, high voltage (optional) Do not use the laser in the presence of flammable
Grounding strap (optional) anesthetics or other volatile substances or materials
(e.g., alcohol), or in oxygen-rich atmospheres, because
Calibrated flowmeter of the serious risk of explosion and fire. Remove from
the working area or cover with flame-resistant opaque
Special precautions material all reflective surfaces likely to be contacted
Inspecting and maintaining lasers is a dangerous as by the laser beam. Whenever possible, use a firebrick
well as necessary process, and far greater care is or other nonflammable material behind the target mate-
required than with most devices. Personnel who in- rial (e.g., black Delrin) when the laser is to be activated.
spect or service lasers should receive special training Target materials will ignite when exposed to high laser
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Argon Surgical Lasers
energies; use short durations when practical. A CO2 and ensure that they have been turned off
fire extinguisher should be readily available. after the last use. Examine the exterior of the
unit for cleanliness and general physical con-
Some surgical lasers use high voltages (e.g., 20 kV), dition. Be sure that all housings are intact and
which can be lethal. Capacitors may store charges long properly aligned, that assembly hardware is
after the device has been disconnected from line volt- present and tight, that any retractable parts
age. Consult the manufacturer’s recommended proce- slide easily and lock in place if so constructed,
dures for servicing high-voltage laser circuits, and that there are no signs of spilled liquids or
avoid contact with any portion of the high-voltage other evidence of abuse, and that there are no
circuit until you are certain that the charge has been obvious signs of water or oil leakage.
drained. In such instances, a good ground must be
present; preferably, use a redundant ground strap if Shutters. If manual shutters for the aiming sys-
you must enter the laser cabinet. When possible, dis- tem or the therapeutic lasers are accessible,
connect the laser from line voltage before entering the ensure that they operate smoothly and cor-
laser cabinet, and use insulated gloves for those proce- rectly. Be sure to leave the shutter in the
dures in which contact with a high-voltage source is proper position for normal operation.
possible (and the gloves are not otherwise contraindi-
cated). Ensure that equipment intended to be used to 1.2 Mounts/Holders. Check that the mounts se-
measure, drain, or insulate high voltages carries the curely contain any gas cylinders that may be in
appropriate insulation rating (e.g., above 20 kV). use. Be sure that mounts or holders intended to
secure the fiber to the fiber support (to protect
Where possible, perform tests with the unit turned the fiber when in use) are present, in good work-
off. Because of the presence of high voltage, perform ing order, and being used. Similarly, check
the Grounding Resistance test (Item 2.1) before any mounts or holders for other devices (e.g., exter-
other test that requires operation of the laser. nal power meters, footswitches).
WARNING: Do not use an anesthesia or other simi- If the device is mounted on a stand or a cart,
lar bag that may have a mold-release agent (e.g., starch, examine the condition of the mount. Verify that
talc) on its inside surface because the agent could the mounting apparatus is secure and that all
contaminate the gas recirculation system of the laser hardware is firmly in place.
and ultimately contaminate a patient wound during a
subsequent procedure. 1.3 Casters/Brakes. Verify that the casters roll and
swivel freely. Check the operation of brakes and
Report any laser accident immediately to the laser swivel locks.
safety officer or equivalent, as well as to the hospital
risk manager. 1.4 AC Plug/Receptacle. Examine the AC power
plug for damage. Wiggle the blades to deter-
Procedure mine whether they are secure. Shake the plug,
Before beginning the inspection, carefully read this and listen for rattles that could indicate loose
procedure and the manufacturer’s operator instruc- screws. If damage is suspected, open the plug
tions and service manual; be sure that you understand and inspect it.
how to operate the equipment, the significance of each 1.5 Line Cords. Inspect line cords for signs of dam-
control and indicator, and precautions needed to en- age. If a cord is damaged, replace the entire cord,
sure safety and avoid equipment damage. Also, deter- or, if the damage is near one end, cut out the
mine whether any special inspection or preventive defective portion. Be sure to wire a new power
maintenance procedures or frequencies are recom- cord or plug with the correct polarity.
mended by the manufacturer.
1.6 Strain Reliefs. Examine the strain reliefs at
1. Qualitative tests both ends of the line cord. Be sure that they grip
1.1 Chassis/Housing. the cord securely.
General. Verify that the key has not been left in 1.7 Circuit Breakers/Fuses. If the device has a
the laser. (Remove it if it has been, and inform switch-type circuit breaker, check that it moves
users of the importance of storing the key in a freely. If the device is protected by an external
controlled location.) Examine any external fuse(s), check its value and type against what is
gas tanks that may be in use with the laser, marked on the chassis or noted in the instruction
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
service manual. Ensure that a spare is provided 1.13 Controls/Switches.
or readily available. General. Before moving any controls, check and
1.8 Tubes/Hoses. Check the condition of all cool- record their positions. If any position appears
ing-system hoses and any other hoses or tubing inordinate, consider the possibility of inappro-
the laser may have (e.g., drain, gas). Check that priate use or of incipient device failure. Exam-
they are of the correct type; that they have not ine all controls and switches for physical
become cracked and do not show other signs of condition, secure mounting, and correct mo-
significant abuse; that they are connected cor- tion. If a control has fixed-limit stops, check
rectly and positioned so that they will not leak, for proper alignment as well as positive stop-
kink, trail on the floor, or be caught in moving ping. Check membrane switches for tape resi-
parts; and that they are secured adequately to due and for membrane damage (e.g., from
any connectors. fingernails, pens, or surgical instruments). If
you find such evidence, notify users to avoid
1.9 Cables. Inspect all cables and their channels or using tape and sharp instruments. During the
strain reliefs for general physical condition. Ex- inspection, be sure that each control and
amine cables carefully to detect breaks in insu- switch works properly.
lation and to ensure that they are gripped
Remote. Examine the exterior of the control for
securely in the connectors at each end to prevent
cleanliness and general physical condition. Be
strain on the cable.
sure that housings are intact, that assembly
1.10 Fittings/Connectors. Examine all optical (e.g., hardware is present and tight, and that there
fiber), gas, liquid, and electrical fittings and con- are no signs of spilled liquids or other serious
nectors for general physical condition. Gas and abuse. If the remote control is attached by
liquid fittings should be tight and should not cable to the laser, ensure that the cable and
leak. Electrical contacts should be straight, any connectors are in good condition. Examine
clean, and bright. all controls and switches for general physical
condition, secure mounting, correct motion,
There should be no visible dirt or residue in and intended range of settings. Where a con-
the optical path of the laser aperture. Ensure trol should operate against fixed-limit stops,
that any mechanism to close off the laser aper- check for proper alignment as well as positive
ture (fiber port) is clean, operates smoothly, and stopping. During the course of the inspection,
is in use. be sure to check that each control and switch
If external gas tanks or wall-supply outlets performs properly.
can be used, gas-specific connectors should be Footswitch. Examine the footswitch for general
present. Be sure that no pins are missing from physical condition, including evidence of
yokes and that the keying and indexing of con- spilled liquids. Footswitches for lasers include
nectors for each gas to be used is correct. A laser an internal switch that activates according to
that connects to a central piped medical gas the depth of pedal depression. It is usually
system or to a freestanding medical gas system possible to feel the vibration caused by closure
should have the matching DISS or quick-connect of the switch, even through a shoe. Check that
fitting for the gas that it is to be used with. Verify the internal switch is operating and that the
that suitable unique connectors are supplied so footswitch does not stick in the on position.
that adapters are not required. Some footswitches include two internal
1.12 Filters. Check the condition of all liquid and air switches; in this case, verify the operation of
filters. Some argon surgical lasers require deion- both. Some footswitches also include a switch
ized water, and most require special filtration. to operate the liquid- or gas-cooling system.
Measuring the pressure drop across a liquid Check to be sure that this switch operates
filter can be helpful in determining whether the reliably.
filter should be replaced. Clean or replace filters During the procedure, check to be sure that
according to the manufacturer’s recommenda- the laser activates consistently when the foot-
tions (e.g., replace if the pressure drop is >5 psi), switch is depressed and that the fiber-coolant
and indicate this in the preventive maintenance system operates properly when the fiber-cool-
section of the inspection form. Clean or replace ant switch is activated and deactivated. Flex
air filters that are obviously dirty. the cable at the entry to the switch, and, using
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Argon Surgical Lasers
an ohmmeter, check for internal wire breaks information expected. Ensure that user prompts
that cause intermittent operation. Confirm occur in the proper sequence. Store some sample
that strain reliefs are secure. information, and verify that it is correct. If a
feature to manually reset this information is
Examine the male and female connectors
available, ensure that it works.
for attaching the footswitch to the laser
cabinet to be sure that no pins are bent and 1.19 Laser Delivery System Calibration. Some argon
that no other damage is present. Ensure surgical lasers include a user-accessible calibra-
that the connector secures acceptably to the tion port or power meter that allows output cali-
laser cabinet. bration and/or testing of the laser fiber. This
feature is provided because transmission of laser
1.15 Motors/Pumps/Fans/Compressors. Check the
energy through a fiber may change as a result of
physical condition and proper operation of these
fiber use. Based on the measurement from the
components, if present. If lubrication is required,
calibration power meter, the laser may automat-
note this in the preventive maintenance section
ically recalibrate itself and/or adjust displays so
of the form.
that the power indicated to be delivered to the
1.16 Fluid Levels. Check all fluid (e.g., coolant) lev- patient will be correct; or it may require the user
els. Refill or change the fluid according to the to do this manually. Verify that this feature is
manufacturer’s recommendations, and note this functioning by using the manufacturer’s recom-
in the preventive maintenance section of the mended calibration procedure to test one deliv-
inspection form. If an external water supply is in ery system (e.g., fiber, handpiece) that the
use, ensure that the water pressure is properly manufacturer indicates can be acceptably cali-
regulated and at the appropriate pressure and brated using these procedures. A good-quality
that the supply and drain system is properly (e.g., >85% transmissibility, undamaged sheath)
configured (e.g., filters are oriented for proper fiber or handpiece should be used for this test.
flow, drain hoses are positioned in a sink or
1.20 Alarms/Interlocks. Operate the device in a
drain).
manner that will activate the self-check feature,
1.17 Battery. Inspect the physical condition of batter- if present, and verify that all visual and audible
ies and battery connectors, if readily accessible. alarms activate according to the manufacturer’s
If a remote control or display is battery powered, documentation. If no self-check feature is pre-
check or replace the battery (periodic prophylac- sent, operate the laser in a manner that will
tic battery replacement is often preferred to risk- activate each audible and visual alarm; be sure
ing battery failure during use). When it is to test only those alarms that will not cause
necessary to replace a battery, label it with the damage to the laser or present an unnecessary
date. risk of laser beam exposure to the user or by-
standers.
1.18 Indicators/Displays. During the course of the
inspection, verify proper operation of all lights, If a door or window interlock is used, ensure
indicators, meters, gauges, and visual displays that it deactivates the laser properly. (Do not
on the unit and remote control. Ensure that all disassemble major parts of the laser to test in-
segments of a digital display function. Note any ternal interlocks.) After deactivating the laser
error messages displayed during the power-on and reclosing the door or window, check to be
self-test. sure that the laser will restart. Be sure to check
the interlocks in all locations where the laser is
If primary and remote-control indicators and used. (For some lasers, the function of the inter-
displays can be used at the same time or if control locks can be checked using an ohmmeter.)
can be switched from one to the other during the
course of a procedure, verify that the same infor- If the laser is equipped with an emergency
mation (e.g., settings, displays) is indicated on “kill” switch, test this feature to be sure that it
both control panels during laser operation. deactivates the laser and that the laser will
subsequently restart.
If display screens or digital displays are pro-
vided for user prompts or for viewing accumulated 1.21 Audible Signals. Operate the device to activate
information (e.g., pulse or accumulated energy any audible signals (e.g., laser emission, setting
counter), ensure that each display provides the change). Check for proper operation, and verify
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
that the signal can be heard in the environment recommendations for the procedures and
in which the laser will be used. cleaning agents to use to clean lenses.
1.22 Labeling. Check that all placards, labels, and Ensure that major subcomponents of the
instruction cards noted during acceptance test- handpiece, when assembled, are secure. En-
ing are present and legible. Check to see that an sure that the mechanisms used to connect the
instruction manual is kept with the laser or is handpiece(s) to the fiber are in good working
readily available. order and that they reliably secure each hand-
piece to the fiber.
1.23 Accessories.
Microscope micromanipulator. Examine the mi-
General. Verify that all necessary accessories croscope micromanipulator for cleanliness
are available and in good physical condition. and general physical condition. Be sure to
Set up reusable accessories with the laser to handle it by the main body; do not hold it by
ensure compatibility and proper functioning. the joystick, and do not touch the reflecting
Checking all fibers or accessories during a lenses in the body. Inspect micromanipulators
single inspection and preventive mainte- provided by both the laser manufacturer and
nance procedure is unnecessary as long as the laser accessory manufacturer.
accessories are routinely checked by the per- Ensure that the reflecting lenses are intact
son(s) responsible for laser setup and opera- and clean. Consult the manufacturer’s recom-
tion. In addition, many of the accessories are mendations for the procedures and cleaning
sterile and would require resterilization be- agents to use to clean reflecting lenses.
fore use, making the laser potentially un-
Examine the joystick to ensure that it is
available. Be sure to check with the person
firmly attached and that it freely moves the
responsible for scheduling the use of the laser
reflecting lens. If a finger rest is present,
before beginning the procedure.
ensure that it is firmly attached and properly
Fibers. For the test fiber or before each use, oriented.
examine the connector, cable, and tip of each
If a zoom focus feature is present, be sure
fiber that may be used, as well as the fiber
that it turns easily and does not slip. Examine
support, for cleanliness and general physical
each objective lens to ensure that it is intact
condition. Be sure that all hardware (e.g.,
and clean. Do not touch the lens surface. Con-
laser gas tubing channels) is present, in good
sult the manufacturer’s recommendations for
condition, and firmly attached. Ensure that
the procedures and cleaning agents to use to
the connector properly seats into the laser
clean the objective lenses. Carefully insert
aperture of the laser cabinet. Examine the
each lens into the micromanipulator, and en-
distal end of fibers to ensure that any connect-
sure that it fits snugly.
ing mechanisms (e.g., threads) are in proper
working order. Inspect the mechanism used to attach the
micromanipulator to the microscope to ensure
If a fiber appears to be dirty or damaged, that all parts are present and that it is in good
remove it from service. If a fiber is reusable, working order. Connect the micromanipula-
notify the person(s) responsible for fiber re- tor to the microscope to check for a secure
pair. The fiber should be repaired and/or connection.
cleaned according to the manufacturer’s rec-
ommendations. Verify fiber performance. Safety filters. Verify operation of safety filters
in the microscope and endoscope delivery
Handpieces. Examine each handpiece compo- systems.
nent (e.g., body, tips, lenses) for cleanliness
and general physical condition. Examine in- 1.24 Aiming Beam. Argon lasers typically use an at-
dividually only those components that are tenuated therapeutic beam as the aiming beam.
intended for removal during normal use and Activate the aiming beam (without the therapeu-
storage. (Do not remove other parts that are tic beam), and verify that it produces a round,
press-fit or attached by screws, bolts, or uniformly bright spot, with no halo. For hand-
snap-rings.) If lenses are detachable, be sure pieces that provide adjustable spot sizes, verify
not to touch the lens surface; handle lenses that the spot size changes as expected and still
by the edges only. Consult the manufacturer’s remains uniform.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Argon Surgical Lasers
1.25 Laser Aperture. on the chassis should not exceed 300 µA; in no
case should it exceed 500 µA. Where it is greater
WARNING: Make this inspection with the la-
than 300 µA, ensure that appropriate grounding
ser powered off. Remove and inspect the protec-
is present.
tive window (e.g., blast shield) behind the laser
aperture. It should be clean and undamaged; 2.3 Exposure Duration. Some laser power meters
replace if needed. There should be no visible dirt can measure pulse duration. If the power meter
or residue in the optical path of the laser aper- can react to pulse duration (this is the preferred
ture. circumstance), test the laser at each setting.
However, if the laser power meter does not meas-
1.26 Gas Regulators. Examine any gas regulators for
ure pulse duration, use the following less prefer-
cleanliness and general physical condition. En-
able alternative.
sure that the gauges on the regulators are not
broken. During the procedure, ensure that the Place and secure the laser fiber, handpiece, or
regulator and the gauge operate as expected. micromanipulator with the aiming system fo-
Verify that the correct gas is attached to each cused on the black Delrin or a tongue depressor.
regulator. Be sure that a key or wrench to facili- With the laser set to about 10 W and the expo-
tate changing the gas supply is with the unit or sure set at a minimum duration, activate the
readily available. laser and create a burn. Carefully move the
Delrin to expose a clean area, maintaining the
If the laser includes a gas recirculation sys-
same distance. Adjust the exposure setting in
tem, ensure proper operation by allowing it to
increments of 0.1 sec or the next longest dura-
control the gas supply into and out of a sealed
tion, and activate the laser at each setting. Con-
plastic bag.
tinue this process until you have tested all
WARNING: Do not use an anesthesia or other exposure settings, except continuous, and have
similar bag that may have a mold-release agent developed a series of burns. Compare the burns
(e.g., starch, talc) on its inside surface because the to verify that progressively larger burns oc-
agent could contaminate the gas recirculation curred as the exposure duration increased.
system of the laser and ultimately contaminate a
patient wound during a subsequent procedure. 2.4 Repeat Pulse. If the unit includes a repeat pulse
feature, which repeats the pulse at a fixed or
If proper operation is questionable, consider adjustable rate, test this feature with the laser
using a calibrated flowmeter to measure actual set at the minimum, median, and maximum
gas flow. repeat pulse settings, if adjustable. Some laser
power meters can react quickly enough to be
2. Quantitative tests used to test this feature of the laser. If you are
using such a power meter, test the laser to be
2.1 Grounding Resistance. Use an ohmmeter, elec-
sure that the correct power is repeatedly deliv-
trical safety analyzer, or multimeter with good
ered over the correct time period.
resolution of fractional ohms to measure and
record the resistance between the grounding pin If your laser power meter cannot be used for
on the power cord and exposed (unpainted and this test, use the following alternative test
not anodized) metal on the chassis, accessory method. Set the laser to about 10 W and a 0.1
outlet, ground pins, and footswitch. We recom- sec exposure duration with the fiber, handpiece,
mend a maximum of 0.5 Ω. (If the footswitch is or micromanipulator attached, and verify that
of low voltage, grounding is not required.) the repeat pulse feature operates as expected by
moving the Delrin or the colored tongue depres-
2.2 Leakage Current.
sor slightly between each pulse. Be extremely
WARNING: Do not reverse power conductors careful to keep hands out of the laser beam path.
for this or any other test. Improper attachment of If the number or duration between repeat pulses
conductors may damage the laser. is adjustable, test that setting changes made
throughout the range result in the expected
With the laser attached to a grounded power- performance.
distribution system, measure the leakage current
between the chassis and ground with the unit 2.5 Footswitch Exposure Control. Set the output
grounded and ungrounded. The leakage current time for about 5 sec, activate the unit, and re-
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
lease the footswitch after about 1 sec. Verify that 3.3 Calibrate/adjust any components (e.g., printer)
the beam turns off when the footswitch is re- according to the manufacturer recommenda-
leased. tions. Only appropriately trained personnel
should attempt laser adjustments. Ensure that
2.10 Power Output. Select one delivery system (e.g., all hoses and tubes are tight.
fiber, handpiece, micromanipulator), and per-
form the manufacturer’s recommended user cali- 3.4 Replace filters if needed. Check all fluid levels
bration procedure. Secure the delivery system at and supplement or replace fluids if needed.
the appropriate distance from the detector of the
laser power meter to meet spot-size require- 4. Acceptance Testing
ments specified in the instructions for the meter. Conduct major inspection tests for this procedure
(Do not focus the beam to a small spot on the and the appropriate tests in the General Devices Pro-
power meter. Some power meters require that cedure/Checklist 438.
the unfocused or a defocused laser beam be pro-
jected into the power meter to cover the majority WARNING: Lasers may be damaged by switching
of the absorber surface. If the laser beam is between normal and reverse polarity while the device is
focused on the detector of such meters, the meter on. If reverse-polarity leakage current measurements
may be damaged.) are made, turn off the unit being tested before switching
polarity. Also, lasers powered by three-phase electrical
WARNING: Accessing the unfocused laser systems may be damaged if proper electrical phase
beam may require defeating internal interlocks. connections are not made initially and maintained
Because of the heightened risk associated with an thereafter. Thus, do not switch conductor connections
unfocused, nondiverging laser beam, exercise or wiring configurations for any tests, including leak-
great care if the interlocks are to be defeated. age current measurement. Do not conduct electrical
With the laser set at low (e.g., 10% of full leakage current tests with reversed-polarity wiring.
scale), medium (e.g., 50% of full scale), and maxi- Also test the ability of the laser to deliver laser
mum output, activate the laser for a sufficient energy as expected in all configurations and with all
period to acquire acceptable readings. (Power provided laser accessories. In addition, perform the
meters use different time constants to acquire an following tests.
acceptable reading, and you must know and me-
ticulously follow them.) Compare the reading 4.1 Areas of Use. Visit the area(s) in which the laser
with the power display of the laser; the measured is to be used and ensure that laser signs,
and displayed values should all be within 10% of eyewear, and window coverings are available
one another. In addition, compare the reading and being used and that safety interlocks for
obtained with the reading taken on incoming doors or windows, if present, are functioning
acceptance testing, at the last preventive main- properly.
tenance procedure, or after the last service pro-
4.2 Casters/Mounts/Holders. Ensure that the as-
cedure. If the laser includes a low-power (e.g.,
sembly is stable and that the unit will not tip
mW) feature, test it in a similar fashion with a
over when pushed or when a caster is jammed on
power meter of appropriate resolution in the
an obstacle (e.g., a line cord, threshold), as may
low-power range.
occur during transport. If the device is designed
to rest on a shelf, ensure that it has nonslip legs
3. Preventive maintenance
or supports.
Verify that all daily preventive maintenance proce-
dures recommended by the manufacturer are carried 4.3 Labeling. Examine the unit and note the pres-
out. ence, location, and content of all labels. Labeling
information is typically found in the laser’s op-
3.1 Clean the exterior. Clean accessible optical com- erator manual.
ponents (e.g., blast shield, microscope lenses), if
necessary, using techniques and cleaning solu- 4.4 Electrical Wiring Configuration. Ensure that
tions recommended by the manufacturer. the branch circuits and the outlets for the laser
are properly wired and rated for use with the
3.2 Lubricate any motor, pump, fan, compressor or laser. Examine the receptacles at each location
printer components as recommended by the where the laser is to be used to ensure that the
manufacturer. proper electrical configuration (e.g., proper
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Argon Surgical Lasers
neutral and ground connections, proper phase output accuracy at several low, medium, and
rotation) has been installed. Verify proper wir- high settings.
ing and connect the laser to each receptacle and
4.9 Laser Delivery System Calibration. Use the
confirm that the laser operates properly, specifi-
manufacturer’s recommended calibration proce-
cally confirming that motors are operating in the
dure to test each new reusable delivery system
proper direction.
(e.g., fiber, handpiece) that the manufacturer
4.5 AC Plug. Verify that the plug is acceptable for indicates can be acceptably calibrated using
use with the maximum current and voltage these procedures. Note the fiber transmission for
specifications for operating the laser. (Consult each delivery system tested if this information is
National Electrical Manufacturers Association provided by the laser. Or, you can calculate it
[NEMA] configurations for general-purpose non- using the following formula:
locking and locking connectors if in doubt.) Delivered power
% Transmission = × 100%
Power entering the fiber
4.6 Pulse Duration. Verify that progressive in-
creases in pulse duration throughout its range of Delivery systems with less than the manufac-
adjustment result in progressively larger burns. turer-recommended transmission (typically
>80%) should be returned to the manufacturer.
4.7 Repeat Pulse. If the unit includes a Repeat Pulse
feature, test this feature as described in Item 2.4, Before returning to use
but over the full range of available settings. Be sure to return controls to their starting position,
and place a Caution tag in a prominent position so that
4.8 Power Range. Using the technique described in the next user will be careful to verify control settings,
the Power Output test (Item 2.10), test the power setup, and function before using the unit.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Procedure/Checklist 433-0595
Aspirators
Used For:
Aspirators [10-208]
Aspirators, Emergency [15-016]
Aspirators, Low-Volume [10-215]
Aspirators, Surgical [10-217]
Aspirators, Thoracic [10-218]
Aspirators, Tracheal [10-219]
Aspirators, Uterine [10-222]
Pumps, Breast [10-485]
Also Called: Portable suction units, gastric aspirators (low-volume aspirators), pleural aspirators (thoracic
aspirators), Gomco (a registered trademark of Allied Healthcare Products, Inc. to be used only when referring
to that device)
Commonly Used In: Ambulances, critical care units, emergency departments, operating rooms; tracheal
aspirators also found on “code carts” and low-volume (or intermittent) aspirators frequently used in
medical-surgical units
Scope: Applies to virtually all electric-powered portable and mobile suction sources; does not apply to suction
regulators (see Procedure/Checklist 459)
Risk Level: ECRI Recommended, High for Emergency and Tracheal Aspirators, Medium for Surgical, Thoracic,
and Uterine Aspirators, Low for Low-volume Aspirators and Breast Pumps; Hospital Assess-
ment, for Breast Pumps, for Emergency Aspirators, for
Low-volume Aspirators, for Surgical Aspirators, for Thoracic Aspira-
tors, for Tracheal Aspirators, for Uterine Aspirators
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months* months . hours
* Emergency and tracheal aspirators only.
Overview Emergency, surgical, and tracheal (high-vacuum)
aspirators, 0 to 200 mm Hg
Aspirators are among the most common types of clinical
Multipurpose high-vacuum aspirators, 0 mm Hg to
equipment in use within the hospital; some (e.g., emer-
>400 mm Hg
gency and tracheal) are critical for life support. Aspira-
tors are categorized by their vacuum levels as follows:
Low-volume aspirators typically operate intermit-
Thoracic aspirators, 0 to 45 mm Hg tently, cycling between atmosphere and 120 mm Hg. In
hospitals with central vacuum systems, suction regula-
Low-volume aspirators, 0 to 150 mm Hg tors are commonly used as an alternative to aspirators.
009008 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
433-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Suction, or aspiration, is used to remove obstructing Flowmeter, 10 to 50 L/min, ±5%
secretions, blood, or vomitus from a patient’s airway to Tubing and adapters for connecting vacuum gauge
keep air passages to the lungs open and to allow or pressure meter and flowmeter (a T fitting is
spontaneous or mechanical ventilation. Suctioning can needed)
be either oropharyngeal (to prepare for emergency
intubation or to remove secretions from the upper Disposable suction canister (if applicable)
airway above the glottis) or tracheal (to remove ob-
structions from the trachea of an intubated patient). Special precautions
Aspirators may be contaminated with contagious
In emergency medical services (EMS) use (in ambu-
microorganisms from contaminated aspirant. Keep
lances and in the field), portable aspirators are usually
your face away from the exhaust port of the unit.
used for oropharyngeal suctioning. However, more and
Never place your mouth on any part of the regulator to
more emergency medical technicians (EMTs) and
blow or suck as a qualitative test of operation or to blow
paramedics are being trained in intubation and ad-
dirt out of a part. Wash hands thoroughly after inspec-
vanced airway maintenance in which, after suctioning,
tion, especially if any accessories were disassembled.
a rescuer intubates the clear airway with an endotra-
cheal tube. Since the cuff of that tube interferes with When it is necessary to disassemble an aspirator for
the natural evacuation of mucus, tracheal aspiration repair, wear latex gloves, wrap cellophane or another
is also used to remove obstructions after intubation. nonpermeable barrier around the handles of all tools, and
Tracheal aspiration may also be required during inter- work on a surface that can be easily disinfected. Dispose
hospital (nonemergency) transport of intubated pa- of gloves and tool handle wrappings as infectious waste.
tients.
Portable emergency aspirators are used by EMS
Procedure
personnel outside the hospital and on bedside stands Before beginning an inspection, carefully read this
in the hospital. They draw power for charging their procedure and the manufacturer’s instruction and serv-
batteries from an AC line, an ambulance DC-to-AC ice manuals; be sure that you understand how to oper-
inverter, or the ambulance’s 12 VDC electrical system. ate the equipment and the significance of each control
and indicator. Also determine whether any special in-
Data gathered during ECRI surveys of hospitals spection or preventive maintenance procedures or fre-
indicate that even serious performance degradation in quencies are recommended by the manufacturer.
suction apparatus is often not apparent to clinical
personnel. This emphasizes the need for periodic in- It is vital to identify the type and/or application of
spection. Critical performance parameters for suction the aspirator to be inspected in order to define the
apparatus are vacuum, vacuum rise, and, in some performance criteria for the inspection. This is often
types, free airflow. A supply of clean catheters, suction difficult because most devices bear only a model or
tips, and tubing should be stored near the aspirator or catalog number. Obtain this information from the
kept readily available. manufacturer’s literature, previous inspection forms,
or clinical personnel. Once the type of aspirator has
Citations from Health Devices been identified or when new units are purchased, enter
this information on the equipment control or inventory
Suction canisters [Evaluation], 1983 Apr; 12:127-49. record so that it can be determined quickly from the
Portable emergency aspirators [Evaluation], 1991 Feb; control number on the device in future inspections.
20:55-72.
1. Qualitative tests
Should vacuum pump effluent be treated? [User Expe-
1.1 Chassis/Housing. Examine the exterior of the
rience NetworkTM], 1994 Jul; 23:310.
unit for cleanliness and general physical condi-
tion. Be sure that housings are intact, that all
Test apparatus and supplies assembly hardware is present and tight, and that
Ground resistance ohmmeter with resolution of 0.1 Ω there are no signs of spilled liquids or other abuse.
Leakage current meter or electrical safety analyzer 1.2 Mount. If the device is mounted on a stand or
Stopwatch or watch with a second hand cart, examine the condition of the mount.
Vacuum gauge, 0 to 760 mm Hg, ±3%, or pressure 1.3 Casters/Brakes. If the device moves on casters,
meter with equivalent capabilities check their condition. Look for accumulations of
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Aspirators
lint and thread around the casters, and be sure If the device has an adjustable suction level,
that they both turn and swivel, as appropriate. verify that the control is usable over the full range
Check the operation of brakes and swivel locks, of vacuum settings. Although generally adjust-
if the unit is so equipped. able over a much wider range, tracheal aspirators
should normally be operated at about 150 mm Hg
1.4 AC Plug. Examine the AC power plug for dam- during tracheal aspiration. Therefore, confirm
age. Attempt to wiggle the blades to determine that the unit is easily adjusted to this vacuum
that they are secure. Shake the plug and listen level (with the patient port occluded).
for rattles that could indicate loose screws.
1.15 Motor/Pump. Confirm physical condition and
1.5 Line Cord. Inspect the cord for signs of damage. proper operation. Lubricate if required, and
If damaged, replace the entire cord or, if the note this on Line 3.2 of the form (but do not
damage is near one end, cut out the defective check 3.2 until you have completed all necessary
portion. Be sure to wire a new power cord or plug lubrication).
with the same polarity as the old one. Also check
line cords of battery chargers. 1.17 Battery/Charger. Inspect the physical condition
of batteries and battery connectors, if readily ac-
1.6 Strain Reliefs. Examine the strain reliefs at cessible. Check operation of battery-operated
both ends of the line cord. Be sure that they hold power-loss alarms, if so equipped. Operate the unit
the cord securely. on battery power for several minutes to check that
the battery is charged and can hold a charge.
1.7 Circuit Breaker/Fuse. If the device has a Check remaining battery capacity by activating
switch-type circuit breaker, check that it moves the battery test function or measuring the output
freely. If the device is protected by an external voltage. Check the condition of the battery charger
fuse, check its value and type against that and, to the extent possible, confirm that it does, in
marked on the chassis, and ensure that a spare fact, charge the battery. When it is necessary to
fuse is provided. replace a battery, label it with the date.
1.8 Tubes/Hoses. Check the condition of all tubing 1.18 Indicators/Displays. During the course of the in-
and hoses. Be sure that they are not cracked, spection, confirm the operation of all lights, indica-
kinked, or dirty. Replace if needed and indicate tors, meters, gauges, and visual displays on the unit
this on Line 3.4 of the inspection form. and charger if so equipped. Inspect the vacuum
gauge for cracks and scale visibility. Make sure the
1.10 Fittings/Connectors. Examine all fittings and indicator resets on zero without vacuum applied.
connectors for general condition. Replace if
needed and indicate this on Line 3.4 of the form. 1.22 Labeling. Check that all necessary placards, la-
bels, conversion charts, and instruction cards
1.12 Filters. Check the condition of all liquid and are present and legible.
pneumatic (air) filters. Replace if needed and
indicate this on Line 3.4 of the form. 1.23 Accessories. Verify that clean canisters, suction
catheters, suction tips, and tubing are available.
1.13 Controls/Switches. Before moving any controls,
check their positions. If any of them appear inordi- 1.24 Overflow Protection. To verify operation of the
nate, consider the possibility of inappropriate clini- overflow protection on units so equipped, liquid
cal use or of incipient device failure. Record the must be aspirated into the collection bottle until
settings of those controls that should be returned to the protective device is activated. (Observe while
their original positions following the inspection. doing so that liquid will not be aspirated into the
pump if the mechanism fails.) Place a bucket of
Examine all controls and switches for physical water on the floor adjacent to the device being
condition, secure mounting, and correct motion. tested, connect a short length of hose to the patient
Where a control should operate against fixed- fitting on the machine, and suction the water into
limit stops, check for proper alignment, as well as the collection bottle. In units with relatively low
for positive stopping. Check membrane switches flow rates (e.g., low-volume aspirators used for
for membrane damage (e.g., from fingernails, gastric suction), this test is expedited by pouring
pens). During the course of the inspection, be sure water directly into the collection bottle until it is
to check that each control and switch performs its nearly full, then reassembling the system and
proper function. suctioning the remainder from the bucket. In
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
devices where overflow protection is provided by
a hollow plastic ball (e.g., a table tennis ball), the Aspirator Performance Values
These performance values represent best current opinion on clinical
ball will not function reliably if it is dented or need and typical aspirator capability, not optimal design criteria. Dis-
cracked or has solids adhering to it. Conduct this cuss units unable to meet these criteria with clinical staff and sched-
ule them for replacement or repair.
test only on units with reusable suction canisters
or overflow mechanisms. Do not test completely Maximum Maximum
Vacuum Rise Time Free Flow
disposable systems. Type (mm Hg) (sec/mm Hg) (L/min)
Emergency >400 <4/300 25
2. Quantitative tests Low Volume >40 <30/30 NA
Surgical >400 <4/300 25
2.1 Grounding Resistance. Using an ohmmeter, Thoracic >40 <4/30 20
electrical safety analyzer, or multimeter with Tracheal >400 <4/300 25
good resolution of fractional ohms, measure and Uterine >400 <3/300 30
Breast Pump >200 <2/150 NA
record the resistance between the grounding pin
of the power cord and exposed (unpainted and
not anodized) metal on the chassis. We recom- this value. If a unit does not provide the ex-
mend a maximum of 0.5 Ω. pected maximum vacuum (see the Aspirator Per-
2.2 Leakage Current. Measure chassis leakage cur- formance Values table above), look for air leaks,
rent to ground with the grounding conductor of especially in the collection bottle caps and hoses.
plug-connected equipment temporarily opened. Some low-volume aspirators have “low” and
Record the maximum leakage current with the “high” settings; record the vacuum attained for
unit off and on. Leakage current should not each, measuring the low level first. Thermal
exceed 300 µA. intermittent aspirators (e.g., Gomco Models
764/5, 200/2000) do not reach maximum vacuum
2.3 Maximum Flow. Measure the maximum free during the first few cycles, and it is necessary to
airflow with the flowmeter and compare it with wait 5 to 10 min until maximum vacuum is
recommended values in the table. (This meas- reached.
urement need not be made on low-volume suc-
2.6 Vacuum Gauge Accuracy. Check the accuracy of
tion machines, since their flows are generally
the vacuum gauges on units so equipped at a
very low.) Set the unit for maximum suction.
vacuum level typical for primary usage. To
Test the aspirator with the collection bottle(s) or
make this measurement, connect the vacuum
canister(s) in place, but without patient cathe-
gauge or pressure meter to the fitting on the
ters. Use a short piece of large-diameter tubing
collection bottle intended for the patient catheter
from the flowmeter to the device, with the correct
or tubing. Turn the unit on and adjust it to the
size adapters inserted at the aspirator end. Any
desired vacuum reading on the machine’s gauge.
restrictions (e.g., internal adapters) will tend to
Record this reading and that of the test gauge or
reduce the free airflow.
meter. Readings should be within 10%.
2.4 Rate of Vacuum Rise. This test is necessary only
on tracheal, emergency, and intrauterine aspira- 3. Preventive maintenance
tors, where rapid vacuum rise is essential. Connect 3.1 Clean the exterior and interior, if needed.
the vacuum gauge or pressure meter to one side of
a T fitting and attach the T to the canister or 3.2 Lubricate the motor and pump, if needed.
collection bottle patient connector. Turn the unit 3.4 Replace filter(s), hoses/tubing, fittings/connec-
on and set the unit for maximum suction. Occlude tors, if needed.
the open port of the T with a finger while using a
stopwatch or watch with a second hand to measure 4. Acceptance tests
the time required to reach maximum vacuum.
Conduct major inspection tests for this procedure
Refer to the Aspirator Performance Values table to
and the appropriate tests in the General Devices Pro-
determine acceptable rise time values.
cedure/Checklist 438.
2.5 Maximum Vacuum. Connect the vacuum gauge
or pressure meter to the canister or collection Before Returning to Use
bottle patient connector. Turn on the aspirator, Recharge battery-powered devices, or equip them
adjust it to provide maximum vacuum, and record with fresh batteries, if needed.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 449-0595
Autotransfusion Units
Used For:
Autotransfusion Units, Blood Processing [17-537]
Also Called: Cell Saver (a registered trademark of Haemonetics Corp. to be used only when referring to
that device)
Commonly Used In: Operating rooms
Scope: Applies to machines used for intraoperative separation and cleaning of red blood cells recovered from
surgical sites
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 6 months months . hours
Minor NA months . hours
Overview During autotransfusion with these machines, blood
that pools in the operative site is aspirated and simul-
Autotransfusion, or autologous transfusion, is the taneously mixed with an anticoagulant, then deposited
process of reinfusing a patient’s own blood rather than in a cardiotomy reservoir. After coarse filtration, the
relying on banked stores of homologous blood. Several blood is either pumped or drained into the spinning
types of intraoperative autotransfusion devices are centrifuge bowl. The lighter plasma separates from
available today. The simpler systems consist of collec- the RBCs and is discarded in a waste bag. Automated
tion canisters or cardiotomy reservoirs that are filled systems monitor the level of RBCs in the bowl with
through suction tubing originating at the operative optical sensors and stop the centrifuge once the cells
site. These systems generally include a means of in- have filled the bowl. In manual operation, the operator
fusing proportioned quantities of anticoagulant as must determine when the centrifuge bowl is full and
blood is aspirated, and a filtration system to remove initiate the next phase of processing, generally the
clotted blood and other debris that may be aspirated RBC wash.
with the blood. Processing systems use a centrifuge to
separate, wash, and pack the red blood cells (RBCs) During the RBC wash, cellular debris from ruptured
extracted from salvaged whole blood. cells, clots, and other contaminants are removed. RBC
washing is accomplished by introducing normal saline
This procedure applies to blood processing systems into the full, spinning centrifuge bowl. Because saline
that employ a centrifuge to separate RBCs from whole is less dense than the RBCs, it disperses the cells and
blood aspirated from the surgical site. Currently mar- rises up through them, carrying debris out and into the
keted units perform essentially the same procedures waste bag. Automated systems will deliver a predeter-
in separating cells from whole blood; differences mined volume of saline during the wash phase; manual
among the units are related primarily to the degree of systems require that the operator monitor the clarity
machine automation. Prices of the units reflect that of the waste leaving the centrifuge bowl. When the
degree of automation. waste fluid is clear, the wash phase is terminated.
084750 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
449-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
The final stage of processing involves pumping the Vacuum gauge, 0 to 600 mm Hg, or pressure meter
packed and washed cells into an infusion bag. The with equivalent capabilities
filled infusion bag is hung with an infusion line and a
microaggregate filter to reinfuse the cells into the The following may be necessary during acceptance
patient. The infusion bags are generally provided testing:
(without infusion lines or filters) with the disposable Citrate solution to anticoagulate 2 L of blood, such
centrifuge bowls and tubing sets for each autotransfu- as 80 g sodium citrate in 200 mL normal saline or
sion machine. CPD (citrate phosphate dextrose) anticoagulant so-
lution (consult with pharmacy to determine correct
While intraoperative autologous transfusion may be concentration)
safer than donor transfusion, which carries the risk of
cross infection and transfusion reactions, autologous 2 L of whole, fresh pig or cow blood anticoagulated
transfusion is not without risk. Some rare complica- with citrate (because of the risk of bloodborne patho-
tions currently associated with autotransfusion in- gens, human blood should not be used for the proce-
clude air embolism, kidney dysfunction, and dures; animal blood may be obtained from a local
disseminated intravascular coagulation. Of these com- slaughterhouse)
plications, the latter two are thought to be related to
blood damage that occurs during the processing. Ex- Special precautions
cessive centrifuge speed, overheating of the blood, and Although the disposable components of the
excessive vacuum applied during aspiration can cause autotransfusion machines are intended to contain
RBC damage. Air embolism has generally been asso- blood during processing, blood may be spilled on the
ciated with the use of pressure infusors for reinfusion machine housing or components during processing.
of recovered cells or infusion occurring concurrently When working on external components (including the
with processing. Some autotransfusion machines are centrifuge well) and the machine housing where blood
equipped with air-in-line detectors that are designed may have been spilled, it is prudent to wear examina-
to detect air in the reinfusion line returning packed tion gloves. If a unit is contaminated with blood,
cells to the patient. (For more details about the risks especially if the blood is still liquid, it should be decon-
associated with autotransfusion, refer to the Health taminated (preferably by a machine operator or central
Devices articles cited below.) supply personnel). Verify that the centrifuge well is
clean before working on the unit. In addition to gloves,
Citations from Health Devices wear a gown and eye protection while the machine is
cleaned. (See Infection Control in the “IPM Safety”
Air embolism from autotransfusion units [Hazard],
article behind the Guidance Tab in this binder for
1986 Jul; 15:210-2.
additional precautions and suggestions.)
Automated intraoperative processing autotransfusion
machines [Evaluation], 1988 Aug; 17:219-42. Procedure
Autotransfusion machines [Evaluation update], 1988 Before beginning the inspection, carefully read this
Dec; 17:371. procedure and the manufacturer’s instruction and
service manuals; be sure that you understand how to
Hemolysis and renal dysfunction associated with operate the equipment, the significance of each control
autotransfusion, 1990 Jan; 19:25-7. and indicator, and the alarm capabilities. Also, deter-
mine if any special inspection or preventive mainte-
Test apparatus and supplies nance procedures or frequencies are recommended by
the manufacturer. For software-driven units, note the
Leakage current meter or electrical safety analyzer
software revision number on Line 1.19 (System Self-
Ground resistance ohmmeter Test) of the inspection form.
Leak-detect solution
1. Qualitative tests
1,000 mL graduated cylinder
1.1 Chassis/Housing. Examine the exterior of the
Stopwatch or watch with a second hand unit for cleanliness and general physical condi-
Bucket with capacity of at least 1 L tion. Be sure that plastic housings are intact,
that all hardware is present and tight, and that
Set of disposables for autotransfusion unit there are no signs of spilled liquids or other
Stroboscopic tachometer serious abuse. (See Special Precautions.)
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Autotransfusion Units
1.3 Casters/Brakes. If the device moves on casters, 1.10 Fittings/Connectors. Examine all gas and liq-
check their condition. Verify that they turn and uid fittings and connectors, as well as electrical
swivel, as appropriate, and look for accumula- cable connectors, for general condition. Electri-
tions of lint and thread around the casters. cal contact pins or surfaces should be straight,
Check the operation of brakes and swivel locks, clean, and bright. Verify that connections are
if the unit is so equipped. Conductivity checks, secure. Gas fittings should be tight and should
where appropriate, are usually done more effi- not leak. (If in doubt, check fittings using a
ciently as part of a check of all equipment and leak-detect solution.)
furniture of an area. (See Procedure/Inspection
Form 441.) 1.12 Filters. Check the condition of all air filters.
Clean or replace as appropriate and indicate this
1.4 AC Plug/Receptacles. Examine the AC power on Lines 3.1 or 3.4 of the inspection form.
plug for damage. Attempt to wiggle the blades
to check that they are secure. Shake the plug 1.13 Controls/Switches. Before changing any con-
and listen for rattles that could indicate loose trols or alarm limits, check their positions. If
screws. If any damage is suspected, open the any settings appear inordinate, consider the pos-
plug and inspect it. sibility of inappropriate clinical use or of incipi-
ent device failure. Record the settings of those
If the device has electrical receptacles for ac- controls that should be returned to their original
cessories, verify presence of line power, insert an positions following the inspection. Some units
AC plug into each, and check that it is held firmly. may store modifications of standard processing
If accessories are plugged and unplugged often, procedures in memory even when the power is
consider a full inspection of the receptacles. shut off; consult the operator’s manual if there is
any question about the effect of changing con-
1.5 Line Cord. Inspect the cord for signs of damage.
trols if they are not set back to their original
If damaged, replace the entire cord or, if the
positions. (If in doubt, have the machine opera-
damage is near one end, cut out the defective
tor review settings before using the unit.)
portion. Be sure to wire a new power cord or plug
with correct polarity. Examine all controls and switches for physical
condition, secure mounting, and correct motion.
1.6 Strain Reliefs. Examine the strain reliefs at
Check that control knobs have not slipped on
both ends of the line cord. Be sure that they hold
their shafts. Where a control should operate
the cord securely. If the line cord is detachable
against fixed-limit stops, check for proper align-
(by the user), affix the cord to the unit so that it
ment, as well as positive stopping. Check mem-
cannot be removed by the operator. (See Health
brane switches for membrane damage (e.g., from
Devices 1993 May-Jun; 22[5-6]:301-3.)
fingernails, pens). During the course of the in-
1.7 Circuit Breaker/Fuse. If the device has a spection, be sure to check that each control and
switch-type circuit breaker, check that it moves switch performs its proper function.
freely. If the device is protected by an external
1.15 Motor/Pump/Fan/Compressor. Check the phy-
fuse, check its value and type against that
sical condition and proper operation of these
marked on the chassis and ensure that a spare
components. Clean and lubricate as required,
is provided.
and note this on Lines 3.1 and 3.2 of the inspec-
1.8 Tubes/Hoses. Check the condition of all tubing tion form. (However, do not check these items
and hoses in the unit. Be sure that they are not until all necessary cleaning and lubrication is
cracked, kinked, or dirty. completed.) Inspect brushes (if present) of
pump, centrifuge, and compressor motors for
1.9 Cables. Inspect any cables and their strain re- wear. If worn, replace. If drive belts are present,
liefs for general condition. Carefully examine check them for wear and replace if needed.
cables to detect breaks in the insulation and to
ensure that they are gripped securely in the 1.18 Indicators/Displays. During the course of the
connectors at each end to prevent rotation or inspection, confirm the operation of all lights,
other strain. Verify that there are no intermit- indicators, meters, gauges, and visual displays
tent faults by flexing electrical cables near each on the unit and charger (if so equipped). Be sure
end and looking for erratic operation or by using that all segments of a digital display function
an ohmmeter. (see Item 1.19).
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
1.19 System Self-Test. Many automated autotransfu- Using the disposable autotransfusion set (or
sion units have a software-based self-check fea- tubing of the same size and hardness), verify that
ture that performs several diagnostic tests when the clamp valves work by installing the tubing
the machine is powered up. Record the software in the valves so that at least 3 ft of tubing is
version on the inspection form when the program available on one side of the valve. With the 3 ft
is started. Verification of proper display and section of tubing held in a vertical position and
indicator function may also be checked during the the clamp valve closed, fill the tubing with water
self-check. to verify that water will not leak through the
valve.
1.20 Alarms. Autotransfusion machines may have
alarms, depending on the degree of automation Next, trigger the valve to open by operating
of the unit. Some alarm conditions that should the unit (consult manufacturer if it is not clear
be checked (where appropriate) include full how to trigger valves to open). If clamps do not
waste bag, empty wash reservoir, and open cen- open or open sluggishly, consult the service man-
trifuge cover. Induce alarm conditions to activate ual or have the manufacturer repair or clean the
audible and visual alarms. Full waste bag valve.
alarms (present on some units) may be triggered 1.25 Centrifuge Chuck. Inspect centrifuge chuck for
by the weight of the bag or by the system’s wear or damage. Inspect entire centrifuge well
volume-accounting system, which keeps track of for presence of debris. Install a centrifuge bowl
how much fluid has been pumped into the waste in the chuck according to the operator’s manual,
bag. Empty reservoir alarms are typically trig- verify that the bowl is firmly seated and that,
gered when the air-in-line detector senses that when the centrifuge is spinning, the bowl re-
no fluid is in the line during the washing phase mains fairly quiet. If the chuck employs O-rings
of processing. (Testing this alarm will also verify to secure the bowl, inspect the O-rings for wear
that the air-in-line detector is functioning.) or nicks; replace as necessary.
Some autotransfusion machines may have cen-
trifuge-cover interlocks that prevent the opening 2. Quantitative tests
of the cover while the centrifuge is spinning; they
may not alarm to warn that the cover is open. 2.1 Grounding Resistance. Using an ohmmeter,
Consult the operator’s manual or the manufac- electrical safety analyzer, or multimeter with
turer to determine if the unit being tested has an good resolution of fractional ohms, measure and
alarm to detect an open centrifuge cover. (None record the resistance between the grounding pin
of the tests in this section will require blood; of the power cord and exposed (unpainted and
water or saline may be used if fluid is required.) not anodized) metal on the chassis. We recom-
mend a maximum of 0.5 Ω. If the system is
1.21 Audible Signals. Operate the device to activate modular or composed of separate components,
any audible signals. Confirm appropriate vol- verify grounding of the mainframe and each
ume, as well as the operation of a volume control, module or component. If the device is double
if so equipped. If audible alarms have been si- insulated, grounding resistance need not be
lenced or the volume set too low, alert clinical measured; indicate “DI” instead of the ground
staff to the importance of keeping alarms at the resistance value.
appropriate level.
If the device has an accessory receptacle,
check its grounding to the main power cord.
1.22 Labeling. Check that all necessary placards, la-
bels, conversion charts, and instruction cards 2.2 Leakage Current. Measure chassis leakage cur-
are present and legible. rent to ground with the grounding conductor of
plug-connected equipment temporarily opened.
1.23 Accessories. Confirm the presence and condition Operate the device in all normal modes, includ-
of accessories, such as tools, separate air-in-line ing on, standby, and off, and record the maxi-
sensors, and cardiotomy reservoir clamps. mum leakage current.
1.24 Clamp Valves. Inspect clamp valves on each Measure chassis leakage current with all ac-
unit, if so equipped, to determine if they are clean cessories normally powered from the same line
and in good condition. If material has accumu- cord connected and turned on and off. This in-
lated on the clamps, clean as needed. cludes other equipment that is plugged into the
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Autotransfusion Units
primary device’s accessory receptacles, as well as 3.2 Lubricate per manufacturer’s instructions.
equipment plugged into a multiple-strip outlet
(“Waber strip”), so that all are grounded through 3.4 Replace motor brushes, drive belts, and centri-
a single line or extension cord. fuge bowl O-rings, as appropriate.
Chassis leakage current to ground should not 4. Acceptance tests
exceed 300 µA. Conduct major inspection tests for this procedure
2.3 Roller Pumps. Check the rollers on pumps to and the appropriate tests in the General Devices Pro-
make sure that they are running smoothly and cedure/Checklist 438. In addition, consider perform-
that there are no unusual noises from bearings ing the following test.
or other indications of excessive bearing wear. 4.1 Cycle Function. If a manufacturer-recom-
Using tubing of the correct size and hardness mended procedure is available, verify that the
in the pump, immerse both ends of the tubing in blood-level detection system (in automated
a bucket of saline solution or water at atmos- units) and the rest of the autotransfusion unit
pheric pressure and turn on the pump. (This functions properly through one or more complete
may require triggering of some sensors for the cycles. For the manufacturer-recommended test
more automated units; contact the manufacturer protocol, contact your representative. If the
if it is not clear how to get the pump to run.) To manufacturer does not provide a way to perform
check pump accuracy, set it to deliver 500 and this test, use pig or cow blood to confirm complete
1,000 mL/min, and collect the volume for a con- functioning; other solutions will not activate sen-
venient time interval in a calibrated 1,000 mL sors. Since there is no history of problems re-
graduated cylinder. Flows should be accurate to ported for new units, testing with animal blood
within 5% of the setting or the manufacturer’s is optional. If the autotransfusion machine is
specifications. new to your clinical staff, and you will be testing
with blood, consider including this testing as
2.4 Vacuum Pump. Check the accuracy of vacuum part of in-service instruction.
pump regulation on units equipped with vacuum
pumps by connecting a length of tubing to the To test with animal blood, install the dispos-
vacuum port and to a vacuum gauge. Vacuum able components, then suction fresh citrated
levels should be within 50 mm Hg of the dis- blood into the collection reservoir. Blood should
played value at full vacuum. be collected in a solution of 8 g of sodium citrate
dissolved in 200 mL of normal saline for every 2
2.5 Centrifuge Speed. Measure centrifuge speed L of blood required. Generally, 2 L of blood is
with a stroboscope tachometer illuminating the more than adequate for testing. Operate the unit
centrifuge bowl chuck while the centrifuge is according to the operator’s manual, verifying that
spinning. A piece of tape may be applied to the the system will detect the packed RBC level.
chuck to facilitate speed determination. Centri-
fuge speed should be within 10% of the specified Before returning to use
speed or within the range specified by the manu-
facturer. If centrifuge speed is outside of accept- Make sure that all controls are set properly. Set
able specification, contact the manufacturer to alarms loud enough to alert personnel in the area in
inquire about adjustment. which the device will be used. Other controls should
be in their normal pre-use positions.
3. Preventive maintenance Attach a Caution tag in a prominent position to alert
3.1 Clean exterior and clamps, as needed. users that control settings may have been changed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 402-0595
Beds, Electric
Used For:
Beds, Air-Fluidized [16-889]
Beds, Birthing [15-732]
Beds, Circle Electric [10-345]
Beds, Electric [10-347]
Beds, Electric, Obese [15-760]
Beds, Flotation Therapy [10-348]
Beds, Low-Air-Loss [17-593]
Beds, Rocking [10-363]
Beds, Tilt [16-991]
Tables, Examination/Treatment [13-958]
Commonly Used In: Most patient care areas
Scope: Applies to electrically operated patient beds, treatment tables (not including OR tables), flotation
therapy beds, turning frames, and a variety of specialty electric beds designed for prevention or treatment
of pressure sores (decubitus ulcers) or burns, with additional tests for special features of these units
Risk Level: ECRI Recommended, Low for most Electric Beds, Medium for Special Care Beds; Hospital
Assessment, for most Electric Beds, for Special Care Beds
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA* months . hours
* Special care beds — including rocking beds (also called kinetic treatment tables), turning frames, circle beds,
and air-fluidized and low-air-loss flotation therapy beds — should receive a minor inspection at least every six
months, in addition to the annual major inspection (see Health Devices 1988 Jan; 17:3).
Overview simple (e.g., bed rails can be checked and repaired
before they fail to restrain a patient; a missing IV pole
Electrically operated beds are in widespread use in can be replaced before it is urgently needed).
most hospitals. Properly used and maintained, they
can provide long service, save much nursing staff time, Inspection of electric beds must be correlated with
and afford the patient comfort and convenience. bed occupancy and coordinated with nursing personnel
or the admissions office. If a bed is occupied at the time
Periodic inspection of electric beds is necessary, its inspection is due and the patient cannot leave the
primarily because of their potential electrical risks. bed for the few minutes required for the inspection,
Electric motors tend to have leakage currents that request that the floor nurse advise the maintenance
increase with age and use, and the line cord, plugs, and department when the inspection can be performed.
control units on beds are often subject to abuse by
patients and personnel. Periodic inspection of all beds, In most hospitals, responsibility for inspection and
nonelectric as well as electric, can often detect impend- preventive maintenance of electric beds rests with the
ing failures at a stage where correction is relatively plant or facilities engineering department, rather than
009032 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
402-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
with clinical engineering. However, because these beds (e.g., walkaway down) that could result in potentially
are also medical devices, it is important that the docu- serious crushing injuries.
mentation of their inspection be thorough and consis-
tent with that of the clinical engineering department. Procedure
Citations from Health Devices Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and
Electrical safety of electrical beds, 1978 Apr-May;
service manuals; be sure that you understand how to
7:152-3.
operate the equipment and the significance of each
Water mattresses on electric beds [Consultant’s Cor- control and indicator. Also determine whether any
ner], 1978 Sep; 7:290. special inspection or preventive maintenance proce-
dures or frequencies are recommended by the manu-
Electric beds in pediatric areas [Consultant’s Corner], facturer.
1982 Sep; 11:302.
Electric beds — A status report, 1983 May; 12:177. 1. Qualitative tests
Electric beds and the pediatric patient [Hazard], 1983 1.1 Frame. Examine the bed frame for cleanliness
Jun; 12:203-7. and general physical condition. Be sure that all
assembly hardware is present and tight. Verify
Hill-Rom electric beds [User Experience NetworkTM], smooth and secure operation of siderails. Check
1986 Jun; 15:177. mechanical integrity and degradation (weld
Electric beds [Evaluation], 1986 Nov; 15:299-316. (See cracks, loose fasteners, caster security, stripped
also Erratum, 1987 Jan; 16:33.) threads), especially on special care beds.
Amedco electric hospital beds [Hazard], 1986 Nov; 1.3 Casters/Brakes. If the bed moves on casters,
15:317-8. check their condition. Look for accumulations of
lint and thread around the casters, and be sure
Electric beds can kill children [Hazard update], 1987 that they turn and swivel, as appropriate. Check
Mar-Apr; 16:109-10. the operation of brakes and swivel locks, if the
bed is so equipped.
Electrical safety of electric beds [User Experience Net-
workTM], 1987 Mar-Apr; 16:118. 1.4 AC Plug. Electric bed plugs are especially sub-
Special care beds require special attention [Hazard], ject to physical abuse. Therefore, carefully ex-
1988 Mar; 17:101-2. amine the plug and use Hospital Grade plugs on
all electric beds. Examine the AC power plug for
Electric beds can kill children [Hazard update], 1989 damage. Attempt to wiggle the blades to deter-
Sep; 18:323-5. mine that they are secure. Shake the plug and
listen for rattles that could indicate loose screws.
Electric beds: Do not use in psychiatric wards [Haz- If any damage is suspected, open the plug and
ard], 1991 Dec; 19:495-6. inspect it.
Test apparatus and supplies 1.5 Line Cord. Inspect the cord for signs of damage.
Leakage current meter or electrical safety analyzer If damaged, replace the entire cord or, if the
damage is near one end, cut out the defective
Ground resistance ohmmeter portion. Be sure to wire a new power cord or plug
Lubricants (20-weight low-detergent oil, graphited with the same polarity as the old one.
oil, grease)
1.6 Strain Reliefs. Examine the strain reliefs at
Special precautions both ends of the line cord. Be sure that they hold
the cord securely.
Keep fingers and clothing away from all moving
parts during inspection. Perform parts inspection, 1.7 Circuit Breaker/Fuse. If the unit has a switch-
cleaning, and lubrication with the power cord un- type circuit breaker, check that it moves freely.
plugged. Never get underneath a bed while the con- If the device is protected by an external fuse,
trols are being operated. Some controls will cause check its value and type against that marked on
continued motion even after the switch is released the chassis, and ensure that a spare is provided.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Beds, Electric
1.9 Cables. Inspect the cables (e.g., pendants, inter- turer that they meet the requirements for pro-
connecting) and their strain reliefs for general tection against tampering set forth in UL 544,
condition. Examine cables carefully to detect Section 23C4. For older beds, check with the
breaks in the insulation and to ensure that they manufacturer to determine the modification pro-
are gripped securely in the connectors of each cedure to disable the feature. This recommenda-
end to prevent rotation or other strain. tion is based on incidents in which children have
been fatally crushed (see Health Devices, 1987
1.10 Fittings/Connectors. Examine all electrical ca-
Mar-Apr; 16:109-10 and 1989 Sep; 18:323-5).
ble connectors for general condition, as well as
Walkaway down capability can be included on
all gas and liquid fittings and connectors, if pre-
four-poster beds.
sent (e.g., in special care beds). Electrical contact
pins or surfaces should be straight, clean, and 1.25 Function and Limits of Patient Controls. Oper-
bright. ate each of the controls in both directions to the
full extent of its limits. Note any unusual sounds
1.13 Controls/Switches. Before moving any controls,
or other deviations from normal performance of
check their positions. Examine all controls and
the controls themselves, the motors, or the lim-
switches, both patient and nurse actuated, for
its.
physical condition, secure mounting, and correct
motion. Check membrane switches for mem- 2. Quantitative tests
brane damage (e.g., from fingernails or pens).
2.1 Grounding Resistance. Using an ohmmeter,
1.15 Motors/Mechanisms. Inspect for general clean- electrical safety analyzer, or multimeter with
liness, condition, and freedom from accumulated good resolution of fractional ohms, measure and
dirt and lint. Follow manufacturer’s recommen- record the resistance between the grounding pin
dations for lubrication (but do not check Line 3.2 of the power cord and exposed (unpainted and
on the inspection form until all necessary lubri- not anodized) metal on the chassis. We recom-
cation has been completed). mend a maximum of 0.5 Ω.
1.22 Labeling. Check that all necessary placards, la- 2.2 Leakage Current. Measure chassis leakage cur-
bels, and instruction cards are present and leg- rent to the chassis of the unit with the grounding
ible. conductor of plug-connected equipment tempo-
1.23 Accessories. Note the general condition of the rarily opened. Operate the device in all normal
bed and mattress. If the bed should be equipped modes, including on, standby, and off, and record
with an IV pole or a manual handcrank (e.g., the maximum leakage current. Leakage current
stored behind the headboard), verify its presence from the bed frame should not exceed 300 µA.
and condition. The IV pole’s elevating latch or This limit applies whether the bed is used in a
thumbscrew should function easily. Inspect IV general or special care area.
sockets for cleanliness, alignment, and mechani- 2.3 Supplemental Tests. Check any special features
cal integrity. of the particular model for condition and operation.
1.24 Function and Limits of Nurse Controls/Lock-
outs. Operate each of the controls in both direc- 3. Preventive maintenance
tions to the full extent of its limits. Note any 3.1 Clean the exterior and interior (e.g., motors,
unusual sounds or other deviations from normal mechanisms).
performance of the controls themselves, the mo-
tors, or the limits. Verify operation of patient 3.2 Lubricate motors, mechanisms.
lockout switches.
4. Acceptance tests
Pedestal-style electric beds should not have a
walkaway down feature unless the bed has UL- Conduct major inspection tests for this procedure
listed controls. The bed should descend only as and the appropriate tests in the General Devices Pro-
long as the down button is pressed; motion cedure/Checklist 438.
should stop as soon as the button is released.
This applies to all areas of the hospital. If in Before returning to use
doubt about new beds, verify with the manufac- Place the bed in its lowest position.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 454-0595
Blood Pressure Monitors, Electronic Indirect
Used For:
Sphygmomanometers, Electronic [16-157]
Sphygmomanometers, Electronic, Automatic [16-173]
Sphygmomanometers, Electronic, Manual [16-174]
Also Called: Noninvasive blood pressure (NIBP) units
Commonly Used In: All patient care areas
Scope: Applies to electronic noninvasive blood pressure monitors with either automatic or manual inflation;
does not include manual sphygmomanometers (see Procedure/Checklist 424) or invasive blood pressure
monitors or transducers (see Procedure/Checklist 434 or 435, respectively); can be used on physiologic
monitoring systems and vital signs monitors that include NIBP measurement
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview provide greater accuracy and permit continuous meas-
urement during cardiac and respiratory cycles, nonin-
Electronic sphygmomanometers noninvasively meas- vasive techniques are most often used because of their
ure and display a patient’s arterial blood pressure. low risk and simplicity, and they have proven suffi-
The use of these devices may help to overcome some of ciently accurate for many clinical applications.
the problems associated with manual sphygmoma-
nometry, such as variations in user techniques and Two primary methods of determining blood pres-
hearing acuity and the difficulty of obtaining measure- sure are used with noninvasive electronic blood pres-
ments on hypotensive patients. In addition, many sure monitors. The auscultatory method uses a
automatic blood pressure units can be programmed for transducer under the occluding cuff to detect arterial
readings at regular intervals and will sound an alarm sounds (Korotkoff sounds) as cuff pressure is gradually
if a patient’s blood pressure exceeds preset limits. lowered from above the systolic pressure. This enables
Some units can display heart rates based on the blood the system to directly determine both systolic and
pressure waveform. diastolic values but not mean arterial pressure (MAP).
Some of these units display a MAP that is calculated
Arterial blood pressure measurement is an essen- from the systolic and diastolic values using an empiri-
tial indicator of physiologic condition. As one of the cally derived algorithm. Hypotensive patients and
most frequently used diagnostic tests, it is critical to patients about to go into shock can be very difficult to
the ongoing management of patients under anesthesia monitor with this method because the Korotkoff
or undergoing drug and other therapies to determine sounds are difficult to detect at low pressures.
the need for blood, a volume substitute (e.g., plasma
expander), or a change in medication. Although inva- The oscillometric method of determining arterial
sive techniques for measuring blood pressure may blood pressure does not require a transducer under the
084753 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
454-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
occluding cuff and is the most common method used. Physiologic monitoring and the standard of care, 1991
This method detects volume displacements that origi- Mar-Apr; 20:79-80.
nate within the artery (as cuff pressure is reduced) and
Physiologic patient monitors [Evaluation], 1991 Mar-
that are sensed as pressure oscillations in the occlud-
Apr; 20:81-136.
ing cuff. The point of maximal oscillation corresponds
to the MAP. Systolic and diastolic pressures may be
determined by special measurement techniques or
Test apparatus and supplies
clinically tested algorithms. This method may be more Leakage current meter or electrical safety analyzer
reliable than auscultation on hypotensive patients and Ground resistance ohmmeter
patients who are likely to become hypotensive.
Calibrated pressure gauge or meter (0 to 300 mm Hg)
A third method, the differential sensor technique, is Y connector compatible with cuff tubing connectors
a composite of the two techniques described above.
Cylindrical object to simulate an arm (e.g., can or
This method typically uses a dual-head sensor that is
pipe) with a 3 in to 4 in outer diameter
located under the occluding cuff. One side of the sensor
is positioned above the artery and detects the signal Stopwatch or watch with a second hand
generated by the Korotkoff sounds and the oscillomet- NIBP simulator
ric pressure wave. The opposite side of the transducer
detects only the oscillometric signal. By subtracting Procedure
these two signals, this method filters out extraneous Before beginning an inspection, carefully read this
signals from the Korotkoff sounds, isolating the signal procedure and the manufacturer’s instruction and
that identifies the systolic and diastolic pressures. service manuals; be sure that you understand how to
The oscillometric method is used to measure MAP, operate the equipment, the significance of each control
even when Korotkoff sounds may be too weak to meas- and indicator, and the alarm capabilities. Also deter-
ure systolic and diastolic pressures. mine whether any special inspection or preventive
There are several oscillometric NIBP simulators on maintenance procedures or frequencies are recom-
the market, costing approximately $4,000 to $5,000. mended by the manufacturer.
These devices attempt to simulate the dynamic signals
1. Qualitative tests
that the occlusive cuff would sense if placed on a patient’s
arm. The devices also have a test mode that can provide 1.1 Chassis/Housing. Examine the exterior of the
an easier means of performing the static accuracy test, unit for cleanliness and general physical condition.
leak test, and overpressure test. If the simulator does not Be sure that plastic housings are intact, that all
use the NIBP monitor’s patient cuff (i.e., the simulator hardware is present and tight, and that there are
has an internal bladder), then the leak test will need to no signs of spilled liquids or other serious abuse.
be repeated with the patient cuff in place.
1.2 Mount/Fasteners. If the device is mounted on a
Simulators also provide a means of evaluating the stand or cart, examine the condition of the
dynamic performance of the NIBP monitor. However, mount. If it is attached to a wall or rests on a
while they are useful in looking at long-term trends of shelf, check the security of this attachment.
device performance, they are not necessarily useful in 1.3 Casters/Brakes. If the device is mounted on a
evaluating device accuracy. Since NIBP monitors calcu- cart or stand, check the condition of its casters.
late their readings based on an algorithm, and the simu- Verify that they turn and swivel, as appropriate,
lators use a similar algorithm to generate their signals, and look for accumulations of lint and thread
if the two algorithms are not exactly matched, then what around the casters. Check the operation of brakes
the simulator states the pressure should be may differ and swivel locks, if the unit is so equipped.
from the pressure that the monitor indicates. It is also
necessary to take several readings at each setting and 1.4 AC Plug. Examine the AC power plug for damage.
average them; this average, over time, should remain Attempt to wiggle the blades to check that they are
constant for each individual NIBP monitor. secure. Shake the plug and listen for rattles that
could indicate loose screws. If any damage is sus-
Citations from Health Devices pected, open the plug and inspect it.
Automatic sphygmomanometers [Evaluation], 1986 1.5 Line Cord. Inspect the cord for signs of damage.
Jul; 15:187-208. (See also 1986 Aug; 15:247 and If damaged, replace the entire cord or, if the
1986 Nov; 15:317.) damage is near one end, cut out the defective
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Blood Pressure Monitors, Electronic Indirect
portion. Be sure to wire a new power cord or plug battery is charged and can hold a charge. (The
with correct polarity. Also check line cords of inspection can be carried out on battery power to
battery chargers. help confirm adequate battery capacity.) Check
battery condition by activating the battery test
1.6 Strain Reliefs. Examine the strain reliefs at function or measuring the output voltage. Con-
both ends of the line cord. Be sure that they hold firm the operation of a charging indicator. Be
the cord securely. sure that the battery is recharged or charging
1.7 Circuit Breaker/Fuse. If the device has a switch- when the inspection is complete. If it is necessary
type circuit breaker, check that it moves freely. If to replace a battery, label it with the date.
the device is protected by an external fuse, check
1.18 Indicators/Displays. During the course of the
its value and type against that marked on the
inspection, confirm the operation of all lights,
chassis and ensure that a spare is provided.
indicators, meters, gauges, and visual displays
1.8 Tubes/Hoses/Bulbs. Check the condition of all on the unit. Be sure that all segments of a digital
tubing, all hoses, the cuff, and the bulb (if pre- display function.
sent). Be sure that they are not cracked, kinked,
1.19 User Calibration. Verify that the calibration
or dirty. Replace loose or cracked tubing.
function operates.
1.10 Fittings/Connectors. Examine all fittings and
1.20 Alarms. Induce alarm conditions to activate
connectors for general condition. Fittings
audible and visual alarms. Check that any asso-
should be tight (or within manufacturer’s speci-
ciated interlocks (e.g., auto deflate) function. If
fications) and should not leak. If keyed connec-
the unit has an alarm-silence feature, check the
tors are used, make sure that the keying is
method of reset (i.e., manual or automatic)
correct.
against the manufacturer’s specifications. It
1.11 Transducers (non-oscillometric units). Confirm may not be possible to check out all alarms at
that any necessary transducers are on hand and this time, since some may require abnormal op-
check their physical condition. erating conditions that will be simulated later in
this procedure.
1.13 Controls/Switches. Before changing any con-
trols or alarm limits, check their positions. If 1.21 Audible Signals. Operate the device to activate
any settings appear inordinate (e.g., alarm limits any audible signals. Confirm appropriate vol-
at the ends of their range), consider the possibil- ume, as well as the operation of a volume control,
ity of inappropriate clinical use or incipient de- if so equipped. If audible alarms have been si-
vice failure. Record the settings of those controls lenced or the volume set too low, alert clinical
that should be returned to their original posi- staff to the importance of keeping alarms at the
tions following the inspection. appropriate level.
Examine all controls and switches for physical 1.22 Labeling. Check that all necessary placards, la-
condition, secure mounting, and correct motion. bels, conversion charts, and instruction cards
Check that control knobs have not slipped on are present and legible.
their shafts. Where a control should operate
1.23 Accessories. Use of an improperly sized cuff can
against fixed-limit stops, check for proper align-
cause significant errors in measuring blood pres-
ment, as well as positive stopping. Check mem-
sure. Clinical personnel should be instructed
brane switches for membrane damage (e.g., from
never to substitute an improper cuff. Verify that
fingernails, pens). During the course of the in-
appropriate cuff sizes either are stored with the
spection, be sure to check that each control and
unit or are readily available (e.g., at a nearby
switch performs its proper function.
nursing station). These should correspond to
1.15 Pump. Check the physical condition and proper physical characteristics of the patients on whom
operation of this component. the instrument is likely to be used (e.g., smaller
cuffs in a pediatric area).
1.17 Battery. Inspect the physical condition of batter-
ies and battery connectors, if readily accessible. All cuffs should be clean and in good condition
Check operation of battery-operated power-loss with no torn stitching. Look for signs of degra-
alarms, if so equipped. Operate the unit on bat- dation or cracking of the bladder. Check that
tery power for several minutes to check that the Velcro closures hold firmly.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
If the unit has a printer/recorder, check to see
that it operates when it is supposed to, that the
paper folds smoothly, and that the printout is
accurate and legible.
1.24 Deflation Switch. Confirm the operation of the
control that enables manual deflation.
1.25 Operation on Volunteer. Apply the cuff to your-
self or a volunteer, activate the unit, and verify
that it cycles through the measurement cor-
rectly. Perform Item 2.4 at the same time (for
major inspection).
2. Quantitative tests
2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with
good resolution of fractional ohms, measure and
record the resistance between the grounding pin Figure 1. Test setup.
of the power cord and exposed (unpainted and
not anodized) metal on the chassis. We recom- 2.4 Heart Rate. Connect the cuff to yourself or a
mend a maximum of 0.5 Ω. If the system is volunteer. Displayed heart rate should corre-
modular or composed of separate components, spond to manually palpated rate within 10%.
verify grounding of the mainframe and each
module or component. If the device is double 2.10 Pressure Accuracy. Connect the blood pressure
insulated, grounding resistance need not be set to a pressure gauge or meter as shown in
measured; indicate “DI” instead of the ground Figure 1. Inflate the system to around 200 mm
resistance value. Hg with either the squeeze bulb or the unit’s
calibration mode. The readings on the unit and
2.2 Leakage Current. Measure chassis leakage cur- the standard gauge should not differ by more
rent to ground with the grounding conductor of than 3 mm Hg. Repeat the test for a pressure
plug-connected equipment temporarily opened. around 120 mm Hg and 80 mm Hg.
Operate the device in all normal modes, includ-
ing on, standby, and off, and record the maxi- 3. Preventive maintenance
mum leakage current. 3.1 Clean as needed.
Chassis leakage current to ground should not 3.2 Lubricate per manufacturer’s instructions.
exceed 300 µA.
3.3 Calibrate per manufacturer’s instructions.
2.3 Air Leakage. Wrap the cuff around a simulated
limb. Inflate the cuff (use the calibration func- 3.4 Replace tubing, hoses, connectors, cuffs, and bat-
tion) to about the maximum scale indication. teries if needed.
Read the indicator after 1 min to determine the
rate of pressure loss in mm Hg/min. This rate 4. Acceptance tests
should not exceed 15 mm Hg/min. If it does, Conduct major inspection tests for this procedure
recheck all fittings and repeat the test. and the appropriate tests in the General Devices Pro-
cedure/Checklist 438. In addition, perform the follow-
If a unit does not allow testing this way, an ing test.
alternative leakage measurement can be used.
Wrap the cuff around a simulated limb. Connect 4.1 Accuracy on Volunteer. Check the unit’s per-
the blood pressure set to a calibrated gauge or formance by comparing measurements made by
meter as shown in Figure 1. The deflation rate a nurse to the blood pressure readings with the
should be 2 to 6 mm Hg/sec, unless the device has unit. The nurse’s reading and the unit’s reading
an algorithm that interpolates the reading be- should not differ by more than 10% mm Hg.
tween pulses. If the rate is faster, check all Differences in readings may be due to technique,
fittings and repeat the test. cuff location (i.e., right or left arm), and time (if not
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Blood Pressure Monitors, Electronic Indirect
taken simultaneously). If significant differences Before returning to use
are obtained on repetitive tries, consider having
another qualified person obtain the manual Make sure that all controls are set properly. Set
reading before contacting the manufacturer. alarms loud enough to alert personnel in the area in
which the device will be used. Other controls should
4.2 Auto Deflate Function. Using the simulated be in their normal pre-use positions.
limb setup in Figure 1, inflate the cuff to the
point of auto deflation activation. It should de- Recharge battery-powered devices or equip with
flate at a point no higher than 330 mm Hg. fresh batteries if needed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 434-0595
Blood Pressure Monitors, Invasive
Used For:
Pressure Monitors, Blood, General/Invasive [16-764]
Manometer Sets, Venous, Central/Peripheral [10-776]
Commonly Used In: Special care units, emergency department, operating rooms, cardiac catheterization
laboratories; often included as a component of physiological monitoring systems
Scope: Applies to invasive blood pressure monitors and is adaptable to other physiologic pressure monitors
(e.g., uterine pressure monitors used in conjunction with fetal heart monitors) that use the same measurement
principles; does not apply to noninvasive, indirect manual blood pressure measuring units (see Proce-
dure/Checklist 424) or electronic indirect blood pressure monitors (see Procedure/Checklist 454); blood
pressure transducers are covered in Procedure/Checklist 435
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview Electrical isolation of blood pressure channels [User
Experience NetworkTM], 1986 Dec; 15:331.
Monitoring blood pressure in addition to the ECG
provides a more comprehensive view of cardiovascular Test apparatus and supplies
status than the ECG alone can provide. However,
invasive blood pressure monitoring requires more skill Leakage current meter or electrical safety analyzer
and involves greater risk. Blood pressure monitors are Ground resistance ohmmeter
used to monitor systolic, diastolic, or mean arterial
Transducer simulator
pressures, central venous pressures, and pulmonary
artery wedge pressures. Transducer connector (without transducer at-
tached) or small-diameter probe for leakage current
meter to gain access to terminals on monitor (accep-
Citations from Health Devices tance testing only)
Blood pressure readings — Cuff versus monitor [Con-
sultant’s Corner], 1977 Jul; 6:236. Procedure
Air embolism during calibration of invasive blood pres- Before beginning the inspection, carefully read this
sure monitoring systems [Hazard], 1982 Nov; 12:22-5. procedure and the manufacturer’s instruction and
service manuals; be sure you understand how to oper-
Alternative in-use calibration techniques, 1982 Nov; ate the equipment, the significance of each control and
12:24. indicator, and the alarm capabilities. Also determine
whether any special inspection and preventive main-
Patient monitoring systems [Evaluation], 1985 Mar- tenance procedures or frequencies are recommended
Apr; 14:143. by the manufacturer.
009009 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
434-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
This procedure is applicable to a stand-alone blood attached to a wall or rests on a shelf, check the
pressure monitor or a pressure module or a section of a security of this attachment.
multiple-parameter physiologic patient monitor. You
need not perform Items 1.2 through 1.7 each time a 1.4 AC Plug. Examine the AC power plug for damage.
different monitoring function of a multiple parameter Attempt to wiggle the blades to determine that
monitor is inspected; these tests are usually performed they are secure. Shake the plug and listen for
during the ECG Monitors inspection (see Proce- rattles that could indicate loose screws. If any
dure/Checklist 409) and are recorded on that form. damage is suspected, open the plug and inspect it.
1.5 Line Cord. Inspect the cord for signs of damage.
For efficiency, test all the monitors in one area with a
If damaged, replace the entire cord or, if the
transducer simulator (these devices were evaluated in
damage is near one end, cut out the defective
Health Devices 1980 Jan; 9:59) or one transducer that is
portion. Be sure to wire a new power cord or plug
known to be accurate; then test all the transducers in
with the same polarity as the old one.
that area (see Procedure/Checklist 435) using one moni-
tor. 1.6 Strain Reliefs. Examine the strain reliefs at
both ends of the line cord. Be sure that they hold
When filling in the identifying information at the the cord securely.
top of the form, include the control or serial number of
the transducer used to test the monitor (unless a 1.7 Circuit Breaker/Fuse. If the device has a switch-
simulator is used). type circuit breaker, check that it moves freely.
If the device is protected by an external fuse,
Testing the accuracy of blood pressure monitors check its value and type against that marked on
and transducers presents a practical problem. Clini- the chassis, and ensure that a spare is provided.
cal requirements for blood pressure measurements
call for an accuracy of ±5% for arterial pressure ranges 1.9 Cables. Inspect the cables (e.g., reusable cables
and ±2 mm Hg for venous or pulmonary pressure for disposable transducers) and their strain re-
measurements. Since the criteria apply to the meas- liefs for general condition. Examine cables care-
urement system, both the monitor and the transducer fully to detect breaks in the insulation and to
must be more accurate than this. Therefore, we rec- ensure that they are gripped securely in the
ommend using a pressure simulator for testing pres- connectors of each end to prevent rotation or
sure monitors. The simulator can be used to test other strain.
monitor accuracy alone, without the need to maintain 1.10 Fittings/Connectors. Verify that the connector
a well-calibrated pressure transducer. Moreover, the for the transducer cable is secure, clean, and lacks
cost of a basic static pressure simulator is less than any signs of damage (e.g., cracks, bent connector
the cost of a pressure transducer. Also, a transducer pins, excessively worn pin receptacles).
alone cannot be used to establish the accuracy of the
monitor. As long as the transducer-monitor combina- 1.11 Transducers. If they are normally stored with
tion is accurate to within 5% or ±2 mm Hg of a given the unit, confirm that transducers are on hand,
static pressure, the monitor and transducer can be and check their physical condition.
considered acceptably accurate. We have found that
1.13 Controls/Switches. Before moving any controls
most pressure monitor and transducer problems re-
and alarm limits, check their positions. If any of
sult in either complete failure of the unit or relatively
them appear inordinate (e.g., a gain control at
large errors.
maximum, alarm limits at the ends of their range),
consider the possibility of inappropriate clinical
1. Qualitative tests use or of incipient device failure. Record the set-
tings of those controls that should be returned to
1.1 Chassis/Housing. Examine the exterior of the their original positions following the inspection.
unit for cleanliness and general physical condi-
tion. Be sure that plastic housings are intact, Examine all controls and switches for physical
that necessary assembly hardware is present condition, secure mounting, and correct motion.
and tight, and that there are no signs of spilled Where a control should operate against fixed-
liquids or other serious abuse. limit stops, check for proper alignment, as well
as positive stopping. Check membrane switches
1.2 Mount. If the device is mounted on a stand or for membrane damage (e.g., from fingernails,
cart, examine the condition of the mount. If it is pens). During the course of the inspection, be
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Blood Pressure Monitors, Invasive
sure to check that each control and switch per- Because some monitors do not compute the
forms its proper function. true mean, the indicated mean value may vary
depending on the waveform and monitor used.
1.18 Indicators/Displays. During the inspection,
confirm the operation of all lights, indicators, 2. Quantitative tests
meters, gauges, and visual displays. Be sure
that all segments of the digital display function. 2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with
1.19 User Calibration. Verify that the zero-adjust-
good resolution of fractional ohms, measure and
ment and any calibration controls function prop-
record the resistance between the grounding pin
erly.
of the power cord and exposed (unpainted and
nonanodized) metal on the chassis. We recom-
Zero the monitor with a transducer or
mend a maximum resistance of 0.5 Ω. If the
transducer simulator attached, making sure
system is modular, verify grounding of the main-
that the zero adjustment is not at an extreme
frame and each module.
setting. Confirm that the calibration function
operates and that the calibration or gain adjust- If the device has an accessory outlet, check its
ment, if user adjustable, provides an adequate grounding to the main power cord.
range on both sides of the correct adjustment
point. 2.2 Leakage Current. Measure the leakage current
from the monitor chassis with the grounding
Some monitors have a calibration resistor in- conductor temporarily opened. Check the moni-
side the transducer cable connector. With such tor while on and off and record the maximum
units, the monitor’s calibration function will not leakage current. Chassis leakage current to
operate with a transducer simulator, which does ground should not exceed 300 µA.
not usually include this calibration resistor. Use
the transducer intended for use with the monitor 2.10 Accuracy, High (Arterial) Pressure Range. This
for this test. test checks the monitor’s accuracy and linearity.
The most convenient method for testing the
1.20 Alarms. Operate the device in such a way as to monitor’s accuracy is with a transducer simula-
activate each audible and visual alarm. If the tor that contains a resistive network. Plug the
monitor has an alarm-silence feature, check the transducer simulator into the monitor and zero
method of reset (i.e., manual or automatic) against it. Test pressures are 100 mm Hg and maximum
the manufacturer’s specifications. Although it (or 200 mm Hg) for the systolic, diastolic, and
may not be possible to verify the operation of all mean arterial modes. Normally, the monitor will
alarms at this time (e.g., high blood pressure), it is read approximately the same in each mode. Re-
important to understand all of the alarm capabili- cord values from only one mode (the least accu-
ties and remember to check them at the appropri- rate), and indicate on the form which mode was
ate time during the procedure. recorded. When using a pressure simulator, the
pressure monitor should measure to within 2%
1.24 Pressure Modes. Verify that the monitor cor- of a given static pressure (or 1 mm Hg at pres-
rectly indicates systolic, diastolic, and mean ar- sures below 50 mm Hg).
terial pressures by switching the transducer
simulator between two pressure settings and Although considerably less convenient, an ac-
noting that the indicated pressure in the systolic curate pressure transducer, a 0 to 300 mm Hg
mode is highest, the mean pressure lower, and pressure gauge or meter, a sphygmomanometer
the diastolic pressure lowest. The pulse pres- squeeze bulb, a Y connector, and tubing may be
sure, if available, should be the difference be- substituted for the transducer simulator. Con-
tween the systolic and diastolic pressures. (A nect the stem of the Y connector to the
more quantitative and reproducible test can be transducer and the Y connector arms to the
performed if a transducer simulator with a dy- sphygmomanometer squeeze bulb and pressure
namic pressure waveform output is available. gauge (see Figure 1). The monitor should be
However, the qualitative test is adequate, and zeroed as it normally is during clinical use (with
we do not recommend purchasing a dynamic the transducer open to atmospheric pressure).
simulator solely for this purpose.) Be sure that the dome is properly attached to the
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
respectively), and test for the actual alarm val-
ues by varying the applied or simulated pres-
sure. Record the actual values on the form.
Alternatively, set appropriate applied or simu-
lated pressures and raise and lower the high and
low alarm settings, respectively, until the alarm
activates. The unit should alarm within 5% of
the set value.
Many monitors have an alarm delay (up to
about 11 sec), which must be taken into account
when conducting this test. If the alarm delay is
excessive, compare it to the manufacturer’s
specification and arrange for adjustment or re-
pair, if appropriate.
Figure 1. Pressure accuracy test
3. Preventive maintenance
transducer, especially if a disposable dome is 3.1 Clean the exterior.
used. Test the monitor as described previously.
4. Acceptance tests
The overall accuracy of the transducer moni- Conduct major inspection tests for this procedure
tor system should be within 5% of a given static and the appropriate tests in the General Devices Pro-
pressure (or 2 mm Hg at pressures below 50 mm cedure/Checklist 438. Determine whether the unit is
Hg). If the error is excessive, determine whether of an isolated input design to decide on appropriate
it is introduced by the transducer, monitor, or leakage current limits from each transducer connector
both by using another transducer (or pressure terminal to ground. If not labeled on the front panel,
simulator) to test the monitor or another monitor check with the manufacturer to see if the monitor is
to test the transducer. rated for this type of isolation test before proceeding.
2.11 Accuracy, Low Pressure Range. Repeat the pres- Perform the isolation test only if your monitor is
sure accuracy test, as described in Item 2.10, for designed with patient input isolation from ground.
the venous and pulmonary ranges. Be sure the Some blood pressure monitors rely upon isolation at
monitor is accurately zeroed in each range before the transducer, rather than having isolated electronic
taking measurements. Suggested test pressures circuitry; performing this test on such a monitor may
are 10 mm Hg and maximum (or 20 mm Hg). damage the unit. If it is of isolated design, measure the
Accuracy should be within 1 mm Hg if a blood currents to each transducer connector terminal.
pressure transducer is used or 2 mm Hg if a
transducer is used. Before returning to use
2.12 Alarm Accuracy. Set the alarm at appropriate Return alarms and other controls to their preinspec-
low and high settings (e.g., 100 and 180 mm Hg, tion settings.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 445-0595
Blood/Solution Warmers
Used For:
Warmers, Blood/Solution [10-447]
Also Called: Blood warmers, fluid warmers, solution warmers
Commonly Used In: Operating rooms, anesthesia departments, emergency departments, critical care areas,
blood banks
Scope: Applies to all types of warmers that heat blood or solutions in-line as they pass from the fluid bag or
infusion device to the patient; does not apply to unregulated water bath warmers (i.e., those with little or no
control over bath temperature) typically used for warming and/or thawing blood products in the clinical
laboratory or to pretransfusion microwave (radio-frequency) warmers
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview circumstances, such as during massive (generally ac-
cepted to be five units or more) and/or rapid transfu-
Blood/solution warmers are typically categorized by the sion, is it widely agreed that blood/solution warmers
method of in-line heat transfer they use to warm incom- should be used. In these applications, effective
ing solutions. Types of heat exchangers include coun- blood/solution warmer operation is crucial.
tercurrent fluid flow, dry heat, forced air, microwave, Should a temperature controller malfunction and
and regulated water bath technologies. Countercurrent allow the blood to overheat, damaged or lysed red blood
devices pump heated water around the blood or solution cells can be delivered to the patient. Although overtem-
in a direction opposite to its flow. Dry heat warmers use perature alarms are considered a necessary feature,
a disposable cassette, pouch, or tubing set positioned some units lack them. Hospitals should replace such
against one or two heated metal surfaces. Forced air units with units equipped with alarms. Failure of the
units utilize convective warming by pumping heated air heater to adequately warm blood could significantly
around a disposable tubing set. Microwave devices con- lower body temperature and further compromise the
trol blood or solution temperature through the use of patient. Thus, periodic inspection of these units is
noninvasive radiometric sensing, allowing immediate particularly important to detect a malfunction likely
power adjustment. Regulated water bath units typi- to escape the user’s attention.
cally consist of a disposable bag or coiled tubing im-
mersed in a controlled temperature bath. Manufacturers should provide fluid output tem-
perature data as a function of flow rate through a
Blood/solution warmers are generally used in the disposable set. Clinicians use such information in con-
operating room by the anesthesia staff. Clinicians sidering the actual contribution of a blood/solution
disagree on when a blood/solution warmer should be warmer to patient thermoregulation. Although not
used for patient thermoregulation. Only under certain required as a routine inspection procedure, assess-
016703 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
445-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
ment of this performance characteristic is covered in unit from use; this may be due to test error or subtle
an acceptance test (Item 4.2). Data from this testing differences in test methods. Contact the manufacturer
should be used in evaluating a unit for purchase. to determine whether such a difference (e.g., >0.5°C
beyond service manual limits) is acceptable.
Citations from Health Devices
Testing alarms and thermostatic settings may re-
Blood warmers [Evaluation], 1984 Jul; 13:191-219. quire disassembly of the unit and temporary modifica-
tion of the wiring. We hesitate to recommend such
Test apparatus and supplies action as part of a routine inspection procedure be-
Ground resistance ohmmeter cause unskilled personnel may inadvertently damage
Leakage current meter or electrical safety analyzer the unit; however, there may be no other way to deter-
mine whether the backup thermostat or overtempera-
A mercury-in-glass calibration thermometer or elec- ture alarms are functional. Unfortunately, for some
tronic thermometer accurate to at least ±0.2°C over units, temporarily bypassing the primary thermostat
the range of 30° to 45°C or similar control is the only way to determine whether
Blood/solution warmer disposable set backup or safety thermostats are functioning properly.
Personnel responsible for inspecting blood/solution
Wire or jumper leads
warmers must recognize their own limitations and,
Silicone heat sink compound or other thermally where appropriate, seek qualified help when perform-
conductive medium (use on thermometer or tem- ing this test. Return the unit to its normal operating
perature probe for better contact with heat ex- condition immediately after completing the test. Per-
changer in dry heat warmers) form the operating temperature test (Item 2.10 or 2.11)
Hot (50° to 60°C) and room temperature water after the temperature protection test (Item 2.3) to help
ensure that the device has been correctly returned to
General-purpose infusion pump and infusion set
its proper operating condition.
Fluid container (0.5 to 1.0 L) filled with refrigerated
(4° to 6°C) saline Procedure
Special precautions Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and
Caution: Treat blood warmers as contaminated de- service manuals; be sure that you understand how to
vices. Follow manufacturer-recommended decontami- operate the equipment, the significance of each control
nation procedures; also see “IPM Safety,” behind the and indicator, and the alarm capabilities. Also deter-
Guidance Tab of this binder, for infection control guide- mine whether any special inspection or preventive
lines. maintenance procedures or frequencies are recom-
Many warmers have special temperature measure- mended by the manufacturer.
ment ports or accessories to assist biomedical person-
nel in determining heat exchanger temperature and 1. Qualitative tests
alarm settings. However, even when properly used, 1.1 Chassis/Housing. Examine the exterior of the
these options may not correctly reflect the actual heat unit for cleanliness and general physical condi-
exchanger temperature, and the measurements ob- tion. Be sure that plastic housings are intact and
tained by these methods will not necessarily agree are not cracked, that necessary assembly hard-
with the unit’s displayed temperatures. When using ware is present and tight, and that there are no
these options during quantitative inspections to deter- signs of spilled liquids or other serious abuse.
mine display accuracy and alarm settings, check the Check that all doors, hinges, and closure mecha-
service manual for correct thermometer or tempera- nisms work properly. Examine the interior sur-
ture probe placement and for allowable differences faces where the disposable set will contact the
between measured and expected readings. Use a sili- heat exchange medium. Remove any corrosion,
cone heat sink compound to improve the contact be- debris, or fungal buildup that may interfere with
tween the thermometer or temperature probe and the the temperature-sensing mechanism or heating
measured surface. Be sure to remove the compound as of fluid in the disposable set.
soon as measurements are completed. If you find a
slightly larger difference than expected between your 1.2 IV Pole Mount. Examine mounting clamps,
measurements and the temperature values provided bolts, and other mechanisms for cracks and a
by the manufacturer, do not immediately remove the secure fit. Verify that a water bath warmer is
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Blood/Solution Warmers
reasonably stable when filled with water and each control and switch performs its proper func-
mounted on the IV pole. tion. If the switch has a protective boot to guard
against fluid infiltration, make sure that the boot
1.3 Base Supports. If the warmer has a freestand- is intact and protects the switch.
ing capability, check that all rubber feet or other
supports are securely in place. Remount or 1.14 Heater(s). If the heater component is readily
reglue any loose supports to ensure stability and available for visual inspection without disassem-
adequate clearance for any components (e.g., bly, examine its physical condition (e.g., corro-
overtemperature alarms, reset features) that sion of its sheath, deteriorated insulation).
may be located on the base of the warmer. Operate the warmer to ensure that it does heat
up and that the display follows a reasonable
1.4 AC Plug. Examine the AC power plug for dam- pattern of increasing temperature. If the unit
age. Attempt to wiggle the blades and determine has an indicator light to show that the heater is
whether they are secure. Check for fluid infiltra- operating, check that it functions normally.
tion in the plug. Shake the plug and listen for
rattles that could indicate loose screws. If any 1.18 Indicators/Displays. During the course of the
damage is suspected, open the plug and inspect inspection, confirm the operation of all lights,
it fully. indicators, meters, gauges, and visual displays
on the unit. Be sure that all segments of a digital
1.5 Line Cord. Inspect the cord for signs of damage. display function.
If damaged, replace the entire cord or, if the
damage is near one end, cut out the defective 1.20 Alarms. Many warmers have an alarm-test fea-
portion. Be sure to wire a new power cord or plug ture that activates their audible and visual
with the correct polarity. After any modifica- alarms. If so equipped, operate the warmer, ac-
tions, make sure that the line cord is long enough tuate this feature, and ensure operation of the
to preclude the need for an extension cord. high-temperature alarm. Otherwise, circulate
hot water (50° to 60°C) through an installed dis-
1.6 Strain Reliefs. Examine the strain reliefs at posable set, and verify that the alarm activates
both ends of the line cord; be sure that they hold and that the heater cycles off. Most water bath
the cord securely and that they have not become units do not have an alarm-test feature, but the
dislodged from the chassis of the unit. overtemperature alarm can be easily triggered by
1.7 Circuit Breaker/Fuse. If the warmer has a filling the well with hot water (50° to 60°C).
switch-type circuit breaker, check that it moves 1.21 Audible Signals. Operate the device to activate
freely. If the warmer is protected by a fuse, any audible signals. Confirm the adequacy of
check its value and type (as well as those of any alarm volume.
spares provided) against that marked on the
chassis or in the instruction manual. 1.22 Labeling. Check that all necessary placards, la-
bels, conversion charts, and instruction cards
1.11 Temperature Sensor (water bath units). The
are present and legible.
temperature sensor of a water bath unit may be
located at the base of the water well. Inspect its 1.24 Alignment Features for Disposable Sets. Check
sheath or surface for corrosion and mechanical for loose or missing pins, blocked channels, or
integrity. Many units provide some form of pro- missing guides that may hinder placement of the
tection or grid to isolate the disposable set from disposable set. Using the manufacturer’s in-
the temperature sensor and/or heaters. Confirm structions, position the disposable set and check
that the grid is in place and fits properly. Re- that it is secure.
place the grid if it is excessively corroded.
2. Quantitative tests
1.13 Controls/Switches. Examine all controls and
switches for physical condition, secure mount- 2.1 Grounding Resistance. Using an ohmmeter,
ing, and correct motion. Where a control should electrical safety analyzer, or multimeter with
operate against fixed-limit stops, check for good resolution of fractional ohms, measure and
proper alignment, as well as positive stopping. record the resistance between the grounding pin
Check membrane switches for membrane dam- of the power cord and exposed bare (not painted
age (e.g., from fingernails, pens). During the or anodized) metal on the chassis. We recom-
course of the inspection, be sure to check that mend a maximum of 0.5 Ω.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
2.2 Leakage Current. Measure chassis leakage cur- with the displayed temperature to ascertain
rent to ground with correct and reversed polarity proper functioning of the display temperature
wiring and with the grounding conductor tempo- sensors.
rarily opened. Operate the device in all normal
modes, including on (while the heater cycles on (Applying power to some warmers when they
and off) and off, and record the maximum leak- lack a fluid flow through the unit’s disposable set
age current. Leakage current should not exceed may result in temperature overshoot and alarms
300 µA. that make assessing temperature sensor accu-
racy difficult. If, after reading the service man-
2.3 High-Temperature Protection. Determine the ual, you find it necessary to establish a cold fluid
warmer’s various means of protection against flow through the disposable set before proceed-
overheating blood. If the manufacturer has pro- ing, perform Item 2.11 to determine display ac-
vided a detailed method by which backup con- curacy and temperature control.)
trollers and alarms can be tested, follow this
procedure. Otherwise, obtain schematics and/or To determine display accuracy and tempera-
instructions to bypass the primary temperature ture control, position the thermometer or tem-
control (see Special Precautions). perature probe against or within the unit’s heat
exchange medium (some units require special
If there are no procedures available, first by- accessories or have built-in ports for this pur-
pass the primary temperature control in the pose). If possible, position probes at three sepa-
warmer (by shorting or opening it, as appropri- rate points within the heat exchanger and, if
ate) and turn on the warmer so that the heater is necessary, use a silicone heat sink compound to
controlled by the backup mechanism. Follow the establish better thermal contact. (Remember to
manufacturer’s recommended procedure for set- remove this compound and thermometer or tem-
ting up the blood/solution warmer. With the ther- perature probe from the unit when finished.) The
mometer or temperature probe in place within heat exchanger should be at room temperature
the heat exchanger, confirm that alarms go off at before proceeding. Turn the unit on and compare
intended set points and that power to the heater the unit’s displayed temperature with the probe
is cut off at the intended settings. At no time temperature(s) as the unit heats up and reaches
should heat exchanger temperatures exceed 42°C. a steady state. These temperatures should be
The difference between the values for alarm set within 1.0°C during warm-up and within 0.5°C
points and backup control as given by the manu- during steady state. Observe the unit for 5 min
facturer and those observed on the blood warmer at steady state for proper maintenance of heat
temperature display should not exceed 0.5°C. exchanger temperature. Allow a total of 15 to 20
The difference may be greater for some units with min to observe temperatures, because some
alarms and backup control based on a thermostat warmers require 10 to 12 min to warm up and
with a lag. In these cases, check that the unit is reach a stable heat exchanger temperature.
not alarming at a point different from the point
observed in acceptance testing, measure the ac- 2.11 Temperature Controller Performance. (This pro-
tual heat exchanger temperature in several loca- cedure need not be followed if Item 2.10 can be
tions, and ensure that it does not exceed 42°C successfully used to determine accuracy and tem-
upon activation of the alarm. perature control.) Position the temperature probe
Caution: Remove any bypasses installed for this against or within the heat exchanger, using any
test. If any recalibration is carried out involving special adapters or ports designated for this pur-
sealed potentiometer or thermostat screws, reseal pose but insulated from the disposable set. Use
them. When reassembling the unit, reseal the refrigerated (4° to 6°C) saline and maintain a flow
back or bottom plates or panels into place with of 500 mL/hr through the unit with an infusion
silicone compound to prevent fluid infiltration. pump. During heat exchanger warm-up, compare
the temperature displayed on the warmer with the
2.10 Display Accuracy and Temperature Control. thermometer at three separate points. If the probe
Most temperature displays on blood warmers has been successfully insulated from sensing the
indicate heat exchanger temperature, not the temperature of the cold fluid, the display and the
exiting temperature of blood or fluid. Therefore, heat exchanger temperature measurements
in most units, it is necessary to measure only the should be within 1.0°C. Allow the warmer to
heat exchanger temperature and compare it stabilize for 5 min, and compare probe tempera-
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Blood/Solution Warmers
ture with the displayed temperature; the dis- 4.2 Fluid Temperature. (This procedure is optional,
crepancy should be within 0.5°C. Check that the but may be particularly useful in evaluating a
operating range of the warmer, as determined unit for purchase. It can be used to provide fluid
from the display, conforms to values specified by output temperature data as a function of fluid
the manufacturer. flow.)
To assess the warmer’s heating capability, se-
3. Preventive maintenance lect its maximum temperature setting and allow
the unit to stabilize. Monitor and record ambient
3.1 Clean the unit’s exterior and heating plates or
temperature (i.e., 18° to 22°C) for future compari-
bath. Clean debris from door hinges. The inte-
son of results. Use a thermometer or temperature
rior of water bath units should be rinsed and
probe to measure the outflow temperature of
dried after each use.
refrigerated (4° to 6°C) saline at various flow
3.3 Calibrate if needed. rates corresponding to intended clinical applica-
tions or the manufacturer’s recommendations for
use. Fluid temperature measurement should be
4. Acceptance tests at the end of the manufacturer’s disposable set or
Conduct major inspection tests for this procedure at the outlet of any extension tubing required to
and the appropriate tests in the General Devices Pro- accurately simulate a clinical setting. Ideally, the
cedure/Checklist 438. In addition, perform the follow- unit should deliver fluids at 37° to 42°C at the
ing tests. highest flow setting that clinicians expect to use
with this unit. If the unit’s heat exchanger ex-
4.1 Patient Lead Leakage Current. Prime the dis- ceeds 42°C, also measure the output fluid tem-
posable set with saline, and allow a drip flow perature as close to the heat exchanger as
through the warmer. Measure the patient lead possible to verify that it does not exceed 42°C, as
leakage current from a steel-hub hypodermic well. Record all output fluid temperatures and
needle on the distal connector of the administra- the corresponding flows for future reference.
tion set to ground with correct polarity but with
an open grounding pin. Operate the device in all Before returning to use
modes, including on (while the heater cycles on Verify that any control circuits that were bypassed
and off) and off. Patient lead leakage current or deactivated for testing purposes have been returned
should not exceed 100 µA. to their normal operating conditions.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 450-0595
Capnometers and Multiple Medical Gas
Monitors
Used For:
Carbon Dioxide Monitors, Exhaled Gas [16-938]
Multiple Medical Gas Monitors [17-443]
Multiple Medical Gas Monitors, Respired [17-444]
Multiple Medical Gas Monitors, Respired/Anesthetic [17-445]
Also Called: Capnographs, end-tidal CO2 monitors
Commonly Used In: Operating rooms, critical care units, emergency departments; portable units may be
used by EMS
Scope: Applies to monitors that analyze concentrations of respired and/or anesthetic gases, and that may
also be equipped with additional capabilities, such as pulse oximetry or airway pressure and minute and tidal
volume monitoring (inspection of the pulse oximetry capability is covered in Pulse Oximeters Proce-
dure/Checklist 451)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
* Some manufacturers may recommend calibration at a semiannual or monthly interval.
Overview Capnometers, which are battery powered and light-
weight, are suitable for emergency medicine (e.g.,
Carbon dioxide (CO2) monitors (e.g., capnometers) use prehospital use, emergency departments, crash carts)
infrared spectrometry to measure CO2 concentrations. and patient transport. These units are used clinically
Currently, CO2 monitors are used primarily in the to detect esophageal intubation, monitor for and de-
operating room to monitor patients during anesthesia; tect complete loss of ventilation or apnea, and assess
the devices alert physicians to inadequate ventilation respiration.
(i.e., minute volume that is too low), patient circuit
disconnections, and airway leaks. CO2 monitoring can Multiple medical gas monitors (MMGMs) incorporate
also detect ventilator failure and the inadvertent monitoring of several gases, including CO2, along with
placement of the endotracheal tube in the esophagus. other parameters such as pulse oximetry, respiration
rate, and airway pressure. Information provided by
Interest in applying CO2 monitoring to intensive MMGMs is easier to review, and an MMGM’s cost is
care mechanical ventilation is increasing, primarily to lower than the combined cost of the monitors it replaces.
evaluate the effects of changing ventilation modes, of
bronchodilator treatment effectiveness, and of the pa- Two types of MMGMs are available. Respired-gas
tient’s ability to breathe spontaneously after ventilator MMGMs are used in critical care areas to monitor
support is discontinued. ventilation of mechanically ventilated patients and to
084776 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
450-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
assess the adequacy of their parenteral nutrient intake mount. If it is attached to a wall or rests on a
by tracking their metabolic rate. MMGMs that monitor shelf, check the security of this attachment.
respired and anesthetic gases are intended for use in
the OR and can indicate malfunctions or disconnec- 1.4 AC Plug. Examine the AC power plug for damage.
tions in the gas delivery system and abnormalities in Attempt to wiggle the blades to check that they are
the uptake, removal, and delivery of gases. secure. Shake the plug and listen for rattles that
could indicate loose screws. If any damage is sus-
pected, open the plug and inspect it.
Citations from Health Devices
Carbon dioxide monitors [Evaluation], 1986 Sep-Oct; 1.5 Line Cord. Inspect the cord for signs of damage.
15:255-85. (See also 1986 Nov; 15:316.) If damaged, replace the entire cord, or if the
damage is near one end, cut out the defective
Marquette Series 7000 capnometer [Update], 1987 portion. Be sure to wire a new power cord or plug
Feb; 16:56. with the correct polarity.
Hewlett-Packard Model 47210A capnometers [User 1.6 Strain Reliefs. Examine the strain reliefs at
Experience NetworkTM], 1987 Jun; 16:219. (See also both ends of the line cord. Be sure that they hold
1987 Jul; 16:251.) the cord securely. If the line cord is detachable
(by the user), affix the cord to the unit so that it
Multiple medical gas monitors, respired/anesthetic
cannot be removed by the operator. (See Health
[Evaluation], 1990 Feb; 20:43-54.
Devices 1993 May-Jun; 22:301-3.)
Test apparatus and supplies 1.7 Circuit Breaker/Fuse. If the device has a switch-
type circuit breaker, check that it moves freely.
Leakage current meter or electrical safety analyzer
If the device is protected by an external fuse,
Ground resistance ohmmeter check its value and type against that marked on
Calibration gas the chassis, and ensure that a spare is provided.
Stopwatch or watch with a second hand 1.9 Cables. Inspect any cables and their strain re-
Flowmeter (0 to 1 L/min air) liefs for general condition. Carefully examine
cables to detect breaks in the insulation and to
ensure that they are gripped securely in the
Special precautions connectors at each end to prevent rotation or
Exposure to waste anesthetic gas can be hazardous. other strain. Verify that there are no intermit-
Gases containing inhalated anesthetics (e.g., N2O, ha- tent faults by flexing electrical cables near each
logenated agents) should be scavenged. end and looking for erratic operation or by using
an ohmmeter.
Procedure
1.10 Fittings/Connectors. Examine gas sample inlet
Before beginning an inspection, carefully read this and exhaust port connectors, as well as electrical
procedure and the manufacturer’s instruction and cable connectors, for general condition. Electri-
service manuals; be sure that you understand how to cal contact pins or surfaces should be straight,
operate the equipment, the significance of each control clean, and bright. Verify that sensors and sam-
and indicator, and the alarm capabilities. Also deter- pling lines are firmly gripped in their appropri-
mine whether any special inspection or preventive ate connectors. Fittings should be tight and
maintenance procedures or frequencies are recom- should not leak.
mended by the manufacturer.
1.11 Sensors/Sampling Lines. Examine these for
1. Qualitative tests general condition. If disposable sampling lines are
used, verify that an adequate supply is available.
1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condition. 1.12 Filters. Check the condition of all gas (air) fil-
Be sure that plastic housings are intact, that all ters. Clean or replace if appropriate, and indicate
hardware is present and tight, and that there are this on Line 3.1 or 3.4 of the inspection form.
no signs of spilled liquids or other serious abuse.
1.13 Controls/Switches. Before changing any con-
1.2 Mount/Fasteners. If the device is mounted on a trols or alarm limits, check their positions. If any
stand or cart, examine the condition of the settings appear inordinate (e.g., a gain control at
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Capnometers and Multiple Medical Gas Monitors
maximum, alarm limits at the ends of their displays a respiration rate and that the CO2
range), consider the possibility of inappropriate waveform indicates the breaths.
clinical use or of incipient device failure. Record
the settings of those controls that should be 1.19 User Calibration. Verify that the calibration
returned to their original positions following the function operates.
inspection. 1.20 Alarms. Induce each alarm condition with each
procedure below, and verify that the unit acti-
Examine all controls and switches for physical
vates an audible and visual alarm for each alarm
condition, secure mounting, and correct motion.
limit that has been exceeded. If the unit has an
Check that control knobs have not slipped on
alarm-silence feature, check the method of reset
their shafts. Where a control should operate
(i.e., manual or automatic) against the manufac-
against fixed-limit stops, check for proper align-
turer’s specifications. Verify that reset silenced
ment, as well as positive stopping. Check mem-
alarms reactivate within the manufacturer’s
brane switches for membrane damage (e.g., from
specified time. It may not be possible to check out
fingernails, pens). During the course of the in-
all alarms at this time, since some may require
spection, be sure to check that each control and
abnormal operating conditions that will be simu-
switch performs its proper function.
lated later in this procedure.
1.15 Pump. Check the physical condition and proper Gas concentration alarms. Set the gas alarm
operation of the pump. Clean and lubricate if limits so that the concentration in the calibra-
required, and note this on Lines 3.1 and 3.2 of tion gas will exceed the limits (i.e., set the
the inspection form. (However, do not check high-concentration alarm limits below the
these items until all necessary cleaning and lu- calibration gas concentrations and the low-
brication are completed.) concentration alarm limits above the calibra-
tion gas concentrations). Deliver the
1.17 Battery/Charger. Inspect the physical condi-
calibration gas to the monitor. Verify that
tion of batteries and battery connectors, if read-
visual and audible high-concentration and
ily accessible. Check operation of
low-concentration alarms activate.
battery-operated power-loss alarms, if so
equipped. Operate the unit on battery power for Occlusion alarm. Block the sampling line, and
several minutes to check that the battery is observe the alarm.
charged and can hold a charge. (The inspection Other alarms. If the unit indicates any other
can be carried out on battery power to help alarm condition, induce the alarm, and verify
confirm adequate battery capacity.) Check bat- that the alarm condition is indicated by the unit.
tery condition by activating the battery test func-
tion or measuring the output voltage. Check the 1.21 Audible Signals. Operate the device to activate
condition of the battery charger, and to the ex- any audible signals. Confirm appropriate vol-
tent possible, confirm that it does in fact charge ume, as well as the operation of a volume control,
the battery. Be sure that the battery is re- if so equipped. If audible alarms have been si-
charged or charging when the inspection is com- lenced or the volume set too low, alert clinical
plete. When it is necessary to replace a battery, staff to the importance of keeping alarms at the
label it with the date. appropriate level.
1.18 Indicators/Displays. During the course of the 1.22 Labeling. Check that all necessary placards, la-
inspection, confirm the operation of all lights, bels, conversion charts, and instruction cards
indicators, meters, gauges, and visual displays are present and legible.
on the unit and charger (if so equipped). Be sure 1.23 Accessories. Confirm the presence and condition
that all segments of a digital display function of breathing circuit adapters and sampling lines
and that the unit displays waveforms and trend- and, when applicable, water traps and filters.
ing information. Observe a signal on a CRT dis-
play, if present, and check its quality (e.g., 2. Quantitative tests
distortion, focus, 60 Hz noise).
2.1 Grounding Resistance. Using an ohmmeter,
Connect a clean airway adapter and sampling electrical safety analyzer, or multimeter with
line to the unit, and blow several breaths into the good resolution of fractional ohms, measure and
adapter before stopping. Verify that the monitor record the resistance between the grounding pin
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
of the power cord and exposed (unpainted and calibration gas containing that agent to the unit.
not anodized) metal on the chassis. We recom- Record the delivered and displayed agent con-
mend a maximum of 0.5 Ω. If the system is centrations on the inspection form. The display
modular or composed of separate components, should be within 0.25 vol% of the delivered con-
verify grounding of the mainframe and each centration. If the gas concentration display is
module or component. If the device is double inaccurate, calibrate the unit.
insulated, grounding resistance need not be
2.6 Nitrous Oxide (N2O) Concentration Display Ac-
measured; indicate “DI” instead of the ground
curacy. Deliver calibration gas containing N2O
resistance value.
to the unit, and record the delivered and dis-
2.2 Leakage Current. Measure chassis leakage cur- played N2O concentrations on the inspection
rent to ground with the grounding conductor of form. The display should be within 5 vol% or
plug-connected equipment temporarily opened. within 10%, whichever is greater, of the deliv-
Operate the device in all normal modes, includ- ered concentration. If the gas concentration dis-
ing on, standby, and off, and record the maxi- play is inaccurate, calibrate the unit.
mum leakage current.
2.7 Sampling Flow Accuracy. Attach a flowmeter to
Measure chassis leakage current with all ac- the sampling inlet, and verify the sampling flow
cessories normally powered from the same line at the highest flow setting. The flow rate should
cord connected and turned on and off. This in- be within the manufacturer’s specified range. If
cludes other equipment that is plugged into the the manufacturer’s information is unavailable,
primary device’s accessory receptacles, as well as the flow should be within 20% of the flow setting.
equipment plugged into a multiple-outlet strip Calibrate the unit per the manufacturer’s in-
(“Waber strip”) so that all are grounded through structions, if the flow is inaccurate.
a single line or extension cord.
3. Preventive maintenance
Chassis leakage current to ground should not
3.1 Clean if needed, including the internal sampling
exceed 300 µA.
line if specified by the manufacturer.
2.3 Oxygen (O2) Concentration Display Accuracy.
3.2 Lubricate pump if required.
Deliver calibration gas containing O2 to the unit,
and record the delivered and displayed O2 con- 3.3 Calibrate if required per the manufacturer’s in-
centrations on the inspection form. The display structions.
should be within 2 vol% or within 5%, whichever
is greater, of the delivered concentration. If the 3.4 Replace O2 cell, air filters, water traps, and the
gas concentration display is inaccurate, calibrate CO2 absorber, if needed. Record the replace-
the unit. ment date on the O2 cell label before installing it
in the monitor.
Note: Vol% refers to the absolute value ver-
sus % of value. For example, a 5% (of value) error 4. Acceptance tests
at 40 vol% of O2 is the same as a 2 vol% error. Conduct major inspection tests for this procedure
2.4 Carbon Dioxide (CO2) Concentration Display Ac- and the appropriate tests in the General Devices Pro-
curacy. Deliver calibration gas containing CO2 cedure/Checklist 438.
to the unit, and record the delivered and dis-
played CO2 concentrations on the inspection Before returning to use
form. The display should be within 0.4 vol% (±3 Make sure that all controls are set properly. Set
mm Hg) or within 10%, whichever is greater, of alarms loud enough to alert personnel in the area in
the delivered concentration. If the gas concentra- which the device will be used. Other controls should
tion display is inaccurate, calibrate the unit. be in their normal pre-use positions.
2.5 Halogenated Agent Concentration Display Accu- Recharge battery-powered devices or equip them
racy. Select an agent on the monitor, and deliver with fresh batteries if needed.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 446-0595
Carbon Dioxide Surgical Lasers
Used For:
Lasers, Surgical, Carbon Dioxide [16-942]
Also Called: CO2 lasers, surgical lasers, gynecology lasers, ENT lasers, neurosurgical lasers
Commonly Used In: Operating rooms, short procedure areas, physicians’ offices
Scope: Applies to general-purpose CO2 surgical lasers that include an articulating arm, emit mid-infrared energy
at 10,600 nm, and provide sufficient power output to vaporize tissue; also applies to low- and high-power CO2
surgical lasers that are typically used for general surgery, gynecology, ENT, neurosurgery, podiatry, and dermatology
procedures; does not apply to handheld CO2 lasers, other infrared lasers, Nd:YAG and argon lasers, and ophthalmic
lasers; however, many of the tests listed herein can be used or modified for these other lasers
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview General-purpose CO2 surgical lasers have a flowing-
gas laser tube or a sealed or semisealed gas tube.
Energy leaving the laser tube through a partially re-
CO2 lasers are normally checked before each use by the flecting mirror is typically directed into an articulating
laser’s power-on self-test and by user examination of arm. This arm contains a series of hollow tubes con-
the aiming beam and calibration of the system with the nected by knuckles at the ends to allow 360° rotation,
delivery system to be used. This minimizes the need with mirrors in the knuckles to redirect the energy
for frequent additional periodic testing. down the next tube. A laser handpiece or a laser
micromanipulator (used to interface the laser with the
Failure of a CO2 surgical laser can cause patient or surgical microscope) is usually attached to the last
staff injury, an abrupt interruption of a surgical pro- tube of the articulating arm; these attachments focus
cedure, or damage to the laser system. CO2 surgical the energy into a small spot size at a known working
lasers must be meticulously maintained to ensure distance. Because the mid-infrared energy emitted by
proper and safe operation. the CO2 laser is invisible, a second, nontherapeutic
aiming helium-neon (He-Ne) laser emitting visible red
CO2 surgical lasers affect tissue by focusing invis- light simultaneously traverses the articulating arm
ible, far-infrared energy at a sufficient power density to and is focused coincident (i.e., at the same point) with
cause vaporization. This energy heats the water in the the CO2 laser beam. Some newer lasers have orange or
cells to the boiling point, which in turn vaporizes the yellow aiming beams.
tissue. The wavelength is readily absorbed by water
and has little scatter in tissue. It cannot be transmitted Like most lasers, CO2 lasers are somewhat ineffi-
through liquids (e.g., water, blood). CO2 surgical lasers cient in converting electrical energy from their stan-
are considered good cutting instruments. dard 115 VAC source into laser energy of 0 to 100 W.
042241 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
446-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
As a result, excess heat is generated in the laser tube, Insulating gloves, high voltage (optional)
requiring a cooling system. Some CO2 lasers use air Grounding strap (optional)
cooling, although most use a combination water/air cool-
ing system. Flowing-gas tube lasers require regulation of Special precautions
the pressure and flow of special gas mixtures. Hence,
Inspecting and maintaining lasers is a dangerous as
either an internal or external gas regulation system must
well as necessary process, and far greater care is
be included. Flowing and semisealed lasers typically use
required than with most devices. Personnel who in-
a vacuum pump to maintain tube pressure.
spect or service lasers should receive special training
Citations from Health Devices from the manufacturer or from a qualified alternative
training source.
Lasers in medicine: An introduction, 1984 Jun; 13:151-
78. Laser energy can cause serious injury, particularly
when the internal interlock is overridden or in any
Lasers as investigational devices: Appendix A, 1984 other situation in which the energy does not diverge
Jun; 13:167-9. significantly over long distances. Under some circum-
Lasers: Model policy and procedures statement: Ap- stances, the beam may not diverge significantly, even
pendix B, 1984 Jun; 13:169-71. a full room length or more away from the laser (and
can harm tissue or burn material even at this dis-
Sharplan 733 carbon dioxide surgical lasers [User Ex- tance). Therefore, exercise great care whenever a laser
perience NetworkTM], 1984 Sep; 13:291. beam is accessible. Area security and use of personnel
Surgilase CO2 lasers [Hazard], 1987 May; 16:176. protective devices and practices should be consistent
with hospitalwide laser safety procedures and/or
Lack of pin-indexing on laser gas supplies [Hazard], should be approved by the laser safety committee.
1987 Jun; 16:216.
Wear appropriate laser safety eyewear at all times
Lack of pin-indexing on laser gas supplies [Hazard whenever the laser is in the Operating mode. WARN-
update], 1987 Aug; 16:286. ING: Laser safety eyewear may not protect the wearer
from the aiming system light. Do not stare directly into
Power requirements for Coherent Excelase 55 CO2
the aiming system beam or the therapeutic laser beam,
laser [User Experience NetworkTM], 1989 Oct;
even when wearing laser safety eyewear. Avoid placing
18:365.
the laser beam path at eye level (i.e., when kneeling,
Surgical lasers [Evaluation], 1991 Jul-Aug; 20:239-316. sitting, or standing). (Window covers are not necessary
with carbon dioxide lasers.)
Loose caster screws on Sharplan lasers, 1992 Feb;
21:79. Do not perform these procedures when a patient is
present or when clinical staff is working, and do not aim
Test apparatus and supplies the laser across a path that a person might normally
Leakage current meter or electrical safety analyzer use as a thoroughfare. Furthermore, at minimum, post
doors to the room with appropriate laser safety signs
Ground resistance ohmmeter stating that the laser is in use and that it is unsafe to
Black Delrin block ≥1⁄2″ thick, ≥1″ wide, about 3″ to enter the room without authorization by the service
4″ long; or firebrick person performing the procedure. A second person
should be present, especially during procedures of rec-
Laser beam imaging media (e.g., thermal imaging
ognized risk, to summon help in case of an accident.
paper, thermal imaging plates; wood tongue depres-
sors may be an acceptable alternative) The laser should remain in the Off position when
Laser radiometer (power meter) not in use. When in use, it should be in the
Standby/Disabled mode. Do not switch it to the Oper-
Laser safety signs
ating mode until the procedure is about to begin and
Laser safety eyewear specifically designed for use the laser and its delivery system are properly posi-
with CO2 surgical lasers and of sufficient optical tioned. If the procedure must be interrupted, discon-
density to protect the wearer’s eyes from laser injury nect the laser from line voltage, and remove the laser
Vise with padded jaws or ring stand with padded operation key and store it in a controlled location.
clamp Do not use the laser in the presence of flammable
Outlet test fixture (optional) anesthetics or other volatile substances or materials
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Carbon Dioxide Surgical Lasers
(e.g., alcohol) or in an oxygen-enriched atmosphere and ensure that they have been turned off
because of the serious risk of explosion and fire. Re- after the last use. Examine the exterior of the
move from the working area or cover with flame-resis- unit for cleanliness and general physical con-
tant opaque material all reflective surfaces likely to be dition. Be sure that all housings are intact
contacted by the laser beam. Whenever possible, use and properly aligned, that assembly hard-
a firebrick or other nonflammable material behind the ware is present and tight, that any retractable
target material (e.g., black Delrin) when the laser is to parts slide easily and lock in place if so con-
be activated. A CO2 fire extinguisher should be readily structed, that there are no signs of spilled
available. liquids or other evidence of abuse, and that
there are no obvious signs of water or oil
Some surgical lasers use high voltages (e.g., 20 kV),
leakage.
which can be lethal. Capacitors may store charges
long after the device has been disconnected from line Articulating arm. Examine the exterior of the
voltage. Consult the manufacturer’s recommended articulating arm for cleanliness and general
procedures for servicing high-voltage laser circuits, physical condition. Be sure that all hardware
and avoid contact with any portion of the high-voltage (e.g., laser gas tubing channels) is present, in
circuit until you are certain that the charge has been good condition, and firmly attached. Ensure
drained. In such instances, a good ground must be that the arm is properly counterbalanced and
present; preferably, use a redundant ground strap if maintains its position without any motion af-
you must enter the laser cabinet. When possible, dis- ter it has been moved and released. Ensure
connect the laser from line voltage before entering the that each knuckle of the arm moves easily in
laser cabinet, and use insulated gloves for those proce- each direction. Examine the distal end of the
dures in which contact with a high-voltage source is articulating arm to ensure that the mecha-
possible (and the gloves are not otherwise contraindi- nism (e.g., threads or quick-connect fitting) is
cated). Ensure that equipment intended to be used to in proper working order.
measure, drain, or insulate high voltages carries the
appropriate insulation rating (e.g., above 20 kV). Shutters. If manual shutters for the aiming or
therapeutic laser are accessible, ensure that
Where possible, perform tests with the unit turned they operate smoothly and correctly. Be sure
off. Because of the presence of high voltage, perform to leave the shutter in the proper position for
the Grounding Resistance Test (Item 2.1) before any normal operation.
other item that requires operation of the laser.
Telescoping columns. Examine the exterior of
Report any laser accident immediately to the laser the telescoping column for cleanliness and
safety officer or equivalent, as well as to the hospital general physical condition. Ensure that the
risk manager. column can be adjusted through its full range.
If lubrication is required, note this on Line 3.2
Procedure of the inspection form.
Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and 1.2 Mounts/Holders. Check that the mounts se-
service manuals; be sure that you understand how to curely contain the gas cylinders. Be sure that
operate the equipment, the significance of each control mounts or holders intended to secure the articu-
and indicator, and precautions needed to ensure safety lating arm to the chassis (to protect the arm
and to avoid equipment damage. Also, determine when the unit is not in use) are present, in good
whether any special inspection or preventive mainte- working order, and being used. Similarly, check
nance procedures or frequencies are recommended by mounts or holders for other devices (e.g., exter-
the manufacturer. nal power meters, footswitch).
1. Qualitative tests If the device is mounted on a stand or a cart,
1.1 Chassis/Housing. examine the condition of the mount. Verify that
the mounting apparatus is secure and that all
General. Verify that the key has not been left in hardware is firmly in place.
the laser. (Remove it if it has, and inform
users of the importance of storing the key in a 1.3 Casters/Brakes. Verify that the casters roll and
controlled location.) Examine any external swivel freely. Check the operation of brakes and
gas tanks that may be in use with the laser, swivel locks.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
1.4 AC Plug/Receptacle. Examine the AC power used with. Verify that suitable connectors are
plug for damage. Wiggle the blades to determine supplied so that adapters are not required.
if they are secure. Shake the plug, and listen for
rattles that could indicate loose screws. If you 1.12 Filters. Check the condition of all liquid and air
suspect damage, open the plug and inspect it. filters. Clean or replace filters according to the
manufacturer’s recommendations (e.g., replace
1.5 Line Cords. Inspect line cords for signs of dam- if the pressure drop is >5 psi), and indicate this
age. If a cord is damaged, replace the entire cord in the preventive maintenance section of the
or, if the damage is very near one end, cut out inspection form. Clean or replace air filters and
the defective portion. Be sure to wire a new radiators that are obviously dirty.
power cord or plug with the correct polarity.
1.13 Controls/Switches.
1.6 Strain Reliefs. Examine the strain reliefs at
both ends of the line cord. Be sure that they grip General. Before moving any controls, check and
the cord securely. record their positions. If any position appears
unusual, consider the possibility of inappro-
1.7 Circuit Breakers/Fuses. If the device has a priate use or of incipient device failure. Ex-
switch-type circuit breaker, check that it moves amine all controls and switches for physical
freely. If the device is protected by an external condition, secure mounting, and correct mo-
fuse(s), check its value and type against what is tion. If a control has fixed-limit stops, check
marked on the chassis or noted in the instruction for proper alignment, as well as positive stop-
or service manual. Ensure that a spare is pro- ping. Check membrane switches for tape resi-
vided or readily available. due and for membrane damage (e.g., from
fingernails, pens, or surgical instruments). If
1.8 Tubes/Hoses. Check the condition of all cooling-
you find such evidence, notify users to avoid
system hoses and any other hoses or tubing the
using tape and sharp instruments. During the
laser may have (e.g., drain, gas). Check that they
inspection, be sure that each control and
are of the correct type; that they have not become
switch works properly.
cracked and do not show other signs of signifi-
cant abuse; that they are connected correctly and Remote. Examine the exterior of the control for
positioned so they will not leak, kink, trail on the cleanliness and general physical condition.
floor, or be caught in moving parts; and that they Be sure that plastic housings are intact, that
are secured adequately to any connectors. assembly hardware is present and tight, and
that there are no signs of spilled fluids or other
1.9 Cables. Inspect all cables and their channels or
serious abuse. If the remote control is at-
strain reliefs for general physical condition. Ex-
tached by cable to the laser, ensure that the
amine cables carefully to detect breaks in insu-
cable and any connectors are in good condi-
lation and to ensure that they are gripped
tion. Examine all controls and switches for
securely in the connectors at each end to prevent
general physical condition, secure mounting,
strain on the cable.
correct motion, and intended range of set-
1.10 Fittings/Connectors. Examine all gas and liq- tings. Where a control should operate against
uid fittings and connectors, as well as all electri- fixed-limit stops, check for proper alignment,
cal connectors, for general physical condition. as well as positive stopping. During the
Gas and liquid fittings should be tight and not course of the inspection, be sure to check that
leak. Electrical contacts should be straight, each control and switch performs properly.
clean, and bright. Pin indexed gas connectors
should be present. Ensure that no pins are miss- Footswitch. Examine the footswitch for general
ing and that the keying and indexing for each gas physical condition, including evidence of
to be used is correct. spilled fluids. Footswitches for lasers include
internal switches that activate according to
If other hospital equipment will be attached the depth of pedal depression. It is usually
to the connector, be sure that the connectors possible to feel the vibration caused by clo-
match. Lasers that connect to the central piped sure of the switch, even through a shoe.
medical gas system or to a freestanding medical Check that the internal switch is operating
gas system should have the matching DISS or and that the footswitch does not stick in the
quick-connect fitting for the gas that it is to be On position. Some footswitches include two
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Carbon Dioxide Surgical Lasers
internal switches; in this case, verify the op- information (e.g., pulse or accumulated energy
eration of both. counter), ensure that each display provides the
During the procedure, check to be sure that information expected. Ensure that user prompts
the laser activates consistently when the foot- occur in the proper sequence. Store some sample
switch is depressed. Flex the cable at the information, and verify that it is correct. If a
entry to the switch, and using an ohmmeter, feature to manually reset this information is
check for internal wire breaks that might available, ensure that it works.
cause intermittent operation. During the pro- 1.20 Alarms/Interlocks. Operate the device in a
cedure, check to be sure that the laser acti- manner that will activate the self-check feature,
vates consistently when the footswitch is if present, and verify that all visual and audible
depressed. Confirm that strain reliefs are se- alarms activate according to the manufacturer’s
cure. documentation. If no self-check feature is pre-
Examine the male and female connec- sent, operate the laser in a manner that will
tors for attaching the footswitch to the la- activate each audible and visual alarm; be sure
ser cabinet to be sure that no pins are bent to test only those alarms that will not cause
and that no other damage is present. En- damage to the laser or present an unnecessary
sure that the connector secures acceptably risk of laser beam exposure to yourself or by-
to the laser cabinet. standers.
1.15 Motors/Pumps/Fans/Compressors. Check the If a door or window interlock is used, ensure
physical condition and proper operation of these that it properly deactivates the laser. (Do not
components. If lubrication is required, note this disassemble major parts of the laser to test in-
in the preventive maintenance section of the ternal interlocks.) After deactivating the laser
form. Clean any obvious dust from these and reclosing the door or window, check to be
components. sure that the laser will restart. Be sure to check
the interlocks in all locations where the laser is
1.16 Fluid Levels. Check all fluid (e.g., coolant) lev- used. (For some lasers, the function of the inter-
els. Refill or change the fluid according to the locks can be checked using an ohmmeter.)
manufacturer’s recommendations, and note this
in the preventive maintenance section of the If the laser is equipped with an emergency
form. “kill” switch, test this feature to be sure that it
deactivates the laser and that the laser will
1.17 Battery. If the remote control is battery pow- subsequently restart.
ered, check or replace the battery (periodic pro-
phylactic battery replacement is often preferred 1.21 Audible Signals. Operate the device to activate
to risking battery failure during use). When it is any audible signals (e.g., laser emission, setting
necessary to replace a battery, label it with the change). Check for proper operation, and verify
date. that the signal can be heard in the environment
in which the laser will be used.
1.18 Indicators/Displays. During the course of the
inspection, verify proper operation of all lights, 1.22 Labeling. Check that all placards, labels, and
indicators, meters, gauges, and visual displays instruction cards noted during acceptance test-
on the unit and the remote control. Ensure that ing (see Item 4.3) are present and legible. Check
all segments of a digital display function. Note to see that an instruction manual is kept with
any messages displayed during the power-on the laser or is readily available.
self-test.
1.23 Accessories.
If primary and remote-control indicators and General. Verify that all necessary accessories are
displays can be used at the same time or if control available and in good physical condition. Set
can be switched from one to the other during a up each accessory with the laser to ensure
procedure, operate the laser in a way that will compatibility and proper functioning.
verify that the same information (e.g., settings,
displays) is indicated on both controls. Checking all accessories during a single
inspection and preventive maintenance pro-
If display screens or digital displays are pro- cedure is unnecessary as long as accessories
vided for user prompts or for viewing accumulated are routinely checked by the person(s) respon-
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
sible for laser setup and operation. In addi- are soluble in water. Carefully insert each
tion, many of the accessories are sterile and lens into the micromanipulator, and ensure
would require resterilization before use, mak- that it fits snugly.
ing the laser potentially unavailable. Be sure
Inspect the mechanism used to attach the
to check with the person responsible for
micromanipulator to the microscope to ensure
scheduling the use of the laser before begin-
that all parts are present and that it is in good
ning the procedure.
working order. Connect the micromanipulator to
Handpieces. Examine each handpiece compo- the microscope to check for a secure connection.
nent (e.g., body, tips, lenses) for cleanliness
and general physical condition. Examine in- Inspect the mechanism used to attach the
dividually only those components that are in- micromanipulator to the articulating arm to
tended for removal during normal use and ensure that it is in good working order. Con-
storage. (Do not remove other parts that are nect the micromanipulator to the articulating
press-fit or attached by screws, bolts, or snap- arm to check for a secure connection.
rings.) If lenses are detachable, be sure not to
1.24 Aiming Beam. Activate the aiming beam (with-
touch the lens surface; handle lenses by the
out the therapeutic beam), and verify that it
edges only. Consult the manufacturer’s rec-
produces a round, uniformly bright spot with no
ommendations for the procedures and clean-
halo. For handpieces that provide adjustable
ing agents to use to clean lenses. Avoid
spot sizes, verify that the spot size changes as
exposing the lenses to water, since most CO2
expected and still remains uniform. Check that
lens materials are soluble in water.
the intensity control, if present, does change the
Ensure that major subcomponents of the brightness of the aiming beam. Similarly, check
handpiece, when assembled, are secure. En- pulsing controls to verify that the aiming beam
sure that the mechanisms used to connect the can be pulsed. If several color choices are avail-
handpiece(s) to the articulating arm are in able for the aiming beam, verify that each color
good working order and that they reliably is present and working properly.
secure each handpiece to the arm.
1.25 Gas Regulators. Examine the gas regulators (if
Microscope micromanipulator. Examine the mi- external to the cabinet) for cleanliness and gen-
croscope micromanipulator for cleanliness eral physical condition. Ensure that the gauges
and general physical condition. Be sure to on the regulators are not broken. While per-
handle it by the main body; do not hold it by forming the preventive maintenance items, en-
the joystick, and do not touch the reflecting sure that the regulator and the gauge operate as
lenses in the body. Inspect micromanipulators expected. Verify that the correct gas is attached
provided by both the laser manufacturer and to each regulator. Be sure that a key or wrench
the laser accessory manufacturers. to facilitate changing the gas supply is with the
Ensure that the reflecting lenses are intact unit or readily accessible.
and clean. Consult the manufacturer’s recom-
mendations for the procedures and cleaning 2. Quantitative tests
agents to use to clean reflecting surfaces and
2.1 Grounding Resistance. Use an ohmmeter, elec-
lenses.
trical safety analyzer, or multimeter with good
Examine the joystick to ensure that it is resolution of fractional ohms to measure and
firmly attached and that it freely moves the record the resistance between the grounding pin
reflecting lens. If a finger rest is present, ensure on the power cord and exposed (unpainted and
that it is firmly attached and properly oriented. not anodized) metal on the chassis, accessory
If a zoom focus feature is present, be sure outlet, ground pins, and footswitch. We recom-
that it turns easily and does not slip. Examine mend a maximum of 0.5 Ω. (If the footswitch is
each objective lens to ensure that it is intact of low voltage, grounding is not required.)
and clean. Do not touch the lens surface. Con- 2.2 Leakage Current.
sult the manufacturer’s recommendations for
the procedures and cleaning agents to use to WARNING: Do not reverse power conductors
clean the objective lenses. Avoid exposing the for this or any other test. Improper attachment
lenses to water, since most CO2 lens materials of conductors may damage the laser.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Carbon Dioxide Surgical Lasers
With the laser attached to a grounded power- Repeat Pulse settings, if adjustable. Some laser
distribution system, measure the leakage cur- power meters can react quickly enough to be
rent between the chassis and ground with the used to test this feature of the laser. If you are
unit grounded and ungrounded. The leakage using such a power meter, test the laser to be
current on the chassis should not exceed 300 µA; sure that the correct power is repeatedly deliv-
in no case should it exceed 500 µA. Where it is ered over the correct time period.
greater than 300 µA, ensure that appropriate
If your laser power meter cannot be used for
grounding is present.
this test, use the following alternative test
2.3 Exposure Duration. Some laser power meters method. Set the laser to about 5 W and a 0.1 sec
can measure pulse duration. If the power meters exposure duration with the fiber, handpiece, or
can react to pulse duration (this is the preferred micromanipulator attached, and verify that the
circumstance), test the laser at each setting. Repeat Pulse feature operates as expected by
However, if the laser power meter does not meas- moving the target material slightly between
ure pulse duration, use the following less prefer- each pulse. Be extremely careful to keep hands
able alternative. out of the laser beam path. You should obtain a
series of burn spots of similar density and size as
Place and secure the laser handpiece with the long as you maintain the same handpiece-to-
aiming beam focused on the target material (e.g., tongue-depressor distance and angle relation-
black Delrin, a tongue depressor). With the laser ships for each exposure and as long as the laser
set to about 5 W and the exposure setting at its is operating properly. If the number or duration
minimum duration, activate the laser and create between repeat pulses is adjustable, test that
a burn. Carefully move the target material to setting changes made throughout the range re-
expose a clean area, maintaining the same dis- sult in the expected performance.
tance. Adjust the exposure setting in increments
2.5 Footswitch Exposure Control. Set the output
of 0.1 sec or the next longest duration, and acti-
time for about 5 sec, activate the unit, and re-
vate the laser at each setting. Continue this
lease the footswitch after about 1 sec. Verify that
process until you have tested all exposure set-
the beam turns off when the footswitch is re-
tings, except continuous, and developed a series
leased.
of burns. Compare the burns to verify that pro-
gressively larger burns occurred as the exposure 2.6 Therapeutic and Aiming Beam Coincidence. CO2
duration increased (see Fig. 1). surgical lasers include a He-Ne aiming laser and a
CO2 therapeutic laser. These two lasers should
2.4 Repeat Pulse. If the unit includes a Repeat Pulse create a spot at the same location. (It may be
feature, which repeats the pulse at a fixed or convenient to perform this test in conjunction with
adjustable rate, test this feature with the laser Item 2.7, since all reusable accessories will need to
set at the minimum, median, and maximum be checked for both coincidence and pattern.)
First check beam coincidence and pattern
with the microscope manipulator, since this will
be more sensitive to misalignment and distortion
problems. To check concentricity of the two la-
sers, position the micromanipulator so the lasing
beam is perpendicular to the face of the wooden
tongue depressor and focused to its smallest spot
on the depressor. Circle the spot created by the
aiming laser. With the laser set at about 5 W
and an exposure duration of about 0.5 sec, acti-
vate the therapeutic laser, and compare the burn
created by the therapeutic laser on the tongue
depressor with the circled area. The burn and
the circled area should overlap (although not
necessarily be of the same size), and the center
Figure 1. Tongue depressor with laser burns produced of the burn and the center of the circle should be
during progressive exposure durations in virtually the same location (see Fig. 2). The
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
dirty mirror can disturb the beam pattern sig-
nificantly and can affect the clinical performance
of the laser.
It is possible for the aiming and therapeutic
lasers to appear to be concentric and to develop
an even burn, despite a poor beam pattern; er-
rors in mirror adjustment or dirt on the mirrors
can qualitatively seem to cancel each other. (In
this case, the maximum power [see Item 2.10]
that can be developed usually drops. Comparing
the results of this item’s testing with those of
Item 2.10 can help to pinpoint the source of the
problem.)
Figure 2. Circled He-Ne aiming beam spot (shaded) and Beam pattern can be roughly assessed by
therapeutic laser spot (dark), demonstrating concentric evaluating the uniformity of a burn on a tongue
alignment (left) and poor alignment (right) depressor (as described in Item 2.6) or laser
thermal imaging paper or by using thermal im-
more the centers of the burn and circle diverge, aging plates.
the poorer the alignment, and the greater the
The surface of the thermal imaging plate is
risk that a surgeon will inadvertently irradiate
exposed to an ultraviolet light, and the surface
unintended tissue.
fluoresces. When the therapeutic laser impacts
Lasers using mirrors in articulating arms are the surface, the thermal energy creates a beam
subject to beam wander, in which concentricity pattern that appears as a brown spot. Thermal
of the aiming and therapeutic laser may change imaging plates may provide an indication of
as the physical orientation of the articulating beam pattern but do not provide a permanent
arm (e.g., the angle or degree of rotation of one record for later comparison, may be difficult to
arm section in relation to another section or the view with the aiming beam on, and may be easily
chassis) changes. Hence, repeat this test with damaged if accidentally overexposed. The plates
the articulating arm in several physical configu- are designed to respond to different power den-
rations. If the aiming and therapeutic lasers sities of CO2 laser energy. To minimize the risk
diverge significantly during any test, the system of damaging a plate’s surface, always start with
requires complete alignment. (Alignment is very the least sensitive surface. Also, do not focus the
difficult and should be performed only by quali- beam on the surface.
fied personnel.)
Position the target beyond the point of focus
Repeat this testing with each reusable acces- to expand the spot, thereby decreasing the power
sory, including handpieces, laser laparoscopes, density in the spot. The beam must be perpen-
and laser bronchoscopes. Handpieces can be po- dicular to the target surface. When using laser
sitioned and secured in the vise or ring stand. It paper, the laser should be set at about 5 W and
is not necessary to test the effect of manipulating operated in the Pulsed mode at a 0.1 sec exposure
the articulating arm for each accessory. If a setting or the nearest available setting. The burn
problem is found in beam alignment or pattern (or spot on an imaging plate) should be fairly
without a corresponding problem with the micro- consistent in darkness throughout and circular
manipulator, the source of the problem is prob- in shape (see Fig. 3).
ably in the accessory.
Some laser delivery systems (e.g., microma-
2.7 Laser Beam Pattern. The spot created by a nipulators) provide features that allow the user
therapeutic laser beam perpendicular to the tar- to change the spot size. Measuring absolute spot
get should be circular, and the energy through- size from a laser is difficult, results are not
out the spot should be fairly uniform. Laser beam always comparable, and the cost of equipment
pattern is a measure of how well the mirrors of exceeds the expected benefits to an inspection
the laser tube, articulating arm, and handpiece program. However, measuring relative change
are aligned and performing. A misaligned or in spot size caused, for example, by changing
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Carbon Dioxide Surgical Lasers
Because of the heightened risk associated with an
unfocused, nondiverging laser beam, exercise
great care if the interlocks are to be defeated.
With the laser set at a low (e.g., 10% of full scale),
medium (e.g., 50% of full scale), and maximum
output, activate the laser for a sufficient period to
acquire acceptable readings. (Power meters use
different time constants to acquire an acceptable
reading, and you must know and meticulously
follow the power meter’s instructions for use.)
Compare the reading obtained with the power
display of the laser; the measured and displayed
values should all be within 10% of one another. In
addition, compare the reading with the reading
taken on incoming acceptance testing, at the last
preventive maintenance procedure, or after the
last service procedure; a significant change in out-
Figure 3. Acceptable therapeutic beam pattern (left) and
unacceptable (right) put may indicate the need for service. If the laser
includes a low-power (e.g., mW) feature, test it in
a similar fashion with a power meter of appropri-
lenses or the aperture setting on micromanipu- ate low-power resolution.
lators is worthwhile and can be accomplished
without undue cost. 3. Preventive maintenance
You can evaluate the change in relative spot Verify that all daily preventive maintenance proce-
size using either of the test methods detailed dures recommended by the manufacturer are carried
above (i.e., using a thermal imaging plate or out.
laser paper). If you use different lenses to
change the spot size, expose the thermal imaging 3.1 Clean the exterior. Clean accessible optical com-
plate or laser paper to the focused beam created ponents (e.g., microscope lenses) if necessary,
when using each lens, and compare the relative using techniques and cleaning solutions recom-
spot size, spot shape, and beam uniformity of the mended by the manufacturer.
images or imprints. If you use fixed points or 3.2 Lubricate the telescoping column and any mo-
continuously variable aperture control to change tor, pump, fan, compressor, or printer compo-
the spot size, expose the thermal imaging plate nents with the lubricant recommended by the
or laser paper to the focused beam created when manufacturer.
the aperture control is set at its minimum, me-
dian, and maximum aperture settings. Compare 3.3 Calibrate/adjust any components (e.g., printer)
relative spot size, spot shape, and beam uniform- according to manufacturer recommendations.
ity. Only appropriately trained personnel should at-
tempt laser adjustments. Ensure that all hoses
2.10 Power Output. Place and secure the laser hand- and tubes are tight.
piece or aperture of the articulating arm at the
appropriate distance from the laser power me- 3.4 Replace filters, if needed. Check all fluid levels
ter to meet spot-size requirements specified in and supplement or replace fluids if needed.
the instructions with the meter. (Some power
meters require that the aperture of the articu- 4. Acceptance tests
lating arm be inserted into or placed in direct Conduct major inspection tests for this procedure
contact with the power meter. If the handpiece and the appropriate tests in the General Devices Pro-
is used on these meters, the meter may be dam- cedure/Checklist 438.
aged by the high power density caused by the
focused beam.) WARNING: Lasers may be damaged by switching
between normal and reverse polarity while the device is
WARNING: Accessing the unfocused laser on. If reverse-polarity leakage current measurements
beam may require defeating internal interlocks. are made, turn off the unit being tested before switching
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Inspection and Preventive Maintenance System
polarity. Also, lasers powered by three-phase electrical proper electrical configuration (e.g., proper neu-
systems may be damaged if proper electrical phase tral and ground connections, proper phase rota-
connections are not made initially and maintained tion) has been installed. Connect the laser to
thereafter. Thus, do not switch conductor connections each receptacle and confirm that the laser oper-
or wiring configurations for any tests, including leak- ates properly, specifically confirming that mo-
age current measurement. Do not conduct electrical tors are operating in the proper direction.
leakage current tests with reversed-polarity wiring.
4.5 AC Plug. Verify that the plug is acceptable for
The handpiece (which could conceivably come into use with the maximum current and voltage
contact with a patient’s heart) should meet the criteria specifications for operating the laser. (Consult
for isolated input devices. National Electrical Manufacturers Association
[NEMA] configurations for general-purpose non-
Also test the ability of the laser to deliver laser locking connectors if in doubt.)
energy as expected in all configurations and with all
provided laser accessories. In addition, perform the 4.6 Pulse Duration. If the laser includes an en-
following tests. hanced pulse feature and the pulse duration is
adjustable, verify that progressive increases in
4.1 Areas of Use. Visit the area(s) in which the laser pulse duration throughout its range of adjust-
is to be used, and ensure that laser signs, laser ment result in progressively larger burns.
safety eyewear, and window coverings are avail-
able and being used and that safety interlocks 4.7 Repeat Pulse. If the laser includes a Repeat
for doors or windows, if present, are functioning Pulse feature, test this feature as described in
properly. Item 2.4, but over the full range of available
settings.
4.2 Casters/Mounts/Holders. Ensure that the as-
sembly is stable and that the unit will not tip 4.8 Power Range. Test the power output accuracy,
over when pushed or when a caster is jammed on using the technique described in Item 2.10, at
an obstacle (e.g., a line cord threshold), as may several low, medium, and high settings. If the
occur during transport. If the device is designed laser includes an enhanced pulse feature, verify
to rest on a shelf, ensure that it has nonslip legs that adjusting the power setting incrementally
or supports. through its full range produces the expected
effect on a tongue depressor. For all tests using
4.3 Labeling. Examine the unit and note the pres- high continuous-wave or Superpulse, it is par-
ence, location, and content of all labels. Labeling ticularly important to use a firebrick behind the
information is typically found in the laser’s op- tongue depressor for added safety.
erator manual.
4.4 Electrical Wiring Configuration. Ensure that Before returning to use
the branch circuits and the outlets for the laser Be sure to return controls to their starting position,
are properly wired and rated for use with the and place a Caution tag in a prominent position so that
laser. Examine the receptacles at each location the next user will be careful to verify control settings,
where the laser is to be used to ensure that the setup, and function before using the unit.
Inspection and Preventive Maintenance System
10 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 421-0595
Cardiac Resuscitators
Used For:
Resuscitators, Cardiac [13-361]
Also Called: External cardiac compressor, Thumper (registered trademark of Michigan Instruments, Inc., to
be used only when referring to that device)
Commonly Used In: Emergency departments, critical care areas, ambulances
Scope: Applies to cardiac resuscitators; does not apply to cardiac presses that are not pneumatically powered
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
*An interval of 6 months should be considered if a resuscitator is frequently used and/or located in an ambulance.
Overview Test apparatus and supplies
Pneumatically powered cardiac resuscitators are used Pressure gauge or meter with a range of at least
during emergency cardiopulmonary resuscitation 0 to 80 cm H2O
(CPR) as an alternative to manual cardiac compres-
Spirometer or gasometer
sion. They can provide consistent cardiac compression,
with adequate sternal depression and rhythmic com- Beam balance patient floor scale
pression rates, as well as oxygen-enriched ventilation.
Stopwatch or watch with a second hand
By eliminating the need to rotate personnel for the
fatiguing task of cardiac compression, these devices Ruler
reduce the number of people required to maintain
support of the patient. Special precautions
Use of pneumatically powered cardiac resuscita- Never oil any part of an oxygen-powered cardiac
tors does not eliminate the need to train hospital and compressor. Oil in the presence of oxygen is a danger-
ambulance personnel in effective airway mainte- ous fire and explosion hazard.
nance, manual external cardiac compression, and
mouth-to-mouth breathing. In all cases, the patient
must be maintained by manual techniques until the
Procedure
cardiac resuscitator is available, applied, and placed Before beginning an inspection, carefully read this
in operation. procedure and the manufacturer’s instruction and serv-
ice manuals; be sure that you understand how to oper-
Citations from Health Devices ate the equipment and the significance of each control
and indicator. Also determine whether any special in-
External cardiac compressors [Evaluation], 1973 Apr; spection or preventive maintenance procedures or fre-
2:136-50. quencies are recommended by the manufacturer.
009010 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
421-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
1. Qualitative tests make it more versatile for a wider range of
patients.
1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condi- Use only transparent masks with resusci-
tion. Be sure that plastic housings are intact, tators. If opaque masks are in use, order
that all assembly hardware is present and tight, transparent replacements but do not remove
and that there are no signs of spilled liquids or opaque masks from use until replacements
other serious abuse. are available and the change has been dis-
cussed with users.
1.2 Mount. If the device is mounted on a stand or
Inspect the masks for signs of deterioration.
cart, examine the condition of the mount.
Reinflate inflatable rims if they are collapsed,
1.8 Tubes/Hoses. Check the condition of all tubing and check for leaks or damage by immersing the
and hoses. Be sure that they are not cracked, mask in water. Replace if necessary.
kinked, or dirty.
1.24 Ventilation Hose Fitting. Verify that the venti-
1.10 Fittings/Connectors. Confirm that appropriate lation hose terminates at the patient end in a
quick-connect fittings are being used with corre- standard 15/22 mm coupling to allow connection
sponding gases. Observe that pin-index safety to a standard ventilator mask and tracheal or
system pins are present and intact. tracheostomy tube. If it does not, an adapter
should be provided.
1.13 Controls/Switches. Before moving any controls,
check their positions. If any of them appear 2. Quantitative tests
inordinate, consider the possibility of inappro-
priate clinical use or of incipient device failure. 2.3 Compression Rate with Ventilation. Using a
Record the settings of those controls that should stopwatch or watch with a second hand, count the
be returned to their original positions following number of compressions over a 1 min period. If
the inspection. the unit includes a ventilator, count the number
of compressions per minute with it operating. The
Examine all controls and switches for physical compression rate, unless otherwise specified by
condition, secure mounting, and correct motion. the manufacturer, should be in accordance with
Where a control should operate against fixed- AHA/ARC two-person CPR standards (i.e., 60 to
limit stops, check for proper alignment as well as 80/min).
positive stopping. During the course of the in-
spection, be sure to check that each control and 2.4 Piston Displacement. With the unit not operat-
switch performs its proper function. ing, check that the compression piston moves
freely in and out of its cylinder. The maximum
1.18 Indicators/Displays. During the course of the displacement should not exceed 5 cm (2 in).
inspection, confirm the operation of all indica-
tors, gauges, and visual displays on the unit. 2.5 Compression Force. Position the compression
piston on the weighing platform of a conven-
1.22 Labeling. Check that all necessary placards, la- tional patient floor scale by tilting the scale back
bels, conversion charts, and instruction cards and sliding the compressor base plate under the
are present and legible. platform. If the scale is at a significant angle
from its original position, use blocks or other
1.23 Accessories. List the accessories that are to be
objects to level it again.
stored with each resuscitator. Check that the
items on the accessories list are found with the Connect the compressor to its normal oxygen
resuscitator at each inspection. Examine all acces- source. Set the scale to 45 kg (100 lb) and adjust
sories for cleanliness and mechanical integrity. the compression force control to its maximum
Cylinders. If an oxygen cylinder is stored with point. Activate the compressor. It should raise
the resuscitator, check the amount of oxygen the balance beam.
it contains. Maintain a full cylinder with the
2.6 Ventilator Regulation. Determine if the ventila-
unit. A cylinder wrench should be chained to
tion gauge measures pressure (cm H2O) or vol-
the regulator and yoke assembly.
ume (cc). If the gauge measures pressure,
Masks. An assortment of masks (e.g., adult, in- connect the ventilator output to a pressure gauge
fant) should be stored with the resuscitator to or meter or a water manometer and compare the
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Cardiac Resuscitators
measured ventilation pressure to that indicated setting and measure the maximum inspiratory
on the gauge at 30 and 50 cm H2O. If the gauge volume. It should be at least 1.5 L.
measures volume, connect the ventilator output
to a spirometer or gasometer. Compare the 2.9 Compression/Ventilation Ratio. With the com-
measured ventilation volume to that indicated pressor and ventilator operating, count the
on the unit’s gauge at the 1 L setting. The number of piston thrusts between each venti-
difference between measured and indicated val- lation. There should be five compressions per
ues should not exceed 20%. (Such high errors ventilation.
are tolerable in short-term emergency equip-
ment but would not be acceptable in other venti- 3. Preventive maintenance
lators.) 3.1 Clean the exterior.
2.7 Inspiratory Pressure. Connect the patient end of
the ventilator tubing to a pressure gauge or
4. Acceptance tests
meter. Adjust the ventilator control to its maxi- Conduct major inspection tests for this procedure.
mum setting and measure the maximum venti-
latory pressure. It should not exceed 60 cm H2O. Before returning to use
This test confirms operation of the inspiratory
Make sure controls are set at normal positions and
pressure-relief valve.
oxygen cylinders are turned off. Place a Caution tag
2.8 Ventilator Volume Output. Connect the output in a prominent position so that the next user will be
of the ventilator to a spirometer or gasometer. careful to verify control settings, setup, and function
Adjust the ventilator control to its maximum before use.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 456-0595
Centrifuges
Used For:
Centrifuges [10-778]
Centrifuges, Blood Bank [15-115]
Centrifuges, Cell Washing, Automatic [16-815]
Centrifuges, Cytological [16-765]
Centrifuges, Floor [15-116]
Centrifuges, Floor, Nonrefrigerated [17-177]
Centrifuges, Microhematocrit [10-779]
Centrifuges, Refrigerated [15-117]
Centrifuges, Tabletop [10-780]
Microcentrifuges [17-452]
Ultracentrifuges [15-193]
Commonly Used In: General clinical laboratories, as well as specific laboratory departments (e.g., blood
bank, hematology, clinical chemistry)
Scope: Applies to all types of centrifuges
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview Certain hazards are associated with the operation of
centrifuges. Sample tubes may break; breakage is most
Centrifuges use centrifugal force to separate suspended likely to occur if manufacturers’ instructions, such as
particles from a liquid or to separate liquids of various using correct tube sizes and locations and using cushions,
densities. These liquids can include body fluids (blood, are not followed. Rotors may detach or fail, possibly
serum, urine), commercial reagents, or combinations of because of a loose retaining nut or imbalanced tube
the two with other additives. Centrifugation is used for placement; rotor or tube failures may result in operator
most sample preparations in a clinical laboratory. exposure to physical or infectious hazards. Aerosols may
be created from the samples. Or the operator may be
There are three general classifications of centrifuges: harmed while attempting to slow down or stop the rotor
low speed (≤6,000 rpm), high speed (6,000 to 25,000 rpm), by hand. Therefore, the lid should never be opened while
and ultraspeed (25,000 to 110,000 rpm). These three types the rotor is spinning, and safety inner protective lids
of centrifuges are available as tabletop and/or floor models, should be used when available.
and some are refrigerated units. Microhematocrit centri-
fuges are specialized centrifuges used in a hematology Hazards also exist when the centrifuge is not in
department to determine an accurate packed cell volume operation; for example, broken glass, possibly contami-
of red blood cells. The speed of a microhematocrit centri- nated with blood, may be found inside the centrifuge
fuge ranges from 7,000 to 15,000 rpm. during cleaning or IPM.
236945 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
456-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
In addition to careful adherence to use and mainte- Electronic thermometer accurate to 0.5°C (for
nance instructions, equipment with appropriate safe- refrigerated units only)
guards should be used. As a minimum, units should
Tachometer or phototachometer
have a lid and a latch that will prevent the lid from
opening in the event of a failure while the rotor is
spinning. A safety interlock, which permits the lid to
Special Precautions
be opened only after the rotor has stopped (or reached Check with laboratory personnel before performing
a very low speed), is preferred, and all new units should any maintenance or shipping centrifuges to the manu-
have this feature. facturer for repair. Laboratory personnel should have
properly decontaminated the centrifuge. A centrifuge
Laboratory personnel are required by the College of
should be vacuumed out before any testing is started.
American Pathologists (CAP) to do the following:
(Broken glass, which may be contaminated with blood,
Clean and properly maintain all centrifuges. (Note: is sometimes found inside. In addition, visible blood
Contact the manufacturer for guidance if the opera- may be located on or in the centrifuge.)
tor’s manual does not specify cleaning or disinfect-
ing agents. Prolonged contact with some Be careful not to touch a spinning rotor if an inter-
disinfection solutions [e.g., 10% sodium hypo- lock fails or if you are operating the unit with the lid
chlorite] may damage the rotor and other centrifuge open. NEVER attempt to stop a moving rotor with your
components; ensure that such solutions are re- hands or with a tool or object.
moved by rinsing well with water.)
Ensure that the centrifuge tubes are properly bal-
Check and record timer accuracy monthly. anced and that the speed and tube length are in accord-
Check and record speed (rpm) accuracy monthly ance with the tube and centrifuge manufacturers’
(critical use) or quarterly. recommendations. Use proper-sized tubes for the ro-
tor. If using a swinging-bucket rotor, ensure that the
Check and record built-in tachometer monthly.
tubes are placed in accordance with the manufac-
(Note: Operators should refer to CAP’s Laboratory turer’s instructions; long tubes (e.g., 100 mm) placed
Instrument Evaluation Verification & Maintenance in the corner tube holders closest to the rotor shaft will
Manual, 4th edition, 1989.) probably break when the rotor buckets swing out.
ALWAYS follow universal precautions when centri-
Citations from Health Devices fuging blood or body fluids. These precautions include
Tabletop centrifuges [User Experience NetworkTM], wearing gloves, face protection (e.g., shields), gowns or
1987 Feb; 16(2):55. laboratory coats, and plastic aprons, and are described
IEC DPR-6000 refrigerated centrifuges [User Experi- in detail in the National Committee for Clinical Labo-
ence NetworkTM], 1987 Jul; 16(7):255. ratory Standards (NCCLS) Document M29-T2, Vol. 11,
No. 14, Protection of Laboratory Workers from Infec-
Missing roll pin from Beckman Spinchron centrifuge tious Disease Transmitted by Blood, Body Fluids, and
rotor [User Experience NetworkTM], 1992 May; Tissue (tentative guideline),* as well as in the Occupa-
21(5):182. tional Safety and Health Administration’s (OSHA)
bloodborne pathogens standard.**
Risks from centrifuges [Hazard], 1992 Aug; 21(8):290.
Improper sealing of Baxter Megafuge C1725-2 centri- Procedure
fuges [Hazard], 1992 Sep; 21(9):331.
Before beginning an inspection, carefully read this
Centrifuges [Hazard summary], 1992 Dec; 21(12):459. procedure and the manufacturer’s instruction and
service manuals; be sure that you understand how to
Centrifuges [Hazard report summary], 1995 Apr; 24: operate the equipment, the significance of each control
158-9. and indicator, and the alarm capabilities. Also deter-
mine whether any special inspection or preventive
Test Apparatus and Supplies maintenance procedures or frequencies are recom-
Wrench to tighten the rotor nut mended by the manufacturer.
Leakage current meter or electrical safety analyzer * This document can be obtained from the NCCLS, 771 E. Lancaster
Ave., Villanova PA 19085; (610) 525-2435.
Ground resistance ohmmeter
** Occupational exposure to bloodborne pathogens. Fed Regist 1991
Stopwatch or watch with a second hand Dec 6; 56(235):64004-182.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Centrifuges
1. Qualitative tests 1.15 Motor/Rotor/Pump. Check the physical condi-
tion and proper operation of these components.
1.1 Chassis/Housing. Examine the exterior of the Check the brushes, commutator, and bearings of
unit for cleanliness and general physical condi- the motor. Check the condition of gaskets, seals,
tion. Be sure that plastic housings are intact, and mounts. Check the rotor for balance and the
that all hardware is present and tight, and that condition of trunnion bearings, and check the
there are no signs of spilled liquids or other rotor attachment for tightness and excessive
serious abuse. wear. (Note: If using an ultraspeed centrifuge,
follow the manufacturer’s derating schedule for
1.2 Mount/Fasteners. If the device is mounted on a
the rotor. It should be outlined in the operator’s
stand, examine its condition. If it rests on a shelf,
manual.) Clean and lubricate components as re-
check the security of the shelf. If units have
quired, and note this on Lines 3.1 and 3.2 of the
suction-type feet, check the integrity of the feet.
inspection form (however, do not check these
1.4 AC Plug. Examine the AC power plug for damage. items until all necessary cleaning and lubrica-
Attempt to wiggle the blades to check that they are tion are completed). If a unit has a vacuum or
secure. Shake the plug and listen for rattles that diffusion pump, check its condition, and perform
could indicate loose screws. If any damage is sus- appropriate maintenance according to the
pected, open the plug and inspect it. manufacturer’s specifications.
1.5 Line Cord. Inspect the cord for signs of damage. 1.18 Indicators/Displays. During the course of the
If damaged, replace the entire cord or, if the inspection, confirm the operation of all lights,
damage is near one end, cut out the defective indicators, meters, gauges, and visual displays
portion. Be sure to wire a new power cord or plug on the unit. Be sure that all segments of a digital
with the correct polarity. display illuminate and function properly.
1.6 Strain Reliefs. Examine the strain reliefs at 1.20 Alarms/Interlocks. Induce alarm conditions,
both ends of the line cord. Be sure that they hold and verify that alarms are activated. Refriger-
the cord securely. If the line cord is detachable ated units should indicate whether the unit is at
(by the user), attach the cord to the unit so that the appropriate temperature. Check the lid
it cannot be easily removed. (See Health Devices latching mechanism for wear, and verify that it
1993 May-Jun; 22[5-6]:301-3.) holds the lid securely. A lid interlock should
either shut off the motor when the lid is opened
1.7 Circuit Breaker/Fuse. If the device has a or keep the lid latched until the rotor has
switch-type circuit breaker, check that it moves stopped. The centrifuge should not start with the
freely. If the device is protected by an external lid open. If the lid can be opened with the rotor
fuse, check its value and type against those spinning at high speed, check for appropriate
marked on the chassis and ensure that a spare labeling on or near the centrifuge, warning the
is provided. operator not to open the centrifuge lid during
operation. If the lid can be opened while the
1.13 Controls/Switches. Before changing any con-
centrifuge rotor spins at a low speed, the buckets
trols, consider the possibility of inappropriate
or rotor should have an inner protective lid.
clinical use or of incipient device failure. Record
Replace or modify any centrifuges that lack a
the settings of those controls that should be
latch. Do not use centrifuges that lack a lid; if a
returned to their original positions following the
lid is retrofitted, it should have a safety latch.
inspection.
Examine all controls and switches for physical 1.21 Audible Signals. Operate the device to activate
condition, secure mounting, and correct motion. any audible signals. Confirm appropriate vol-
Check that control knobs have not slipped on ume, as well as the operation of a volume control,
their shafts. Where a control should operate if so equipped.
against fixed-limit stops, check for proper align- 1.22 Labeling. Check that all necessary placards, la-
ment, as well as positive stopping. Check mem- bels, conversion charts, and instruction cards
brane switches for membrane damage (e.g., from are present and legible.
fingernails, pens). During the course of the in-
spection, be sure to check that each control and 1.23 Accessories. Confirm the presence and condition
switch performs its proper function. of accessories (e.g., sample buckets, sample
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
holders). Check for the proper type of accessory should not vary by more than ±10%. Depending
(e.g., proper-sized tubes for the buckets used). on various state regulations, this value may need
Check that every tube holder has a cushion. If to be recorded on the inspection tag.
protective lids for the buckets or the rotor (inner
safety lid) are available for that model centri- 2.12 Accuracy of Speed Setting. Determine the range
fuge, verify that they are kept with the centri- of speeds at which the centrifuge is used and a
fuges and are routinely used; also ensure that typical load (e.g., number of filled containers). Set
the protective lids form a tight seal and posi- the centrifuge to two or three speeds, and meas-
tively lock onto the bucket. ure the different speeds using a tachometer. If a
unit has an opaque cover, refer to the manufac-
1.24 Brake. Check the action of the mechanical or turer’s service manual to check the speed accu-
electrical brake. When the brake is applied (e.g., racy. (Note: A vibrating reed-type tachometer
by pushing the STOP button), the centrifuge may be used with most centrifuges with opaque
should decelerate smoothly. covers.) The measured speed should not vary by
more than ±10% of the displayed speed. (Note: If
2. Quantitative tests brushes have been changed, check speed settings
2.1 Grounding Resistance. Using an ohmmeter, after brushes are properly replaced.)
electrical safety analyzer, or multimeter with
good resolution of fractional ohms, measure and 3. Preventive maintenance
record the resistance between the grounding pin 3.1 Clean exterior (interior if appropriate).
of the power cord and exposed (unpainted and not
anodized) metal on the chassis. We recommend a 3.2 Lubricate per manufacturer’s instructions.
maximum of 0.5 Ω. If the device is double insu-
3.4 Replace brushes, brake, gaskets, seals, and vac-
lated, grounding resistance need not be meas-
uum pump, if needed. (For the proper procedure
ured; indicate “DI” instead of the ground
for replacing brushes, refer to the manufac-
resistance value.
turer’s manual and to the CAP Laboratory Instru-
2.2 Leakage Current. Measure chassis leakage cur- ment Evaluation Verification & Maintenance
rent to ground with the grounding conductor of Manual.)
plug-connected equipment temporarily opened.
Operate the device in all normal modes, includ- 4. Acceptance tests
ing on, standby, and off, and record the maxi- Conduct major inspection tests for this procedure
mum leakage current. If the unit has heating and the appropriate tests in the General Devices Pro-
and cooling modes, set the thermostats so that cedure/Checklist 438. All new centrifuges should have
each operates while taking measurements. a lid and a safety interlock that prevents the lid from
Chassis leakage current to ground should not being opened while the rotor is spinning at high
exceed 500 µA. speeds. Purchase only those centrifuges on which the
2.10 Temperature Accuracy. Check the temperature rotor stops completely before the lid can be opened
control on refrigerated centrifuges using an elec- and/or, for units that operate at a low speed, those that
tronic thermometer. Place the electronic ther- have a protective lid for the buckets or an inner safety
mometer probe in the centrifuge bowl near the lid for the rotor. Give preference to those centrifuges
automatic temperature control sensor. (Refer to that have protective lids for the buckets or rotor. If the
the manufacturer’s specifications to determine units being purchased allow the lid to be opened while
where the temperature control sensor is located.) the rotor is spinning at low speeds, protective lids
Close the centrifuge, sealing the gasket around should be included.
the thermometer cable. Compare the tempera-
ture control with the electronic thermometer at Before Returning to Use
each setting or at the settings being used. The Make sure controls are set in their normal pre-use
readings should not differ by more than ±3°C. positions.
2.11 Timer Accuracy. Check the timer against a stop- Attach a caution tag in a prominent position to alert
watch or watch with a second hand. A centrifuge the user that control settings may have been changed.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 412-0595
Circulating-Fluid Pumps
Used For:
Pumps, Circulating-Fluid, Localized Heat [17-647]
Also Called: Heating pads; K-Module, a registered trademark of Baxter to be used only when referring to
that device; T-Pump, a registered trademark of Gaymar Industries Inc. to be used only when referring to that
device
Commonly Used In: Most patient care areas
Scope: Applies to circulating-fluid heating pad pumps
Risk Level: ECRI Recommended, Low; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview Citations from Health Devices
Circulating-fluid pumps and pads are used for apply- Circulating-fluid pumps and heating pads [Evalu-
ing long-term mild heating to the skin. ation], 1989 May; 18:154-73.
Circulating-fluid pumps and heating pads [Evaluation
A fluid pump consists of a reservoir that holds a
Update], 1989 Dec; 18:418.
supply of distilled water; a heater, mounted in the
reservoir, that warms the fluid; a pump that circulates Circulating-fluid pumps: Do not use for ECMO [Haz-
the fluid to the heating pad; a controller that main- ard], 1992 Jan; 21:39.
tains the fluid temperature; and safety devices that
deactivate the unit if the fluid temperature exceeds Test apparatus and supplies
the maximum allowable temperature limit. The Ground resistance ohmmeter
pump circulates the distilled water through a plastic
pad; the pad is placed under or on the skin to allow Leakage current meter or electrical safety analyzer
conductive heat flow. Shunt thermometer with appropriate connectors to
install in series with the pump and heating pad to
Heating pads are available in three types: all-plas- check the temperature of the circulating fluid (tem-
tic single-patient-use, some of which can be reused; perature calibration assemblies may be available
covered single-patient-use, which have a layer of fab- from manufacturers of circulating-fluid pumps and
ric bonded to their surface; and all-plastic reusable, may be used in place of the temperature-measuring
made from thick plastic sheets to resist wear and procedure described in Item 2.4)
improve durability (these come with a repair kit).
Pads are constructed from two plastic sheets that are Flowmeter (0 to 20 gallons per hour [gph] range)
heat-sealed together; each manufacturer uses a with water
unique flow pattern. Heating pad
009064 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
412-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Special precautions portion. Be sure to wire a new power cord or plug
with the correct polarity.
Some testing requires disabling temperature control
circuits; to avoid damage to the unit, this testing should 1.6 Strain Reliefs. Examine the strain reliefs at
be performed only by qualified personnel familiar with both ends of the line cord. Be sure that they hold
unit design. Although we hesitate recommending such the cord securely.
wiring modifications as part of a routine inspection
1.7 Circuit Breaker/Fuse. If the device has a
procedure because unskilled personnel may inadver-
switch-type circuit breaker, check that it moves
tently damage the unit, there may be no other way to
freely. If the device is protected by an external
determine whether the backup thermostat or overtem-
fuse, check its value and type against that
perature alarms are functional. Personnel responsible
marked on the chassis, and ensure that a spare
for inspecting heating pads must recognize their own
is provided.
limitations and, where appropriate, seek qualified help
when performing this test. Return the unit to its normal 1.8 Tubes/Hoses. Check the condition of all tubing
operating condition immediately after completing the and hoses. Be sure that they are not cracked,
test. Performing the operating temperature test (Item kinked, or dirty.
2.4) after the high-temperature protection test (Item
2.3) will help ensure that the device has been correctly 1.10 Fittings/Connectors. Examine liquid fittings
returned to its proper operating condition. and connectors, as well as all electrical cable
connectors, for general condition.
Procedure 1.13 Controls/Switches. Before moving any controls,
Before beginning an inspection, carefully read this check their positions. If any of them appear
procedure and the manufacturer’s instruction and inordinate (e.g., a temperature control at maxi-
service manuals; be sure that you understand how to mum), consider the possibility of inappropriate
operate the equipment, the significance of each control clinical use or of incipient device failure. Record
and indicator, and the alarm capabilities. Also deter- the settings of those controls that should be
mine whether any special inspection or preventive returned to their original positions following the
maintenance procedures or frequencies are recom- inspection.
mended by the manufacturer.
Examine all controls and switches for physical
1. Qualitative tests condition, secure mounting, and correct motion.
Where a control should operate against fixed-
1.1 Chassis/Housing. Examine the exterior of the limit stops, check for proper alignment, as well
unit for cleanliness and general physical condi- as positive stopping. Check membrane switches
tion. Be sure that plastic housings are intact, for membrane damage (e.g., from fingernails,
that necessary assembly hardware is present pens). During the course of the inspection, be
and tight, and that there are no signs of spilled sure to check that each control and switch per-
liquids or other serious abuse. forms its proper function.
1.2 Mount/Fasteners. If the device is mounted on a 1.14 Heater. Operate it to be sure that its controls
stand or bracket, examine the condition of the function properly (e.g., that a variable tempera-
mount. Verify that the mounting apparatus is ture control does, in fact, determine the amount
secure and that all hardware is firmly in place. of heating; that On/Off controls work). Verify
Check for weld cracks. Ensure that the assem- that the pad warms up when the unit is operated
bly is stable. to ensure that the heater and the pump are
1.4 AC Plug. Examine the AC power plug for dam- functioning.
age. Attempt to wiggle the blades to determine 1.15 Motor/Pump/Fan. Check physical condition
that they are secure. Shake the plug and listen and for proper operation.
for rattles that could indicate loose screws. If
any damage is suspected, open the plug and 1.16 Fluid Levels. Check all fluid levels. Replenish
inspect it. any fluids that are low.
1.5 Line Cord. Inspect the cord for signs of damage. 1.18 Indicators/Displays. During the course of the
If damaged, replace the entire cord, or, if the inspection, confirm the operation of all lights,
damage is near one end, cut out the defective indicators, or visual displays on the unit.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Circulating-Fluid Pumps
1.20 Alarms. Many units have low-water-level and Determine from the manufacturer’s literature
high-temperature alarms. Operate the unit in how backup thermostats can be tested. Connect
such a way as to activate the low-water-level the shunt thermometer in series with the input
alarm and any other audible and visual alarms line to the heating pad. Record the maximum
(e.g., tilt). Verification of the high-temperature water temperature for each backup thermostat,
alarm requires abnormal operating conditions and note any alarms or indicators. Maximum
that will be simulated in Item 2.3. temperatures should be within the manufac-
turer’s specified range, but should not exceed
1.22 Labeling. Check that all necessary placards, la-
43°C. Remove any bypasses installed for this test.
bels, and instruction cards are present and legible.
2.4 Operating Temperature. Operate the pump at
1.23 Accessories. Verify that the pad is clean, free of
37°C and at maximum control settings with the
leaks, and stored without sharp folds or creases.
thermometer shunt still installed as in Item 2.3.
Also verify the presence and operation of a key
Actual water temperature should be within 1°C
for adjusting fluid temperature.
of the set temperatures.
2. Quantitative tests 2.5 Flow. Remove the temperature shunt, and place
2.1 Grounding Resistance. Using an ohmmeter, a flowmeter (0 to 20 gph range) in series with the
electrical safety analyzer, or multimeter with input line to the heating pad. Record the flow
good resolution of fractional ohms, measure and rate. The flow should exceed the minimum flow
record the resistance between the grounding pin specified by the manufacturer.
of the power cord and exposed (unpainted and
not anodized) metal on the chassis. We recom- 3. Preventive maintenance
mend a maximum of 0.5 Ω. 3.1 Clean the exterior.
2.2 Leakage Current. Measure chassis leakage cur- 3.4 Flush/fill the reservoir, if needed.
rent to the chassis of the device with the ground-
ing conductor temporarily opened. Operate the 4. Acceptance tests
device in all normal modes, including on (with Conduct major inspection tests for this procedure
the heater operating) and off, and record the and the appropriate tests in the General Devices Pro-
maximum leakage current. Leakage current cedure/Checklist 438.
should not exceed 300 µA.
2.3 High-Temperature Protection. Circulating-fluid Before returning to use
pumps should have high-temperature protection Verify that any control circuits that were bypassed
(backup thermostats) to limit the water tem- or deactivated for testing purposes have been returned
perature if the main temperature control fails. to their normal operating condition.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Form 441-0595
Conductive Furniture and Floors
Used For:
Flooring, Conductive [15-832]
Used In: Operating rooms, other flammable anesthetizing locations
Scope: Complies with the requirements for periodic testing of conductive casters on equipment and furniture
used in flammable anesthetizing locations and conductive flooring installed in these areas
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 1 month* months . hours
Minor NA months . hours
*
This procedure is not required in areas where flammable anesthetics are no longer used and where the floors
have been treated to make them nonconductive.
Overview Unlike the requirements for grounding medical de-
vices to ensure safety from electrical shock, low resis-
tance is not required for conductivity established for
Some inhalation anesthetics (e.g., cyclopropane, di- the purpose of electrostatic control. Rather, it is some-
ethyl ether, ethyl chloride, ethylene) are flammable times preferable to ensure that a certain minimum
and pose a considerable fire and explosion risk when level of resistance be maintained to minimize electric
mixed with air, oxygen, and nitrous oxide. The most shock hazards. For example, conductive flooring for
likely ignition source for these gas mixtures in the this purpose is required to offer an average resistance
operating room or other flammable anesthetizing loca- of at least 25,000 Ω and less than 1 MΩ.
tions is a spark caused by an electrostatic (static elec-
tricity) discharge. Other possible sources of ignition Flammable anesthetics were once a necessary part
include heating or sparking in electrically powered of surgery; however, nonflammable inhalation anes-
devices, electrosurgical or electrocautery equipment, thetics are now available and are used in most cases.
and percussion sparks. Flammable anesthetics are used only for rare circum-
stances (e.g., where a flammable anesthetic is claimed
Conductive floors and electrical interconnection of to offer some pharmacologic advantage or a physician
all furniture and devices with conductive surfaces is familiar with a flammable anesthetic and unwilling
minimize the risk of electrostatic charge accumulation to change technique).
and resultant spark. NFPA 99, Standard for Health
Care Facilities, 1993 Edition, Section 12-4.1.3, con- In areas designated and posted for the use of only
tains requirements calling for all furniture and devices nonflammable anesthetics, antistatic precautions are
located in a flammable anesthetizing location to have not required. Equipment or furniture with conductive
conductive casters (or equivalent means) to ensure casters can be used in nonflammable anesthetizing
continuity with the conductive flooring. locations, but conductivity need not be maintained or
010828 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
441-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
measured. Conductive floors in nonflammable anes- and metal frame or chassis should not exceed
thetizing locations, unless they are treated to make 250,000 Ω. Only one caster need meet this requirement
them nonconductive, must be inspected to ensure that to ensure continuity and to conform with NFPA 99;
each of the five floor-resistance measurements in each however, we recommend testing all casters during initial
room yields a reading of 10,000 Ω or more to minimize acceptance testing of the device or furniture.
electric shock risk from an excessively conductive floor.
For convenience, perform routine periodic tests of
No further testing is required once this criterion is met.
furniture and equipment conductivity by placing one
ECRI recommends treating or replacing floors to make
of the 5 lb electrodes on the conductive floor and an-
them nonconductive, especially if the power supply is
other on the furniture or equipment. Unplug the de-
changed from isolated to grounded.
vice (and remove any nonpermanent grounding
Test apparatus and supplies straps). The resistance should not exceed 5 MΩ; if it
does, perform the entire inspection procedure. Indicate
High-voltage megohmmeter intended for this type on the form whether floor-to-frame or caster-to-frame
of application, which has an open-circuit voltage of tests were performed. It is not necessary to record the
500 VDC and meets the requirements of NFPA 99 resistance value, but space is provided on the form if
Two 5 lb, 21⁄2″ diameter circular electrodes that it is desired in the event of a failure.
meet the requirements of NFPA 99
Conductive floors. Make sure that the floor is clean
Metal plate and insulating plate or sheet (for caster and dry. Place the electrodes 3 ft apart on the floor,
conductivity tests) and measure and record the resistance between the
two electrodes and from one electrode to a ground point
Special precautions (e.g., grounding jack, grounded exposed metal in the
The megohmmeter used for this testing is capable room). Measure the resistance at five different loca-
of shocking personnel. Never touch the leads or equip- tions in the room, and average each set of five readings.
ment under test when the ohmmeter is activated.
Each of the five individual floor resistance readings
Procedure should be no greater than 5 MΩ and no less than
10,000 Ω, and the average should be no greater than
Equipment/Furniture. Inspect leg tips, casters, or
1 MΩ and at least 25,000 Ω. Each measurement from
other conductive devices on furniture and equipment
the floor to a ground point should be at least 10,000 Ω,
to ensure that they are free of wax, lint, or other
and the average resistance should be at least 25,000
materials that interfere with conductivity.
Ω.
Lubricate casters if needed with dry graphite or
Conductive flooring is not required in nonflamma-
graphited oil. Avoid excessive lubrication, since this
ble anesthetizing locations. However, if a conductive
can cause accumulations of oil and grime on caster
floor is present, test as above. No individual reading
wheels and sides.
should be less than 10,000 Ω. If the floor does not meet
Test conductive casters, chains, or other mechanisms this criterion, test the floor conductivity every month
by placing one caster on a metal plate that is insulated until the condition is corrected. No further testing is
from the floor. The resistance between the metal plate required once the criterion is met.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Conductive Furniture and Floors
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 458-0595
Critical Care Ventilators
Used For:
Ventilators, Intensive Care [17-429]
Ventilators, Intensive Care, Neonatal/Pediatric [14-361]
Ventilators, Pressure-Cycled [14-360]
Ventilators, Transport [18-098]
Also Called: Respirators
Commonly Used In: Critical care units, general medical/surgical units, emergency departments
Scope: Applies to all ventilators except jet ventilators, negative-pressure ventilators, portable ventilators
(see Procedure/Checklist 471), and anesthesia unit ventilators (see Procedure/Checklist 461)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 6 months* months . hours
Minor NA months . hours
* Inspection and preventive maintenance intervals should be scheduled according to the manufacturer’s
recommendations, which may be related to hours of use. However, units should have a major inspection at
least every six months. Pre-use checks should be performed by a respiratory therapist or respiratory equipment
technician.
Overview attainment of dangerous pressures in the patient’s
lungs.
Mechanical ventilators are used to compensate for
deficiencies in normal breathing. A ventilator may aid The ventilator provides direct control of the patient’s
or augment spontaneous breathing or may completely ventilatory variables, as well as other variables (e.g., the
regulate a prescribed breathing pattern for patients concentration of inspired oxygen), and the limits on certain
who cannot breathe for themselves. Most modern ven- variables for safe operation. All these controls allow the
tilators use positive-pressure inflation of the lungs to clinician to provide better patient management, even for
accomplish these functions. patients with serious respiratory impairments.
Ventilators are classified according to the method in A mechanical ventilator is composed of four basic
which ventilation is accomplished. Most adult ventila- subsystems: the ventilator and its controls; monitors
tors are volume cycled, in that they are set to deliver a and alarms; gas supply; and patient circuit (which
predefined volume of gas to the patient. Most infant includes the breathing circuit and may include a humidi-
ventilators are time cycled, in that they are set to fier and nebulizer). Each subsystem requires its own
deliver gas for a predefined inspiratory time. A pres- inspection and preventive maintenance procedures.
sure-cycled ventilator delivers gas until a predefined
pressure is reached. Volume- and time-cycled ventila- Many microprocessor-controlled ventilators have
tors also have a pressure-limit control to prevent the self-diagnostic programs. When the ventilator’s
232575 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
458-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
hardware (e.g., solenoid valves, transducers) is IPM Task ManagerTM, the software component of the
checked by its own software, manual inspection items Inspection and Preventive Maintenance System, en-
can be eliminated. ables easy production of customized procedures and
checklists for specific ventilator models and clinical
Citations from Health Devices needs. Items performed by outside vendors can be
excluded from the checklist; a separate checklist for
Inadequate pressure relief in infant ventilators [Haz- use by outside vendors can be produced to ensure that
ard], 1983 Apr; 12:150-1. those items agreed upon are performed by the vendor.
Leaving ventilator-dependent patients unattended The following framework should be supplemented
[Hazard], 1986 Apr; 15:102-3. by the manufacturer’s recommended preventive main-
Infant ventilators [Evaluation], 1986 Aug; 15:219-46. tenance procedures for mechanical ventilators.
Remote alarms for ventilators and other life-support 1. Qualitative tests
equipment, 1986 Dec; 15:323-4. 1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condi-
Microprocessor-controlled third-generation critical
tion. Be sure that plastic housings are intact,
care ventilators [Evaluation], 1989 Feb; 18:59-83.
that all hardware is present and tight, and that
there are no signs of spilled liquids or other
Test apparatus and supplies serious abuse.
Lung simulator with adjustable compliance or ven-
1.2 Mount/Fasteners. If the device is mounted on a
tilator tester
stand or cart, examine the condition of the
Pressure gauge or meter with 2 cm H2O resolution mount. If it is attached to a wall or rests on a
from -20 to +120 cm H2O shelf, check the security of this attachment.
Various breathing circuit adapters Check the mounting security of all components
or attached monitors.
Leakage current meter or electrical safety analyzer
1.3 Casters/Brakes. If the device moves on casters,
Ground resistance ohmmeter check their condition. Verify that they turn and
Additional items as required for specific manufac- swivel, as appropriate, and look for accumula-
turers’ procedures tions of lint and thread around the casters.
Check the operation of brakes and swivel locks,
Procedure if the unit is so equipped.
Before beginning an inspection, carefully read this 1.4 AC Plug. Examine the AC power plug for dam-
procedure and the manufacturer’s instruction and age. Attempt to wiggle the blades to check that
service manuals; be sure that you understand how to they are secure. Shake the plug and listen for
operate the equipment, the significance of each control rattles that could indicate loose screws. If any
and indicator, and the alarm capabilities. Also deter- damage is suspected, open the plug and inspect it.
mine whether any special inspection or preventive
1.5 Line Cord. Inspect the cord for signs of damage.
maintenance procedures or frequencies are recom-
If damaged, replace the entire cord or, if the
mended by the manufacturer.
damage is near one end, cut out the defective
Manufacturers’ recommended procedures for inspec- portion. Be sure to wire a new power cord or plug
tion and preventive maintenance of mechanical ventila- with the correct polarity. Also, check line cords
tors vary in both methods and required accuracy. In of battery chargers.
addition, ventilation modes, controls, and algorithms for 1.6 Strain Reliefs. Examine the strain reliefs at
calculated variables vary greatly according to manufac- both ends of the line cord. Be sure that they hold
turer and model. This procedure provides the basic the cord securely. If the line cord is detachable
framework for complete ventilator inspection and pre- (by the user), affix the cord to the unit so that it
ventive maintenance. Manufacturers’ recommended cannot be removed by the operator. (See Health
procedures should be added where appropriate. Refer- Devices 1993 May-Jun; 22:301-3.)
ences to specific pages of the manufacturer’s manual
should be added to the checklist. (The checklist includes 1.7 Circuit Breaker/Fuse. If the device has a
blank spaces for the insertion of these page references.) switch-type circuit breaker, check that it moves
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Critical Care Ventilators
freely. If the device is protected by an external fingernails, pens). During the inspection, be sure
fuse, check its value and type against that to check that each control and switch performs
marked on the chassis and ensure that a spare its proper function.
is provided.
1.14 Heater (for heated portions of the breathing cir-
1.8 Tubes/Hoses. Check the condition of all tubing cuit). Check the physical condition and proper
and hoses. Be sure that they are not cracked, operation of the heater.
kinked, or dirty.
1.15 Fan/Compressor. Check the physical condition
1.9 Cables. Inspect any cables and their strain re- and proper operation of these components.
liefs for general condition. Carefully examine Check for automatic activation of the compressor
cables to detect breaks in the insulation and to when the piped gas supply pressure falls below
ensure that they are securely gripped in the operating pressure. Clean or replace fan and/or
connectors at each end, which will prevent rota- compressor filters and lubricate as required, ac-
tion or other strain. Where appropriate, verify cording to the manufacturer’s instructions, and
that there are no intermittent faults by flexing note this on Lines 3.1 and 3.2 of the form.
cables near each end and looking for erratic
1.17 Battery/Charger. Inspect the physical condi-
operation or by using an ohmmeter.
tion of batteries and battery connectors if readily
1.10 Fittings/Connectors. Examine all gas fittings accessible. Check operation of battery-operated
and connectors for general condition. Gas fit- power-loss alarms, if so equipped. Operate the
tings should be tight and should not leak. Verify unit on battery power for several minutes to
that keyed connectors (e.g., pin-indexed gas con- check that the battery is charged and can hold a
nectors) are used where appropriate, that all charge. (The inspection can be carried out on
pins are in place and secure, and that keying is battery power to help confirm adequate battery
correct. Connectors to hospital central piped capacity.) Check battery condition by activating
medical gas systems should have the appropri- the battery test function or measuring the output
ate DISS or quick-connect fitting to eliminate the voltage; for lead-acid batteries, measure the spe-
need for adapters. cific gravity and check the fluid level. Check the
condition of the battery charger and, to the ex-
1.12 Filters. Check the condition of gas filters. Check tent possible, confirm that it does, in fact, charge
for corrosion residue indicative of liquid, gase- the battery. Be sure that the battery is recharged
ous, or solid particle contaminants in the gas or charging when the inspection is complete.
supply; advise appropriate personnel if found. When it is necessary to replace a battery, label
Clean or replace if appropriate, and indicate this it with the date.
on Lines 3.1 and 3.4 of the inspection form.
1.18 Indicators/Displays. Confirm the operation of all
1.13 Controls/Switches. Before changing any con-
lights, indicators, meters, gauges, and visual dis-
trols or alarm limits, check their positions. If any plays on the unit and charger (if so equipped). Be
settings appear inordinate (e.g., alarm limits at sure that all segments of a digital display function.
the ends of their range), consider the possibility
Record reading of an hour meter, if present.
of inappropriate clinical use or of incipient device
failure. Investigate questionable control settings 1.20 Alarms/Interlocks. Induce alarm conditions to
on a home care unit. Consult with the patient’s activate audible and visual alarms. Verify alarm
physician to determine correct settings. The pa- messages on displays. Check that any associated
tient or caregiver should receive additional interlocks function. If the unit has an alarm-si-
training, if required. Record the settings of those lence feature, check the method of reset (i.e.,
controls that should be returned to their original manual or automatic) against the manufacturer’s
positions following the inspection. specifications. It may not be possible to check out
all alarms at this time, since some may require
Examine all controls and switches for physical
special conditions that must be established ac-
condition, secure mounting, and correct motion.
cording to the manufacturer’s recommendations;
Check that control knobs have not slipped on
include these in Item 2.4. Verify that the remote
their shafts. Where a control should operate
alarm indicator functions properly.
against fixed-limit stops, check for proper align-
ment, as well as positive stopping. Check mem- 1.21 Audible Signals. Operate the device to activate
brane switches for damage (e.g., from any audible signals. Confirm appropriate volume,
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
as well as the operation of a volume control, if may include tidal volume, respiration rate, inspi-
so equipped. If audible alarms have been si- ratory time, expiratory time, inspiratory:expira-
lenced or the volume set too low, alert clinical tory (I:E) ratio, flow, and waveshape, among
staff to the importance of keeping alarms at the others. Typically, these tests are performed by
appropriate level. attaching the ventilator to a lung simulator or
ventilator tester and comparing measured val-
1.22 Labeling. Check that all necessary placards, la- ues of pressure, flow, and/or volume and time to
bels, and instruction cards are present and leg- settings on the ventilator. The manufacturer
ible. should recommend the appropriate ventilator
1.23 Accessories. Confirm the presence and condition settings (e.g., tidal volume, rate, inspiratory
of accessories, including the humidifier and the time) at which to verify proper operation and
nebulizer (see Procedure/Checklist 431 for accuracy (generally within 10%). Check the ac-
heated humidifiers). curacy of flowmeters on infant ventilators.
2.4 Monitors and Alarms. The following parame-
2. Quantitative tests ters are commonly monitored and should be in-
2.1 Grounding Resistance. Using an ohmmeter, elec- spected for accuracy (generally within 10%)
trical safety analyzer, or multimeter with good according to the manufacturer’s specifications:
resolution of fractional ohms, measure and record Breathing rate
the resistance between the grounding pin of the
Inspiratory time
power cord and exposed (unpainted and not ano-
dized) metal on the chassis. We recommend a Peak inspiratory pressure (PIP)
maximum of 0.5 Ω. If the system is modular or Peak or mean inspiratory flow
composed of separate components, verify
PEEP
grounding of the mainframe and each module or
component. Mean airway pressure (MAP)
Volume (both tidal and minute volume)
2.2 Leakage Current. Measure chassis leakage cur-
rent to ground with the grounding conductor of Fraction of inspired oxygen (FIO2); see Oxy-
plug-connected equipment temporarily opened. gen Analyzers Procedure/Checklist 417
Operate the device in all normal modes, includ- Temperature of inspired air
ing on, standby, and off, and record the maxi-
Other monitors
mum leakage current.
Alarm settings (e.g., high PIP, low MAP, low
Measure chassis leakage current with all ac- pressure, low FIO2) should be inspected for
cessories normally powered from the same line proper and accurate activation.
cord connected and turned on and off. This in-
cludes other equipment that is plugged into the 2.5 Gas Supply.
primary device’s accessory receptacles, as well as Oxygen-air proportioner. See Procedure/Check-
equipment plugged into a multiple-outlet strip list 444.
(“Waber strip”) so that all are grounded through
a single line or extension cord. Compressor. Test according to the manufac-
turer’s recommendations.
Chassis leakage current to ground should not Pneumatic lines (including air filters). Verify that
exceed 300 µA. appropriate gas-specific connectors are used.
2.3 Modes and Settings. The following modes are Gas cylinders, gauges, and regulators (for trans-
commonly found on most ventilators: control, port ventilators). Verify that these components
assist/control, intermittent mandatory ventila- are present, securely mounted, and in good con-
tion/synchronized intermittent mandatory ven- dition and that there is adequate gas supply.
tilation (IMV/SIMV), pressure support, and
continuous positive airway pressure/positive 2.6 Patient Circuit.
end-exhalation pressure (CPAP/PEEP). The Breathing circuit (including filters). Verify that
function of these modes should be inspected and these components are compatible with the
verified for proper operation. Check the opera- ventilator according to the manufacturer’s
tion and accuracy of ventilation controls, which recommendations (see Health Devices 1988
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Critical Care Ventilators
Apr; 17:109). Check for leaks in the breathing 3.4 Replace components according to the manufac-
circuit, ensuring that fittings, adapters, and turer’s instructions.
other components (e.g., exhalation valves,
H-valves, PEEP valves, water traps, nebu- 4. Acceptance tests
lizers) are properly assembled and func- Conduct major inspection tests for this procedure
tioning correctly. and the appropriate tests in the General Devices Pro-
Humidifiers. See Heated Humidifiers Proce- cedure/Checklist 438.
dure/Checklist 431.
Pressure-relief Mechanism. Check the proper
Before returning to use
operation of the pressure-relief mechanism by Ensure that all controls are set properly. Set alarms
occluding the breathing circuit and measuring loud enough to alert personnel in the area in which the
the resulting peak pressure on the pressure device will be used. Other controls should be in their
gauge. Verify that pressure is vented in the normal pre-use positions. If the unit is being used at
breathing circuit. home, ensure that controls are set correctly before it is
returned to the patient.
3. Preventive maintenance Attach a Caution tag in a prominent position so that
3.1 Clean the exterior, interior, and components if the user will be aware that control settings may have
needed. been changed.
3.3 Calibrate according to the manufacturer’s in- Recharge battery-powered devices, or equip them
structions. with fresh batteries, if needed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 457-0595
Cryosurgical Units
Used For:
Cryometers [11-066]
Cryosurgical Units [11-067]
Cryosurgical Units, Ophthalmic [11-068]
Also Called: CSUs
Commonly Used In: Operating rooms; OB/GYN, urology, proctology, and dermatology professional offices;
surgical clinics
Scope: Applies to all cryosurgical units, except disposable ophthalmic cryoextractors; portions of this
procedure are applicable to tissue-temperature and tissue-impedance cryometers that may be integral to a
CSU
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview suitable for both benign and malignant tumors. N2O
and CO2 units are most suitable for benign and inflam-
Cryosurgical units (CSUs) apply a gaseous or liquid matory diseases, although they have been used suc-
refrigerant (cryogen) to freeze target tissue either cessfully to treat small malignancies; the lowest
through direct application of liquid cryogen (open-sys- probe-tip temperatures they can attain are -89° and
tem CSUs) or indirectly through contact with a cryo- -79°C, respectively.
gen-cooled probe (closed-system CSUs). Cryosurgically
treated tissue is usually allowed to become necrotic and Liquid nitrogen CSUs deliver the cryogen to the tip
slough off. The advantages of cryosurgery for tissue as a liquid, where its rapid vaporization cools the
destruction include ease of use, the need for little or no probe. In closed-system N2O units and CO2 units,
anesthesia, the avoidance of hemorrhage, and rela- cooling occurs through the Joule-Thompson effect, in
tively few postoperative complications. which a compressed gas (often at or near room tem-
perature) is allowed to expand suddenly through a
Cryosurgery is used in dermatology, oral surgery, small aperture inside the probe tip, causing a consid-
gynecology, urology, ophthalmology, otolaryngology, and erable drop in gas temperature and liquefaction of
proctology. Although some CSUs and their probe tips are some of the cryogen. The vaporization of the liquefied
designed for use within only one specialty (e.g., ophthal- cryogen from the interior of the tip, combined with the
mology, gynecology), most units have a wide range of drop in gas temperature caused by expansion, lowers
applications and associated interchangeable tips. the tip temperature to near the boiling point of the
cryogen.
The two types of CSUs — those that use liquid ni-
trogen and those that use N2O or CO2 — have signifi- Cryogen flows through an insulated probe shaft,
cantly different freezing capabilities. Liquid nitrogen cooling the tip, and exhausts back through the probe
units can attain temperatures as low as -196°C and are (closed-system design) or is applied directly to the
085109 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
457-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
target tissue (open-system design). CSUs using N2O or and cancer. Because exposure of clinical engineering
CO2 are not usually suitable for use as open systems personnel to the gas will be only occasional, a more acute
because cryogen “snow” builds up on target tissue and concern for their safety during the inspection is to guard
insulates the lesion from the cryogen spray. Liquid against temporary N2O intoxication.
nitrogen CSUs can be either open or closed.
Most older N2O CSUs expose personnel to levels
Most closed-system CSUs have active defrosting of the well in excess of the 25 parts per million time-weighted
probe tip to allow its safe and rapid removal from the average concentration limit of N2O gas recommended
target tissue. Active defrosting warms the probe from by the National Institute of Occupational Safety and
within and allows the tip to be removed safely and Health (NIOSH). In addition, the flow of gas from
quickly, usually within seconds; it can be achieved using CSUs is much higher than that from anesthesia ma-
an electric heater within the probe tip, exhaust occlusion chines, so the total quantity of N2O used during a
(resulting in gas pressure buildup in the tip that causes cryosurgical procedure or inspection is substantial and
the cryogen to heat up), or gas flooding of the tip with potentially very dangerous. We recommend switching
low-pressure cryogen at room temperature. to CO2 as the cryogen. Alternatively, the hospital must
scavenge all N2O from CSUs and vent it to the outside,
CSUs are available in three basic configurations: con-
away from air-intake ducts; N2O should never be
sole, stand-alone, and handheld. Consoles are freestand-
vented into a sink, drain trap, or the piped medical/sur-
ing units that typically contain the cryogen gas cylinders,
gical suction system. Users should contact the manu-
pressure regulators, indicators, and operating controls.
facturer of their unit and request information on
Stand-alone units are freestanding cryogen tanks on
scavenging the N2O exhaust; the manufacturer or a
carts without controls or displays. Handheld units are
local supplier can probably order the proper size and
lightweight, portable CSUs that use liquid nitrogen as
type of exhaust hose for equipment with an N2O scav-
the cryogen. Gun-type and pencil-shaped probes attach
enging port. An N2O CSU should not be used or tested
to both console and stand-alone units.
unless its exhaust is properly scavenged.
To ensure that the unit is freezing properly, the
If an N2O CSU is used in an OR with 100% outside air
probe tips on many console CSUs contain a cryometer
ventilation, one end of the exhaust hose should be placed
(usually incorporating a thermocouple) to measure
1 to 2 ft into the room air exhaust vent (permanent
probe-tip temperature. This reading, however, does
installation of a short length of exhaust hose through the
not directly reflect the cryolesion temperature and is
vent grill is advisable if vents are inconveniently located
not used as the definitive indicator of the depth and
[e.g., near the ceiling]), and the exposed hose end should
temperature of the frozen tissue. Some console CSUs
be equipped with a connector appropriate for attachment
also have a tissue-temperature cryometer; hypodermic
to the exhaust hose. If the OR has a dedicated system for
thermocouples are used to monitor the target-tissue
venting scavenged anesthetic gases with a flow capacity
temperature. Alternatively, the unit may be equipped
100 L/min (3.5 ft3/min), the N2O exhaust can be vented
with an impedance cryometer, which uses hypodermic
through this system rather than the return air system if
needle electrodes to assess the extent of freeze.
it is more convenient. For treatment rooms in clinics and
Questions have arisen over whether it is advisable, offices (and for ORs where the N2O cannot be vented as
practical, or safe for a hospital to repair its own cryo- discussed above), N2O can be vented to the outside through
surgical equipment. We do not recommend such a a window or small hole drilled in the window frame or the
practice; the units operate at very high pressures, and wall of the room where the equipment is used.
undetected probe damage can result in explosion and
serious patient injury. Furthermore, the equipment CO2 should be used for CSUs if scavenged N2O
needed to safely service and inspect CSUs is expensive. cannot be safely or conveniently vented or if N2O
However, clinical engineering staff should perform cannot be scavenged because of the design of the CSU.
annual routine general equipment inspections to de- Facilities that can operate with either N2O or CO2
tect any impending problem or improper scavenging of should strongly consider using CO2 — even if scaveng-
exhausted N2O. ing is possible — because it is intrinsically safer. N2O
units that cannot be scavenged or converted for use
Scavenging exhausted N2O from CSUs is essential. with CO2 should be removed from use and only CO2
N2O is both teratogenic and mutagenic; the reported units purchased. If an unscavenged N2O CSU must be
long-term hazards of exposure to this and other anes- used while awaiting proper scavenging modifications
thetic gases include increased rate of spontaneous abor- or before switching to a CO2 CSU, it should be used in
tion, increased incidence of hepatic and renal disorders, an extremely well-ventilated area, such as a hospital
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Cryosurgical Units
operating room. Pregnant staff members should never States, liquid N2O tanks are usually blue with a silver
be present during use or testing of an unscavenged neck; gaseous N2O tanks are entirely blue. All cylin-
N2O CSU. ders should be tested before they are connected to the
CSU. First, make sure that the valve is not pointed
Citations from Health Devices toward anyone. Then, open the valve one half to one
Nitrous oxide exhausted from cryosurgical units [Haz- full turn for 2 to 4 sec; no mist should be seen. If a
ard], 1979 Oct; 8:293. continuous mist is observed, the cylinder contains a
siphon and should be used only with CSUs specified
Update: Nitrous oxide exhausted from cryosurgical for liquid N2O use.
units, 1980 May; 9:180.
Siphon gas cylinders and cryosurgical units [Hazard],
Procedure
1980 May; 9:187. Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and
Personnel exposure to waste anesthetic gases, 1983 service manuals; be sure that you understand how to
May; 12:169-77. operate the equipment, the significance of each control
Frigitronics Model CCS-100 cryosurgical cart [User and indicator, and the alarm capabilities. Also deter-
Experience NetworkTM], 1986 Jan; 15:24. mine whether any special inspection or preventive
maintenance procedures or frequencies are recom-
Should hospitals repair cryosurgical units? [User Ex- mended by the manufacturer.
perience NetworkTM], 1986 Dec; 15:332-3.
Although many CSUs are gas powered, we have
N2O cryosurgical units must be scavenged [Hazard included tests for electrical safety and special func-
update], 1987 Dec; 16:407-9. tions for use on those units that are so equipped.
Surgical devices omitted from equipment control pro- 1. Qualitative tests
grams [Hazard], 1989 Feb; 18:86.
1.1 Chassis/Housing. Examine the exterior of the
Test apparatus and supplies unit for cleanliness and general physical condi-
tion. Be sure that plastic housings are intact,
Leakage current meter or electrical safety analyzer
that all hardware is present and tight, and that
Ground resistance ohmmeter there are no signs of spilled liquids or other
10× loupe serious abuse.
Stopwatch or watch with a second hand 1.2 Mount/Fasteners. If the device is mounted on a
Cup filled with tap water (temperature not critical) stand or cart, examine the condition of the
mount. If it is attached to a wall or rests on a
Special precautions shelf, check the security of this attachment. Gas
cylinder mounts should securely fasten the cyl-
Liquid nitrogen must be handled with care to prevent inders to the CSU stand or console.
operator injury. Read and follow the precautions and
warnings for handling liquid nitrogen presented in the 1.3 Casters/Brakes. If the device moves on casters,
equipment manual for any CSU using this cryogen. check their condition. Verify that they turn and
swivel, as appropriate, and look for accumula-
All N2O CSUs must have their exhaust safely scav- tions of lint and thread around the casters.
enged during inspections to prevent acute physical and Check the operation of brakes and swivel locks,
psychological impairment and possible long-term ad- if the unit is so equipped.
verse health effects to the inspector.
1.4 AC Plug/Receptacles. Examine the AC power
Siphon-type gas cylinders used with liquid N2O plug for damage. Attempt to wiggle the blades to
CSUs can be mistakenly installed on a CSU designed check that they are secure. Shake the plug and
for gaseous N2O use if the cylinders are mislabeled or listen for rattles that could indicate loose screws.
if medical personnel are unaware that siphon cylinders If any damage is suspected, open the plug and
should not be used with gas units. Very few N2O CSUs inspect it.
are designed to accept siphon cylinders of liquid N2O.
If a siphon cylinder is fitted to a gas unit, liquid N2O If the device has electrical receptacles for acces-
can leak from the fittings or seals of the cryoprobe, sories, verify presence of line power; insert an AC
resulting in patient or operator injury. In the United plug into each and check that it is held firmly. If
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
accessories are plugged and unplugged often, cepted safety standards — immediately replace
consider a full inspection of the receptacles. the yoke with one correctly keyed for that gas.
Destroy and discard the unkeyed yoke.
1.5 Line Cord. Inspect the cord for signs of damage.
If damaged, replace the entire cord or, if the 1.11 Probes and Probe Tips. Confirm that appropri-
damage is near one end, cut out the defective ate probes and probe tips are on hand and check
portion. Be sure to wire a new power cord or plug their physical condition. For ophthalmic probe
with the correct polarity. Also check line cords of tips, use a 10× loupe to inspect them. They
battery chargers. should not have any cracks, abrasion, corrosion,
kinks, dents, or evidence of bending. The pres-
1.6 Strain Reliefs. Examine the strain reliefs at ence of such damage suggests that these delicate
both ends of the line cord. Be sure that they hold probes have been bent or crushed and must be
the cord securely. If the line cord is detachable replaced.
(by the user), we recommend that the cord be
affixed to the unit so that it cannot be removed Operate the unit for about 30 sec with each tip
by the operator. (See Health Devices 1993 May- immersed in water (water temperature is not
Jun; 22[5-6]:301-3.) critical) and check to make sure that ice forms
on the tip. During each tip test, make sure that
1.7 Circuit Breaker/Fuse. If the device has a there is no leakage of cryogen (seen as bubbles
switch-type circuit breaker, check that it moves in the water) from the probe/tip connector. Ex-
freely. If the device is protected by an external amine the probe shaft thermal insulation for
fuse, check its value and type against that cracks or signs of degradation.
marked on the chassis, and ensure that a spare
is provided. 1.12 Filters. Check the condition of all liquid and gas
(air) filters. Clean or replace as appropriate and
1.8 Tubes/Hoses. Check the condition of all tubing indicate this on Lines 3.1 and 3.4 of the inspec-
and hoses. Be sure that they are not cracked, tion form.
kinked, or dirty.
1.13 Controls/Switches. Before changing any con-
1.9 Cables. Inspect any cables (e.g., sensor, elec- trols or alarm limits, check their positions. If
trode, remote control) and their strain reliefs for any settings appear inordinate, consider the pos-
general condition. Carefully examine cables to sibility of inappropriate clinical use or of incipi-
detect breaks in the insulation and to ensure that ent device failure. Record the settings of those
they are gripped securely in the connectors at controls that should be returned to their original
each end to prevent rotation or other strain. Ver- positions following the inspection. Also, make
ify that there are no intermittent faults by flexing sure that users turn off the gas cylinder valves
electrical cables near each end and looking for between uses. This will minimize the chance of
erratic operation or by using an ohmmeter. high-pressure leaks.
1.10 Fittings/Connectors. Examine all gas and liq- Examine all controls and switches for physical
uid fittings and connectors, as well as electrical condition, secure mounting, and correct motion.
cable connectors, for general condition. Electri- Check that control knobs have not slipped on
cal contact pins or surfaces should be straight, their shafts. Where a control should operate
clean, and bright. Verify that leads and hoses against fixed-limit stops, check for proper align-
are firmly gripped in their appropriate connec- ment, as well as positive stopping. Check mem-
tors. Gas and liquid fittings should be tight and brane switches for membrane damage (e.g., from
should not leak; listen for audible leaks and look fingernails, pens). During the course of the in-
for dripping cryogen. Complaints of excessive spection, be sure to check that each control and
gas usage indicate that the CSU may have a leak switch performs its proper function.
between the cryogen gas cylinder and the con-
sole/regulator. 1.17 Battery/Charger. Inspect the physical condi-
tion of batteries and battery connectors if readily
Pin-indexed gas cylinder yokes should be pre- accessible, including battery-operated cryometers.
sent. Make sure that no keying pins are missing Check the condition of the battery charger, if pre-
and that the keying is correct for the gas that is sent, and, to the extent possible, confirm that it
used. If a yoke has no keying pins — which some does in fact charge the battery. When it is neces-
manufacturers have omitted, in violation of ac- sary to replace a battery, label it with the date.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Cryosurgical Units
1.18 Indicators/Displays. During the course of the If the CSU console has an accessory recepta-
inspection, confirm the operation of all lights, cle, check its grounding to the main power cord.
indicators, meters, gauges, and visual displays
on the unit. Check that gas pressure gauges and 2.2 Leakage Current. Measure chassis leakage cur-
flowmeters read zero when the gas is not turned rent to ground with the grounding conductor of
on. Be sure that all segments of a digital display plug-connected equipment temporarily opened.
function. Record reading of an hour meter, if Operate the device in all normal modes, includ-
present. ing on, standby, and off, and record the maxi-
mum leakage current.
1.19 User Calibration. Verify that the self-test func-
tion operates and indicates normal operation, if Measure chassis leakage current with all ac-
so equipped. cessories normally powered from the same line
cord connected and turned on and off.
1.20 Alarms. Induce alarm conditions to activate
audible and visual alarms. Check that any asso- Chassis leakage current to ground should not
ciated interlocks function. If the unit has an exceed 300 µA.
alarm-silence feature, check the method of reset 2.3 Probe-Tip Cryometer. Repeat the defrost control
(e.g., manual or automatic) against the manufac- test described in Item 1.24. The ice ball should
turer’s specifications. It may not be possible to release from the probe tip when the tip tempera-
check all alarms at this time, since some may ture readout indicates 0°C, ±1°C.
require abnormal operating conditions that will
be simulated later in this procedure. 2.4 Tissue-Temperature Cryometer. Touch a tissue-
temperature probe to the probe tip and immerse
1.21 Audible Signals. Operate the device to activate them both in water. Activate the CSU at its
any audible signals. Confirm appropriate vol- maximum freezing power (if adjustable) for ap-
ume, as well as the operation of a volume control, proximately 3 min. The tissue-temperature
if so equipped. probe and probe tip will freeze within the ice ball.
1.22 Labeling. Check that all necessary placards, la- The tissue temperature and probe-tip tempera-
bels, conversion charts, and instruction cards ture should be within 5°C of each other.
are present and legible. 2.5 Elapsed-Time Meter/Timer. Where present,
1.24 Defrost Control. Verify that the defrost feature verify the accuracy of a timing mechanism with
operates. An ice ball on a tip should dislodge a stopwatch or watch with a second hand for 5
within approximately 30 sec after activation of min. The error should not exceed 10 sec.
the defrost mode.
3. Preventive maintenance
1.25 Scavenger. For N2O CSUs, verify the presence
3.1 Clean exterior (interior if appropriate).
of a scavenging attachment and hose. An N2O
CSU should not be used or tested unless its 3.3 Calibrate cryometer, if needed.
exhaust is properly scavenged.
3.4 Replace probe-tip O-rings, if needed.
2. Quantitative tests
4. Acceptance tests
2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with Conduct major inspection tests for this procedure
good resolution of fractional ohms, measure and and the appropriate tests in the General Devices Pro-
record the resistance between the grounding pin cedure/Checklist 438.
of the power cord and exposed (unpainted and
not anodized) metal on the chassis. We recom- Before returning to use
mend a maximum of 0.5 Ω. If the system is Make sure that all controls are set properly. Set
modular or composed of separate components, alarms loud enough to alert personnel in the area in
verify grounding of the mainframe and each which the device will be used. Other controls should
module or component. If the device is double be in their normal pre-use positions. Be sure that the
insulated, grounding resistance need not be inspection did not deplete the cryogen supply to a level
measured; indicate “DI” instead of the ground that disables the unit. Turn off the cryogen gas cylin-
resistance value. der valves after completing the inspection.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 408-0595
Defibrillator/Monitors
Used For:
Defibrillator/Monitors, Line-Powered [15-029]
Defibrillator/Monitor/Pacemakers [17-882]
Commonly Used In: Coronary and special care areas, emergency departments, operating rooms, resusci-
tation carts, ambulances, patient care areas
Scope: Applies to battery- and line-powered defibrillator/monitors; does not apply to defibrillators or ECG
monitors (see Defibrillators Procedure/Checklist 407 and ECG Monitors Procedure/Checklist 409); see
Pacemakers, External Noninvasive Procedure 460 for units with this accessory
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview since every minute of delay significantly decreases the
probability of a successful resuscitation attempt.
Defibrillator/monitors combine the functions of an
ECG monitor and defibrillator into a single unit, which In addition to periodic inspections, clinical staff
allows the operator to quickly assess and monitor the should perform visual inspections and ensure that
ECG and apply a defibrillating pulse, if appropriate. batteries are charging at the beginning of each work
Most units are battery-powered so that they can be shift and after each use of the device. They should also
used during transport within a hospital or in an am- perform discharge testing at least once a week. A User
bulance or carried into the field. Checklist for Defibrillators/Monitors/Pacemakers is
included in Health Devices 1993 May-Jun; 22:291-2.
Defibrillator/monitors are critical resuscitation in-
struments. Their failure to perform effectively may Citations from Health Devices
result in the death of a patient undergoing resuscita- User error and defibrillator discharge failures [Haz-
tion or cause further cardiac damage or even death in ard], 1986 Dec; 15:340.
a patient undergoing elective cardioversion or emer-
gency cardioversion of a life-threatening arrhythmia. Deteriorating insulation on internal defibrillator pad-
dles [Hazard], 1987 Feb; 16:46.
Failure to successfully defibrillate a patient may
occur for a number of reasons, including inadequate Defibrillator paddle resistance (continuity) testing
predefibrillation cardiopulmonary resuscitation [User Experience NetworkTM], 1987 Feb; 16:55.
(CPR) technique, operator error (e.g., poor paddle Battery-powered defibrillator/monitors [Evaluation],
application), or depleted or defective batteries (the 1987 Jun; 16:183-216. (See also 1987 Jul; 16:251.)
most common cause of defibrillator failure with bat-
tery-powered units). There is no time to troubleshoot Mains (AC Line) power switches on battery-powered
or correct even minor difficulties during emergencies, equipment [Hazard], 1987 Sep-Oct; 16:345.
009020 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
408-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Battery-powered defibrillator/monitors [Evaluation Overheating of replacement batteries in Physio-Control
Update], 1987 Dec; 16:389. Lifepak 6, 6s, and 7 defibrillator/monitors [Hazard
Update], 1992 Jun-Jul; 21:250.
Misuse of “Quick Look” defibrillator paddles [Hazard],
1988 Feb; 17:68. Defibrillator/monitors and external noninvasive pace-
makers [Evaluation], 1993 May-Jun; 22:212-94.
Lifepak 8 defibrillator/monitors [Hazard], 1988 Aug;
17:244. Defibrillator/monitors and external noninvasive pace-
makers [Evaluation Update], 1993 Dec; 22:579-82.
Lifepak 8 defibrillator/monitors [Hazard Update],
1988 Sep; 17:273. Misalignment of mating cable and defib cassette con-
nectors on Physio-Control Lifepak 8 defibrilla-
Physio-Control Lifepak 6 and 6s defibrillator/monitors tor/monitor [Hazard], 1993 Dec; 22:595-7.
[Hazard], 1988 Aug; 17:245.
Sparking during discharge testing on Physio-Control
Physio-Control develops Mains Power switch cover Lifepak 9 defibrillator/monitors [User Experience
[Hazard Update], 1988 Nov; 17:356. NetworkTM], 1994 Mar; 23:98-9.
Battery pins on Lifepak 5 defibrillator/monitors [Haz- Fires from defibrillation during oxygen administration
ard], 1989 Feb; 18:84. [Hazard], 1994 Jul; 23:307-9.
Porta Fib III defibrillator/monitor paddles [Hazard], Difficulty synchronizing with Zoll PD 1200 defibrilla-
1989 May; 18:175. tor/monitor/pacemaker [User Experience Net-
workTM], 1994 Aug-Sep; 23:374-5.
Mismatch of CCP R2 181-239 cables and HP43100
defibrillators [Hazard], 1989 Jun; 18:233. Spontaneous charging of Hewlett-Packard 43100A de-
fibrillator/monitor used with anterior/posterior pad-
Maintenance and user errors with the Physio-Control
dle set during monopolar electrosurgery [Hazard],
Lifepak 8 [User Experience NetworkTM], 1990 Feb;
1994 Oct-Nov; 23:455-6.
19:59.
Replacement batteries for the Physio-Control Lifepak Test apparatus and supplies
6 and 7 [User Experience NetworkTM], 1990 Feb; Defibrillator analyzer
19:61.
ECG simulator (calibrated output amplitudes and
Disposable difibrillator pads and electrodes [Evalu- rates are required for some tests)
ation], 1990 Feb; 19:33-56. Ground resistance ohmmeter
Hewlett-Packard defibrillator/monitors and Darox R2 Leakage current meter or electrical safety analyzer
electrodes [User Experience NetworkTM], 1990 Jul; Stopwatch or watch with a second hand
19:246.
The following equipment is necessary during accep-
Alarm lockup on ZMI PD 1200 defibrillator/monitors tance testing only:
[Hazard], 1990 Aug; 19:293-4.
Function generator
Heart-rate alarms on ZMI ZOLL PD 1200 pace- Attenuator
maker/defibrillators [Hazard], 1990 Dec; 19:455-6.
Oscilloscope
Physio-Control Lifepak 10 defibrillator/monitor Sync Transparent metric scale
mode [User Experience NetworkTM], 1991 Jan;
20:30-1. Isolation test supply (included in some electrical
safety analyzers)
ECG artifact and defibrillator/monitors [User Experi-
ence NetworkTM], 1991 Mar-Apr; 20:141. Special precautions
Internal defibrillator paddles [User Experience Net- CAUTION: The high voltage present on defibrillator
workTM], 1991 Dec; 20:497-8. paddles during discharge is extremely dangerous and
possibly lethal. Never perform tests alone. A second
Use of Physio-Control Lifepak 8 defibrillator/monitors person must be present to summon help and/or apply
with optional QUIK-PACE pacing cassette [User CPR in the event of an emergency. Never hold or
Experience NetworkTM], 1992 May; 21:183. contact the conductive electrode portion of the paddles
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Defibrillator/Monitors
unless you have confirmed that the defibrillator is 1.4 AC Plug. Examine the AC power plug for dam-
disarmed (not charged) and preferably off. age. Attempt to wiggle the blades to determine
that they are secure. Shake the plug and listen
Testing input isolation requires the use of a line for rattles that could indicate loose screws. If
voltage source. Although this source should include a any damage is suspected, open the plug and
current-limiting resistor, use caution to avoid contact inspect it.
with any portion of the circuit while it is energized.
If the device is mounted on a cart that has
A defibrillator/monitor must always be available in
electrical receptacles for additional equipment,
the event of an emergency during the inspection.
insert an AC plug into each, and check that it
Thus, perform the inspection in the vicinity of the
holds firmly. Inspect resuscitation cart recepta-
unit’s usual storage location, or ensure that a unit that
cles, including testing for wiring (e.g., using an
the clinical staff is familiar with is available as a
outlet tester) and tension of all three connec-
substitute.
tions. Also inspect the resuscitation cart plug for
Inspection testing may deplete the battery of bat- damage as described above.
tery-powered units. Ensure that a replacement unit
or a fully charged battery is available before you begin 1.5 Line Cord. Inspect the cord (including resusci-
testing. Do not test all the units in an area at one time, tation cart line cord, if appropriate) for signs of
since this will leave the staff inadequately equipped to damage. If damaged, replace the entire cord, or
handle emergencies. if the damage is near one end, cut out the defec-
tive portion. Be sure to wire a new power cord
or plug with the same polarity as the old one.
Procedure Check line cords of battery chargers.
Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and 1.6 Strain Reliefs. Examine the strain reliefs at
service manuals; be sure that you understand how to both ends of the line cord. Be sure that they hold
operate the equipment, the significance of each control the cord securely.
and indicator, and the alarm capabilities. Also deter-
mine whether any special inspection or preventive 1.7 Circuit Breaker/Fuse. If the device has a
maintenance procedures or frequencies are recom- switch-type circuit breaker, check that it moves
mended by the manufacturer. freely. If the device is protected by an external
fuse, check its value and type against that
Defibrillator energies may be specified in either marked on the chassis, and ensure that a spare
joules (J) or watt-seconds; these are equivalent units is provided.
(i.e., 1 J = 1 watt-second).
1.9 Cables. Inspect the cables of internal and exter-
1. Qualitative tests nal paddles, disposable defibrillation electrodes
(if applicable), and ECG electrodes for their
1.1 Chassis/Housing. Examine the exterior of the
strain reliefs and general condition. Examine
unit for cleanliness and general physical condi-
cables carefully to detect breaks in the insulation
tion. Be sure that plastic housings are intact,
and to ensure that they are gripped securely in
that all assembly hardware is present and tight,
the connectors at each end to prevent rotation or
and that there are no signs of spilled liquids or
other strain. Verify that an ECG can be dis-
other serious abuse.
played with either paddles or ECG leads used as
1.2 Mount. If the device is mounted on a stand or input. Wiggle, bend, and pull the cable to check
cart, examine the condition of the mount. If it is that continuity is not affected.
attached to a wall or rests on a shelf, check the
security of this attachment. 1.10 Fittings/Connectors. Examine all cable connec-
tors for general condition. Electrical contact
1.3 Casters/Brakes. If the device moves on casters, pins or surfaces should be straight and clean.
check their condition. Look for accumulation of Verify that leads and electrodes are firmly
lint and thread around the casters, and be sure gripped in their appropriate connectors. During
that they turn and swivel, as appropriate. Check major inspections, disconnect the paddle connec-
the operation of brakes and swivel locks, if the tors and look for misaligned pins, damaged re-
unit is so equipped. ceptacles, and carbon deposits from arcing.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
1.11 Paddles/Electrodes. Confirm that special pad- If the monitor can be separated from the defi-
dles (e.g., pediatric, internal) and electrodes brillator, make sure that it is securely connected
(e.g., disposable difibrillation electrodes) are to the defibrillator. Inform clinical personnel of
available, if appropriate. Examine all paddles any deficiencies so that problems can be avoided
for physical condition and cleanliness. Alert in the future.
clinical personnel responsible for the instrument
to the presence of dried electrode gel, physiologic Perform the inspection with the unit on bat-
fluids, or debris on the paddle surface or handles. tery power to check that monitor and defibrilla-
Dirty electrodes prevent good electrical contact tor batteries are charged and can hold a charge.
and can cause burns. Electrode gel or other Check battery capacity by activating the battery
debris on the insulating portion of the paddle can test function or measuring the battery-powered
cause operator shocks. Clean the paddles, if operating time. When it is necessary to replace
needed, including the electrode surface and han- a battery, label it with the date.
dle seams, and make sure that they are com- Some batteries require periodic deep dis-
pletely dry before proceeding with any further charges and recharging to maintain maximum
testing. battery capacity. If the manufacturer recom-
mends this procedure, verify that it is being
Confirm that an adequate supply of ECG elec-
performed on schedule.
trodes and disposable defibrillation electrodes (if
used) are available and that they are stored 1.18 Indicators/Displays. During the course of the
properly and are within their expiration dates. inspection, confirm the operation of all lights,
indicators, meters, and visual displays on the
1.13 Controls/Switches. Examine all controls and unit and charger. Be sure that all segments of a
switches for physical condition, secure mount- digital display function.
ing, and correct motion. Where a control should
operate against fixed-limit stops, check for Observe a simulated ECG signal on the dis-
proper alignment as well as positive stopping. play, and verify compliance with the following
Check membrane switches for membrane dam- criteria:
age (e.g., from fingernails, pens). During the
The baseline should stay in focus across the
course of the inspection, check that each control
display.
and switch performs its proper function.
The baseline should be horizontal and should
If the unit has redundant control functions not be noticeably sloped or bowed.
(e.g., a charge button on the front panel and on
The pulses from an ECG simulator should be
a paddle), ensure that both controls function
regularly spaced (uneven spacing indicates a
properly. Verify that activating just one paddle
sweep nonlinearity).
discharge button will not cause the unit to dis-
charge. A front-panel discharge button should All portions of a simulated ECG waveform
control only internal paddles (or disposable defi- should be clear and visible, including the
brillator electrodes, on some units) and should P-wave and QRS.
not cause discharge when external paddles are
When the vertical position of the baseline is
connected.
varied by adjusting the vertical position con-
trol, the baseline should move throughout
1.17 Battery/Charger. Inspect the physical condi-
most of the vertical height of the display.
tion of batteries and battery connectors, if read-
There should be no distortion in the baseline
ily accessible. Verify that the charger of
as it is moved up or down on the screen. In
battery-operated units is plugged into a live AC
monitors that incorporate a self-centering
outlet and that the charger is attached to the
baseline and therefore lack a position control,
defibrillator (i.e., charger cable is attached, unit
the baseline should be correctly positioned.
is firmly seated into charging stand or mount,
instrument end of line cord is attached, and Ambient light should not affect the visibility of
charging light is on). For units with removeable the trace. (If monitors are located so that ambi-
batteries that are charged in a separate charger, ent light reflects from the face of the display,
verify that the batteries are properly installed making the ECG difficult to see, control the
and that the charging, or ready, light is on. ambient light or use a filter over the display.)
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Defibrillator/Monitors
alarm-silence feature, check the method of reset
(i.e., manual or automatic) against the manufac-
turer’s specifications.
1.21 Audible Signals. Operate the device to activate
any audible signals (e.g., charge tone). Confirm
appropriate volume, as well as the operation of
a volume control.
1.22 Labeling. Check that all necessary placards, la-
bels, and instruction cards are present and leg-
ible.
Figure 1. The calibration pulse or step response leading 1.23 Accessories (gel, pads, or electrodes). Verify that
edge should have square corners (left). Slight rounding defibrillator gel, disposable defibrillator pads, or
(middle) or small overshoot is acceptable. Excessive disposable defibrillator electrodes are stored
rounding or overshoot (right) indicates the need for with the unit and are within their expiration
adjustment. dates. Confirm that defibrillator gel is being
used, not skin lubricant or ultrasound or TENS
gel. Notify appropriate clinical personnel if any
“Burn spots” should not be visible on the cath-
accessories are missing.
ode-ray tube. (The phosphor may “burn” if the
intensity is set too high. The cathode-ray tube 1.24 Internal Discharge of Stored Energy. To protect
face will be discolored if this condition exists.) personnel from accidental shock, it should be
Sixty-hertz or other noise (interference) possible to discharge the stored energy safely in
should not be superimposed on the baseline the event that the operator decides not to use the
with the ECG simulator attached. Baseline defibrillator after it has been charged. Verify
interference may be apparent as a thick base- that the unit rapidly releases the stored energy
line at high gain settings, but should be invis- when the power is turned off. If the unit also has
ible throughout the lower two-thirds of the a front-panel button for this purpose, verify its
gain control range. operation.
1.19 1 mV Step Response. Depress and hold the 1 mV
calibration button (or apply an external 1 mV
pulse) for about 3 sec. The trace should exhibit a
sharp, square-cornered leading edge that is nei-
ther rounded nor spiked (up to 10% spike or
overshoot is acceptable but will usually not be
observed in a unit that is functioning optimally;
see Figure 1). After 1 to 2 sec, the pulse should
have decayed to no more than half its original
amplitude (see Figure 2).
With the gain set to yield about 20 mm deflec-
tion for a 1 mV input (×2 or 0.5 mV/div), compare
the amplitude of the internal calibration pulse
and an external 1 mV signal (from a calibrated
ECG simulator). At a 20 mm deflection, they
should be within about 2 mm (10%) of each other.
1.20 Alarms. Operate the device in such a way as to
activate each audible and visual alarm (e.g., Figure 2. Sag time is measured to the half-amplitude
heart rate alarm, if so equipped). Check for ade- point. The upper trace indicates a low-frequency re-
quate alarm tone volume and any associated sponse of about 0.05 Hz. The lower trace indicates a
features (e.g., automatic direct writer activation, low-frequency response of between 0.07 and 0.09 Hz.
display freeze function). If the device has an
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
1.25 Special Features. continuity checks. The resistance from the paddle
Synchronizer (major inspection only). If the unit or electrode connector to the appropriate pin of the
has a synchronization mode, verify that the connector should not exceed 0.15 Ω.
unit will not discharge while in this mode
2.4 Rate Calibration. Using a simulated ECG with
when no ECG signal is present and that it will
rates of 60 and 120 pulses per minute, verify that
discharge when a simulated ECG is applied.
the heart rate indicator displays a rate within
Recorder. If the unit has a recorder, confirm that 5% or 5 bpm, whichever is greater, of the set rate
it operates smoothly, that the paper feeds (55 to 65 bpm, 119 to 126 bpm). Verify that the
evenly and does not stray from side to side, QRS visual and audible indicators are function-
and that the trace is of good quality (i.e., dark ing.
and thin) at all paper speeds. Perform the 1
mV step response test (Item 1.19) on the re- 2.5 Rate Alarm. The setup remains the same as for
corder. the previous test. Verify that the alarm activates
when the input rate is set just below or above
2. Quantitative tests typical low and high rate alarm settings (e.g., 40
2.1 Grounding Resistance. Using an ohmmeter, and 120 bpm, respectively). The difference be-
electrical safety analyzer, or multimeter with tween the rate displayed on the rate indicator
good resolution of fractional ohms, measure and that at which the alarm activates should not
and record the resistance between the ground- exceed 5% or 5 bpm, whichever is greater.
ing pin of the power cord (if so equipped) and
exposed (unpainted and not anodized) metal on 2.6 Internal Paddle Energy Limit. When used with
the defibrillator chassis. Repeat this test for internal paddles for application of the defibrilla-
tor output directly to the heart, the energy
the charger, if applicable. We recommend a
should not exceed 50 J. Test this feature on any
maximum of 0.5 Ω.
unit that is located where it may be used with
2.2 Chassis Leakage Current. Measure chassis internal paddles or that may be moved to such a
leakage current to ground with the grounding location. Connect the internal paddles, charge
conductor of plug-connected equipment tempo- the defibrillator to maximum energy, and dis-
rarily opened and the unit off, on, charging, and charge it into the defibrillator analyzer. Verify
charged. Record the maximum leakage current. that the output does not exceed 50 J.
Chassis leakage current to ground should not
exceed 300 µA. 2.10 Output Energy. During major inspections,
measure output energy at minimum, intermedi-
2.3 Paddle Continuity. Paddle continuity is typi- ate, and maximum energy settings. If the defi-
cally checked by verifying the presence of an brillator is commonly used for cardioversion, a
ECG signal obtained through the paddles (Item 50 J level is satisfactory for the intermediate
1.9). However, if additional paddles or disposable range.
defibrillation electrodes are available for use
with the defibrillator (e.g., internal or pediatric At each energy level, record the control set-
paddles), these must be checked. Either attach ting, indicated energy (on the unit’s energy me-
the paddles or electrode cable to the unit (e.g., in ter), and delivered energy (measured by a
conjunction with Item 2.6) and verify continuity defibrillator analyzer) after discharging the de-
with an ECG signal, or use an ohmmeter to verify fibrillator into the analyzer as soon as it is
continuity from each paddle or electrode connec- charged.
tor to the appropriate pin of the connector. Wig-
gle, bend, and pull the cable, especially near the At its maximum setting, the unit should be
paddle and connector, to check that continuity is able to deliver at least 250 J. The output energy
not affected. (Current may jump across a small should be within 4 J at low settings (below 25 J)
break in the paddle lead and may not be detected or 15% of the set energy (and indicated energy if
during defibrillator output tests. A continuity so equipped) at higher energies.
test will detect such a defect before it gets worse.)
This check should also be done for the reusable If the output of a defibrillator is unusually low
cable used with disposable defibrillation electrodes. at very low control settings, check for a break in
Internal paddles may require more frequent the cables or a defective connector.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Defibrillator/Monitors
During minor inspections, verify output at same day unless provisions are made for backup
only one energy level. Use the defibrillator’s in- units or spare charged batteries. Batteries may
ternal test load, if so equipped. Typically, this take considerable time to recharge, and a fully
provides either a numeric or a pass/fail indicator charged unit must be available for emergencies.
to verify that energy was delivered.
3. Preventive maintenance
2.11 Energy After 60 Sec. Deterioration of the energy
storage capacitors in some defibrillators results 3.1 Clean the exterior, paddles, rollers, and platen.
in charge leakage after the charging circuit has
3.2 Lubricate the chart recorder paper drive per the
been de-energized. In these units, it is possible
manufacturer’s recommendations, if required.
for the available energy to decrease if the unit is
not discharged at the earliest possible moment. 3.4 Replace the battery if any of the test procedures
The following test will identify this deficiency. indicate it is weak or defective, even after charg-
ing for 12 hr or more.
Charge the defibrillator to its maximum set-
ting, but do not discharge for 1 min. The deliv- Some users have also reported that periodic
ered energy should be at least 85% of that prophylactic battery replacement, either annu-
obtained when the unit is discharged immedi- ally or every other year, increases reliability and
ately (as in Item 2.10) and should meet manufac- decreases service calls. In this case, mark the
turer specifications for charge leakage. (Note date of the battery replacement on the battery or
that some units are designed to intentionally unit and check it during each inspection. Per-
bleed or discharge the capacitor charge if the form the inspection after battery replacement
defibrillator is not discharged within a set time and a suitable charge period.
period. These units should meet manufacturer
specifications.) Some units have more than one battery (e.g.,
one for the monitor and one for the defibrillator,
2.12 Charge Time and Max Energy (10th Charge). In batteries that can be switched by the user). Be
resuscitation attempts, it is not uncommon for sure that all batteries are checked, maintained,
the operator to call for multiple defibrillation and replaced as required.
shocks in rapid succession. Battery-powered de-
fibrillators may not have sufficient energy left in 4. Acceptance tests
their batteries to deliver 10 shocks. These defi-
Conduct major inspection tests for this procedure
ciencies are best discovered during periodic in-
and the appropriate tests in the General Devices Pro-
spections, rather than during clinical use.
cedure/Checklist 438.
Charge battery-powered units to maximum
energy and discharge 10 times through the ana- CAUTION: Do not measure paddle leakage current
lyzer (verify that the analyzer load will not be with the unit charged or charging or during discharge.
damaged by repeated discharge). On the 10th Most ECG monitors should meet the requirements
cycle, record the charging time (i.e., the time for for isolated input devices for ECG lead-to-ground, in-
the meter to equilibrate or for the ready light to terlead, and input isolation tests. Interlead testing
come on) and the delivered energy. To avoid should include both ECG-to-ECG and ECG-paddle
excessive battery depletion, stop the test and tests. AAMI DF-2-1989, Standard for Cardiac Defibril-
record the number of discharges and the values lator Devices, calls for applying isolated input risk
measured if the charging time exceeds 15 sec current tests (source, sink, and interlead) to defibrilla-
before the 10th discharge. Also stop the test if tor paddles, but with limits of 100 µA for external
the battery-condition meter indicates a weak paddles and 50 µA for internal paddles.
battery or, on some defibrillators, if the internal
circuitry terminates the charge early. In addition, perform the following tests.
The time to charge to maximum energy should 4.1 Synchronizer Operation. Check the synchroniz-
not exceed 15 sec. The output energy should ers of units so equipped. The thoroughness of
remain within 4 J or 15% of the selected energy this test will depend upon the availability of test
throughout the test. equipment.
CAUTION: Do not perform this test on all Set the defibrillator to deliver low output en-
battery-operated defibrillators in an area on the ergy (50 J or less). Use an ECG signal to trigger
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
the synchronizer and fire the defibrillator into a
50 Ω load (e.g., a defibrillator analyzer). Confirm
that, with the ECG simulator off, the defibrilla-
tor does not discharge. With a signal applied,
confirm that the synchronizer marker or other
indicator is functioning properly.
Use a dual-channel oscilloscope to note the time
delay between the peak of a QRS pulse (from an
ECG simulator) and the defibrillator pulse (from a
defibrillator analyzer). Use the ECG signal to trig-
ger the oscilloscope’s sweep. Some defibrillator
analyzers have synchronizer test functions. With
an ECG amplitude sufficient to activate the
marker or indicator and the discharge buttons
depressed, the defibrillator should discharge in Figure 3. Signal input test setup.
60 msec or less following the R-wave peak. Most
units will trigger on the first QRS pulse after the input signal (in mV). The CMRR may then be
buttons are depressed, although some units are calculated as the differential mode deflection fac-
designed to delay until the second or third QRS to tor divided by the common mode deflection factor.
avoid unintentional discharges.
A deflection factor is the change in trace po-
4.2 Internal Paddle Energy Limit. During accep- sition corresponding to a given input voltage to
tance testing, perform Item 2.6 on all units the monitor. Use an unbalanced CMRR meas-
equipped with this feature, regardless of in- urement that has a 5,000 Ω resistor in series
tended location for the device. with one of the input leads to the monitor. This
simulates unequal impedances in the elec-
4.3 Integral Output Tester. Check the operation and trode/skin interface of the monitor electrodes, as
accuracy of any integral defibrillator test load, if commonly exists in practice.
so equipped.
Since most common mode voltage in the hos-
4.4 Common Mode Rejection Ratio (CMRR). The
pital is at 60 Hz, it is most significant to measure
ECG monitor includes a differential amplifier so
the CMRR at or near that frequency. (A fre-
that it can display the voltage difference between
quency of 55 Hz is often used to minimize inter-
two electrodes (the RA and LA in Lead 1) while
ference from power-line frequency noise.) Using
using a third (RL) as a reference. If the same, or
the test setup shown in Figure 3, apply a sinusoid
common, voltage is applied to RA and LA simul-
test signal of 1 mV peak-to-peak at about 60 Hz
taneously, there should be no output from the
to the monitor. Turn up the monitor gain so that
differential amplifier because the voltage differ-
the deflection is at least 20 mm. Measure the
ence between the two inputs is zero. The extent
deflection in millimeters, and record it on the
to which a differential amplifier produces no
inspection form as the differential mode deflec-
output when the same signal is applied to both
tion factor. Since the input signal for this meas-
inputs is called its common mode rejection ratio.
urement was 1 mV, the differential mode
Common mode rejection is needed in monitors deflection factor expressed in mm/mV is numeri-
because of the presence of stray signals, common cally equal to the resultant deflection in millime-
to all input leads primarily at power-line frequency ters. Do not vary the gain of the monitor or the
(60 Hz). While these signals are too minute to be signal frequency for the remainder of this test.
hazardous, they can interfere with the ECG dis- Record the frequency on the form.
play of a monitor with a low CMRR at 60 Hz.
Use the test setup shown in Figure 4 for the
The CMRR is defined as: second part of this measurement. Note that
there is only one connection from the output of
Differential mode deflection factor, or DMD (mm ⁄ mV)
CMMR = the attenuator to the patient leads. The other
Common mode deflection factor, or CMD (mm ⁄ mV)
output terminal is grounded. It is essential that
Calculate the common mode deflection factor by all instruments used in this test be connected to
dividing the resultant deflection (in mm) by the a common ground to minimize noise.
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Defibrillator/Monitors
correction should be made in calculating paper
speed. The paper speed should be accurate to
within 2% (although 5% is allowed by some or-
ganizations). At a chart speed of 25 mm/sec and
a pulse interval of 1,000 msec (60 bpm on an ECG
simulator), the distance between the first and
last of 5 successive peaks should be 100 ±2 mm;
at a chart speed of 50 mm/sec, the distance between
the first and last of 5 successive peaks should be
200 ±4 mm.
4.8 Alarm Delay. In addition to checking rate alarm
accuracy (Item 2.5), use the same test setup to
determine alarm delay. First, set the high rate
Figure 4. Common mode rejection ratio test setup. alarm to 100 bpm and the ECG simulator to 60
bpm. Quickly change the simulator rate to 120
Increase the amplitude of the sinusoid signal bpm, and use a stopwatch or watch with a second
(up to 10 V peak-to-peak) until some measurable hand to measure the time until the alarm
deflection is observed on the monitor. sounds. Check the low rate alarm similarly (set
alarm for 40 bpm, change rate from 60 to 30
If the unit has an ungrounded or plastic case, bpm). Generally, alarm delays should not ex-
measure the CMRR with the unit resting on a ceed about 10 sec.
grounded metal plate. CMRR should meet the
manufacturer’s specification and be at least 10,000:1. 4.9 Repeated Discharge and Operating Time.Verify
that the battery meets hospital or manufacturer
4.5 Gain. Apply a 2 mV signal at a gain setting of specifications for number of defibrillation shocks
10 mV/mm (or ×1) and measure the displayed and monitor operating time. Units should meet
amplitude with a transparent scale. Verify that requirements with all functions operating (includ-
the displayed signal size changes appropriately ing alarms sounding) unless otherwise specified.
(within 10%) as the gain setting is changed. For
example, if a 2 mV signal produces a 20 mm Perform Item 2.12 on line-powered units to
deflection at a ×1 gain, the deflection should be verify that each unit is able to provide at least 10
36 to 44 mm at ×2. Test both the monitor display sequential defibrillation shocks.
and recorder.
4.6 QRS Sensitivity. If the monitor includes a QRS
Before returning to use
indicator or beeper or a heart rate meter, verify Return the energy select control to its normal set-
that the QRS detector circuit is functioning prop- ting. Before connecting the charger on battery-powered
erly. Connect an ECG simulator with variable units, check the battery condition to verify that there
output to the monitor, and set it for a rate of is adequate battery charge. If there is not, or if doubt
60 bpm. Vary the output amplitude over a exists, ensure that a suitable replacement defibrillator
range of 0.5 to 5 mV (use the monitor, display to is available, and allow the unit just inspected to charge
estimate amplitude if the simulator does not in an out-of-the-way location (i.e., where it will not be
have a calibrated output). The monitor should taken for use by clinical personnel). Battery-powered
reliably detect all beats and should not double- units should be connected to the charger, with the
count. It should not detect QRS amplitudes of charger plugged into a wall outlet and the charging
less than 0.15 mV. If the unit has a manual light on. For units with removable batteries that are
sensitivity control, check that it is functioning charged in a separate charger, replace the battery used
properly as evidenced by the need to change the during testing with a fully charged battery, and place
setting during this test. the used battery in the charger for proper charging.
4.7 Paper Speed. On units with a chart recorder, use Conduct a performance verification check, includ-
an ECG simulator set to 60 bpm or a signal or pulse ing pressing all the front-panel function buttons, to
generator set to 1 Hz that has been set or calibrated verify that the unit is in a standard service mode.
with a counter. If the interval between pulses is Performance-verification procedures are often in-
not within 10 msec of 1,000 msec, an appropriate cluded in the service manual.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Procedure/Checklist 407-0595
Defibrillators
Used For:
Defibrillators, Battery-Powered [11-134]
Defibrillators, Line-Powered [11-137]
Also Called: Cardioverters
Commonly Used In: Coronary and special care areas, emergency departments, operating rooms, resusci-
tation carts, patient care areas, emergency medical vehicles
Scope: Applies to battery- and line-powered defibrillators used with external and internal paddles and/or
disposable defibrillation electrodes; does not apply to units that have both defibrillation and monitoring
functions (see Defibrillator/Monitors Procedure/Checklist 408)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview also perform discharge testing at least once a week. A
User Checklist for Defibrillator/Monitor/Pacemakers
Defibrillators are critical resuscitation instruments. is included in Health Devices 1993 May-Jun; 22:291-2.
Their failure to perform effectively may result in the
death of a patient undergoing resuscitation or cause Citations from Health Devices
further cardiac damage or even death in a patient
undergoing elective cardioversion or emergency Daily checks of defibrillators [Consultant’s Corner],
cardioversion of a life-threatening arrhythmia. 1983 Mar; 12:120-1.
Line-powered defibrillators [Evaluation], 1983 Oct;
Failure to successfully defibrillate a patient may
12:291-314.
occur for a number of reasons, including inadequate
predefibrillation cardiopulmonary resuscitation (CPR) Defibrillating patients connected to electrocardio-
technique, operator error (e.g., poor paddle applica- graphs [Evaluation], 1984 Aug; 13:254.
tion), or depleted or defective batteries (the most com-
mon cause of defibrillator failure with battery-powered User error and defibrillator discharge failures [Haz-
units). There is no time to troubleshoot or correct even ard], 1986 Dec; 15:340.
minor difficulties during emergencies, since every m-
Deteriorating insulation on internal defibrillator pad-
inute of delay significantly decreases the probability of
dles [Hazard], 1987 Feb; 16:46.
a successful resuscitation attempt.
Defibrillator paddle resistance (continuity) testing
In addition to periodic inspection, clinical staff [User Experience NetworkTM], 1987 Feb; 16:55.
should perform inspections and ensure that battery-
powered units are charging at the beginning of each Disposable defibrillator pads and electrodes [Evalu-
work shift and after each use of the device. They should ation], 1990 Feb; 19:33-56.
009021 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
407-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Hewlett-Packard defibrillator/monitors and Darox R2 you have confirmed that the defibrillator is disarmed
electrodes [User Experience NetworkTM], 1990 Jul; (not charged) and preferably off.
19:246.
Testing input isolation requires the use of a line
ECG artifact and defibrillator/monitors [User Experi- voltage source. Although this source should include a
ence NetworkTM], 1991 Mar-Apr; 20:141. current-limiting resistor, use caution to avoid contact
with any portions of the circuit while it is energized.
Internal defibrillator paddles [User Experience Net-
workTM], 1991 Dec; 20:497-8. A defibrillator must be available in the event that
an emergency occurs during the inspection. Thus,
Use of Physio-Control Lifepak 8 defibrillator/monitors perform the inspection in the vicinity of the unit’s
with optional QUIK-PACE pacing cassette [User usual storage location, or ensure that a similar unit
Experience NetworkTM], 1992 May; 21:183. that the clinical staff is familiar with is available as a
Overheating of replacement batteries in Physio-Con- substitute.
trol Lifepak 6, 6s, and 7 defibrillator/monitors [Haz- Battery depletion may occur as a result of the in-
ard Update], 1992 Jun-Jul; 21:250. spection testing of battery-powered units. Ensure that
Defibrillator/monitors and external noninvasive pace- a replacement unit or a fully charged battery is avail-
makers [Evaluation], 1993 May-Jun; 22:212-94. able before you begin testing. Do not test all battery-
powered units in an area at the same time, since this
Defibrillator/monitors and external noninvasive pace- will leave the staff inadequately equipped to handle
makers [Evaluation Update], 1993 Dec; 22:579-82. emergencies until the batteries recharge.
Misalignment of mating cable and defib cassette con-
nectors on Physio-Control Lifepak 8 defibrilla- Procedure
tor/monitor [Hazard], 1993 Dec; 22:595-7. Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and serv-
Fires from defibrillation during oxygen administration
ice manuals; be sure that you understand how to oper-
[Hazard], 1994 Jul; 23:307-9.
ate the equipment and the significance of each control
Spontaneous charging of Hewlett-Packard 43100A de- and indicator. Also determine whether any special in-
fibrillator/monitor used with anterior/posterior pad- spection or preventive maintenance procedures or fre-
dle set during monopolar electrosurgery [Hazard], quencies are recommended by the manufacturer.
1994 Oct-Nov; 23:455-6.
Defibrillator energies may be specified in either
joules (J) or watt-seconds; these are equivalent units
Test apparatus and supplies (i.e., 1 J = 1 watt-second).
Defibrillator analyzer
Ground resistance ohmmeter
1. Qualitative tests
Leakage current meter or electrical safety analyzer 1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condi-
Stopwatch or watch with a second hand tion. Be sure that plastic housings are intact,
ECG simulator and ECG monitor (only for units that all assembly hardware is present and tight,
with synchronization capability) and that there are no signs of spilled liquids or
other serious abuse.
Oscilloscope (acceptance testing only)
Isolation test supply (included in some electrical 1.2 Mount. If the device is mounted on a stand or
safety analyzers; acceptance testing only) cart, examine the condition of the mount. If it is
attached to a wall or rests on a shelf, check the
Special precautions security of this attachment.
CAUTION: The high voltage present on defibrillator 1.3 Casters/Brakes. Check the condition of cart
paddles during discharge is extremely dangerous and casters. Look for accumulations of lint and
possibly lethal. Never perform testing alone. A second thread around the casters, and be sure that they
person must be present to summon help and/or apply turn and swivel, as appropriate. Check the op-
CPR in the event of an emergency. Never hold or contact eration of brakes and swivel locks, if the cart is
the conductive electrode portion of the paddles unless so equipped.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Defibrillators
1.4 AC Plug. Examine the AC power plug for dam- cleanliness. Alert clinical personnel responsible
age. Attempt to wiggle the blades to determine for the instrument to the presence of dried elec-
that they are secure. Shake the plug and listen trode gel, physiologic fluids, or debris on the
for rattles that could indicate loose screws. If paddle surface or handles. Dirty electrodes pre-
any damage is suspected, open the plug and vent good electrical contact and often cause
inspect it. burns. Electrode gel or other debris on the insu-
lating portion of the paddle can cause operator
If the device is mounted on a cart that has shocks. Clean the paddles if needed, including
electrical receptacles for additional equipment, electrode surfaces and handle seams, and ensure
insert an AC plug into each and check that it is that they are completely dry before proceeding
held firmly. Inspect resuscitation cart recepta- with any testing.
cles, including testing for wiring (e.g., using an
outlet tester) and tension of all three connec- Confirm that an adequate supply of ECG elec-
tions. Also inspect the resuscitation cart plug for trodes and disposable defibrillation electrodes (if
damage as described above. used) are available and that they are stored
properly and are within their expiration dates.
1.5 Line Cord. Inspect the cord (including resusci-
tation cart line cord, if appropriate) for signs of 1.13 Controls/Switches. Examine all controls and
damage. If damaged, replace the entire cord or, switches for physical condition, secure mount-
if the damage is near one end, cut out the defec- ing, and correct motion. Where a control should
tive portion. Be sure to wire a new power cord or operate against fixed-limit stops, check for
plug with the correct polarity. Check line cords proper alignment, as well as positive stopping.
of battery chargers. Check membrane switches for membrane dam-
age (e.g., from fingernails, pens). During the
1.6 Strain Reliefs. Examine the strain reliefs at
course of the inspection, check that each control
both ends of the line cord. Be sure that they hold
and switch performs its proper function.
the cord securely.
If the unit has redundant control functions
1.7 Circuit Breaker/Fuse. If the device has a switch-
(e.g., a charge button on the front panel and on
type circuit breaker, check that it moves freely. If
a paddle), ensure that both controls function
the device is protected by an external fuse, check
properly. Verify that activating just one paddle
its value and type against that marked on the
discharge button will not discharge the unit
chassis, and ensure that a spare is provided.
(both buttons must be pressed simultaneously to
1.9 Cables. Inspect the cables of internal and exter- discharge). A front-panel discharge button
nal paddles, disposable defibrillation electrodes should control only internal paddles (or dispos-
(if applicable), and synchronizer cables for their able defibrillator electrodes on some units) and
strain reliefs and general condition. Examine should not cause discharge when external pad-
cables carefully to detect breaks in the insulation dles are connected.
and to ensure that they are gripped securely in
1.17 Battery/Charger. Inspect the physical condi-
the connectors at each end to prevent rotation or
tion of batteries and battery connectors, if read-
other strain.
ily accessible. Verify that the charger of
1.10 Fittings/Connectors. Examine all cable connec- battery-operated units is plugged into a live AC
tors for general condition. Electrical contact outlet and that the charger is attached to the
pins or surfaces should be straight and clean. defibrillator (i.e, charger cable is attached, unit
Verify that leads and electrodes are firmly is firmly seated into charging stand or mount,
gripped in their appropriate connectors. During instrument end of line cord is attached, and
major inspections, disconnect the paddle connec- charging light is on). For units with removable
tors and look for misaligned pins, damaged re- batteries that are charged in a separate charger,
ceptacles, and carbon deposits from arcing. verify that the batteries are properly installed
and that the charging, or ready, light is on.
1.11 Paddles/Electrodes. Confirm that special pad- Inform clinical personnel of any deficiencies or
dles (e.g., pediatric, internal) and electrodes improper use.
(e.g., disposable defibrillation electrodes) are
available if appropriate for the area of use. Ex- Perform the inspection with the unit on battery
amine all paddles for physical condition and power to check that the defibrillator batteries are
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
charged and can hold a charge. Check battery exposed (unpainted and not anodized) metal on
capacity by activating the battery test function the defibrillator chassis (and charger if applica-
or measuring the battery-powered operating ble). We recommend a maximum of 0.5 Ω.
time. When it is necessary to replace a battery,
label it with the date. 2.2 Chassis Leakage Current. Measure chassis
leakage current to ground with the grounding
Some batteries require periodic deep dis- conductor of plug-connected equipment tempo-
charges and recharging to maintain maximum rarily opened and the unit off, on, charging, and
capacity. If the manufacturer recommends this charged. Record the maximum leakage current.
procedure, verify that it is being performed on Leakage current from chassis to ground should
schedule. not exceed 300 µA.
1.18 Indicators/Displays. During the course of the
inspection, confirm the operation of all lights, 2.3 Paddle Continuity. Use an ohmmeter to verify
indicators, meters, gauges, and visual displays continuity from each paddle (internal and exter-
on the unit and charger, if so equipped. Be sure nal) to the appropriate pin of the paddle connec-
that all segments of a digital display function. tor. Wiggle, bend, and pull the cable, especially
near the paddle and connector, to check that
1.21 Audible Signals. Operate the device to activate continuity is not affected. (Current may jump
any audible signals (e.g., charge tone). Confirm across a small break in the paddle lead and may
appropriate volume, as well as the operation of not be detected during defibrillator output tests.
a volume control. An ohmmeter test will detect such a discontinuity
before it gets worse.) This check should also be
1.22 Labeling. Check that all necessary placards, la- done for the reusable cable used with disposable
bels, and instruction cards are present and leg- defibrillation electrodes. Internal paddles may
ible. require more frequent continuity checks. The
1.23 Accessories (gel, pads, or electrodes). Verify that resistance from the paddle to the appropriate pin
defibrillator gel, disposable defibrillator pads, or of the paddle connector should not exceed 0.15 Ω.
disposable defibrillator electrodes are stored
with the unit and that they are within their 2.4 Energy After 60 Sec. Deterioration of the energy
expiration dates. Confirm that defibrillator gel storage capacitors in some defibrillators results
is being used, not skin lubricant or ultrasound or in charge leakage after the charging circuit had
TENS gel. Notify appropriate clinical personnel been deenergized. In these units, it is possible
if any accessories are missing. for the available energy to decrease if the unit is
not discharged at the earliest possible moment.
1.24 Internal Discharge of Stored Energy. To protect Use the following test to identify this deficiency.
personnel from accidental shock, it should be
possible to discharge the stored energy safely in Charge the defibrillator to its maximum set-
the event that the operator decides not to use the ting, but do not discharge it for 1 min. The
defibrillator after it has been charged. Verify delivered energy should be at least 85% of that
that the unit releases the stored energy when the obtained when the unit is discharged immedi-
power is turned off. If the unit has a front-panel ately (as in Item 2.10) and should meet manu-
button for this purpose, verify proper operation. facturer specifications for charge leakage.
(Some units are designed to intentionally bleed
1.25 Synchronizer. If the unit has a synchronization or discharge the capacitor charge if the defibril-
mode, verify that the unit will not discharge lator is not discharged within a set time period.
while in this mode when no ECG signal is pre- These units should meet the manufacturer’s
sent and that it will discharge when a simulated specifications.)
ECG signal is applied.
2.5 Internal Paddle Energy Limit. Defibrillator out-
2. Quantitative tests put, when used with internal paddles, should not
2.1 Grounding Resistance. Using an ohmmeter, exceed 50 J. Test this feature on any unit that is
electrical safety analyzer, or multimeter with located where it may be used with internal pad-
good resolution of fractional ohms, measure and dles or that is portable and may be moved to such
record the resistance between the grounding pin a location. Connect the internal paddles, charge
of the power cord (or charger power cord) and the unit to maximum energy, and discharge it
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Defibrillators
into the defibrillator analyzer. Verify that the The time to charge to maximum energy should
output does not exceed 50 J. not exceed 15 sec. The output energy should
remain within 4 J or 15% of the selected energy
2.10 Output Energy. During major inspections, throughout the test.
measure output energy at minimum, intermedi-
ate, and maximum energy settings. If the defi- CAUTION: Do not perform this test on all
brillator is commonly used for cardioversion, a battery-operated defibrillators in an area on the
50 J level would be satisfactory for the interme- same day unless provisions are made for backup
diate range. units or spare charged batteries. Batteries may
take considerable time to recharge, and a fully
At each energy level, record the control set- charged unit must be available for emergencies.
ting, indicated energy (on the unit’s energy me-
ter), and delivered energy (measured by an 3. Preventive maintenance
analyzer) after discharging the defibrillator into 3.1 Clean the exterior and paddles.
the analyzer as soon as it is charged.
3.4 Replace the battery if any of the test procedures
At its maximum setting, the unit should be indicate a weak or defective battery, even after
able to deliver at least 250 J. The output energy charging for 12 hr or more.
should be within 4 J at low settings (below 25 J) Some users have also reported that periodic
or 15% of the set energy (and the indicated en- prophylactic battery replacement, either annu-
ergy, if so equipped) at higher energies. ally or every other year, increases reliability and
decreases service calls. In such a case, mark the
If the output is unusally low at very low con- date of the battery replacement on the battery or
trol settings, check for a break in the cables or a unit and check it during each inspection. Per-
defective connector. form the inspection after battery replacement
and a suitable charge period.
During minor inspections, verify output at
only one energy level. Use the defibrillator’s Since some units have more than one battery,
internal test load, if so equipped. Typically, this be sure that all batteries are checked, main-
provides a numeric or a pass/fail indicator to tained, and replaced as required.
verify that energy was delivered.
4. Acceptance tests
2.11 Charge Time and Max Energy (10th Charge). In
Conduct major inspection tests for this procedure
resuscitation attempts, it is not uncommon for
and the appropriate tests in the General Devices Pro-
the operator to call for multiple defibrillation
cedure/Checklist 438.
shocks in rapid succession. Battery-powered de-
fibrillators may not have sufficient energy left in CAUTION: Do not measure paddle leakage current
their batteries to deliver 10 shocks. These defi- with the unit charged or charging or during discharge.
ciencies are best discovered during periodic in-
spections, rather than during clinical use. AAMI DF-2-1989, Standard for Cardiac Defibrilla-
tor Devices, calls for applying isolated input risk cur-
Charge battery-powered units to maximum rent tests (source, sink, and interlead) to defibrillator
energy and discharge 10 times through the ana- paddles, but with limits of 100 µA for external paddles
lyzer (but first verify that the analyzer load will and 50 µA for internal paddles.
not be damaged by repeated discharge). On the In addition, perform the following tests.
10th cycle, record the charging time (i.e., the
time it takes the meter to equilibrate or the ready 4.1 Synchronizer Operation. Check the synchroniz-
light to come on) and the delivered energy. To ers of units so equipped. An independent monitor
avoid excessive battery depletion, stop the test must be used in conjunction with the defibrilla-
and record the number of discharges and the tor to allow synchronized operation (although
values measured if the charging time exceeds 15 this can be done, AAMI does not recommend it).
sec before the 10th discharge. Also stop the test The thoroughness of this test will depend upon
if the battery-condition meter indicates a weak the availability of test equipment. Connect the
battery or, on some defibrillators, if the internal monitor that will be used clinically to the defi-
circuitry terminates the charge early. brillator. Supply an ECG signal from an ECG
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
simulator to the monitor to trigger the discharge 4.2 Internal Paddle Energy Limit. During accep-
of the defibrillator into a 50 Ω load (e.g., a defi- tance testing, perform Item 2.5 on all units
brillator analyzer). Set the defibrillator to de- equipped with this feature, regardless of the
liver low output energy (50 J or less). Confirm location intended for the device.
that, with the ECG simulator off, the defibrilla-
4.3 Repeated Discharge. Verify that the battery
tor does not discharge. With a signal applied,
meets hospital or manufacturer specifications
confirm that the synchronizer marker or other
for the number of defibrillator shocks that can be
indicator is functioning properly.
delivered. Perform Item 2.11 on line-powered
Use a dual-channel oscilloscope to note the units to verify that the unit is able to provide at
time delay between the peak of a QRS pulse least 10 sequential defibrillation discharges.
(from an ECG simulator) and the defibrillator 4.4 Integral Output Tester. Check the operation and
pulse (from a defibrillator analyzer). Use the accuracy of any integral defibrillator test load, if
ECG signal to trigger the oscilloscope’s sweep. so equipped.
Some defibrillator analyzers have synchronizer
test functions. With an ECG amplitude sufficient Before returning to use
to activate the marker or indicator, the defibril- Return the energy-select control to its normal set-
lator should discharge within 60 msec or less ting. Before connecting the charger on battery-pow-
following the peak of the R wave, after the dis- ered units, check the battery condition to verify that
charge buttons are depressed. The monitor there is an adequate battery charge. If there is not, or
should provide its synchronizing signal within if doubt exists, ensure that a suitable replacement
35 msec of the R wave peak. The delay time defibrillator is available, and allow the unit just in-
between the application of the most recent syn- spected to charge in an out-of-the-way location (i.e.,
chronizing signal from the monitor and the dis- where it will not be taken for use by clinical personnel).
charge should not exceed 25 msec. Thus, the Otherwise, connect battery-powered units to the
overall delay from the defibrillator and monitor charger, plug the charger into a wall outlet, and verify
should not exceed 60 msec. that the charging light is on.
Most units will trigger on the first QRS after For units with removable batteries that are charged
depressing buttons, although some units are de- in a separate charger, replace the battery used during
signed to delay until the second or third QRS to testing with a fully charged battery and place the used
avoid unintentional discharges. battery in the charger for proper charging.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 409-0595
ECG Monitors
Used For:
ECG Monitors [12-599]
Also Called: Cardiac monitors
Commonly Used In: Operating rooms, emergency rooms, critical care units as part of a physiologic
monitoring system, other special care areas, cardiac catheterization laboratories
Scope: Primarily applies to stand-alone ECG monitors (line or battery powered); appropriate for use in
conjunction with other procedures when inspecting physiologic monitoring systems that include multiple
physiologic parameters; adaptable for use with ECG telemetry systems and systems with central stations; also
applies to rate meters and direct writers for monitors with these features; does not apply to ECG arrhythmia
monitors or to monitors in defibrillator/monitor units (use Defibrillator/Monitors Procedure/Checklist 408)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
*
This procedure is generally not required for a permanently installed system if the hospital routinely performs
a visual inspection of the area, paying reasonable attention to the monitors.
Overview Physiologic patient monitors [Evaluation], 1991 Mar-
Apr; 20:81.
ECG monitors are routinely used on patients with
known or suspected cardiac arrhythmias. The moni- ECG artifact in the OR [User Experience NetworkTM],
tors display the patient’s electrocardiogram so that 1991 Mar-Apr; 20:140.
those attending the patient may continuously observe
Thermal injuries and patient monitoring during MRI
the electrical activity of the heart. Since the monitor is
studies [Hazard], 1991 Sep; 20:362.
used only to observe the patient’s basic cardiac
rhythm, it need not meet the accuracy and fidelity Physiologic patient monitors [Evaluation update],
criteria expected of an electrocardiograph. 1992 Mar-Apr; 21:123-8.
Citations from Health Devices Risk of electric shock from patient monitoring cables
and electrode lead wires [Hazard], 1993 May-Jun;
Artifacts from piezoelectric voltages [Consultant’s Cor- 22:301.
ner], 1982 Nov; 12:27.
Patient monitoring systems [Evaluation], 1985 Mar- Test apparatus and supplies
Apr; 14:143. ECG simulator (calibrated output amplitudes and
GIGO: A compendium of ECG monitoring problems, rates may be required for some tests)
1985 Mar-Apr; 14:158. Leakage current meter or electrical safety analyzer
009026 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
409-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Ground resistance ohmmeter Some monitors or monitoring systems provide mul-
tilead ECG signal processing and display (simultane-
The following equipment is necessary during accep- ous display of two ECG leads). Conduct display quality
tance testing only: and performance tests on each channel. On single-
Signal generator channel units that have lead switching, except where
otherwise indicated, all tests can be performed in one
Attenuator
lead, using the appropriate electrode leads (e.g., lead
Oscilloscope I, using LA and RA as inputs).
Transparent metric scale When a monitor is part of a system with a remote or
Stopwatch or watch with a second hand central station display, use a separate inspection form
to record results for each display. Verify interactive
Special precautions functions from each bedside (e.g., central station alarm
sounds, chart recorder activates when heart rate ex-
Testing monitor isolation requires the use of a line
ceeds set limits). Test displays for each bedside sepa-
voltage source. Although this source should include a
rately, but test common elements (e.g., quality of
current-limiting resistor, use caution to avoid contact
central chart recorder tracing) from only one bedside.
with any portions of the energized circuit.
This is most easily accomplished with two people.
Inspection testing may deplete the battery of bat-
tery-powered units. Ensure that a replacement unit or 1. Qualitative tests
a fully charged battery is available before you begin 1.1 Chassis/Housing. Examine the exterior of the
testing. Do not test all the units in an area at one time, unit for cleanliness and general physical condi-
since this will leave the staff inadequately equipped. tion. Be sure that plastic housings are intact,
that all assembly hardware is present and tight,
Procedure and that there are no signs of spilled liquids or
Before beginning an inspection, carefully read this other serious abuse.
procedure and the manufacturer’s instruction and
1.2 Mount. If the device is mounted on a stand or
service manuals; be sure that you understand how to
cart, examine the condition of the mount. If it is
operate the equipment, the significance of each control
attached to a wall or rests on a shelf, check the
and indicator, and the alarm capabilities. Also deter-
security of this attachment.
mine whether any special inspection or preventive
maintenance procedures or frequencies are recom- 1.3 Casters/Brakes. If the device moves on casters,
mended by the manufacturer. check their condition. Look for accumulations of
lint and thread around the casters, and be sure
Enter cross-referenced data related to the ECG that they turn and swivel, as appropriate. Check
monitor at the top of the inspection form. Since the the operation of brakes and swivel locks, if the
monitor may be installed in a mainframe along with unit is so equipped. Conductivity checks, where
other removable modules (e.g., blood pressure unit, appropriate, are usually done more efficiently as
body temperature unit, recorder), assign a separate part of a check of all equipment and furniture of
control number to the mainframe and to each discrete an area (see Procedure/Form 441, Conductive
module. Enter the mainframe control number in the Furniture and Floors).
Control No. space of the inspection form to identify the
entire device. This will help you locate the whole moni- 1.4 AC Plug. Examine the AC power plug for dam-
tor or an individual module if follow-up action is age. Attempt to wiggle the blades to determine
needed. Enter all module control numbers in the Sys- that they are secure. Shake the plug and listen
tem Components box on the form, and indicate which for rattles that could indicate loose screws. If
are covered on separate forms. any damage is suspected, open the plug and
inspect it.
If the device is configured (i.e., different functions
are not in removable modules but are contained within 1.5 Line Cord. Inspect the cord for signs of damage.
a single integral housing), assign only one control If damaged, replace the entire cord or, if the
number. In the System Components box, list any func- damage is near one end, cut out the defective
tions that will be inspected but recorded on separate portion. Be sure to wire a new power cord or plug
inspection forms (e.g., blood pressure), and note the with the same polarity as the old one. Also check
use of other forms. line cords of battery chargers.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
ECG Monitors
1.6 Strain Reliefs. Examine the strain reliefs at 1.17 Battery/Charger. Inspect the physical condi-
both ends of the line cord. Be sure that they hold tion of batteries and battery connectors, if read-
the cord securely. ily accessible. Check operation of
battery-operated power-loss alarms, if so
1.7 Circuit Breaker/Fuse. If the device has a equipped.
switch-type circuit breaker, check that it moves
freely. If the device is protected by an external Perform the inspection with the unit on bat-
fuse, check its value and type against that tery power or operate the unit on battery power
marked on the chassis, and ensure that a spare for several minutes to check that the batteries
is provided. are charged and can hold a charge. Check battery
capacity by activating the battery test function
1.9 Cables. Inspect the patient cable and leads and or measuring the output voltage. When it is
their strain reliefs for general condition. Exam- necessary to replace a battery, label it with the
ine cables carefully to detect breaks in the insu- date. Check the condition of the battery charger
lation and to ensure that they are gripped and, to the extent possible, confirm that it does,
securely in the connectors of each end to prevent in fact, charge the battery.
rotation or other strain. Connect the unit to an
ECG simulator and verify that an adequate trace Some batteries require periodic deep discharges
is received at each patient lead selection. Flex and recharging to maintain maximum battery ca-
the patient cable near each end to verify that pacity. If this is recommended by the manufac-
there are no intermittent faults. turer, verify that it is being performed on schedule.
1.18 Indicators/Displays. During the course of the in-
1.10 Fittings/Connectors. Examine all cable connec-
spection, confirm the operation of all lights, indi-
tors for general condition. Electrical contact
cators, meters, and visual displays on the unit and
pins or surfaces should be straight and clean.
the charger (if appropriate). Be sure that all seg-
Verify that leads and electrodes are firmly
ments of a digital display function. Observe a
gripped in their appropriate connectors.
simulated ECG signal on a CRT display, and verify
1.11 Electrodes. Confirm that an adequate supply of compliance with the following criteria:
electrodes is on hand, and check the electrodes’ The baseline should stay in focus across the
physical condition. display.
1.13 Controls/Switches. Before moving any controls The baseline should be horizontal and should
and alarm limits, check their positions. If any of not be noticeably sloped or bowed.
them appear inordinate (e.g., a gain control at The pulses from an ECG simulator should be
maximum, alarm limits at the ends of their range), regularly spaced (uneven spacing indicates a
consider the possibility of inappropriate clinical sweep nonlinearity).
use or of incipient device failure. Record the set-
tings of those controls that should be returned to All portions of a simulated ECG waveform
their original positions following the inspection. should be clear and visible, including the P-
wave and QRS.
Examine all controls and switches for physical When the vertical position of the baseline is
condition, secure mounting, and correct motion. varied by adjusting the vertical position con-
Check that control knobs have not slipped on trol, the baseline should move throughout
their shafts. Where a control should operate most of the vertical height of the display.
against fixed-limit stops, check for proper align- There should be no distortion in the baseline
ment, as well as positive stopping. Check mem- as it is moved up or down on the screen. In
brane switches for membrane damage (e.g., from monitors that incorporate a self-centering
fingernails, pens). During the course of the in- baseline (and thus lack a position control), the
spection, check that each control and switch per- baseline should be correctly positioned.
forms its proper function.
Ambient light should not affect the visibility
Check alignment of touchscreen sensors. Ver- of the trace. (If monitors are located so that
ify that functions are activated when the center ambient light reflects from the face of the
of the desired function box is touched. display, making the ECG difficult to see, con-
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
trol the light or use a filter over the display step response test (Item 1.19) on the direct
faceplate.) writer.
“Burn spots” should not be visible on the cath-
ode ray tube. (If the intensity is set too high, 2. Quantitative tests
the phosphor may “burn”; the cathode-ray
tube face will be discolored if this condition 2.1 Grounding Resistance. Using an ohmmeter,
exists.) electrical safety analyzer, or multimeter with
60 Hz or other noise (interference) should not good resolution of fractional ohms, measure and
be superimposed on the baseline with the record the resistance between the grounding pin
ECG simulator attached. Baseline interfer- of the power cord and exposed (unpainted and
ence may be apparent as a thick baseline at not anodized) metal on the defibrillator chassis
high gain settings but should not be visible (and charger chassis if appropriate). We recom-
throughout the lower two-thirds of the gain mend a maximum of 0.5 Ω. If the system is
control range. modular, verify grounding of the mainframe and
each module.
1.19 1 mV Step Response. Depress and hold the 1 mV
calibration button for about 3 sec (or apply an 2.2 Chassis Leakage Current. Measure chassis
external 1 mV pulse if the unit does not have a leakage current to ground with the grounding
calibration pulse). The trace should exhibit a conductor of plug-connected equipment tempo-
sharp square-cornered leading edge that is nei- rarily opened. Operate the device in all normal
ther rounded nor spiked (any spike should be less modes, including on, standby, and off, and record
than 10%). After 1 sec, the pulse should have the maximum leakage current. Chassis leakage
decayed no more than half its original amplitude current to ground should not exceed 300 µA.
(see Figure 1). With the gain set to yield about
20 mm deflection for a 1 mV input (×2 or 1/2 If a bedside or central station monitor is
mV/div), compare the amplitude of the internal grounded through system interconnections in
calibration pulse and an external 1 mV signal addition to power-line grounding (and is used
(from a calibrated ECG simulator). At a 20 mm only in this configuration), do not disconnect the
deflection, they should be within 2 mm (±10%) of monitor from the system to measure chassis
each other. leakage current during routine inspections.
Verifying low grounding resistance is adequate.
1.20 Alarms. Operate the device in such a way as to
activate each audible and visual alarm. Check 2.10 Rate Calibration. Using simulated ECG rates of
for adequate alarm tone volume and any asso- 60 and 120 pulses per minute, verify that the
ciated features, such as automatic direct heart rate indicator displays a rate within 5% or
writer activation or display freeze function. If 5 bpm, whichever is greater, of the set rate (55
the device has an alarm-silence feature, check to 65 bpm, 119 to 126 bpm). Verify that the QRS
that the unit resets automatically or that the visual and audible indicators are functioning.
manual reset functions. Check bed-to-bed and
bed-to-central station alarm networking
(where appropriate).
1.21 Audible Signals. Operate the device to activate
any audible signals. Confirm appropriate vol-
ume, as well as the operation of a volume control.
1.22 Labeling. Check that all necessary placards, la-
bels, and instruction cards are present and leg-
ible.
Figure 1. The calibration pulse or step response leading
1.24 Direct Writer. If the unit has a direct writer, edge should have square corners (left). Slight rounding
confirm that it operates smoothly, that the paper (middle) or small overshoot is acceptable. Excessive
feeds evenly and does not stray from side to side, rounding or overshoot (right) indicates the need for
and that the trace is of good quality (i.e., dark adjustment.
and thin) at all paper speeds. Perform the 1 mV
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
ECG Monitors
2.11 Rate Alarm. Use the same setup as for the pre- Common mode rejection is needed in monitors
vious test. For typical low- and high-rate alarm because of the presence of stray signals common
settings of 40 and 120 bpm, respectively, verify to all input leads primarily at power-line fre-
that the alarm activates when the input rate is quency (60 Hz). While these signals are too m-
set just below or above the respective rate alarm inute to be hazardous, they can interfere with
settings. The difference between the rate dis- the ECG display of a monitor with a low CMRR
played on the rate indicator and that at which at 60 Hz.
the alarm is activated should not exceed 5% or 5
bpm, whichever is greater. The CMRR is defined as:
Differential mode deflection factor or DMD (MM / mV)
3. Preventive maintenance CMRR =
Common mode deflection factor or CMD (MM / mV)
3.1 Clean the exterior, rollers, and platen, if needed.
A deflection factor is the change in trace posi-
3.2 Lubricate the chart recorder paper drive per the tion corresponding to a given input voltage to the
manufacturer’s recommendations, if required. monitor. Use an unbalanced CMRR measure-
ment that includes a 5,000 Ω resistor in series
3.4 Replace filters and batteries, if required. Some with one of the input leads to the monitor, to
units have air filters that accompany the cooling simulate unequal impedances in the elec-
fan. These filters should be checked and replaced trode/skin interface of the monitor electrodes, as
if needed. commonly occurs in practice.
If any of the test procedures indicate a weak Since most common mode voltage in the hos-
or defective battery, even after charging for 12 pital is at 60 Hz, it is most significant to measure
hr or more, replace the battery. Some users have the CMRR at or near that frequency. Using the
also reported that periodic, prophylactic battery test setup shown in Figure 2, apply a sinusoid
replacement, either annually or every other test signal of 1 mV peak-to-peak at about 60 Hz
year, increases reliability and decreases service to the monitor. A frequency of 55 Hz is often
calls. If the battery is replaced, mark the date of used to minimize interference from line fre-
the replacement on the battery or unit. Perform quency noise. Turn the monitor gain so that the
the inspection after battery replacement and a deflection is at least 20 mm. Measure the deflec-
suitable charge period. tion (mm), and record it on the inspection form
as the differential mode deflection factor. Since
4. Acceptance tests the input signal for this measurement is 1 mV,
the differential mode deflection factor expressed
Conduct major inspection tests for this procedure in mm/mV is numerically equal to the resultant
and the appropriate tests in the General Devices Pro- deflection in mm. Do not vary the gain of the
cedure/Checklist 438. Most ECG monitors should meet monitor or the signal frequency for the remain-
the requirements for isolated input devices for ECG der of this test. Record the frequency on the
lead-to-ground, interlead, and input isolation tests. inspection form.
In addition, perform the following tests.
4.1 Common Mode Rejection Ratio (CMRR). The
ECG monitor includes a differential amplifier so
that it can display the voltage difference between
two electrodes (the RA and LA in lead 1) while
using a third electrode (RL) as a reference. If the
same, or common, voltage is applied to RA and
LA simultaneously, there should be no output
from the differential amplifier because the volt-
age difference between the two inputs is zero.
The extent to which a differential amplifier pro-
duces no output when the same signal is applied
to both inputs is called its common mode rejec- Figure 2. Signal input test setup.
tion ratio.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
Use the test setup shown in Figure 3 for the Connect an ECG simulator with variable output
second part of this measurement. Note that to the monitor and set it for a rate of 60 bpm.
there is only one connection from the output of Vary the output amplitude over a range of 0.5 to
the attenuator to the patient leads. The other 5 mV (use the monitor display to estimate ampli-
output terminal is grounded. It is essential that tude if the simulator does not have a calibrated
all instruments used in this test be connected to output). The monitor should reliably detect all
beats and should not double-count. It should not
detect QRS amplitudes of less than 0.15 mV. If
the unit has a manual sensitivity control, check
that it is functioning properly as evidenced by
the need to change the setting during this test.
4.4 Paper Speed. Use an ECG simulator set to 60
bpm or a signal or pulse generator that has been
set to 1 Hz with a calibrated counter. If the
interval between pulses is not within 10 msec of
1,000 msec, an appropriate correction should be
made in calculating paper speed. Paper speed
should be accurate to within 2%. At a chart speed
of 25 mm/sec and a pulse interval of 1,000 msec
Figure 3. Common mode rejection ratio test setup. (60 bpm on an ECG simulator), the distance
between the first and last of five successive peaks
should be 100 ±2 mm; at a chart speed of 50
a common ground to minimize noise. mm/sec, the distance between the first and the
Increase the amplitude of the sinusoid signal last of five successive peaks should be 200 ±4 mm.
(10 V peak-to-peak) until some measurable de- 4.5 Alarm Delay. In addition to checking rate
flection is observed on the monitor. Calculate the alarm accuracy (Item 2.11), use the same test
common mode deflection factor by dividing the setup to determine alarm delay. First, set the
resultant deflection (in mm) by the input signal high-rate alarm to 100 bpm and the ECG simu-
(in mV). The CMRR can then be calculated as the lator to 60 bpm. Quickly change the simulator
differential mode deflection factor divided by the rate to 120 bpm and use a stopwatch or a watch
common mode deflection factor. with a second hand to measure the time until the
If the unit has an ungrounded or plastic case, alarm sounds. Check the low-rate alarm simi-
measure the CMRR with the unit resting on a larly (set alarm for 40 bpm, change rate from 60
grounded metal plate. CMRR should meet the to 30 bpm). Generally, alarm delays should not
manufacturer’s specification and be at least exceed 10 sec.
10,000:1.
4.6 Battery Operating Time. If the unit can operate
4.2 Gain. Apply a 2 mV signal at a gain setting of on battery power, verify that it meets hospital or
10 mV/mm (or ×1) and measure the displayed manufacturer specifications for operating time.
amplitude with a transparent scale. Verify that Units should meet requirements with all func-
the displayed signal size changes appropriately tions operating (including alarms sounding) un-
(within 10%) as the gain setting is changed. For less otherwise specified by the manufacturer.
example, if a 2 mV signal produces a 20 mm
deflection (at a ×1 gain), the deflection should be Before returning to use
36 to 44 mm at ×2. Test both the monitor display
Return controls and alarm limits to their original
and recorder.
positions, and make sure that the unit is not left in a
4.3 QRS Sensitivity. If the monitor has a QRS indi- service mode. Check the battery condition meter indi-
cator or beeper or a heart rate meter, verify that cator on battery-powered units to verify that there is
the QRS detector circuit is functioning properly. adequate charge.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Form 437-0595
Electrical Receptacles
Used For:
Receptacles, Hospital Grade [15-859]
Also Called: Electrical outlets
Scope: Applies to three-wire parallel-blade grounding-type electrical receptacles used in grounded electrical
distribution systems throughout the hospital; does not apply to explosion-proof or other special types of
receptacles (for information on testing of isolated power systems, see Procedure/Form 439)
Risk Level: ECRI Recommended, Low; Hospital Assessment,
ECRI-Recommended Interval: See Overview below for NFPA requirements and ECRI recommendations
Overview 99 requires semiannual testing in wet areas in existing
facilities that are not supplied with special protective
A defective or deteriorating electrical system exposes systems, such as ground fault circuit interrupters
patients and staff to the risk of electrical shock and [GFCIs] or isolated power.)
potential interruption of power required to operate
medical equipment. A periodic inspection program NFPA 99, Section 3.5.2.1, specifies that voltage and
designed to detect and correct deficiencies at each impedance tests be performed to measure the effective-
receptacle is required to reduce these risks. ness or quality of the grounding system. This section
specifies that these tests be performed before acceptance
NFPA 99, 1993 Edition, specifies that receptacles in on all new construction and when the electrical system
general care areas be tested every 12 months and that has been altered or replaced. Sections 3.5.2.2 and
those in critical care areas and designated wet locations 3.6.2.3.1 require that the physical integrity, polarity,
be tested every 6 months. (See the Patient Care Areas retention force of the grounding blade, and continuity of
box for explanations of the italicized terms used in the the grounding circuit of each receptacle be verified every
NFPA standard.) NFPA permits extending the inter- 12 months in general care and wet locations and every 6
vals if documented performance data justify longer months in critical care areas. The ECRI procedures
intervals. Initially, inspections should be conducted at given in the sections on Ground Potentials and Ground-
the specified 12- and 6-month intervals. The data ob- ing Resistance below cover both of these requirements.
tained during these initial inspections should then be
examined and used to determine appropriate intervals. A power plug and receptacle combination should:
Provide a safe, reliable means of connecting and
Although there is no formal guideline on an acceptable disconnecting an electrically powered device
number of defects, ECRI believes that the testing inter-
val can be extended if fewer than 2% of the receptacles Permit only devices intended for use with that sup-
in an area require replacement or other corrective action. ply to be connected
A recent study by ECRI of more than 800,000 receptacles Allow only one orientation of plug contacts in the
inspected between 1987 and 1994 indicates that more receptacle
than 13% failed to meet one or more of the criteria in this
procedure. However, little is known about the history of Have low electrical contact resistance between the
these receptacles. Annual testing should be adequate in plug and the receptacle
areas where receptacles receive frequent use; other areas Withstand normal use and reasonable mechanical
may require even less frequent testing. (Note that NFPA abuse
094735 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
437-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
have higher current or voltage ratings, are used in
Patient Care Areas hospitals for housekeeping equipment, food carts, and
mobile x-ray units. Explosion-proof plugs and recepta-
In specifying testing requirements for electrical cles are required in operating rooms where flammable
receptacles, NFPA refers to general care areas, anesthetics are used and in other areas where arcing
critical care areas, and wet locations; these terms when inserting or removing a plug could ignite flam-
are explained below. mable gases.
General care areas are patient bedrooms, ex-
Only two conductors are required to operate a 120 V
amining rooms, treatment rooms, clinics, and
device, and two-wire parallel-blade plugs and receptacles
similar areas in which it is intended that the
have been in common use for many years. One of these
patient shall come into contact with ordinary
conductors is connected to earth ground near the point
appliances, such as a nurse call system, electric
where the power enters the building. This conductor,
beds, examining lamps, a telephone, and enter-
colored white, is commonly called the neutral wire but is
tainment devices. In such areas, it may also be
frequently referred to in codes as the grounded conduc-
intended that patients be connected to elec-
tor. The other conductor, carrying power to the recepta-
tromedical devices (e.g., heating pads, electrocar-
cles, is called the hot conductor and is usually colored
diographs, drainage pumps, monitors, otoscopes,
black. Its voltage is approximately 120 V with respect to
ophthalmoscopes, peripheral intravenous lines).
the neutral conductor or ground reference.
Critical care areas are those special care units,
The third conductor in a three-wire power cord for
intensive care units, coronary care units, angiog-
conventional equipment does not carry normal load
raphy laboratories, cardiac catheterization labo-
current. At the equipment end of the cord, it connects
ratories, delivery rooms, operating rooms, and
to the chassis and exposed metal. When the plug is
similar areas in which patients are intended to be
inserted into a properly installed three-slot grounding
subjected to invasive procedures and connected to
receptacle, the third wire is connected to ground. This
line-operated electromedical devices.
grounding wire (not to be confused with grounded
Wet locations are patient care areas that are connector), usually green, is intended to carry nor-
normally subject to wet conditions while patients mally small leakage currents, as well as large fault
are present; this includes standing fluids on the currents resulting from shorts, from the hot conductor
floor or drenching of the work area, either of to the chassis. By connecting the equipment chassis to
which condition is intimate to the patient or staff. ground, this third wire protects people touching the
Routine housekeeping procedures and incidental chassis against electric shocks. Because load current
spillage of liquids do not define a wet location. does not normally flow through it, the green wire will
(Note: Areas that may typically be designated as be closer to ground potential than the neutral wire.
wet locations include hydrotherapy areas, dialy-
The grounding slot of the receptacle is attached to the
sis units, and certain wet laboratories. Operating
yoke with which the receptacle mounts in its box, and the
rooms, even though there may be significant
box is grounded through the metal conduit through
amounts of spilled fluids, are generally not con-
which the wires run. The receptacle ground terminal can
sidered wet areas.)
also be grounded by a separate grounding conductor
connected to the grounding point in the electrical distri-
Ensure that the grounding pin on the plug cap is the bution system panel board. The separate wire, or pulled
first to engage and the last to disengage in the ground, is a more reliable means of grounding, because
receptacle at all angles of entry and withdrawal the conduit is made of a material that can corrode and
has mechanical joints that can loosen. Current electrical
Provide strain relief for the power cord where it codes for new construction require that the ground ter-
enters the plug cap minals of all receptacles in patient care areas be con-
nected to ground by a separate insulated copper
Several plug and receptacle configurations are conductor. An exception to the code allows existing con-
available for specific applications. The two-pole, struction that does not use a separate grounding conduc-
three-wire, parallel-blade grounding-type receptacle tor to continue in use provided it meets the specified
is most familiar because of its widespread use. This grounding performance requirements.
configuration can be made to satisfy the require-
ments for a reliable plug-receptacle combination. The common three-slot, parallel-blade, grounding-
Other receptacle configurations, which generally type receptacle is intended for branch circuits rated at
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Electrical Receptacles
15 A, which is adequate for most 120 V devices. Re- Special precautions
ceptacles and plugs of a slightly different configuration
are available for branch circuits and equipment that Testing in occupied areas must not pose a hazard to
require between 15 and 20 A. The 20 A receptacle is patients. Devices used to determine ground quality or
designed to accept both the 20 A and 15 A plugs, but grounding impedance apply power to the grounding
the 20 A plug cannot be used in a 15 A receptacle. circuit. To minimize risks to the patient and equip-
ment in the testing area and potentially in other areas
The conventional three-prong plug and three-slot served by the same circuit, the output of the testing
receptacle are polarized so that they will mate in only devices should be limited to 500 mV RMS (1.4 V peak
one direction. Assuming that the receptacle and to peak) or 1.4 VDC even under open-circuit conditions.
equipment are wired correctly, the polarization en-
sures that the hot, neutral, and ground wires in the Receptacles should be tested with all equipment
power cord connect to their counterparts in the recep- unplugged. Consult clinical personnel before discon-
tacle. The conventional two-slot receptacle provides necting patients from devices or unplugging equip-
for polarization by the difference in the size of the ment and before turning off a branch circuit breaker
receptacle slots (the hot wire slot is smaller than the to correct defective receptacles. Do not attempt to
neutral slot). Thus, equipment requiring polarization unplug life support and critical monitoring devices
is equipped with plugs that have blades of different that are in use; return when the bed is unoccupied or
sizes. occupied by a patient better able to withstand the
transfer of devices to alternate power sources.
Citations from Health Devices Procedure
Ground fault circuit interrupters [Evaluation], 1973 Before beginning the receptacle inspections, deter-
Mar; 2:112-5. mine the extent to which inspecting personnel should
Hospital Grade duplex receptacles [Evaluation], 1978 correct deficiencies on the spot. Certainly, such minor
Nov; 8:3-18. defects as a loose screw on the cover plate should be
corrected. Inspecting personnel might also carry a sup-
OR renovations and the use of isolated power and ply of new receptacles and cover plates and replace and
explosion-proof plugs [User Experience NetworkTM], retest defective receptacles as identified. Alternatively,
1992 Sep; 21:334. inspectors can identify defective receptacles with “Defec-
tive — Do Not Use” tags; qualified personnel can follow
Electrical outlets in anesthesizing locations, 1993 Aug- up by correcting defective receptacles and retesting.
Sep; 22:420.
Because the Universal Inspection Form does not
Test apparatus and supplies apply, use the special Electrical Receptacles Form 437
included with this procedure.
Three-lamp receptacle wiring polarity tester
AC voltmeter, range 100 to 140 V Identify the area to be tested; this may be a room,
special care area, corridor, or an area with many recep-
Low-resistance ohmmeter, resolution to 0.01 Ω in tacles (e.g., coronary care unit, isolated power system). If
the 0 to 0.2 Ω range failures occur, note these on the form and identify the
Leakage current meter or voltmeter capable of location of the receptacle. Using a standard method for
measuring 20 to 500 MV numbering the receptacles in an area will prove helpful.
One way is to enter the area and start to the left of the
Receptacle tension tester door, proceeding clockwise around the area. If a defective
Leads and adapters to connect receptacle and other receptacle is not repaired or replaced at the time of
ground points inspection, put a “Defective — Do Not Use” tag on it.
GFCI tester (electrical safety analyzer or isolated Exception reporting can save time when using the
power tester) form. If no defects are encountered in an area or room,
Defective receptacle tags indicate the area, room, and outlet on the form, write OK
in the “Status” box and check off the “Exception Report-
Test equipment that combines the function of the ing Used” box. You need only record measurements that
above test devices or that automates the testing de- fall outside the criteria for any test in the appropriate box
scribed in this procedure is available and may be on the form. If you are planning to adjust the inspection
substituted. intervals, record the total number of outlets inspected
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
(use the margin) so that the percentage of defective Line voltage
receptacles can be determined.
The following line voltage tests are not required by
Inspect every receptacle in the area with all equip- NFPA 99. We have included them as optional tests.
ment unplugged from the receptacle under test. Cau- These tests should be performed following new con-
tion: Consult clinical personnel before unplugging any struction, renovations, or major repairs to the electri-
equipment. cal distribution system to ensure that voltage taps are
set correctly on distribution transformers. Repeating
If deficiencies are found, identify the defective outlet the tests after typical loads are applied or in existing
on the form and indicate the need for corrective action facilities may indicate poor wiring or inadequate sys-
in the “Comments” column. If the space provided on tem capacity. The tests may also be helpful in diag-
the form is inadequate, write “See note” in the block nosing suspected problems and indicating whether a
and use the back of the form. Be sure to include the more extensive investigation of the electrical distribu-
receptacle number on all such notes. If more than one tion system is necessary.
form is needed for an area, number each sheet, and
attach them together. Use an AC voltmeter to measure the hot-to-neutral
voltages at representative receptacles in an area or in
To save time, you may want to perform all of the the branch circuit panel board. The hot-to-neutral
tests, except Ground Potentials and Grounding Resis- voltage should normally be within the 115 to 125 V
tance, on each individual receptacle in a room or area, range. It should not fall below 100 V with heavy loads
then proceed with the remaining tests on all receptacles. on the circuit or rise above 130 V during no-load
conditions. A significant difference in line voltages to
receptacles taken under typical load conditions indi-
Mechanical condition cates overloaded circuits or faulty wiring and requires
further investigation. An optional means of testing for
Visually inspect the receptacle and cover plate for adequate wiring is to measure the line voltage with
physical damage and security of physical mounting of the and without a load connected to the other half of the
receptacle and outlet box. Replace the receptacle if its duplex receptacle being tested.
face is badly chipped or broken. Replace the cover plate
if it is cracked. Correct any defects in physical mounting. Measure the AC voltage between the neutral and
ground connections. A reading of above 4 V indicates
If any sensation of heat is noted when touching the possible miswiring of the neutral and/or ground sys-
surface of the receptacle or when unplugging con- tems or excessive resistance in the wiring.
nected equipment, investigate further. Heating within
the receptacle can be caused by several deficiencies, Ground potentials
including high resistance at the receptacle contact due The purpose of this test is to determine whether
to wear, damage, or loose wiring, especially if improper voltage differences exist between points that should be
techniques have been used with aluminum wiring. at ground potential. These voltage differences could
Rarely will a receptacle develop internal leakage. Be- be caused by high ground-to-ground resistances and/or
fore condemning the receptacle, rule out any defect in heavy currents flowing through the ground system.
the equipment that causes it to draw excessive current
or poor connections in the plug cap. For new construction, NFPA 99 requires that the
voltage limit between a reference point and grounding
contact of each receptacle in the patient vicinity not
Wiring polarity exceed 20 mV. In existing construction, the voltage
should not exceed 500 mV in general care areas and 40
Check each receptacle for wiring errors with a three- mV in critical care areas. However, voltages in modern
lamp polarity tester. This tester will indicate loss from construction are usually less than 10 mV; voltages
hot, neutral, or ground wires and whether hot and exceeding 20 mV may indicate a deteriorating condi-
neutral or hot and ground wires have been inter- tion and should be investigated. It should be under-
changed. It does not detect neutral/ground reversal stood that these limits are not precise, and differences
and does not verify that grounding is adequate to carry of less than 20% should be considered insignificant.
fault currents. Correct any wiring errors. Look for
flickering of the tester’s lights as it is inserted, jiggled Measure ground potentials with a voltmeter or leak-
moderately in place, and withdrawn. Such flickering age current meter. Leakage current readings can be
may indicate poor contacts and should be investigated. converted to millivolts if the leakage current meter’s
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Electrical Receptacles
impedance is known. (Most leakage current meters carry sufficient current to quickly blow the branch fuse
have a 1,000 Ω impedance at line frequency; the read- or circuit breaker. More recently, the grounding sys-
ing in µA is then numerically equivalent to the voltage tem has been called upon to drain leakage current and
in mV.) Connect one lead of the meter to a reference fault currents not large enough to blow a fuse or
ground point that is known to be securely grounded. It breaker and to protect hospital patients against mi-
is usually most convenient to use the ground contact croshock under these conditions. In this application,
of one receptacle, but a ground plug or structural the grounding system resistance must be low enough
member can also be used. Do not use the cover plate to prevent dangerous voltages when anticipated leak-
screw because this may not be adequately grounded. age or fault currents flow through it.
Connect the other lead to the ground contact of each
receptacle in turn. To save time, measure ground To avoid risk to patients in the area in which testing
potentials on an entire room or area at one time, rather is being conducted and in areas distant from the test-
than while performing other tests on each receptacle. ing site, any device used to determine ground quality
or grounding resistance on occupied patient care areas
Ground potentials will not be constant with time but must limit the output to 500 mV RMS (1.4 V peak to
will depend on what equipment is connected and oper- peak) or 1.4 VDC. Several test devices are available
ating at the time of measurement. A high ground using different measurement methodologies. Any of
potential measurement at a receptacle grounding con- these special-purpose devices or an ohmmeter with
tact may indicate that the ground and the neutral resolution to 0.01 Ω may be used. For periodic meas-
conductor in the receptacle wiring are reversed. The urement in existing construction, the measurement
three-lamp testers will not detect such reversal (which, current can be either AC or DC.
in fact, will often be undetected during ground poten-
tial measurements, since the outlet ground contact will Select a ground reference point (such as that used
usually be grounded through the conduit). for the ground potential test), and measure the resis-
tance between each receptacle ground contact and the
Neutral-to-ground resistance reference. The resistance should not exceed 0.2 Ω and,
in new construction, should not exceed 0.1 Ω.
The safety provided by a good ground system can be
compromised if the neutral wires of the receptacles are Action required as a result of ground potential and
not properly connected to the grounding system at an grounding resistance failures may not be restricted to
appropriate location. For example, if a device plugged replacement of a receptacle but may involve the entire
into a receptacle with high neutral-to-ground resis- area’s wiring and grounding. The need for corrective
tance develops a hot-wire-to-chassis short circuit, then action should be discussed with the plant engineer or
120 V would exist as a shock hazard to anyone touching other responsible person.
that chassis. If the neutral-to-ground resistance were
When performing ground potential and resistance
low, then the heavy currents flowing from the
tests on new construction and renovations, note the
grounded chassis back to the neutral wire would trip
appropriate criteria for new construction included in
the receptacle’s circuit breaker. ECRI suggests a mini-
those test methods. NFPA 99 requires the use of an
mum of 1.0 Ω between the neutral and ground contact
AC measuring source for postconstruction impedance
of each receptacle.
measurement (but allows the use of AC or DC devices
on existing construction).
Grounding resistance
The three-lamp testers used to check receptacle Contact tension
wiring as part of the basic inspection will indicate the
complete lack of ground. However, a ground whose Contact tension — the force with which the spring
resistance is as high as several thousand ohms may be contacts of the receptacle grip the blades of the plug —
considered acceptable by these testers. The purpose of affects the performance of the plug/receptacle combi-
the grounding resistance test is to determine whether nation both electrically and mechanically. If contact
the grounding circuit resistance is low enough to serve tension is insufficient, reliable, low-resistance electri-
its intended function. cal connections cannot be assured. High resistance in
the hot and neutral connections can cause internal
Originally, the ground contact in a receptacle was heating of the receptacle. Plugs with bent blades may
designed to prevent the chassis of connected equip- not make electrical contact at all. This will be easily
ment from becoming energized in the event of a line- recognized with the hot and neutral blades, since the
to-chassis fault. In this application, the ground must equipment will not function. However, loss of contact
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
on the ground will not be obvious and will compromise
the safety of the equipment. Contact Tension Testers
In addition, the contact tension must be sufficient
to prevent the plug from inadvertently coming out of Contact tension testers are available in many
the receptacle. On the other hand, contact tension configurations and brands. Inaccurate probe
should not be so great that the plug cannot be easily sizes and surface finishes, measurement inaccu-
inserted or withdrawn. Also, in the event that some- racies, and poor repeatability can cause errone-
one trips over a line cord, the plug should withdraw ous results. Also, many testers are not rugged
from the outlet, rather than the equipment being enough to survive transport in a tool box.
pulled down or the line cord severing.
We offer the following suggestions for pur-
It has been shown that good electrical contact re- chase and use of these devices:
quires a lower gripping force than is needed to grasp
the plug firmly. Thus, a mechanical test of tension is Check for an appropriate test range of up to at
sufficient. least 8 oz. Make sure that the tester has a
specified accuracy or is accurate to within 10%.
Measure contact tension on each receptacle while
withdrawing the tester straight and smoothly from the Ask the manufacturer about probe sizes and
outlet. Retention force on the ground prong must be 4 finishes. They should be made of tool steel or a
oz or more. We recommend measuring the retention metal of equivalent hardness. Though directed
force on the hot and neutral prongs, although this is at manufacturers, UL and ANSI values may
not required. A retention force of 4 oz is also adequate serve as guidelines for hospitals:
for the hot and neutral prongs, and forces of 2 to 4 oz
— Ground probe — cylindrical, 0.4674 to
are satisfactory if the plug brand in use tends to
0.4826 cm (0.184 to 0.190 in) diameter, 8 µ
stabilize at this value and does not continue to deterio-
in finish (UL).
rate. (See the Contact Tension Testers box.)
— Power probe — 0.1397 to 0.1651 cm (0.055
GFCIs to 0.065 in) thick (ANSI).
A GFCI is a device designed to interrupt the electri-
cal circuit to the load when a fault current to ground Before each receptacle inspection, calibrate
exceeds some predetermined value that is less than the tester to ensure accuracy. Suspend a
that required to operate the overcurrent protective known weight from the tester, check its scale
device (fuse or circuit breaker) of the supply circuit. reading, and adjust if necessary.
The device is usually installed as part of the electrical
When using the tester, be sure the probes are
wiring supplying power to a receptacle. In many cases,
clean and dry. Inadvertent lubrication can sig-
it is an integral component of the power receptacle.
nificantly affect readings. Carry alcohol wipes
The GFCI continuously senses the difference in and clean the probes periodically.
current flow between the hot and neutral wire of the
receptacle circuit. Normally, this difference is quite
small. However, under fault conditions, current re- as an additional test that applies only to receptacles
turns to the source by a path other than the neutral protected by a GFCI.
wire, thus causing the difference to increase. When
NFPA specifies that a device or component that
the GFCI senses that this difference is greater than
causes 6 mA of current to flow to ground shall be
some critical value (usually 6 mA), it interrupts the
momentarily connected between the energized conduc-
circuit to the receptacle.
tor of the power distribution circuit being protected
GFCIs are used for added protection against and ground to verify that the GFCI does indeed inter-
macroshock hazards in areas where the risk of these rupt the power. Many GFCIs have a built-in test circuit
hazards is increased due to environmental conditions, and reset button. We believe this is an adequate test
such as the presence of water. The use of GFCIs is an for routine testing. If such a circuit is not built into the
acceptable method of reducing macroshock hazards in receptacle or for a more accurate validation, many
areas designated as wet locations. NFPA 99 specifies electrical safety analyzers and isolated power test de-
that GFCIs used in wet locations be tested at least vices have a built-in test for GFCIs, and simple GFCI
every 12 months. The GFCI test procedure is included test devices are available commercially.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 410-0595
Electrocardiographs
Used For:
Electrocardiographs, Interpretive [16-231]
Electrocardiographs, Multichannel [11-411]
Electrocardiographs, Single-Channel [11-413]
Also Called: EKG units, ECG units, EKG machines
Commonly Used In: Electrocardiography departments, emergency departments, and most patient care
areas
Scope: Applies to single-channel and multichannel electrocardiographs typically used for recording an
electrocardiogram on paper; may also be adapted for some systems that digitally store data and later provide
hard-copy tracings; not suitable for verifying performance of automated diagnostic functions; does not apply
to strip-chart recorders or direct writers, which should be inspected with the ECG monitor or the
defibrillator/monitor they are used in conjunction with (use ECG Monitors Procedure/Checklist 409 and
Defibrillator/Monitors Procedure/Checklist 408, respectively)
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview the various lead signals provides a more specific and
accurate diagnosis than would be possible with a sin-
An electrocardiograph detects the electrical activity of gle-lead recording.
the heart and produces a graphic record, an electrocar-
diogram (ECG), of voltage versus time. Each portion of Several standards and guidelines include perform-
the ECG is directly related to an electrical cardiac ance criteria to ensure that recording errors do not
event, and variations or abnormalities seen in the ECG interfere with accurate interpretation of the ECG.
can often be traced to a particular site in the heart. While verification that an electrocardiograph meets
Each ECG trace, which is derived from the electrical these criteria is an important part of a prepurchase
activity detected by two or more electrodes placed at evaluation program and should be included as part of
certain points on the patient’s skin surface, is called a acceptance testing, experience indicates that most of
lead. A full-lead ECG records 12 leads derived from 10 these characteristics do not change on modern electro-
electrode locations. cardiographs unless there is a major (and usually
obvious) equipment failure. Therefore, the inspection
By using a high-fidelity recording of multiple leads, procedure has been designed to reduce the amount of
it is possible to accurately examine and quantify testing required.
rhythm and waveform morphology. Voltage levels and
timing between events are measured with calipers or Portable and mobile electrocardiographs deserve
automatically by the electrocardiograph. Comparing special attention; rough handling may change circuit
009028 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
410-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
characteristics and adversely affect recording or Some older electrocardiographs may fail to meet
safety. Mishandling frequently damages the delicate current criteria for performance and safety. While
writing stylus, galvanometer, chart drive or paper units that show deteriorating performance or safety
feed, and power cords and plugs. should be repaired or replaced, those that meet their
original design specifications may still be suitable for
Citations from Health Devices use. When evaluating these units, take into account
clinical needs, realistic levels of safety, and funding
Single-channel electrocardiographs [Evaluation],
priorities. Because this Procedure/Checklist covers
1973-74 Dec-Jan; 3:31-56.
electrocardiographs used in their conventional appli-
Three-channel electrocardiographs [Evaluation], 1984 cation and not as components of larger systems, auxil-
Aug; 13:235. iary inputs or outputs of the writer are not tested here.
If these are used, test them for performance charac-
Defibrillating patients connected to electrocardio- teristics that pertain to the specific application. En-
graphs, 1984 Aug; 13:254. courage ECG technicians to check their instruments
Signal-averaging ECGs: An update, 1990 Sep; 19:328-30. at the start of each shift and to ensure that the units
are clean when returned.
12-lead multichannel interpretive electrocardiographs
[Evaluation], 1991 Oct; 20:367-408. 1. Qualitative tests
Test apparatus and supplies 1.1 Chassis/Housing. Examine the exterior of the
ECG simulator with calibrated output amplitudes unit for cleanliness and general physical condi-
and rates tion. Be sure that plastic housings are intact,
that necessary assembly hardware is present
Ground resistance ohmmeter
and tight, and that there are no signs of spilled
Leakage current meter or electrical safety analyzer liquids or other serious abuse.
Contact cleaner and lubricant
1.2 Mount. If the device is mounted on a stand or
Counter (optional) cart, examine the condition of the mount. If it is
attached to a wall or rests on a shelf, check the
The following equipment is necessary during accep-
security of this attachment.
tance testing only:
Function generator 1.3 Casters/Brakes. If the device moves on casters,
Attenuator check their condition. Look for accumulations of
lint and thread around the casters, and be sure
Oscilloscope that they turn and swivel, as appropriate. Check
Transparent metric scale the operation of brakes and swivel locks, if the
unit is so equipped.
Isolation test supply (included in some electrical
safety analyzers) 1.4 AC Plug. Examine the AC power plug for dam-
age. Attempt to wiggle the blades to determine
Special precautions that they are secure. Shake the plug and listen
Testing input isolation requires the use of a line- for rattles that could indicate loose screws. If
voltage source. Although this source should include a any damage is suspected, open the plug and
current-limiting resistor, use caution to avoid contact inspect it.
with any portions of the energized circuit.
1.5 Line Cord. Inspect the cord for signs of damage.
If damaged, replace the entire cord or, if the
Procedure damage is near one end, cut out the defective
Before beginning an inspection, carefully read this portion. Be sure to wire a new power cord or plug
procedure and the manufacturer’s instruction and serv- with the same polarity as the old one. Also check
ice manuals; be sure that you understand how to oper- line cords of battery chargers, if applicable.
ate the equipment and the significance of each control
and indicator. Also determine whether any special in- 1.6 Strain Reliefs. Examine the strain reliefs at
spection or preventive maintenance procedures or fre- both ends of the line cord. Be sure that they hold
quencies are recommended by the manufacturer. the cord securely.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Electrocardiographs
1.7 Circuit Breaker/Fuse. If the device has a battery-operated power-loss alarms, if so
switch-type circuit breaker, check that it moves equipped.
freely. If the device is protected by an external
fuse, check its value and type against that Perform the inspection with the unit on bat-
marked on the chassis, and ensure that a spare tery power or operate the unit on battery power
is provided. for several minutes to check that the battery is
charged and can hold a charge. Check battery
1.9 Cables. Inspect the cables and leads for their capacity by activating the battery test function
strain reliefs and general condition. Examine or measuring the battery-powered operating
cables carefully to detect breaks in the insulation time. When it is necessary to replace a battery,
and to ensure that they are gripped securely in label it with the date.
the connectors of each end to prevent rotation or
other strain. Check the condition of the battery charger,
and to the extent possible, confirm that it does,
Connect the unit to an ECG simulator, and in fact, charge the battery.
verify that an adequate trace is received at each
patient lead selection. (Checking all leads in Some batteries require periodic deep dis-
some units will require either a 12-lead simula- charges and recharging to maintain maximum
tor or connection and disconnection of every battery capacity. If this is recommended by the
lead.) Flex the patient cable near each end to manufacturer, verify that it is being performed
verify that there are no intermittent faults. on schedule.
1.10 Fittings/Connectors. Examine all cable connec- 1.18 Indicators/Displays. During the course of the
tors for general condition. Electrical contact inspection, confirm the operation of all lights,
pins or surfaces should be straight and clean. indicators, and visual displays on the unit and
Leads and electrodes should be firmly gripped in charger, if so equipped. Be sure that all seg-
their appropriate connectors. ments of a digital display function.
1.11 Electrodes. Confirm that an adequate supply of 1.19 1 mV Step Response. Depress and hold the 1 mV
ECG electrodes is available, and check their calibration button (or apply an external 1 mV
physical condition and that they are within their pulse) for about 3 sec. The trace should exhibit a
expiration dates. sharp, square-cornered leading edge that is nei-
ther rounded nor spiked. (Up to 10% spike or
1.13 Controls/Switches. Before moving any controls, overshoot is acceptable but will usually not be
check their positions. If any appear inordinate observed in a unit that is functioning optimally;
(e.g., a filter switch in the monitor mode rather see Figure 1.) After 2 sec (50 mm of paper at a
than the diagnostic mode), consider the possibil- speed of 25 mm/sec), the pulse should have de-
ity of inappropriate clinical use or of incipient
device failure. Record the settings of those con-
trols that should be returned to their original
positions following the inspection.
Examine all controls and switches for physical
condition, secure mounting, and correct motion.
Check that control knobs have not slipped on
their shafts. Where a control should operate
against fixed-limit stops, check for proper align-
ment, as well as positive stopping. Check mem-
brane switches for membrane damage (e.g., from
fingernails, pens). During the course of the in-
spection, be sure to check that each control and
Figure 1. The calibration pulse or step response leading
switch performs its proper function.
edge should have square corners (left). Slight rounding
(middle) or small overshoot is acceptable. Excessive
1.17 Battery/Charger. Inspect the physical condi-
rounding or overshoot (right) indicates the need for
tion of batteries and battery connectors, if read- adjustment.
ily accessible. Check operation of
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
need to be set near either extreme to obtain a
satisfactory setting.
All portions of a simulated ECG waveform
should be clearly visible, including the P wave
and QRS.
There should be no 60 Hz noise when the lead
selector switch is set to the lead 0 or standard
position and the chart motor is activated.
1.25 Paper Transport. Verify that the paper moves
smoothly and without hesitation at all paper
speeds. Problems might be caused by the trans-
port mechanism or by a roll of paper that is
wound too tightly. The paper should not drift
sideways in the transport mechanism. If a for-
matted output is used (i.e., unit prints a single
formatted sheet for each electrocardiogram),
verify that all alphanumerics and tracings ap-
Figure 2. Sag time is measured to the half-amplitude
pear in the correct location and that the paper
point. The upper trace indicates a low-frequency re-
sponse of about 0.05 Hz. The lower trace indicates a starts and stops at the correct points.
low-frequency response of between 0.07 and 0.09 Hz.
2. Quantitative tests
2.1 Grounding Resistance. Using an ohmmeter,
cayed to no more than half its original amplitude
electrical safety analyzer, or multimeter with
(see Figure 2 on page 4).
good resolution of fractional ohms, measure and
1.22 Labeling. Check that all necessary placards, la- record the resistance between the grounding pin
bels, and instruction cards are present and leg- of the power cord and exposed (unpainted and
ible. not anodized) metal on the chassis. We recom-
mend a maximum of 0.5 Ω.
1.23 Accessories. Verify that an adequate supply of 2.2 Chassis Leakage Current. Measure chassis
electrodes and paper and a fuse are stored with leakage current to ground with the grounding
the device or in the nursing unit for those elec- conductor of plug-connected equipment tempo-
trocardiographs that remain in a fixed location. rarily opened. Operate the device in all normal
A spare patient cable and stylus (or pen) may be modes, including on, standby, and off, and record
kept with units on crash carts. the maximum leakage current. Chassis leakage
1.24 Trace Quality. Observe the tracing with the unit current to ground should not exceed 300 µA.
in the standard lead select position (no input) 2.3 Calibration. This test determines the accuracy
and in lead I with a simulated ECG signal ap- of both the sensitivity control and the internal 1
plied. Verify compliance with the following cri- mV calibration signal and requires the use of an
teria: external source of known amplitude (e.g., cali-
The baseline should have constant thickness; brated ECG simulator). If this calibration source
it should be horizontal and not drift vertically. is battery powered, check its output with a preci-
sion voltmeter or similar instrument to confirm
It should be possible to move the baseline from
the lower to the upper border of the chart that the output is not affected by changing bat-
paper with the vertical position control, except tery voltage. An ECG simulator can be used,
even if its output is not precisely 1 or 2 mV,
on those units where mechanical stops pre-
vent such travel. provided its amplitude is accurately known and
appropriate corrections are made in interpreting
The baseline should remain within 1 mm of its the results.
initial position upon pushing the reset control.
With sensitivity at 20 mm/mV, record a 1 mV
If so equipped, the operator-adjustable stylus pulse from the external reference generator and
heat control should function and should not one from the internal 1 mV calibration signal of
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Electrocardiographs
the writer. For an externally generated pulse of 4. Acceptance tests
exactly 1 mV, the tracing should be between 19
and 21 mm. Deviation greater than this can Conduct major inspection tests for this procedure
often be corrected with the variable gain control and the appropriate tests in the General Devices Pro-
(a screwdriver adjustment in many units). If the cedure/Checklist 438. Electrocardiographs should
internally generated pulse and a 1 mV external meet the requirements for isolated input devices for
pulse produce tracings of heights that differ by ECG lead-to-ground, interlead, and input isolation
more than 0.5 mm, the internal calibrator is not tests. In addition, perform the following tests.
within the recommended 5% accuracy.
4.1 Frequency Response. Use the test setup shown
Next, record 1 mV pulses, either from the in Figure 3. Set the function generator and at-
internal calibrator or the reference generator, at tenuator for a sinusoidal output of 2 Hz with a
sensitivity settings of 2.5, 5, 10, and 20 mm/mV. peak-to-peak amplitude of 1 mV. Set the electro-
At each setting, the trace should double in height cardiograph gain to 10 mm/mV to obtain a peak-
(within 5%). Because of the difficulty in resolving to-peak deflection of 1 cm. (The deflection
small errors, investigate any deviation of more amplitude is not critical. If your signal gener-
than 0.5 mm. ator output is not easily adjusted, set the output
for any convenient peak-to-peak display and note
2.6 Linearity. Apply a calibrated 2 mV input to the the height.) Measure between the extreme top
writer. Record the deflection at 10 mm/mV. It and bottom of the trace. Increase the output
should be twice the deflection (within 5%) ob- frequency from the sinusoidal generator until the
served for a 1 mV signal. display drops to 0.7 cm peak-to-peak, or 0.7 times
the 2 Hz deflection. (The waveform may be
2.7 Paper Speed. Use an ECG simulator set to 60 slightly distorted.) Record this frequency as the
bpm or a signal or pulse generator set to 1 Hz upper 3 dB point. When changing the output
that has been set or calibrated with a counter. If frequency of the function generator, measure the
the interval between pulses is not within 10 msec output amplitude peak-to-peak with the oscillo-
at a pulse interval of 1,000 msec, an appropriate scope (DC response) to ensure that a constant-
correction should be made in calculating paper amplitude sinusoid, 1 mV peak-to-peak, is
speed. The speed should be accurate to within delivered to the electrocardiograph throughout
2%. At a chart speed of 25 mm/sec and a pulse the bandwidth.
interval of 1,000 msec (60 bpm on an ECG simu-
lator), the distance between the first and last of The low-frequency response point can be deter-
five successive peaks should be 100 ±2 mm; at a mined in a similar way by decreasing the fre-
chart speed of 50 mm/sec, the distance between quency from 2 Hz until the display again drops to
the first and last of five successive peaks should 0.7 cm peak-to-peak, or 0.7 times the 2 Hz deflec-
be 200 ±4 mm. tion. However, it is much simpler to determine the
low-frequency response point using the step re-
sponse test (see Item 1.19), Figure 2, and the
3. Preventive maintenance
3.1 Clean the exterior (including front panel con-
trols), all rollers, paper guides, and knife edges,
if needed.
3.2 Lubricate the recorder mechanism and paper
drive per the manufacturer’s specifications.
3.3 Calibrate damping and stylus, if required.
3.4 Replace filters and batteries, if required. Some
units have air filters that accompany the cooling
fan. Check and replace these filters, if needed.
If any of the test procedures indicate a weak or
defective battery, even after charging for 12 or Figure 3. Signal input test setup.
more hours, replace the battery.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
Relationship Between Sag and Low-Frequency LA simultaneously, there should be no output
Response from the differential amplifier because the volt-
age difference between the two inputs is zero.
Distance to Lower 3 dB
The extent to which a differential amplifier pro-
Half Amplitude Frequency
duces no output when the same signal is applied
10 mm 0.27 Hz
20 0.13 to both inputs is called its common mode rejec-
30 0.092 tion ratio.
40 0.069
50 0.055 Common mode rejection is needed because of
55 0.050
60 0.046 the presence of stray signals common to all input
80 0.034 leads primarily at power-line frequency (60 Hz).
While these signals are too minute to be hazard-
ous, they can interfere with the ECG recording
Relationship Between Sag and Low-Frequency
on a unit with a low CMRR at 60 Hz.
Response table on page 6. While the technique
may not accurately predict the low-frequency The common mode rejection ratio is defined as:
response of all units, it does provide an equally
Differential mode deflection factor, or DMD (mm ⁄ mV)
(if not more) clinically relevant response test. CMMR =
Common mode deflection factor, or CMD (mm ⁄ mV)
Some units have selectable frequency re- A deflection factor is the change in trace posi-
sponse modes. In the Filter In mode, low- and tion corresponding to a given input voltage. Use
high-frequency components of the electrocardio- an unbalanced CMRR measurement that in-
gram are attenuated. This mode can be used to cludes a 5,000 Ω resistor in series with one of
reduce baseline wander and high-frequency the input leads. This simulates the unequal im-
noise, but because small distortions of the ECG pedances that usually exist in the electrode/skin
can occur, it should not be used when recording interfaces.
diagnostic ECGs. The diagnostic response mode
provides an expanded bandwidth, as recom- Since most common-mode voltage in the hos-
mended by the American Heart Association. pital is at 60 Hz, it is most significant to measure
This should produce a display that reproduces the CMRR at or near that frequency. (A fre-
more of the low- and high-frequency qualities of quency of 55 Hz is often used to minimize inter-
the electrocardiogram than the Filter In (or moni- ference from line-power frequency noise.) Using
tor) mode. The electrocardiograph should nor- the test setup shown in Figure 3, apply a sinusoid
mally be operated in the diagnostic mode. test signal of 1 mV peak-to-peak at about 60 Hz
to the electrocardiograph. Set the gain to 20
The manufacturer’s specification for each fre- mm/mV, measure the deflection in mm, and re-
quency response mode should be used as a refer- cord it on the inspection form as the differential
ence. The diagnostic mode bandwidth should be mode deflection factor. Since the input signal for
at least 0.67 to 100 Hz. this measurement was 1 mV, the differential
mode deflection factor expressed in mm/mV is
Some units include a notch filter to minimize 60
Hz noise. On such units, confirm the notch filter’s
operation by sweeping past 60 Hz on the signal
generator and looking for a sharp dip in the re-
sponse. If the response increases as the frequency
is increased past the notch filter frequency, then
the upper 3 dB point may be above the notch
filter frequency rather than occurring where the
filter begins to attenuate.
4.2 Common Mode Rejection Ratio (CMRR). The
electrocardiograph includes a differential ampli-
fier so that it can display the voltage difference
between two electrodes (the RA and LA in Lead
1) while using a third (RL) as a reference. If the
same, or common, voltage is applied to RA and Figure 4. Common mode rejection ratio test setup.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Electrocardiographs
numerically equal to the resultant deflection in Using the internal calibration button, gener-
mm. Do not change the gain setting or the signal ate a pulse with the baseline set at the bottom
frequency for the remainder of this test. Record margin of the chart, another with the baseline
the frequency. at the middle of the chart, and a third with the
baseline as close to the top margin of the paper
Use the test setup shown in Figure 4 for the
as possible while still allowing the pulse to
second part of this measurement. Note that
remain on the ruled chart. The height of the
there is only one connection from the output of
calibration pulse should not vary more than
the attenuator to the patient leads. The other
0.5 mm with baseline position.
output terminal is grounded. It is essential that
all instruments used in this test be connected to Display range. The monitor should be able to
a common ground to minimize noise. faithfully display signals of up to 5 mV. Using
the test setup shown in Figure 3 (signal gen-
Increase the amplitude of the sinusoid signal erator set to about 2 Hz) or an ECG simulator
(up to 10 V peak-to-peak) until some measurable with an appropriate output range, apply a
deflection is observed on the recorder. Calculate 5 mV peak-to-peak signal, and observe the
the common mode deflection factor by dividing trace using gain and position settings that
the resultant deflection (in mm) by the input keep the trace on the recording paper rulings.
signal (in mV). The CMRR may then be calcu- Note any distortion or clipping of the signal.
lated as the differential mode deflection factor
divided by the common mode deflection factor. 4.4 Crosstalk. Verify that activation of time and
event markers does not cause a deflection on the
If the unit has an ungrounded or plastic case,
ECG trace. Check for channel crosstalk on mul-
measure the CMRR with the unit resting on a tichannel electrocardiographs by attaching an
grounded metal plate. CMRR should meet the ECG simulator to one lead pair while the others
manufacturer’s specification and be at least
are shorted together. There should be no visible
10,000:1. trace deflection in any of the channel tracings
4.3 Linearity. In addition to the linearity test de- except the one with the simulated ECG.
scribed in Item 2.6, test the effect of baseline
position on linearity and linear input range. Before returning to use
Baseline position. Vary the centering or position Set all controls to their original settings, and re-
control to change baseline position, if possible. charge the battery, if needed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Procedure/Checklist 411-0595
Electrosurgical Units
Used For:
Electrosurgical Units [11-490]
Electrosurgical Units, General-Purpose [16-137]
Electrosurgical Units, Specialty [16-138]
Also Called: ESUs, electrocautery units (although this term more appropriately refers to a different type of
surgical device), Bovie (a registered trademark of MDT Diagnostic Co. to be used only when referring to that
device)
Commonly Used In: Operating rooms, outpatient surgical units
Scope: Applies to units that perform surgical functions (e.g., cutting, coagulation) by using high-frequency
electrical currents that pass through the body (units may include other functions such as insufflation); does not
apply to electrocautery units that use an electrical current to heat a tip for surgical effects
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview They also incorporate microprocessor-controlled cir-
cuitry to monitor unit performance, adjust power set-
Surgical use of high-frequency current dates back to tings, and, in some units, interrogate the quality of
the early 1900s. Tesla and Oudin coil resonators in contact of the return electrode.
conjunction with spark gaps produced high voltages at
very low currents, which were used to destroy superfi- Undamped, continuous sinusoidal currents (about
cial tissue with a spray of sparks from the active 0.2 to 3.0 MHz) cut tissue with a cutting electrode or
electrode (fulguration). No return connection was pro- loop with minimal coagulation. The intense heat ex-
vided between the patient and the electrosurgical unit. plodes and volatilizes tissue cells. This type of current
Vacuum tubes were later introduced and provided can also be used to coagulate with large surface elec-
continuous sinusoidal wave generation. Circuits could trodes or hemostats. Damped waves and current
then be designed to produce lower voltages but higher bursts coagulate, fulgurate, and desiccate with mini-
currents. However, the higher currents required a mal cutting by generating heat in a wider region of
reliable conductive path to complete the circuit, and tissue immediately surrounding the active electrode.
the dispersive electrode (also called the butt, safety, The dry, fibrous residue left by the rapid dehydration
patient, or ground plate, or return or indifferent elec- of cells blocks vessels and prevents bleeding. A combi-
trode) was introduced. nation of damped and undamped waveforms cuts and
coagulates simultaneously.
Most currently marketed units are solid-state de-
vices that permit size reduction and the generation of In electrosurgery, the heat that destroys tissue is
a variety of waveforms without the use of a spark gap. not produced by a heated wire as in electrocautery, but
094428 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
411-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
by conversion of the high-frequency electrical energy Ellman International Manufacturing Surgitron and
in the tissue. Current density and duration determine Surgitron FFPF [Hazard], 1986 Aug; 15:248.
the amount of heat generated and tissue destroyed at
and near the electric arc. Active electrodes have small ESU burns from poor return electrode site preparation
tips to increase the current density at the surgical site. [Hazard], 1987 Jan; 16:35.
Electrodes used specifically for cutting have small Electrosurgical units [Evaluation], 1987 Sep-Oct;
points or edges to concentrate the electrosurgical cur- 16:291-333.
rent; coagulation electrodes have larger surface areas.
Both characteristics can be combined into a single Return electrode monitors: Assessing your needs [Risk
electrode (a blade type) so that electrodes need not be analysis], 1987 Sep-Oct; 16:335-7.
changed during shifts between cutting and coagula-
tion. Since no tissue heating is desired elsewhere, the Controlling the risks of electrosurgery [Risk analysis],
dispersive electrode must contact a much larger area 1987 Sep-Oct; 16:337-9.
of the patient’s skin to reduce the return current den- Bovie CSV: Still accepted? 1987 Sep-Oct; 16:340-1.
sity to harmless levels.
Do ESU output characteristics affect instrument per-
Periodic inspection is not a substitute for routine formance? 1987 Sep-Oct; 16:341-2.
pre-use verification of electrosurgical unit safety fea-
tures and current use practices. Reusable active elec- Pacemakers and electrosurgery: What precautions are
trodes and accessories, such as bipolar and laparoscopic needed? 1987 Sep-Oct; 16:342.
forceps and leads, should be inspected periodically, but
they are not usually readily available with the electro- Electrosurgical units [Evaluation update], 1988 Dec;
surgical unit. Where practical, users or processing per- 17:363-5.
sonnel should routinely inspect these items.
Update: Controlling the risks of electrosurgery [Risk
analysis], 1989 Dec; 18:430-2.
Citations from Health Devices
Electrosurgical units [Evaluation], 1977 Jan-Feb; Electrosurgery checklist, 1989 Dec; 18:432.
6:59-86. (See also: 1977 Jun; 6:194.) Update: ESU return electrode contact quality monitors
Electrosurgical unit safety, 1977 Mar; 6:119-21. [Risk analysis], 1989 Dec; 18:433-6.
Fires during surgery of the head and neck area Argon beam coagulation systems [Evaluation], 1990
[Hazard], 1979 Dec; 9:50. Sep; 19:299-320.
Fires during surgery of the head and neck area Argon beam coagulation systems [Evaluation update],
[Hazard update], 1980 Jan; 9:82. 1990 Dec; 19:444-5.
Adapters and cables for electrosurgical dispersive Stryker Surgical microsurgical drills: Activation by
electrodes [Hazard], 1981 Jan; 10:74-5. ESUs [Hazard], 1991 Oct; 20:409-10.
Adapters and cables for disposable electrosurgical dis- Stryker Surgical microsurgical drills: Activation by
persive electrodes [Hazard update], 1981 Feb; ESUs [Hazard update], 1991 Nov; 20:446.
10:99.
Stryker Surgical microsurgical drills: Activation by
Using two ESUs on one patient [Consultant’s Corner], ESUs [Hazard update], 1991 Dec; 20:496-7.
1982 Sep; 11:301-2.
Birtcher 4400 electrosurgical units and 6400 argon
ESU return electrode contact quality monitors [Evalu- beam coagulation systems [Hazard], 1992 Jun-Jul;
ation], 1985 Feb; 14:115. 21:249-50.
Electrosurgical unit activation tone control [Hazard], Burns and fires from electrosurgical active electrodes
1985 Nov; 14:407. [Hazard update], 1993 Aug-Sep; 22:421-2.
Isolated incidents: Electrosurgical units [User Experi- ESU burns from poor dispersive electrode site prepa-
ence NetworkTM], 1986 May; 15:143. ration [Hazard], 1993 Aug-Sep; 22:422-3.
Hand-switched electrosurgical active electrode pencils Burns and fires from electrosurgical active electrodes
[Evaluation], 1986 Jun; 15:151. [Hazard update correction], 1993 Oct; 22:502.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Electrosurgical Units
Use of an incompatible footswitch with Aspen Excali- Never activate the unit with the active and disper-
bur, Birtcher 5000, and Valleylab Force electrosur- sive electrodes connected together (short-circuited),
gical units [Hazard], 1993 Dec; 22:593-4. since this may damage the unit.
Electrosurgical units with accessory outputs [User Ex- Procedure
perience NetworkTM], 1993 Dec; 22:601-2.
Before beginning an inspection, carefully read this
Fatal gas embolism caused by overpressurization dur- procedure and the manufacturer’s instruction and
ing laparoscopic use of argon enhanced coagulation service manuals; be sure that you understand how to
[Hazard], 1994 Jun; 23:257-9. operate the equipment, the significance of each control
and indicator, and the alarm capabilities. Also deter-
Risk of electrosurgical burns at needle electrode sites mine whether any special inspection or preventive
[Hazard], 1994 Aug-Sep; 23:373-4. maintenance procedures or frequencies are recom-
mended by the manufacturer.
Monopolar electrosurgical safety during laparoscopy
[Guidance article], 1995 Jan; 24:6-27. Use an electrosurgical unit analyzer with appropri-
ate load resistances for measuring electrosurgical unit
Misconnection of bipolar electrosurgical electrodes output. A number of methods for testing electrosurgi-
[Hazard], 1995 Jan; 24:34-5. cal output have been suggested, including the use of
light-bulb loads, sparking the active electrode to the
Test apparatus and supplies return electrode, and cutting a slice of beef placed on
the return electrode. However, none of these provide
Leakage current meter or electrical safety analyzer quantitative performance data, and some methods
Ground resistance ohmmeter may damage the electrosurgical unit.
High-resistance (20 MΩ) ohmmeter When measuring output (e.g., Items 2.3 and 2.10),
do not use excessive lead lengths or coil the leads
Connectors, adapters, active electrode and/or return because either may affect measurement accuracy.
electrode, as required; open-circuited dispersive
electrode connector may be required 1. Qualitative tests
Electrosurgical unit analyzer 1.1 Chassis/Housing. Examine the exterior of the
Oscilloscope and high-voltage probe (acceptance unit for cleanliness and general physical condi-
testing only) tion. Be sure that plastic housings are intact,
that assembly hardware is present and tight,
and that there are no signs of spilled liquids or
Special precautions other serious abuse.
Electrosurgical units deliver high voltage and high 1.2 Mount. If the device is mounted on a stand or
power that can cause serious electrical burns. Be sure cart, examine the condition of the mount. If it is
that all connections are secure and well insulated attached to a wall or rests on a shelf, check the
before performing any power output test. Do not con- security of this attachment.
tact either the active or dispersive electrode while the
unit is activated (under some circumstances, burns can 1.3 Casters/Brakes. If the device moves on casters,
occur even from contact with the dispersive electrode). check their condition. Look for accumulations of
When making connections and whenever testing is not lint and thread around the casters, and be sure
being performed, make sure the unit is off or in the that they turn and swivel, as appropriate. Check
standby mode. the operation of brakes and swivel locks, if the
unit is so equipped.
Never operate any electrosurgical unit for prolonged
periods during testing, especially at maximum control 1.4 AC Plug/Receptacles. Examine the AC power
settings. Electrosurgical units can be damaged by such plug for damage. Attempt to wiggle the blades
operation. to determine that they are secure. Shake the
plug and listen for rattles that could indicate
Hazardous high voltages are present inside elec- loose screws. If any damage is suspected, open
trosurgical units. Do not open the electrosurgical the plug and inspect it. If the device has electri-
units for inspection or adjustment unless you are cal receptacles for accessories, insert an AC plug
qualified to do so. into each, and check that it is held firmly. If
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
accessories are plugged and unplugged often, inspection. Examine all controls and switches
consider a full inspection of the receptacle. for physical condition, secure mounting, and cor-
rect motion. Where a control should operate
1.5 Line Cord. Inspect the cord for signs of damage. against fixed-limit stops, check for proper align-
If damaged, replace the entire cord, or, if the ment, as well as positive stopping. Check mem-
damage is near one end, cut out the defective brane switches for membrane damage (e.g., from
portion. Be sure to wire a new power cord or plug fingernails, pens). During the course of the in-
with the same polarity as the old one. spection, be sure to check that each control and
1.6 Strain Reliefs. Examine the strain reliefs at switch performs its proper function.
both ends of the line cord. Be sure that they hold 1.18 Indicators/Displays. During the course of the
the cord securely. inspection, confirm the operation of all lights,
indicators, meters, gauges, and visual displays
1.7 Circuit Breaker/Fuse. If the device has a
on the unit. Be sure that all segments of a digital
switch-type circuit breaker, check that it moves
display function.
freely. If the device is protected by an external
fuse, check its value and type against that 1.20 Dispersive Cable Continuity Monitor. Confirm
marked on the chassis, and ensure that a spare that this sentry triggers an audible (and on some
is provided. units, a visual) alarm if continuity of the return
cable is interrupted. The electrosurgical unit
1.9 Cables. Inspect the cables (e.g., footswitch) and
should be locked out of activation in this alarm
their strain reliefs for general condition. Exam-
mode.
ine cables carefully to detect breaks in the insu-
lation and to ensure that they are gripped To test the cable continuity monitor, turn all
securely in the connectors at each end to prevent output controls to minimum, disconnect any ac-
rotation or other strain. tive electrodes, connect a complete cable and
dispersive electrode assembly to the electrosur-
1.10 Fittings/Connectors. Examine electrical connec- gical unit, and turn the unit on but do not operate
tors for general condition. Electrical contact pins it. Suspend the dispersive electrode in the air so
or surfaces should be straight, clean, and bright. that it does not touch any metal surface or object
1.11 Dispersive Electrodes. Inspect reusable disper- that might provide a ground pathway back to the
sive electrode cables carefully for any breaks in electrosurgical unit. Do not touch the electrode.
the insulation and other obvious damage. Ex- The alarm should not sound.
amine the electrosurgical unit and return elec- A loose panel connection to the dispersive
trode connectors for signs of damage. Confirm cable often causes the return cable continuity
that their strain reliefs are secure. Check that monitor’s alarm to sound, which may annoy the
several dispersive electrodes and dispersive elec- OR staff. Wiggle the dispersive cable connection
trode cables (separate or preattached) are stored at the unit. If this cable motion sets off the
with the electrosurgical unit. (If reusable disper- alarm, suspect a weak connector, and arrange
sive electrodes are in use, replace them with for repairs.
single-use dispersive electrodes with preat-
tached adhesive. Using disposable dispersive Unplug or unscrew the cable connector from
electrodes with preattached adhesive is much the dispersive electrode. The unit should alarm
less likely to result in patient burns.) immediately and should resist activation. If this
does not occur, the return cable may be shorted
1.12 Filters. Check the condition of all filters. Clean or the alarm itself may be defective. To deter-
or replace if needed, and indicate this on Line 3.1 mine the cause, unplug the dispersive electrode
or 3.4 of the inspection form. cord from the electrosurgical unit. If the alarm
does not activate, it is defective and needs repair.
1.13 Controls/Switches. Before moving any controls,
If the alarm activates, the dispersive cable is
check their positions. If any of them appear
defective and should be replaced.
inordinate (e.g., a control set at maximum out-
put), consider the possibility of inappropriate If the dispersive electrode is permanently at-
clinical use or of incipient device failure. Record tached to the dispersive cable and the electrosur-
the settings of those controls that should be gical unit is designed to automatically disable
returned to their original positions following the the buzzer alarm when the dispersive cable is
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Electrosurgical Units
unplugged, use an open-circuited connector to Dispersive electrode grounding resistance.
test the alarm. Measure the resistance between the dispersive
electrode and the ground pin of the power cord.
1.21 Audible Signals. Operate the device to activate This measurement should indicate an open
any audible signals (e.g., activation indicator, circuit (exceeding 20 MΩ or largest reading of
dispersive cable continuity monitor). Confirm the ohmmeter) for isolated-output units or
appropriate volume, as well as the operation of grounded units equipped with a capacitor be-
a volume control. Serious injury has been asso- tween the dispersive electrode and ground; the
ciated with warning signals (e.g., activation in- latter are called ground-referenced units. A
dicator) whose volume controls had been set so value less than 20 MΩ for ground-referenced
that the signals were not audible. If volume units suggests a defective capacitor between
controls have been set too low, discuss this prob- the dispersive electrode and ground inside the
lem with users so that clinical practices can be electrosurgical unit. An initial low resistance
corrected. Units that lack audible activation in- that drifts up to a value over 20 MΩ is accept-
dicators should be removed from service. Units able; this phenomenon is due to a charging
with audible activation indicators that can be set capacitor. There should be a short circuit (ap-
to inaudible levels should also be removed from proximately 0.15 Ω) for grounded-output units
service or modified by the manufacturer so that without a capacitor. ECRI recommends that
the alarm cannot be set to an inaudible level. units with the dispersive electrode connected
1.22 Labeling. Check that all necessary placards, directly to ground be replaced with isolated-
labels, and instruction cards are present and output or ground-referenced units.
legible.
2.2 Chassis Leakage Current. While electrosurgical
1.23 Accessories. units are generally operated from isolated power
systems in the operating room, power line fre-
Footswitch. Examine the footswitch for general quency and leakage current measurements must
condition, including evidence of spilled fluids. be made with the unit connected to a grounded
Check for any tendency of the footswitch to (conventional) power supply to obtain valid read-
stick in the On position. Activate the switch ings. This is most readily accomplished by remov-
in both the Cut and Coagulation modes and ing the electrosurgical unit from the operating
flex the cable at the entry to the switch to suite to an area with grounded power distribution.
check for internal wire breaks that may cause An adapter cord will be needed if the unit is
intermittent device operation. equipped with a specialized operating room plug.
1.24 Special Protective Features. Test alternative Before measuring the leakage currents, turn
protective features according to instructions all the unit’s power controls to zero. Connect a
from the manufacturer’s literature. These in- return electrode if the unit cannot be activated
clude features intended to monitor the integrity without one. Connect one lead of the leakage
of the patient circuit (e.g., dispersive electrode current meter to ground, and position the meter
contact quality monitors), ensure absence of in- away from the electrosurgical unit. With the
advertent ground contacts (e.g., return fault other lead of the leakage current meter in the
monitors), or minimize injury from active elec- vicinity of the electrosurgical unit but not in
trode insulation failures or capacitive coupling contact, activate the unit in its various operating
(e.g., monopolar electrode shielding devices). modes, keeping the output at the minimum set-
These features can be either integral to the elec- tings. Any significant reading on the leakage
trosurgical unit or add-on devices. current meter indicates that the meter is suscep-
tible to high-frequency interference and cannot
2. Quantitative tests be used when the electrosurgical unit is acti-
vated. A 0.1-microfarad capacitor connected
2.1 Grounding Resistance. Measure and record the across the leakage current meter terminals may
resistance between the grounding pin of the reduce this interference and will not unduly af-
power cord and exposed (unpainted and not ano- fect the line frequency leakage current readings.
dized) metal on the chassis, accessory outlet,
ground pins, and footswitch. We recommend a CAUTION: Never measure 60 Hz leakage cur-
maximum of 0.5 Ω. rents from the active electrode while the unit is
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
activated. Also, when testing an isolated output ate the unit for long periods or at maximum
electrosurgical unit, do not measure currents from control settings, since this will stress the unit.
the return electrode when the unit is activated.
These measurements can expose you to high volt- 2.10 Output Current/Power. Connect the output cur-
age and can damage the leakage current meter. rent or power meter to the active and dispersive
connections on the electrosurgical unit. On units
Measure chassis leakage current to ground with a return electrode continuity monitor, use
with the grounding conductor of plug-connected a dispersive electrode or an appropriately wired
equipment temporarily opened. Measure with adapter.
the unit off, on (standby), and activated in each
Output power should be tested according to
mode (e.g., Cut 1, Cut 2) with power controls set
the manufacturer’s recommendations. If the
at minimum. Record the value for the mode that
electrosurgical analyzer in use does not have the
yields the highest leakage current. Leakage cur-
load resistance suggested by the manufacturer,
rents from the chassis should not exceed 300 µA. it can still be used, but output powers may be
2.3 Output Isolation. This test is intended for iso- different from those given in the service manual
lated output units to determine whether the (some manuals may indicate how output varies
isolation has been degraded. Do not perform this with load resistance). Record the load resistance
test on units with directly grounded dispersive of the output meter on the inspection form.
electrodes or with dispersive electrodes con- Test the unit at the manufacturer’s recom-
nected to ground through a capacitor. Consult mended output settings or at a typical clinical
the unit’s manual if you are uncertain whether setting (or at a dial setting about one-third of
it is an isolated output device. The isolation test maximum and at maximum). Using all the oper-
is normally conducted after the output power ating modes available on the electrosurgical unit,
measurement (Item 2.10). record the output current or power from the meter.
Confirm that power is delivered to secondary mo-
If the tester has an Isolation Test mode, follow
nopolar terminals. Also measure output at bipolar
the tester’s instructions. Otherwise, connect the
terminals. The output should increase smoothly
output current/power meter between the active
from zero or nearly zero to maximum. Do not
cable and a ground (e.g., the chassis of the unit).
operate the unit at high control settings for pro-
The dispersive cable and dispersive electrode of
longed periods, since this places an unrealistic and
the electrosurgical unit must not be in contact
unnecessary strain on both the electrosurgical unit
with ground. If the unit has no dispersive circuit
and the tester. It will not be possible to read
monitor, unplug the dispersive cable from the
low-current values precisely. Compare output
unit. If the unit has a dispersive sentry, suspend
power to the manufacturer’s specifications. Er-
the dispersive electrode in the air by hanging the
ratic output power in spark-gap units suggests
dispersive cable over a hook.
that spark gaps may need maintenance or adjust-
CAUTION: To avoid the possibility of burns, ment. This should be done only by qualified, expe-
do not touch the electrode. rienced personnel. Use Lines 2.11 and 2.12 of the
inspection form as needed for additional output
With the unit in the Pure Cut or Cut 1 mode, power measurements.
increase the controls gradually to one of the
moderate levels used in the output power test 3. Preventive maintenance
and record the power to ground. The extent of 3.1 Clean the exterior and interior, if needed.
output reduction, compared with the output re-
corded in Item 2.10, is an indication of the degree 3.4 Replace the filter.
of isolation.
4. Acceptance tests
P ower (W ) of isolation test (Item 2.3)
Isolation % = 1 – x 100%
Output power (W ) at the sam e setting (Item 2.10) Conduct major inspection tests for this procedure
and the appropriate tests in the General Devices Pro-
Current2 (amps) of isolation test (Item 2.3) cedure/Checklist 438.
or = 1 – x 100%
Output current2 (amps) of same setting (Item 2.10)
CAUTION: Never measure 60 Hz leakage currents
Isolation should meet the manufacturer’s from the active electrode while the unit is activated.
specifications or be ≥80%. As before, do not oper- Also, when testing an isolated output electrosurgical
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Electrosurgical Units
unit, do not measure currents from the return electrode 4.2 Output Isolation (for isolated output units only).
when the unit is activated. These measurements can In addition to the test described in Item 2.3, make
expose you to high voltage and can damage the leakage a similar power measurement from dispersive
current meter. Leakage current from the active and electrode to ground, preferably with a hand-
return electrode should not exceed 50 µA. In addition, switched active handle connected to the unit.
perform the following tests. This will ensure that excessive power is not avail-
able from the dispersive electrode. Set the unit
4.1 Waveform Analysis. If a manufacturer has pro- to Pure Cut, maximum output. Power exceeding
vided output waveform characteristics (e.g., fre- 5 W suggests a fault or design deficiency.
quency, waveform repetition or burst rate,
waveform on-off time), these may be studied and
documented by using an oscilloscope connected Before returning to use
to the appropriate jack on the output power/cur-
rent meter. This test is optional. A high-voltage Ensure that the volume of audible activation indi-
probe should be used for these measurements to cators can be clearly heard, turn off the main power
prevent damage to the oscilloscope and to view switch, rotate the power control knobs to zero, neatly
the full waveforms. coil and store all cables, and store all accessories.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Procedure/Checklist 464-0595
Frequency-Doubled Nd:YAG Surgical Lasers
Used For:
Lasers, Surgical, Nd:YAG, Frequency-Doubled [17-729]
Also Called: KTP lasers, 532 lasers, green lasers, surgical lasers, endoscopic lasers
Commonly Used In: Operating rooms, short procedure areas, endoscopy laboratories
Scope: Applies to general-purpose frequency-doubled Nd:YAG surgical lasers that include contact and/or
noncontact flexible fiberoptic delivery systems (either reusable or disposable), emit visible green light energy
at 532 nm, and can provide sufficient power output to coagulate and vaporize tissue; applies to low- and
high-power frequency-doubled Nd:YAG surgical lasers that are typically used for general surgery, gastroen-
terology, bronchopulmonary, neurosurgery, gynecology, and ENT surgery procedures; does not apply to
frequency-doubled Nd:YAG lasers used solely for ophthalmic surgery; also does not apply to other ophthalmic
lasers or to CO2 lasers, Nd:YAG lasers, argon lasers, or other surgical lasers; however, many of the tests listed
herein can be used or modified for these other lasers
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview sufficient power density to cause vaporization and/or
coagulation. The 532 nm light energy is preferentially
Frequency-doubled Nd:YAG surgical lasers are nor- absorbed by hemoglobin and is typically absorbed
mally checked before each use by the laser’s power-on within 3 mm of the tissue surface. Frequency-doubled
self-test and by user examination of the aiming beam Nd:YAG surgical laser fibers are most often used in
and the delivery system to be used. This minimizes the contact with or close to tissue to cause coagulation or
need for frequent additional periodic testing. vaporization. Moving the fiber tip away from the tissue
lowers the power density, causing less tissue to be
Manufacturers or outside service vendors often vaporized or coagulated.
maintain lasers for hospitals. The extent and fre-
quency of inspection by hospital personnel should be
General-purpose frequency-doubled Nd:YAG surgi-
coordinated with these outside services.
cal lasers direct the beam of an Nd:YAG laser through
Failure of a frequency-doubled Nd:YAG surgical a crystal that halves the 1,064 nm wavelength (i.e.,
laser can cause patient or staff injury, abrupt interrup- doubles the frequency) to 532 nm. (The Nd:YAG laser
tion of a surgical procedure, or damage to the laser uses an yttrium-aluminum-garnet [YAG] crystalline
system. These lasers must be meticulously maintained rod that is doped with neodymium [Nd].) Energy exiting
to ensure proper and safe operation. the crystal is typically directed into a flexible optical
fiber that transmits the laser energy to the tissue. The
Frequency-doubled Nd:YAG surgical lasers affect fiber may be used with additional devices (e.g., through
tissue by delivering green visible light energy at a an endoscope) and/or with a laser handpiece or a laser
230376 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
464-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
micromanipulator (used to interface the laser with the of sufficient optical density to protect the wearer’s
surgical microscope). These attachments can focus the eyes from laser energy
energy into a small spot size at a known working
Vise with padded jaws or ring stand with padded
distance and/or a specific beam direction to accomplish
clamp
special tasks. In addition, frequency-doubled Nd:YAG
lasers can emit a train of pulses or a single pulse. Pressure gauges and coolant system tee fitting
Like most lasers, frequency-doubled Nd:YAG lasers Outlet test fixture (optional)
are inefficient in converting electrical energy into laser Insulating gloves, high voltage (optional)
energy. As a result, excess heat is generated in the
laser cavity and doubling crystal, requiring a cooling Grounding strap (optional)
system. Most frequency-doubled Nd:YAG lasers use Calibrated flowmeter
water/air cooling systems that are self-contained, con-
nected to a freestanding chiller system, or connected
to a water supply and drain.
Special precautions
Inspecting and maintaining lasers is a dangerous as
With frequency-doubled Nd:YAG surgical lasers,
well as necessary process, and far greater care is
unlike those lasers that use mirror delivery systems
required than with most devices. Personnel who in-
(e.g., articulating arms on CO2 lasers), it is not neces-
spect or service lasers should receive special training
sary to periodically verify coincidence of the aiming
from the manufacturer or from a qualified alternative
and therapeutic beam or to assess the therapeutic
training source.
beam pattern (e.g., TEM00) within the beam or spot.
Since the therapeutic and aiming laser beams are Laser energy can cause serious injury, particularly
transmitted through a single optical fiber, these two when the internal interlock is overridden or in any
beams are coincident as they exit the fiber. Any beam other situation in which the energy does not diverge
pattern distortion at the fiber entrance would be elimi- significantly over long distances. Under some circum-
nated as the laser beams travel through the fiber stances, the beam may not diverge significantly, even
because of internal reflections within the fiber. Mis- a full room length or more away from the laser (and
alignment of the beam at the fiber entrance would can harm tissue or burn material even at this dis-
result in decreased power output or loss or distortion tance). Therefore, exercise great care whenever a laser
of the aiming beam. In a well-aligned system, any beam is accessible. Area security and use of personnel
significant problem with the therapeutic beam pattern protective devices and practices should be consistent
introduced by an accessory would be apparent by ex- with hospitalwide laser safety procedures and/or
amining the visible aiming beam. should be approved by the laser safety committee.
Citations from Health Devices In addition, windows should be covered with nonre-
Laser use and safety [Guidance article], 1992 Sep; flective material to prevent transmission of laser en-
21(9):306-10. ergy to other areas.
Surgical lasers [Evaluation], 1991 Jul-Aug; 20(7- Wear appropriate laser safety eyewear at all times
8):239-316. whenever the laser is in the Operating mode. WARN-
ING: Do not stare directly into the aiming system beam
Test apparatus and supplies or the therapeutic laser, even when wearing laser safety
eyewear. Avoid placing the laser beam path at eye level
Leakage current meter or electrical safety analyzer
(i.e., when kneeling, sitting, or standing).
Ground resistance ohmmeter
Do not perform these procedures when a patient is
New, unused fiber delivery system
present or clinical staff is working, and do not aim the
Black Delrin block 1⁄2″ or more thick, 1″ or more laser across a path that a person might normally use
wide, about 3″ to 4″ long; tongue depressors; or as a thoroughfare. Furthermore, at minimum, post
firebrick doors to the room with appropriate laser safety signs
Laser radiometer (power meter) stating that the laser is in use and that it is unsafe to
enter the room without authorization by the service
Laser safety signs person performing the procedure. A second person
Laser safety eyewear specifically designed for use should be present, especially during procedures of rec-
with frequency-doubled Nd:YAG surgical lasers and ognized risk, to summon help in case of an accident.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Frequency-Doubled Nd:YAG Surgical Lasers
The laser should remain in the Off position when Procedure
not in use. When in use, it should be in the
Standby/Disabled mode. Do not switch it to the Oper- Before beginning the inspection, carefully read this
ating mode until the procedure is about to begin and procedure and the manufacturer’s operator instruc-
the laser and its delivery system are properly posi- tions and service manual; be sure that you understand
tioned. If the procedure must be interrupted, discon- how to operate the equipment, the significance of each
nect the laser from line voltage, and remove the laser control and indicator, and precautions needed to en-
operation key and store it in a controlled location. sure safety and avoid equipment damage. Also, deter-
mine whether any special inspection or preventive
Do not use the laser in the presence of flammable maintenance procedures or frequencies are recom-
anesthetics or other volatile substances or materials mended by the manufacturer.
(e.g., alcohol), or in oxygen-enriched atmospheres, be-
cause of the serious risk of explosion and fire. Remove 1. Qualitative tests
from the working area or cover with flame-resistant 1.1 Chassis/Housing.
opaque material all reflective surfaces likely to be
contacted by the laser beam. Whenever possible, use a General. Verify that the key has not been left in
firebrick or other nonflammable material behind the the laser. (Remove it if it has been, and inform
target material (e.g., black Delrin) when the laser is to users of the importance of storing the key in a
be activated. Target materials will ignite when ex- controlled location.) Examine the exterior of
posed to high laser energies; use short durations when the unit for cleanliness and general physical
practical. A CO2 fire extinguisher should be readily condition. Be sure that all housings are intact
available. and properly aligned, that assembly hard-
ware is present and tight, that any retractable
Some surgical lasers use high voltages (e.g., 20 kV), parts slide easily and lock in place if so con-
which can be lethal. Capacitors may store charges long structed, that there are no signs of spilled
after the device has been disconnected from line volt- liquids or other evidence of abuse, and that
age. Consult the manufacturer’s recommended proce- there are no obvious signs of water or oil
dures for servicing high-voltage laser circuits, and leakage.
avoid contact with any portion of the high-voltage
Shutters. If manual shutters for the aiming sys-
circuit until you are certain that the charge has been
tem or the therapeutic laser are accessible,
drained. In such instances, a good ground must be
ensure that they operate smoothly and cor-
present; preferably, use a redundant ground strap if
rectly. Be sure to leave the shutter in the
you must enter the laser cabinet. When possible, dis-
proper position for normal operation.
connect the laser from line voltage before entering the
laser cabinet, and use insulated gloves for those proce- 1.2 Mounts/Holders. Check that the mounts se-
dures in which contact with a high-voltage source is curely contain any gas cylinders that may be in
possible (and the gloves are not otherwise contraindi- use. Be sure that mounts or holders intended to
cated). Ensure that equipment intended to be used to secure the fiber to the fiber support (to protect
measure, drain, or insulate high voltages carries the the fiber when in use) are present, in good work-
appropriate insulation rating (e.g., above 20 kV). ing order, and being used. Similarly, check
mounts or holders for other devices (e.g., exter-
Where possible, perform tests with the unit turned
nal power meters, footswitches).
off. Because of the presence of high voltage, perform
the Grounding Resistance test (Item 2.1) before any If the device is mounted on a stand or a cart,
other test that requires operation of the laser. examine the condition of the mount. Verify that
the mounting apparatus is secure and that all
WARNING: Do not use an anesthesia or other simi-
hardware is firmly in place.
lar bag that may have a mold-release agent (e.g., starch,
talc) on its inside surface because the agent could 1.3 Casters/Brakes. Verify that the casters roll and
contaminate the gas recirculation system of the laser swivel freely. Check the operation of brakes and
and ultimately contaminate a patient wound during a swivel locks.
subsequent procedure.
1.4 AC Plug/Receptacle. Examine the AC power plug
Report any laser accident immediately to the laser for damage. Wiggle the blades to determine
safety officer or equivalent, as well as to the hospital whether they are secure. Shake the plug, and
risk manager. listen for rattles that could indicate loose screws.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
If damage is suspected, open the plug and inspect placed. Clean or replace filters according to the
it. manufacturer’s recommendations (e.g., replace
if the pressure drop is >5 psi), and indicate this
1.5 Line Cords. Inspect line cords for signs of dam- in the preventive maintenance section of the
age. If a cord is damaged, replace the entire cord, inspection form. Clean or replace air filters and
or, if the damage is near one end, cut out the radiators that are obviously dirty.
defective portion. Be sure to wire a new power
cord or plug with same polarity as the old one. 1.13 Controls/Switches.
1.6 Strain Reliefs. Examine the strain reliefs at General. Before moving any controls, check and
both ends of the line cord. Be sure that they grip record their positions. If any position appears
the cord securely. unusual, consider the possibility of inappro-
priate use or of incipient device failure. Exam-
1.7 Circuit Breakers/Fuses. If the device has a
ine all controls and switches for physical
switch-type circuit breaker, check that it moves
condition, secure mounting, and correct mo-
freely. If the device is protected by an external
tion. If a control has fixed-limit stops, check
fuse(s), check its value and type against what is
for proper alignment, as well as positive stop-
marked on the chassis or noted in the instruction
ping. Check membrane switches for tape resi-
or service manual. Ensure that a spare is pro-
due and for membrane damage (e.g., from
vided or readily available.
fingernails, pens, surgical instruments). If
1.8 Tubes/Hoses. Check the condition of all cooling- you find such evidence, notify users to avoid
system hoses and any other hoses or tubing the using tape and sharp instruments. During the
laser may have (e.g., drain, gas). Check that they inspection, be sure that each control and
are of the correct type; that they have not become switch works properly.
cracked and do not show other signs of signifi-
cant abuse; that they are connected correctly Remote. Examine the exterior of the control for
and positioned so that they will not leak, kink, cleanliness and general physical condition. Be
trail on the floor, or be caught in moving parts; sure that housings are intact, that assembly
and that they are secured adequately to any hardware is present and tight, and that there
connectors. are no signs of spilled liquids or other serious
abuse. If the remote control is attached by
1.9 Cables. Inspect all cables and their channels or cable to the laser, ensure that the cable and
strain reliefs for general physical condition. Ex- any connectors are in good condition. Examine
amine cables carefully to detect breaks in insu- all controls and switches for general physical
lation and to ensure that they are gripped condition, secure mounting, correct motion,
securely in the connectors at each end to prevent and intended range of settings. Where a con-
strain on the cable. trol should operate against fixed-limit stops,
check for proper alignment as well as positive
1.10 Fittings/Connectors. Examine all optical (e.g., stopping. During the inspection, be sure to
fiber), liquid, and electrical fittings and connec- check that each control and switch performs
tors for general physical condition. Liquid fittings properly.
should be tight and should not leak. Electrical
contacts should be straight, clean, and bright. Footswitch. Examine the footswitch for general
There should be no visible dirt or residue in physical condition, including evidence of
the optical path of the laser aperture. Ensure spilled liquids. Footswitches for lasers include
that any mechanism to close off the laser aper- an internal switch that activates according to
ture (fiber port) is clean, operates smoothly, and the depth of pedal depression. It is usually
is in use. possible to feel the vibration caused by closure
of the switch, even through a shoe. Check that
1.12 Filters. Check the condition of all liquid and air the internal switch is operating and that the
filters. Some frequency-doubled Nd:YAG surgi- footswitch does not stick in the on position.
cal lasers require deionized water, and most Some footswitches include two internal
require special filtration. Measuring the pres- switches; in this case, verify the operation of
sure drop across a liquid filter can be helpful in both. Some footswitches also include a switch
determining whether the filter should be re- to operate the liquid- or gas-cooling system.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Frequency-Doubled Nd:YAG Surgical Lasers
Check to be sure that this switch operates (e.g., settings, displays) is indicated on both con-
reliably. trol panels.
During the procedure, check to be sure If display screens or digital displays are pro-
that the laser activates consistently when the vided for user prompts or for viewing accumu-
footswitch is depressed and that the fiber-cool- lated information (e.g., pulse or accumulated
ant system operates properly when the fiber- energy counter), ensure that each display pro-
coolant switch is activated and deactivated. vides the information expected. Ensure that user
Flex the cable at the entry to the switch, and, prompts occur in the proper sequence. Store
using an ohmmeter, check for internal wire some sample information, and verify that it is
breaks that cause intermittent operation. correct. If a feature to manually reset this infor-
Confirm that strain reliefs are secure. mation is available, ensure that it works.
Examine the male and female connectors for 1.19 Laser Delivery System Calibration. Some fre-
attaching the footswitch to the laser cabinet to quency-doubled Nd:YAG surgical lasers include
be sure that no pins are bent and that no other a user-accessible calibration port or power meter
damage is present. Ensure that the connector that allows output calibration and/or testing of
secures acceptably to the laser cabinet. the laser fiber. This feature is provided because
transmission of laser energy through a fiber may
1.15 Motors/Pumps/Fans/Compressors. Check the change as a result of fiber use. Based on the
physical condition and proper operation of these measurement from the calibration power meter,
components, if present. If lubrication is required, the laser may automatically recalibrate itself
note this in the preventive maintenance section and/or adjust displays so that the power indi-
of the form. Clean any obvious dust from these cated to be delivered to the patient will be cor-
components. rect, or it may require the user to do this
manually. Verify that this feature is functioning
1.16 Fluid Levels. Check all fluid (e.g., coolant) levels.
by using the manufacturer’s recommended cali-
Refill or change the fluid according to the manu-
bration procedure to test one delivery system
facturer’s recommendations, and note this on the
(e.g., fiber, handpiece) that the manufacturer
preventive maintenance section of the inspection
indicates can be acceptably calibrated using
form. If an external water supply is in use, ensure
these procedures. A good-quality (e.g., >85%
that the water pressure is properly regulated and
transmissibility, undamaged sheath) fiber or
at the appropriate pressure and that the supply
handpiece should be used for this test.
and drain system is properly configured (e.g.,
filters are oriented for proper flow, drain hoses
1.20 Alarms/Interlocks. Operate the device in a
are positioned in a sink or drain).
manner that will activate the self-check fea-
1.17 Battery. Inspect the physical condition of batteries ture, if present, and verify that all visual and
and battery connectors, if readily accessible. If a audible alarms activate according to the manu-
remote control or display is battery powered, check facturer’s documentation. If no self-check fea-
or replace the battery (periodic prophylactic bat- ture is present, operate the laser in a manner
tery replacement is often preferred to risking bat- that will activate each audible and visual
tery failure during use). When it is necessary to alarm; be sure to test only those alarms that
replace a battery, label it with the date. will not cause damage to the laser or present
an unnecessary risk of laser beam exposure to
1.18 Indicators/Displays. During the inspection, yourself or bystanders.
verify proper operation of all lights, indicators,
meters, gauges, and visual displays on the unit If a door or window interlock is used, ensure
and remote control. Ensure that all segments of that it deactivates the laser properly. (Do not
a digital display function. Note any error mes- disassemble major parts of the laser to test in-
sages displayed during the power-on self-test. ternal interlocks.) After deactivating the laser
and reclosing the door or window, check to be
If primary and remote-control indicators and sure that the laser will restart. Be sure to check
displays can be used at the same time or if control the interlocks in all locations where the laser is
can be switched from one to the other during a used. (For some lasers, the function of the inter-
procedure, verify that the same information locks can be checked using an ohmmeter.)
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
If the laser is equipped with an emergency use and storage. (Do not remove other parts
“kill” switch, test this feature to be sure that it thatarepress-fitorattachedbyscrews,bolts,
deactivates the laser and that the laser will or snap-rings.) If lenses are detachable, be
subsequently restart. sure not to touch the lens surface; handle
lenses by the edges only. Consult the manu-
1.21 Audible Signals. Operate the device to activate
facturer’s recommendations for the proce-
any audible signals (e.g., laser emission, setting dures and cleaning agents to use to clean
change). Check for proper operation, and verify lenses.
that the signal can be heard in the environment
in which the laser will be used. Ensure that major subcomponents of the
handpiece, when assembled, are secure. En-
1.22 Labeling. Check that all placards, labels, and sure that the mechanisms used to connect the
instruction cards noted during acceptance test- handpiece(s) to the fiber are in good working
ing are present and legible. Check to see that an order and that they reliably secure each hand-
instruction manual is kept with the laser or is piece to the fiber.
readily available.
Microscope micromanipulator. Examine the mi-
1.23 Accessories. croscope micromanipulator for cleanliness
General. Verify that all necessary accesso- and general physical condition. Be sure to
ries are available and in good physical con- handle it by the main body; do not hold it by
dition. Set up reusable accessories with the joystick, and do not touch the reflecting
the laser to ensure compatibility and proper lenses in the body. Inspect micromanipulators
functioning. provided by both the laser manufacturer and
Checking all fibers or accessories during a the laser accessory manufacturer.
single inspection and preventive mainte- Ensure that the reflecting surfaces and
nance procedure is unnecessary as long as lenses are intact and clean. Consult the
accessories are routinely checked by the per- manufacturer’s recommendations for the pro-
son(s) responsible for laser setup and opera- cedures and cleaning agents to use to clean
tion. In addition, many of the accessories are reflecting surfaces and lenses.
sterile and would require resterilization be-
fore use, making the laser potentially un- Examine the joystick to ensure that it is
available. Be sure to check with the person firmly attached and that it freely moves the
responsible for scheduling the use of the laser reflecting lens. If a finger rest is present,
before beginning the procedure. ensure that it is firmly attached and properly
Fibers. For the test fiber and before each use, oriented.
examine the connector, cable, and tip of each If a zoom focus feature is present, be sure
fiber to be used, as well as the fiber support, that it turns easily and does not slip. Examine
for cleanliness and general physical condition. each objective lens to ensure that it is intact
Ensure that the connector properly seats into and clean. Do not touch the lens surface. Con-
the laser aperture in the laser cabinet. Exam- sult the manufacturer’s recommendations for
ine the distal end of fibers to ensure that any the procedures and cleaning agents to use to
connecting mechanisms (e.g., threads) are in clean the objective lenses. Carefully insert
proper working order. each lens into the micromanipulator, and en-
If a fiber appears to be dirty or damaged, sure that it fits snugly.
remove it from service. If a fiber is reusable,
notify the person(s) responsible for fiber re- Inspect the mechanism used to attach the
pair. The fiber should be repaired and/or micromanipulator to the microscope to ensure
cleaned according to the manufacturer’s rec- that all parts are present and that it is in good
ommendations. Verify fiber performance. working order. Connect the micromanipula-
tor to the microscope to check for a secure
Handpieces. Examine each handpiece compo- connection.
nent (e.g., body, tips, lenses) for cleanliness
and general physical condition. Examine Safety filters. Verify operation of safety filters
individually only those components that in the microscope and endoscope delivery
are intended for removal during normal systems.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Frequency-Doubled Nd:YAG Surgical Lasers
1.24 Aiming Beam. Frequency-doubled Nd:YAG sur- clean area, maintaining the same distance. Ad-
gical lasers typically use an attenuated thera- just the exposure setting in increments of 0.1 sec
peutic beam as the aiming beam. Activate the or the next longest duration, and activate the
aiming beam (without the therapeutic beam), laser at each setting. Continue this process until
and verify that it produces a round, uniformly you have tested all exposure settings, except
bright spot, with no halo. continuous, and have developed a series of
burns. Compare the burns to verify that progres-
1.25 Laser Aperture. sively larger burns occurred as the exposure
WARNING: Make this inspection with the laser duration increased.
powered off. Remove and inspect the protective
window (e.g., blast shield) behind the laser aper- 2.4 Repeat Pulse. If the unit includes a Repeat Pulse
ture. It should be clean and undamaged; replace feature, which repeats the pulse at a fixed or
if needed. There should be no visible dirt or adjustable rate, test this feature with the laser
residue in the optical path of the laser aperture. set at the minimum, median, and maximum
Repeat Pulse settings, if adjustable. Some laser
2. Quantitative tests power meters can react quickly enough to be
2.1 Grounding Resistance. Use an ohmmeter, elec- used to test this feature of the laser. If you are
trical safety analyzer, or multimeter with good using such a power meter, test the laser to be
resolution of fractional ohms to measure and sure that the correct power is repeatedly deliv-
record the resistance between the grounding pin ered over the correct time period.
on the power cord and exposed (unpainted and
not anodized) metal on the chassis, accessory If your laser power meter cannot be used for
outlet, ground pins, and footswitch. We recom- this test, use the following alternative test
mend a maximum of 0.5 Ω. (If the footswitch is method. Set the laser to about 10 W and a 0.1 sec
of low voltage, grounding is not required.) exposure duration with the fiber, handpiece, or
micromanipulator attached, and verify that the
2.2 Leakage Current. Repeat Pulse feature operates as expected by
WARNING: Do not reverse power conductors moving the target material slightly between
for this or any other test. Improper attachment of each pulse. Be extremely careful to keep hands
conductors may damage the laser. out of the laser beam path. If the number or
duration between repeat pulses is adjustable,
With the laser attached to a grounded power- test that setting changes made throughout the
distribution system, measure the leakage cur- range result in the expected performance.
rent between the chassis and ground with the
unit grounded and ungrounded. The leakage cur- 2.5 Footswitch Exposure Control. Set the output
rent on the chassis should not exceed 300 µA; in time for about 5 sec, activate the unit, and re-
no case should it exceed 500 µA. Where it is lease the footswitch after about 1 sec. Verify that
greater than 300 µA, ensure that appropriate the beam turns off when the footswitch is re-
grounding is present. leased.
2.3 Exposure Duration. Some laser power meters
2.10 Power Output. Select one delivery system (e.g.,
can measure pulse duration. If the power meter
can react to pulse duration (this is the preferred fiber, micromanipulator), and perform the
circumstance), test the laser at each setting. manufacturer’s recommended user calibration
procedure. Secure the delivery system at the
However, if the laser power meter does not meas-
ure pulse duration, use the following less prefer- appropriate distance from the detector of the
able alternative. laser power meter to meet spot-size require-
ments specified in the instructions for the meter.
Place and secure the laser fiber, handpiece, or (Do not focus the beam to a small spot on the
micromanipulator with the aiming system fo- power meter. Some power meters require that
cused on the target material (e.g., black Delrin the unfocused or a defocused laser beam be pro-
or a tongue depressor). With the laser set to jected into the power meter to cover the majority
about 10 W and the exposure set at minimum of the absorber surface. If the laser beam is
duration, activate the laser and create a burn. focused on the receiver of such meters, the meter
Carefully move the target material to expose a may be damaged.)
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
WARNING: Accessing the unfocused laser polarity. Also, lasers powered by three-phase electrical
beam may require defeating internal interlocks. systems may be damaged if proper electrical phase
Because of the heightened risk associated with an connections are not made initially and maintained
unfocused, nondiverging laser beam, exercise thereafter. Thus, do not switch conductor connections
great care if the interlocks are to be defeated. or wiring configurations for any tests, including leak-
age current measurement. Do not conduct electrical
With the laser set at low (e.g., 10% of full leakage current tests with reversed-polarity wiring.
scale), medium (e.g., 50% of full scale), and maxi-
mum output, activate the laser for a sufficient Also test the ability of the laser to deliver laser
period to acquire acceptable readings. (Power energy as expected in all configurations and with all
meters use different time constants to acquire an provided laser accessories. In addition, perform the
acceptable reading, and you must know and me- following tests.
ticulously follow them.) Compare the reading
with the power display of the laser; the measured 4.1 Areas of Use. Visit the area(s) in which the laser
and displayed values should all be within 10% of is to be used and ensure that laser signs,
one another. In addition, compare the reading eyewear, and window coverings are available
obtained with the reading taken on incoming and being used and that safety interlocks for
acceptance testing, at the last preventive main- doors or windows, if present, are functioning
tenance procedure, or after the last service pro- properly.
cedure. If the laser includes a low-power (e.g.,
mW) feature, test it in a similar fashion with a 4.2 Casters/Mounts/Holders. Ensure that the as-
power meter of appropriate resolution in the sembly is stable and that the unit will not tip over
low-power range. when pushed or when a caster is jammed on an
obstacle (e.g., a line cord, threshold), as may occur
3. Preventive maintenance during transport. If the device is designed to rest
Verify that all daily preventive maintenance proce- on a shelf, ensure that it has nonslip legs or
dures recommended by the manufacturer are carried supports.
out.
4.3 Labeling. Examine the unit and note the pres-
3.1 Clean the exterior. Clean accessible optical com- ence, location, and content of all labels. Labeling
ponents (e.g., blast shield, microscope lenses), if information is typically found in the laser’s Op-
necessary, using techniques and cleaning solu- erator Manual.
tions recommended by the manufacturer.
4.4 Electrical Wiring Configuration. Ensure that
3.2 Lubricate any motor, pump, fan, compressor, or the branch circuits and the outlets for the laser
printer components as recommended by the are properly wired and rated for use with the
manufacturer. laser. Examine the receptacles at each location
3.3 Calibrate/adjust any components (e.g., printer) where the laser is to be used to ensure that the
according to the manufacturer’s recommenda- proper electrical configuration (e.g., proper neu-
tions. Only appropriately trained personnel tral and ground connections, proper phase rota-
should attempt laser adjustments. Ensure that tion) has been installed. Connect the laser to
all hoses and tubes are tight. each receptacle and confirm that the laser oper-
ates properly, specifically confirming that mo-
3.4 Replace filters as needed. Check all fluid levels tors are operating in the proper direction.
and supplement or replace fluids as needed.
4.5 AC Plug. Verify that the plug is acceptable for
4. Acceptance Testing use with the maximum current and voltage
Conduct major inspection tests for this procedure specifications for operating the laser. (Consult
and the appropriate tests in the General Devices Pro- National Electrical Manufacturers Association
cedure/Checklist 438. [NEMA] configurations for general-purpose non-
locking and locking connectors if in doubt.)
WARNING: Lasers may be damaged by switching
between normal and reverse polarity while the device is 4.6 Pulse Duration. Verify that progressive increases
on. If reverse-polarity leakage current measurements in pulse duration throughout its range of adjust-
are made, turn off the unit being tested before switching ment result in progressively larger burns.
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Frequency-Doubled Nd:YAG Surgical Lasers
4.7 Repeat Pulse. If the unit includes a Repeat Pulse provided by the laser. Or, you can calculate it
feature, test this feature as described in Item 2.4, using the following formula:
but over the full range of available settings. Delivered power
% Transmission = × 100%
Power entering the fiber
4.8 Power Range. Using the technique described in
Item 2.10, test the power output accuracy at Delivery systems with less than the manufac-
several low, medium, and high settings. turer-recommended transmission (typically
>85%) should be returned to the manufacturer.
4.9 Laser Delivery System Calibration. Use the
manufacturer’s recommended calibration proce-
dure to test each new reusable delivery system
Before returning to use
(e.g., fiber, handpiece) that the manufacturer Be sure to return controls to their starting position
indicates can be acceptably calibrated using and place a Caution tag in a prominent position so that
these procedures. Note the fiber transmission for the next user will be careful to verify control settings,
each delivery system tested if this information is setup, and function before using the unit.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Procedure/Checklist 438-0595
General Devices
Commonly Used In: Patient and nonpatient areas
Risk Level and Inspection intervals depend on device and circumstances
Type Interval Time Required
Major months . hours
Minor months . hours
Overview it, even if it entails doing part of one test early and the
rest of it later. However, do not check the Pass or Fail
This procedure provides guidance for inspection of any column until the item has been completed. To the
device for which no specific procedure is applicable; it extent possible, perform preventive maintenance
also provides more detailed instructions for some tasks tasks first; the inspection will reveal any deficiencies
commonly encountered in other procedures, along with that may have been introduced by improper or inade-
general acceptance tests for all devices. It can be used quate maintenance. If the inspection indicates the
as is for many simpler devices. Other devices will need for maintenance, reconfirm the functioning and
require additional performance checks derived from accuracy of the affected portions of the device following
manufacturer-supplied information and the clinical the repair.
engineer’s or technician’s understanding of the device
and its clinical application. Before beginning any inspection, carefully read this
procedure and the manufacturer’s instruction and
Test apparatus and supplies service manuals; be sure that you understand how to
Leakage current meter or electrical safety analyzer operate the equipment, the significance of each control
and indicator, and the alarm capabilities. Also deter-
Ground resistance ohmmeter with a resolution of mine whether any special inspection or preventive
about 0.1 Ω to around 0.5 Ω maintenance procedures are recommended by the
Hydrometer manufacturer. Skip items that are not relevant to the
device being inspected. Modify or add items if needed.
Special precautions
If there is evidence of blood or body fluid contami- 1. Qualitative tests
nation, submit the device for cleaning and decontami- 1.1 Chassis/Housing. Examine the exterior of the
nation before inspecting it. unit for cleanliness and general physical condi-
See the article on IPM Safety, behind the Guidance tion. Ensure that plastic housings are intact, that
Tab of this binder, for additional precautions and all assembly hardware (e.g., screws, fasteners) is
guidelines. present and tight, and that there are no signs of
spilled liquids (e.g., stains, dried patches), physi-
Procedure cal damage, or other serious abuse.
Do not feel constrained to follow the order of items 1.2 Mount/Fasteners. If the device is mounted on
in this or the device-specific procedures and checklists. the wall or on a stand, IV pole, or cart, examine
If a different order is more convenient, feel free to adopt the condition of the mount. Verify that the
095674 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
438-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
mounting apparatus is secure and that all hard- and that the clinical engineering (or other appro-
ware is firmly in place. Check for weld cracks. priate) department should be notified when a
Ensure that the assembly is stable. fuse blows so that it can investigate the cause
and provide another spare fuse.
1.3 Casters/Brakes. If the device moves on casters,
check their condition. Check that the casters roll 1.8 Tubes/Hoses. Check the condition of all tubing
and swivel freely. Check the operation of brakes and hoses. Check that they are correctly con-
and swivel locks. Conductivity checks, if neces- nected and positioned so they will not kink, be
sary, are generally conducted as part of a check caught by moving parts, interfere with the op-
of all furniture or devices within an area (see erator, or be damaged during operation.
Conductive Furniture and Floors Proce-
1.9 Cables. Inspect any cables (e.g., sensor, elec-
dure/Form 441).
trode, remote control) and their strain reliefs for
1.4 AC Plug/Receptacles. Examine the AC power general condition. Carefully examine cables to
plug for damage. Attempt to wiggle the blades to detect breaks in the insulation and to ensure
determine if they are secure. Shake nonmolded that they are securely gripped in the connectors
plugs and listen for rattles that could indicate at each end, which will prevent rotation or other
loose screws. If damage is suspected, open the strain. Where appropriate, verify that there are
plug and inspect it. no intermittent faults by flexing electrical cables
near each end and looking for erratic operation
If the device has electrical accessory outlets, or by using an ohmmeter.
inspect them for damage and insert an AC plug
into each to check that it is held firmly. If the 1.10 Fittings/Connectors. Examine all gas and liq-
outlets are used for critical devices (e.g., outlets uid fittings and connectors, as well as all electri-
on a resuscitation cart) or devices are plugged cal cable connectors, for general condition.
and unplugged frequently, consider more exten- Electrical contacts should be straight, clean, and
sive testing. Use a tension tester to measure the bright. Gas and liquid fittings should be tight
tension of each contact. With the device plugged and should not leak. Cracked or brittle O-rings
in, use an outlet test fixture to verify that the should be replaced. If keyed connectors are used
accessory outlet is energized and correctly wired. (e.g., pin-indexed gas connectors), ensure that no
See Electrical Receptacles Procedure/Form 437 pins are missing and that the keying is correct.
for more information. Keying pins should be securely seated in “blind”
holes so that they cannot be forced in farther.
1.5 Line Cord. Inspect all line cords, including the
battery charger line cord, for signs of damage or 1.11 Electrodes/Transducers. Verify that all elec-
inappropriate repairs (e.g., taped sections). If re- trodes, transducers, and probes are available,
placement is necessary, be sure to wire the new including spares and optional units and — espe-
power cord or plug with the correct polarity. (Re- cially for emergency and resuscitation devices —
versed hot and neutral wiring may pose a hazard an adequate supply of disposables. Check that
to service personnel since the on/off switch may not appropriate transducers and probes are being
open the hot line in the off position.) used; the use of incorrect probes (e.g., those from
another manufacturer) has caused patient in-
1.6 Strain Reliefs. Examine the strain reliefs at jury and erroneous results. Examine the physi-
both ends of the line cord. Be sure that they hold cal condition of reusable units.
the cord securely.
1.12 Filters. Check the condition of all liquid and
1.7 Circuit Breaker/Fuse. If the device has a gas (air) filters. Clean or replace as appropri-
switch-type circuit breaker, check that it moves ate, and indicate this on Line 3.1 or 3.4 of the
freely. If the device is protected by an external inspection form.
fuse, check its current rating and type against
that marked on the chassis. 1.13 Controls/Switches. Before moving any controls
and alarm limits, check their positions. If any of
If there is a spare fuse holder, verify that a them appear inordinate (e.g., a gain control at
fuse of the same rating and type is provided. If maximum, alarm limits at the ends of their
the spare fuse is missing, advise clinical person- range), consider the possibility of inappropriate
nel that a spare fuse is provided primarily to clinical use or incipient device failure. Record
expedite a rapid return of the device to operation the settings of those controls that should be
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
General Devices
returned to their original positions following the Check the condition of the battery charger, and
inspection. verify that battery charge indicators function.
Check parameters that may be set on “hidden” 1.18 Indicators/Displays. During the course of the
user or service menus, including special modes inspection, verify the operation of any lights,
and alarm on/off, volume, and default values. indicators, meters, gauges, and visual displays on
the unit and charger. Ensure that all segments of
Examine all controls and switches for physical a digital display function. Observe a signal on a
condition, secure mounting, and correct motion. waveform display, and note any problems (e.g.,
Check that control knobs have not slipped on distortion, poor focus, 60 Hz interference).
their shafts. If a control has fixed-limit stops,
check for proper alignment, as well as positive 1.19 Calibration/Self-Test. Verify that the calibra-
stopping. Check membrane switches for mem- tion function operates. (Where a quantitative
brane damage (e.g., from fingernails, pens). Dur- check is required, add it to the quantitative sec-
ing the course of the inspection, ensure that each tion.) Activate self-test or service-mode functions
control and switch performs its proper function. that allow simple performance verification.
1.14 Heater. Examine the heater for damage (e.g., 1.20 Alarms/Interlocks. Induce alarm conditions to
corrosion of its sheath, deteriorated insulation). activate audible and visual alarms. Check that
To the extent possible, operate the heater to all associated interlocks or features function (e.g.,
verify that its controls function properly (e.g., an infusion pump initiates KVO rate upon
that a variable temperature control does, in fact, alarm). If the device has an alarm-silence feature,
control heater power). check the method of reset (i.e., manual or auto-
matic) against the manufacturer’s specifications.
1.15 Motor/Pump/Fan/Compressor. Check the physi-
cal condition and proper operation of these compo- Verify that alarms are loud, distinctive,
nents. Check mechanical alignment and proper and/or bright enough to be noticed in the envi-
adjustment of any pulleys, gears, belts, chains, etc. ronment in which the device will normally be
Look for any signs of improper or excessive wear, used. If a remote alarm-indicator is required,
such as metal filings. Lubricate if required, and verify that it is available and functioning. Audi-
note this on Line 3.2 of the form. (However, do not ble alarm-volume controls should not allow the
check the line until all lubrication is completed.) alarm to be turned off or lowered to an indiscern-
ible volume.
1.16 Fluid Levels. Check all fluid levels, including
those in lead-acid batteries. Check alarm parameters that may be set on
hidden menus (see Item 1.13).
1.17 Battery/Charger. Inspect the physical condi-
tion of all batteries and battery connectors if If inspections repeatedly reveal that alarms
readily accessible. Disposable carbon zinc bat- have been turned off or silenced or that the
teries may leak and must be inspected. We are volume has been adjusted too low, inappropriate
not aware of significant leakage problems with use is indicated, and user in-service training is
most other battery types. required.
Check operation of battery-maintained mem- 1.21 Audible Signals. Operate the device to activate
ory and battery-operated power-loss alarms, if so any audible signals (e.g., QRS beeper). Check for
equipped. proper operation of the volume control, and ver-
ify that the signal can be easily heard in the area
Operate the unit on battery power for several
in which the device will be used.
minutes to verify that the battery is charged and
can hold a charge. Activate the battery test func- 1.22 Labeling. Check that all necessary placards, la-
tion (if so equipped), or measure the output volt- bels, conversion charts, and instruction cards
age with the unit on to assess battery capacity. are present, legible, and easy to understand.
(The inspection can be carried out on battery
power to help confirm adequate battery capac- 1.23 Accessories. Verify that all necessary accesso-
ity.) Measure the specific gravity of lead-acid ries are available and in good condition. A copy
batteries. When it is necessary to replace a bat- of the instruction manual should be readily
tery, label it with the date. available to the user.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
2. Quantitative tests connecting cord. The instrument is not usually
grounded. Assuming that the device has met
Most quantitative tests are device specific. Appro- incoming inspection requirements, grounding is
priate tests are listed in the individual procedures or not required.
should be derived from device specifications and an
understanding of the device’s clinical application and 2.2 Chassis Leakage Current. With the polarity of
design. However, the following electrical safety tests the power line normal and the equipment ground
are common to all line-powered devices. (Refer to the wire disconnected, measure chassis leakage cur-
article on Electrical Safety, behind the Guidance Tab rent with the device operating in all normal
of this binder, for the rationale, recommended inter- modes, including on, standby, and off. If the unit
vals, and additional discussion of electrical safety test- has heating and cooling modes, set the thermo-
ing requirements.) stats so that each operates while readings are
taken. Record the maximum leakage current; it
2.1 Ground Resistance. Using an ohmmeter, elec- should not exceed 300 µA for equipment used in
trical safety analyzer, or multimeter with good patient care areas or 500 µA for devices in non-
resolution of fractional ohms, measure and re- patient care locations (e.g., nurses’ station, clini-
cord the resistance between the grounding pin of cal laboratory).
the power cord and exposed metal on the chassis.
Conductive portions of the chassis or housing The measurements should be made with all
that may become energized must be grounded. accessories that are normally powered from the
Metal trim, nameplates, and handles that are same line cord connected and turned on. This
unlikely to be exposed to current-carrying com- applies to devices that are plugged into accessory
ponents of the device need not be grounded. outlets on the device and to devices that are
plugged into a multiple-outlet strip (“Waber
Since poor test lead contact can increase
strip”) so that the devices are grounded through
ground resistance measurements, ensure that
a single line or extension cord.
both test leads are in firm contact with a portion
of the ground prong or chassis that is clean and Leakage current must be measured with the
shiny (e.g., unpainted and not anodized). Also device powered by a conventional (grounded)
check that the ohmmeter reads zero when the power system, even if it is normally used in an
leads are shorted together. area with isolated power. If the device has a
special plug (e.g., explosion proof), a correspond-
Verify that all modules or cable-connected
ing adapter is required.
parts of a system are grounded. If the device has
an accessory outlet, check its grounding to the During routine inspections, it is necessary to
main power cord. test leakage current only in the correct-polarity,
ungrounded mode. If testing in the reversed-po-
Although a stable grounding resistance as
larity mode, remember that some devices, espe-
high as 0.5 Ω is acceptable, an increase in
cially those incorporating a microprocessor,
grounding resistance from one inspection to an-
motor, or compressor, may be damaged by
other may indicate a loosening connection. Open
switching polarity while the device is on. To
the unit or plug, look for the cause of the increase
avoid damage, turn off the unit until the motor
(e.g., a loose or corroded connection), and repair
stops or for at least 10 sec before switching
it.
polarity. Routine lead leakage current measure-
Double-insulated devices may or may not be ments are also not required.
grounded. ECRI believes that either design is
satisfactory. Do not measure grounding resis- Interference from stray radio-frequency (RF)
tance of double-insulated devices unless designed fields or currents produced by some high-fre-
to be grounded; just indicate “DI” on the inspec- quency devices (e.g., electrosurgical units, dia-
tion form. Some double-insulated devices may thermy units) may cause erroneous leakage
have a three-prong plug, but the grounding prong current readings. Two signs of such interference
may be unconnected; this poses no safety risk. are readings obtained with the leakage current
probe held near (but not contacting) the device
Some devices are powered (or recharged) by and needle deflection that does not change ac-
an AC adapter that plugs into a wall outlet and cordingly as the meter scales are changed. In the
carries a low voltage to the instrument by a event of interference, try a different leakage
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
General Devices
current meter, place a small capacitor (0.1 µf) Inspect/clean interior. Opening the housing for
across the leakage current meter input termi- internal cleaning is unnecessary and not rec-
nals, or measure leakage currents with the RF ommended for many devices. Where appro-
generator off. priate (e.g., units with ventilation fans
without air filters, units with evidence of
Though confirmation of grounding integrity spilled fluids that may have entered the unit,
provides reasonable assurance of safety for de- some units with high DC voltages), inspect the
vices with permanent redundant grounding interior of the unit and look for accumulations
(e.g., a bedside monitor grounded through the of dirt, dust, spilled fluids, foreign objects,
line cord and its central station connection), excessive lubrication, and signs of mechanical
NFPA 99 calls for measurement of chassis leak- wear. Clean as necessary. Refer to the Pre-
age current with the redundant ground intact. ventive Maintenance and Cleaning article, be-
2.2. (Alternative) Ground Voltage (For Installed Equip- hind the Guidance Tab of this binder, for
ment). Chassis leakage current of permanently guidelines on the selection of cleaning sol-
wired equipment cannot be readily measured after vents and appropriate techniques.
installation is completed. Though confirmation of 3.2 Lubricate. Lubricate mechanical components
grounding integrity provides reasonable assur- such as motors, bearings, chains, wheels, hinges,
ance of safety, NFPA 99 calls for voltage measure- latches, etc. that have friction points. Excessive
ments for installed devices in the patient vicinity. or inappropriate lubrication can cause damage;
Using a voltmeter, electrical safety analyzer, or refer to the manufacturer’s literature for lubri-
multimeter with appropriate resolution, measure cation requirements. Refer to the Preventive
and record the voltage between a reference Maintenance and Cleaning article, behind the
grounding point (e.g., the grounding pin of an Guidance Tab of this binder, for additional infor-
electrical receptacle or some other known ground) mation on lubrication.
and exposed (i.e., unpainted and not anodized)
metal on the chassis. A voltage reading of 500 mV 3.3 Calibrate/Adjust.
is acceptable for general care areas, and 40 mV is Electrical components. Perform calibration and
acceptable in critical care areas. adjustments as recommended by the manu-
facturer or indicated by inspection results.
3. Preventive maintenance
Mechanical components. Verify the integrity
Most preventive maintenance tasks are device spe- and proper operation of all mechanical com-
cific. Appropriate tasks are called out in the individual ponents and hardware. Inspect for loose
procedures or should be derived from device specifica- and worn components, and tighten as neces-
tions and an understanding of the device’s clinical sary. Align and tighten external control
application and design. However, the following items knobs, switches, and indicators. Ensure the
should be considered and incorporated as appropriate. proper operation of mechanical brakes and
3.1 Clean. interlocks.
Exterior and accessories. Cleaning the exterior 3.4 Replace. Replace liquid, gas, and ventilation
of the equipment is normally the responsibil- (air) filters; deteriorating, cracked, or dry-rotted
ity of the user; however, some users grow tubing; motor brushes; missing spare fuses; O-
complacent or accustomed to the appearance rings; and other components as needed or at
of the equipment. Thus, a periodic extra effort intervals recommended by the manufacturer.
may be required to maintain the appearance
and prevent operational problems. Refer to 4. Acceptance tests
the article on Preventive Maintenance and
Upon initial receipt of a device or following repair,
Cleaning, behind the Guidance Tab of this
make a thorough visual inspection. Add the following
binder, for guidelines on the appropriate
supplemental items to the qualitative and quantitative
cleaning solvents and techniques.
tests that would be conducted during a major inspec-
Clean filters as appropriate (most filters are tion. In addition, conduct appropriate specific tests as
disposable and should be replaced as needed). indicated in the individual inspection procedures and
as required to verify purchase order and manufacturer
Flush fluid lines and reservoirs as necessary. specifications.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
A.1 Qualitative acceptance tests moved frequently. A good quality two-prong
plug is acceptable for double-insulated devices.)
A.1.1 Chassis/Housing. Check for shipping damage; If a special plug is required (e.g., explosion
report any damage to the manufacturer, ship- proof), it should be of suitable type and quality.
per, or service organization, and arrange for Replace the plug or have the supplier replace it
repair or replacement. if it is not Hospital Grade or otherwise suitable.
Check that the unit is suitably constructed to Hospital Grade molded plugs are acceptable.
withstand normal hospital use and abuse. For If the device has electrical accessory outlets,
instance, a unit with venting on the top of the use an outlet test fixture, and with the device
housing or poorly protected or sealed controls plugged in, verify that the accessory outlet is
and indicators may be prone to fluid entry. (Such energized and correctly wired.
design deficiencies should usually be recognized
during prepurchase evaluation. However, if any A.1.5 Line Cord. Ensure that the line cord is long
are evident, discuss corrective action with the enough for the unit’s intended application; an
manufacturer. If not correctable, warn users or extension cord should not be required. (A length
take other preventive measures.) of 10 ft [3 m] is suitable for most applications,
although 18 ft [5.5 m] has been suggested for
A.1.2 Mount. Ensure that the assembly and weight operating room equipment.)
distribution is stable and that the unit will not
tip over when pushed or when a caster is The cord should be of suitable quality and
jammed on an obstacle (e.g., line cord thresh- current-carrying capacity. Hard Service (SO,
old), as may occur during transport. If the de- ST, or STO), Junior Hard Service (SJO, SJT, or
vice is designed to rest on a shelf, ensure that SJTO), or an equivalent-quality cord should be
it has nonslip legs or supports. used.
Inspect wall-mounted devices at the time of If the line cord is operator detachable, affix
installation to verify that the mounting technique the cord to the unit so that it cannot be removed
is appropriate for the weight of the device. Attach- by the operator, or at least label the cord promi-
ing the unit to wallboard (e.g., with Molly bolts) nently (e.g., 120 V), especially for devices that
is unacceptable except for very light devices. Gen- are used in the vicinity of monitors that use
erally, objects should not be mounted over a pa- patient leads. (Electrode lead wires have been
tient. The device should be mounted in a position inserted into line-cord connectors; see Health
and height where it can be easily viewed, ad- Devices 1993 May-Jun; 22:301-3.)
justed, and used by clinical personnel and where
A.1.7 Circuit Breaker/Fuse. If the device is protected
it will not be bumped or hinder access to the
by an external fuse, verify that the fuse type is
patient for routine or emergency care. If the unit
labeled and that all fuses and spares are the
has a heating element, keep hoses, wires, and
proper current rating and type. If the value and
cables away from the unit and place the unit so
type are not labeled, check the manual for the
that patients, staff, and visitors are protected
proper current rating and type and perma-
against contact with hot surfaces.
nently mark this information on the unit hous-
A.1.3 Casters/Brakes. Verify that the correct casters ing near the fuse holder. If no spare fuse is
have been supplied with the unit (e.g., size, provided, consider attaching a fuse clip and
correct swivel). (ECRI recommends 5 in [12.7 spare fuse, particularly for high-risk devices.
cm] diameter casters for mobile devices to re-
Especially for critical or life-support devices,
duce shock to the unit and to minimize the effort
verify that accessory outlets have independent
required to roll the unit across elevator thresh-
overcurrent protection (fuse or circuit breaker)
olds and other uneven surfaces.) Verify brake
so that a short in a device plugged into the
operation.
accessory outlet or an accessory overload will
A.1.4 AC Plug/Receptacles. Verify that the plug is not disable the primary device. If this is not
Hospital Grade (identifiable by a green dot available, then consider labeling the primary
and/or labeling). (A plug of good quality, even if device to clearly indicate where the unit’s fuse
not Hospital Grade, may be left on a device that or circuit breaker is located, and/or install a
is plugged and unplugged infrequently. Right- fused Hospital Grade (or similar quality) plug
angle plugs are unacceptable for devices that are on any commonly used accessories that are not
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
General Devices
already provided with suitable overcurrent A.2 Quantitative acceptance tests
protection.
A.2.2 Chassis Leakage Current.
A.1.10 Fittings/Connectors. Verify that other hospital
Note: Some devices (especially devices incorpo-
equipment or systems to which the device is to be
rating a microprocessor, motor, or compressor)
connected have the matching connectors. Devices
may be damaged by switching polarity while the
that connect to the central piped medical gas
device is on. If you perform reverse polarity test-
system should have the matching DISS or quick-
ing, turn off the unit until the motor stops or for at
connect fitting for the appropriate gas. Verify
least 10 sec before switching polarity.
that suitable connectors are supplied with the
device so that adapters are not required. Measure chassis leakage current as de-
scribed in Item 2.2. Reversed polarity testing
A.1.13 Controls/Switches. Verify that software setup
is not required, although some hospitals per-
parameters accessible through hidden or service
form this measurement; it may be advisable on
menus are correctly set for the appropriate appli-
a device of questionable quality or on devices
cation and are consistent for all units. Instruction
used in the home.
and service manuals may contain instructions
regarding such modes. If they do not, contact the Be alert for leakage current of the device in
manufacturer. Discuss appropriate settings with the off mode that is greater than about 30 µA
the department head and users. If alarm capa- and is greater than or equal to the leakage
bilities are included, see Item A.1.20. current in the on mode. Although this may be
normal and proper for the device, it may indi-
A.1.17 Battery/Charger. To determine operating cate that the on/off switch is incorrectly wired
time, charge the battery overnight (or install in the neutral (instead of the hot) line. Incor-
fresh batteries), then operate the device on bat- rect switch wiring poses a risk to service per-
tery power with all commonly used functions sonnel who believe that the power is
activated. For critical care monitors and thera- disconnected when the switch is off. Check the
peutic devices, it may be desirable to disconnect wiring, or contact the manufacturer.
the battery and determine if the device still
operates on line power. Inspect AC adapters used to power (or re-
charge) certain devices for UL (or other testing
A.1.20 Alarms. Verify that critical alarms cannot be laboratory) listing and to verify that it is labeled
turned off, silenced, or defeated without ade- to identify the device with which it is to be used.
quate warning to the operator or automatic ECRI recommends testing of adapters, particu-
alarm reactivation after a short delay (see larly those that are not listed, by measuring the
Health Devices 1987 Feb; 16:39-44 and 1989 leakage current from each secondary (low volt-
Dec; 18:426-7.) Such deficiencies should usually age) connection to ground. The leakage current
be recognized during prepurchase evaluation. should not exceed the limits for the device chas-
However, if any are found, review the justifica- sis leakage current to ground (300 µA in patient
tion for purchasing this device and discuss cor- care areas, 500 µA in nonpatient care areas).
rective action with the manufacturer. (Alarm See the article on Electrical Safety, behind the
features may be optional or programmable.) If Guidance Tab of this binder, for further details
no remedy is available, a user training program and a discussion of the use of these devices in
should be instituted to reduce the risk of incor- hospitals.
rect use. A warning label on the device or a
poster in the area of use may be appropriate. Measure chassis leakage current of perma-
nently installed (hardwired) equipment during
A.1.23 Accessories. Verify that all necessary features installation only. Before connecting the equip-
and accessories (e.g., transducers) have been ment to ground, measure the leakage current
supplied with the unit. At least one copy each from chassis to ground. The ungrounded leak-
(two are generally preferred) of the instruction age current should be less than 5 mA.
and service manuals, including schematics,
should be shipped with the unit and filed in the ■ ■ ■
central equipment file. A copy of the instruction Experience has not demonstrated the need for lead
manual should be kept with the unit and read leakage and input isolation testing (Items 4.1 through
by all operators before the device is put in use. 4.3) on a routine basis. NFPA 99 specifically excludes
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
the need for periodic lead leakage current testing. We WARNING: Testing input isolation requires
recommend that these tests be performed only during the use of a line voltage source. Perform this test
acceptance testing or following input circuitry repairs. only with an electrical safety analyzer or other
setup that allows safe application of the voltage
4.1 Lead-to-Ground Leakage Current. Measure to the patient leads. Be sure that a current-limit-
leakage current from patient leads (or other ap- ing resistor is included in the setup, but continue
plied parts, such as probes) to ground on any to be careful not to contact any exposed leads,
electrical device that has leads that are inten- since it is still possible to receive a shock.
tionally attached to or held against the patient
or on any device that has a conductive invasive Apply 120 VAC (line voltage applied through
connection. Perform the test with the device on a current-limiting resistor) to each isolated pa-
and with the ground wire intact and open, in all tient connection individually, and measure the
normal operating modes. resulting current (sink current) with the unit
turned on and operating and the power cord
If the device is of nonisolated design and is not
grounding connector intact. The current should
intended to be connected to the heart by a con-
not exceed 50 µA at the patient end of the cable.
ductive lead or fluid-filled catheter, leakage cur-
rent should be 100 µA or less, measured from all
the leads connected together to ground. Before returning to use
If the device has isolated patient connections Ensure that all controls are set properly. Set alarms
(see the article on Electrical Safety, behind the loud enough to attract attention in the area in which
Guidance Tab of this binder, for a discussion of the device will be used. Other controls should be in
isolation), it should be labeled “Isolated” on the their normal pre-use positions.
front panel by the manufacturer or have the IEC
Attach a Caution tag in a prominent position on
symbol signifying isolation (a heart within a
life-support equipment or any other device where the
square). These units are designed to be safe for
user must be aware that control settings may have
use when connected to a conductive lead or fluid-
been changed.
filled catheter that is within, or in contact with,
the heart. Normally, only one lead of the device With battery-powered devices, either recharge the
will be in contact with the heart (or create a battery or equip the device with fresh batteries. When
conductive path to the heart); individually test a new battery is installed, label it with the date.
each lead that may be connected to confirm that
leakage current to ground is 10 µA or less with General Devices Checklist Template
the unit ground intact and 50 µA or less with the
ground open (the open ground limit is a change The checklist associated with this procedure is a
introduced in the 1990 version of NFPA 99). template that can be used to develop checklists and
accompanying procedures for any device. The General
If the device housing is not grounded, measure Devices procedure is the foundation for the template
leakage current from each lead to the housing. and will provide many of the IPM ingredients common
4.2 Interlead Leakage Current. Measure the leakage to line- or battery-powered devices. The first step in
current between leads on devices with multiple using the template is to place a check mark in the
patient leads or contacts. Measure between each Major column for each item that applies to the device.
lead (except ground). Perform the test with the The second step is to determine the specific IPM
device on and with the ground wire both intact and elements that will ensure the safe and effective opera-
open, in all normal operating modes. For noniso- tion of the device. This task focuses on identifying
lated connections, the leakage current should not unique accessories and any parameters requiring
exceed 50 µA (grounded or ungrounded). For iso- measurement (e.g., temperature, pressure, flow). At
lated input connections, the leakage current this point, the author of a new IPM procedure must
should not exceed 10 µA with the device ground specify performance criteria, methods for assessing
intact or 50 µA with the ground open. the criteria, and the frequency for conducting the
major and, if needed, minor IPM procedures. IPM
4.3 Lead Input Isolation. This test should be per- Task ManagerTM, the software component of the IPM
formed only during acceptance testing or follow- System, can then be used to prepare a final procedure
ing input circuit repairs. and device-specific checklist.
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 430-0595
Heart-Lung Bypass Units
Used For:
Heart-Lung Bypass Units [11-969]
Pumps, Extracorporeal Perfusion [13-203]
Also Called: Cardiopulmonary perfusion equipment, heart-lung machines, heart-lung pumps, bypass machines
Commonly Used In: Operating rooms for cardiac surgery
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major * months . hours
Minor NA months . hours
* Heart-lung machines and accessories should be inspected after every 100 hours of use or quarterly, whichever
comes first, barring specific hospital circumstances or manufacturer recommendations to the contrary. The
perfusionist should check pump occlusion before each procedure.
Overview operate at up to 6 L/min, depending on patient require-
ments. A backup arterial pump is usually provided.
Cardiopulmonary perfusion equipment, commonly re- Venous blood normally requires no pumping because
ferred to as heart-lung machines, provides cardiopul- it flows by means of gravity to a reservoir. Membrane
monary support for a patient during open-heart oxygenators (the most common variety; bubble oxy-
surgery, permitting cardiovascular surgeons to isolate genators are rarely used today) require that the arte-
the heart from the circulatory system to perform car- rial pump be positioned between the venous reservoir
diac repairs or valve replacements. The great vessels and the oxygenator and that it actively pump blood
returning to (venae cavae) and leaving (aorta) the from the reservoir to the oxygenator. Because continu-
heart are cannulated, allowing an external circuit to ous operation is imperative, the arterial pump must be
provide circulation and oxygenation while the heart connected to a battery pack, as well as to the emer-
and lungs are bypassed. (For more detailed informa- gency power system. As an additional precaution, a
tion on the procedure, see: Reed CC, Stafford T. Car- hand crank should be kept with each pump in the event
diopulmonary bypass. 2nd ed. Houston: Texas Medical of a power failure.
Press, 1985.)
Cardiopulmonary perfusion systems usually consist Control and monitoring devices. A number of acces-
of blood pumps; control and monitoring devices; and a sories are needed for controlling and monitoring per-
disposable oxygenator, cardiotomy reservoir, tubing fusion. Blood temperature in the extracorporeal
set, and filters. circuit is regulated to produce hypothermia or nor-
mothermia. Oxygenators typically incorporate a heat
Blood pumps. Blood pumps propel blood through the exchanger, and water must be delivered to the ex-
extracorporeal circuit and return extravascular blood to changer at a specified temperature. A mixer valve
the circulating volume using suction (e.g., autotransfu- regulates hot and cold water delivered to the heat
sion, intracardiac suction). The arterial pump propels exchanger; it usually has a thermometer and water
blood through the oxygenator to the patient and may pressure relief valves to prevent overpressurizing the
009070 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
430-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
exchanger part of the oxygenator. A separate electri- to the patient, usually after passing through a blood-
cally powered heater/cooler may be used instead of a line filter in the arterial line. A shunt around the
mixer to provide temperature-regulated water to the blood-line filter permits continued flow if a clogged
heat exchanger. filter must be changed. Some perfusionists incorpo-
rate a filter in this shunt line as well, since releasing
Oxygen is delivered to venous blood from tanks or a clamps to change filters may cause unloading of the
central oxygen supply. A flowmeter and bacteriologic filtrates.
filter are usually incorporated in the oxygen circuit.
Blood oxygen and carbon dioxide concentrations are Suction pumps recover blood at the surgical site and
usually monitored by blood gas determinations from return it to the circulating volume. Intracardiac suc-
drawn samples, but they may be monitored using an tion returns extravascular blood to the cardiotomy
in-line differential oxygen monitor. An oxygen satura- reservoir, where it is filtered and then drained or
tion meter may be used to assess oxygenation. Other pumped to the venous side of the oxygenator. Suction
devices may be used to provide blood chemistry infor- for ventricular vents may also be controlled by suction
mation throughout the perfusion. pumps. Blood from the cardiotomy reservoir may be
passed through an additional blood-line filter before
Temperature monitors may be used, with probes returning to the oxygenator.
placed at various points on the patient or in the extra-
corporeal blood circuit. Citations from Health Devices
Level detectors may be used to monitor the level of Heart-lung bypass machines, 1973 Apr; 2:152.
blood in the reservoirs. These detectors are often
Sarns air bubble detector system [Evaluation], 1981
equipped with audible and visual alarms and may also
Jan; 10:55.
stop the arterial blood pump to avoid pumping air into
the patient in the event of a low blood level in a Delta automatic shutoff valve [Evaluation], 1981 Jan;
reservoir or to avoid too much blood volume in the 10:62.
extracorporeal circuit in the event of a high blood level.
A special valve may be incorporated in the arterial Improper bulb replacement causes Sarns model 7000
tubing to prevent infusion of large amounts of air. Air MDX heart-lung bypass pump failure [Hazard],
bubble detectors give audible and visual alarms and 1987 Jun; 16:218-9.
may also stop the arterial blood pump if air is detected
in the arterial line. Test apparatus and supplies
Ground resistance ohmmeter
Pressure monitors record left atrial, pulmonary ar-
Leakage current meter or electrical safety analyzer
tery, and arterial pressures. These monitors, which
may be included in the console, the drive pressure Equipment for inspecting blood pressure monitors
transducers, or the monitors, may be slaved to other and pressure transducers, as specified in Blood
pressure monitoring equipment. Pressure Monitors, Invasive Procedure/Checklist
434 and Pressure Transducers Procedure/Checklist
Blood contact with foreign surfaces requires that the 435, respectively
coagulation (clotting) mechanism of the blood be con-
trolled to a point where coagulation is inhibited, but in Thermometer accurate to at least 0.5°C over a range
a reversible manner. Heparin is the anticoagulant of 15° to 43°C (a temperature-monitoring device
used in perfusion, and its level must be monitored made of a thermometer sealed into one leg of a Y or
throughout the perfusion to prevent clot formation or T connector, such as is used for the inspection of
overheparinization. hypo/hyperthermia units, may also be used)
Stopwatch or watch with a second hand
Oxygenator, cardiotomy reservoir, filters, and tub-
ing set. These disposable components form the extra- Hydrometer
corporeal blood circuit. The perfusionist usually lays Oxygen flowmeter with 1 to 10 L/min range and 2%
out the circuit, which is made up as a sterile custom accuracy
pack by a manufacturer. Graduated cylinder with at least 1 L capacity (a
Blood taken from the venae cavae normally flows by fluid flowmeter with 0 to 10 L/min range and 5%
gravity (a venous clamp may be used to regulate flow) accuracy may be used)
to a venous reservoir and is then pumped through the Large bucket (5 L) for collecting fluid when checking
oxygenator. After leaving the oxygenator, blood flows high flow settings
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Heart-Lung Bypass Units
Disposable supplies, such as tubing and assorted that it is held firmly. If accessories are plugged
fittings for connecting tubing and test equipment and unplugged often, consider a full inspection
Conductive lubricant, such as Dow #41 graphited oil of the receptacle.
or the equivalent, for conductive casters
1.5 Line Cord. Inspect the cord for signs of damage.
Torque measurement device for checking pump (if If damaged, replace the entire cord, or if the
required) damage is near one end, cut out the defective
portion. Ensure that the line cord is of sufficient
Procedure length to preclude the use of extension cords. Be
Before beginning an inspection, carefully read this sure to wire a new power cord or plug with the
procedure and the manufacturer’s instruction and same polarity as the old one. Also check line
service manuals; be sure that you understand how to cords of battery chargers.
operate the equipment, the significance of each control
1.6 Strain Reliefs. Examine the strain reliefs at
and indicator, and the alarm capabilities. Also deter-
both ends of the line cord and all accessory cords.
mine whether any special inspection or preventive
Be sure that they hold the cord securely.
maintenance procedures or frequencies are recom-
mended by the manufacturer. 1.7 Circuit Breaker/Fuse. If the device has a
Because some inspection items require multiple switch-type circuit breaker, check that it moves
data points and several pumps need to be checked, freely. If the device is protected by an external
enter additional data on the reverse side of the inspec- fuse, check its value and type against that
tion form. marked on the chassis, and ensure that a spare
is provided.
1. Qualitative tests
1.8 Tubes/Hoses. Check the condition of all tubing
1.1 Chassis/Housing. Examine the exterior of the and hoses in the water mixer. Be sure that they
unit for cleanliness and general physical condi- are not cracked, kinked, or dirty. Check for
tion. Be sure that plastic housings are intact, evidence of leaking.
that necessary assembly hardware is present
and tight, and that there are no signs of spilled 1.9 Cables. Inspect the cables of the level sensor and
liquids or other serious abuse. bubble detector and oxygen, temperature, and
pressure monitors, if so equipped, and their
1.2 Mount/Fasteners. Examine each pump module strain reliefs for general condition. Examine
and any other accessories mounted to the cart or cables carefully to detect breaks in the insulation
console for security of attachment. Check the and to ensure that they are gripped securely in
integrity of all special mounting hardware for the connectors at each end to prevent rotation or
oxygenators and cardiotomy reservoirs. other strain.
1.3 Casters/Brakes. If the device moves on casters,
check their condition. Look for accumulations of 1.10 Fittings/Connectors. Check the general condi-
lint and thread around the casters, and be sure tion of all gas and liquid fittings and connectors,
that they turn and swivel, as appropriate. Check such as those on the oxygen flowmeter and water
the operation of brakes and swivel locks, if the mixer, as well as all electrical cable connectors.
unit is so equipped. Conductivity checks, where Electrical contact pins or surfaces should be
appropriate, are usually done more effectively as straight, clean, and bright.
part of a check of all equipment and furniture of 1.11 Electrodes/Transducers. Confirm that neces-
an area. sary electrodes and/or transducers are on hand,
1.4 AC Plug/Receptacles. Examine the AC power and check their physical condition.
plug for damage. Attempt to wiggle the blades
to determine that they are secure. Shake the 1.13 Controls/Switches. Before moving any controls
plug and listen for rattles that could indicate and alarm limits, check their positions. If any of
loose screws. If any damage is suspected, open them appear inordinate, consider the possibility
the plug and inspect it. of inappropriate clinical use or of incipient device
failure. Record the settings of those controls
If the device has electrical receptacles for ac- that should be returned to their original posi-
cessories, insert an AC plug into each, and check tions following the inspection.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
Examine all controls and switches for physical indicators, meters, gauges, and visual displays on
condition, secure mounting, and correct motion. the unit and the charger, if so equipped. Be sure
Where a control should operate against fixed- that all segments of a digital display function.
limit stops, check for proper alignment, as well
as positive stopping. Check membrane switches Examine the oxygen flowmeter for signs of
for membrane damage (e.g., from fingernails, damage or abuse, such as internal nicks,
pens). During the course of the inspection, be scratches, cracks, condensation, or debris. The
sure to check that each control and switch per- valves on some machines do not have a fixed-end
forms its proper function. stop; take care not to overtighten. Check for free
play in the control valve by pushing, pulling, and
1.14 Heater/Mixer. If the unit uses a heater for tem- rocking the stem from side to side with rotation.
perature control, examine the heater for physical The stem should feel firm, and the flowmeter
condition (e.g., verify that a variable tempera- float should not move.
ture control does, in fact, determine the amount
of heating; verify that on/off controls work). 1.20 Alarms/Interlocks. Operate the device in such a
way as to activate each audible and visual alarm.
If the unit uses a mixer valve for temperature Check that any associated interlocks function.
control, examine the valve for proper operation. Check that, once the alarm condition has been
If a high-temperature cutoff is incorporated in corrected, the pumps will start and function prop-
the valve, check its function. Be sure that hot erly. If the device has an alarm-silence feature,
and cold connectors are adequately placarded to check the method of reset (e.g., manual or automat-
prevent cross connection. ic) against the manufacturer’s specifications.
1.15 Motors/Pumps. Confirm the physical condition
1.21 Audible Signals. Operate the device to activate
and proper operation of all pump heads and their
any audible signals. Confirm appropriate vol-
associated motors and transmissions. Eccentric-
ume, as well as the operation of a volume control.
ity of rollers, belt tension, and occlusion mecha-
nisms should be within the manufacturer’s 1.22 Labeling. Check that all necessary placards, la-
specifications. Lubricate bearings if required, bels, conversion charts, and instruction cards
and note this on Line 3.2 of the inspection form. are present and legible.
Ensure that an emergency hand crank is at-
tached to the unit and that the hand crank will 1.23 Accessories. Confirm the presence and condition
turn the pump when power is disconnected. of such accessories as a level sensor and an
oxygenator light. If a venous line clamp is used,
1.16 Fluid Levels. Check all fluid levels, including check that it operates smoothly.
those in lead-acid batteries. Replenish if low.
1.24 Water Supply. If the water supply used for tem-
1.17 Battery/Charger. Inspect the physical condi-
perature control has gauges, check for appropri-
tion of batteries and battery connectors, if read-
ate water pressure and temperature. Verify that
ily accessible. Check operation of
incoming water temperature and pressure con-
battery-operated power-loss alarms, if so
trollers or limitation devices are in place, and if
equipped. Operate the unit on battery power for
possible, verify that they are functioning. (A
several minutes to check that the battery is
pressure-relief valve should be used to prevent
charged and can hold a charge. Check remain-
overpressurizing the oxygenator.)
ing battery capacity by activating battery test
function or by measuring the output voltage; for
lead-acid batteries, measure the specific gravity. 2. Quantitative tests
For sealed lead-acid batteries, it may be neces-
2.1 Grounding Resistance. Using an ohmmeter,
sary to perform a capacity test by running the
electrical safety analyzer, or multimeter with
equipment until the batteries are depleted.
good resolution of fractional ohms, measure and
Check the condition of the battery charger and,
record the resistance between the grounding pin
to the extent possible, confirm that it does, in
of the power cord and exposed (unpainted and
fact, charge the battery. When it is necessary to
not anodized) metal on the chassis. We recom-
replace a battery, label it with the date.
mend a maximum of 0.5 Ω. If the device has an
1.18 Indicators/Displays. During the course of the accessory outlet, check its grounding to the main
inspection, confirm the operation of all lights, power cord.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Heart-Lung Bypass Units
2.2 Leakage Current. Measure chassis leakage cur- any associated interlocks (e.g., stop flow, turn off
rent to ground with the grounding conductor of heater) or alarms at this time.
plug-connected equipment temporarily opened.
(Be sure that connections at the inlet or outlet 2.9 Blood Pump Occlusion. In order to operate cor-
ports or conductive casters on a conductive floor rectly, the pump rollers must occlude the tubing
do not establish alternate ground paths.) Oper- throughout its travel across the backplate.
ate the device in all normal modes, including on, Check tube occlusion with a section of tubing
standby, and off, and record the maximum leak- installed in the pump and filled with water to a
age current. If the unit has heating and cooling height of about 76 cm (30 in) above the pump.
modes, be sure that thermostats permit each Leave the other end of the pump open and empty.
mode to operate while taking readings. Any drop in level should be less than 1 cm/min
or within the manufacturer’s specifications.
Measure chassis leakage current with all ac- Check occlusion at various roller positions on the
cessories normally powered from the same line back plate.
cord connected and turned on and off. This in-
cludes other equipment that is plugged into the 2.10 Blood Pumps. Check the rollers on each pump to
primary device’s accessory receptacles, as well as ensure that they are running smoothly and that
equipment plugged into a multiple-outlet strip there are no unusual noises from the bearings or
(“Waber strip”) so that all are grounded through other indications of excessive bearing wear. If the
a single line or extension cord. manufacturer provides torque specifications for
the pump, check this with torque measuring tools.
Chassis leakage current should not exceed
300 µA. With correct-size tubing in the pump, im-
merse both ends of the tubing in a tank of saline
2.3 Pressure Monitors/Transducers. Perform the solution or water at atmospheric pressure, and
blood pressure monitor (Procedure/Checklist turn on the pump. For greater accuracy, attach
434) and pressure transducer (Procedure/Check- a cannula to the outflow side of the pump to
list 435) inspection and preventive maintenance simulate back pressure. To check the pump ac-
procedures on the respective components. Use curacy at a mid-range flow setting, set it to
separate inspection forms, but record the sys- deliver 3 L/min, and collect the volume for a
tem’s pass/fail determination on the heart-lung convenient time interval in a graduated cylinder
bypass units inspection form. (a fluid flowmeter may also be used). Also check
operation at low and high flow settings. At
2.4 Thermometer Accuracy. To check the accuracy higher settings, it may be necessary to collect
of thermometers in heater/coolers or water mix- fluid in a large bucket and measure out volume
ers, connect the outflow of the heater or mixer to in the graduated cylinder. Flows should be accu-
the temperature-monitoring device. For heater/ rate to within 5% of the setting or the manufac-
coolers, connect the in-line temperature-moni- turer’s specifications.
toring device, allow the unit to stabilize for 15
min, and compare temperatures. When check- For centrifugal pumps, used on some units,
ing water mixers, connect the outflow of the operate with saline and measure flow rate by
temperature-monitoring device to a drain, and pumping saline from a “reservoir” into the
compare temperatures. Thermometers should graduated cylinder. Compare this flow rate with
agree within 1°C. Check at low, medium, and the electronically determined rate, and make
high points in the temperature range (29°, 34°, sure it is within 5%.
and 38°C). When checking blood pump flow on pumps
without direct flow setting indication, it may be
2.5 Temperature Alarms. For units incorporating useful to draw a graph of flow setting versus dial
high-temperature alarms, keep the tempera- setting and placard it on the pump. Be sure to
ture-monitoring device where it was for the pre- indicate tubing size and brand on the graph.
vious test. For heater/coolers, place hot water in
the reservoir, and record the alarm value. For 2.11 Oxygen Flowmeter. Check the accuracy of the
mixers, alter the water mixture, and record the flowmeter by connecting it in series with the cali-
alarm value. Alarms should occur at 42° ±1°C or brated flowmeter. Set it to deliver a known flow,
within manufacturer’s specifications. Examine and compare this flow to that of the calibrated
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
meter. Check low, medium, and high ranges. The 3.2 Lubricate casters and motors.
valve should turn smoothly, with only slight drag,
and the float should rise and fall freely as the flow 3.3 Calibrate if required.
is raised or lowered. Accuracy of the machine
flowmeters should agree within 5% of full scale or 4. Acceptance tests
the manufacturer’s specifications. Also check other
flowmeters (e.g., CO2), if so equipped.
Conduct major inspection tests for this procedure
2.12 Temperature Monitors. Check the accuracy of and the appropriate tests in the General Devices Pro-
all probes with the temperature monitor. Test cedure/Checklist 438.
the accuracy of thermometers in a water bath
of known temperature or with a patient probe It may be useful to indicate with luminous tape or
simulator. Accuracy should be checked at paint the direction that the hand crank should be
20°C, 37°C, and 39°C. Check thermometers turned for normal pump rotation in the event of power
intended for wide temperature range applica- failure.
tion (e.g., hypothermia monitoring) at tem-
peratures near the high and low extremes of
the range. Thermometers should be accurate
Before returning to use
within 0.5°C or within the manufacturer’s Ensure that controls are set at normal positions and
specifications. It may be necessary to allow for that alarm volumes (if adjustable) are set loud enough
errors in the measuring system. to be heard in the clinical setting. Place a Caution tag
in a prominent position so that the next user will be
3. Preventive maintenance careful to verify control settings, setup, and function
3.1 Clean the exterior. before using the unit.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 431-0595
Heated Humidifiers
Used For:
Humidifiers, Heated [12-050]
Commonly Used In: Respiratory care area, critical care areas, recovery rooms, nurseries, operating rooms
Scope: Applies to servo-controlled units, units used in combination with separate temperature controllers
(servo control), and non-servo-controlled units
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview heated wet surface; efficient design ensures saturation
of the gas mixture leaving the humidifier. The gas
During normal inspiration, the mouth, nose, and cools as it flows to the patient, producing rainout
pharynx warm and humidify air. However, during (condensation), and is inspired saturated and at a
long-term ventilatory support or anesthesia when reduced temperature.
the patient is intubated with an oral or nasal tra-
cheal tube or tracheostomy tube, this natural hu- The simplest units heat water by means of a thermo-
midification process is bypassed; dry, cool gases are statically controlled heat transfer surface in contact
delivered directly to the trachea and lungs, thus with a body of water, which in turn heats the gas
increasing heat and moisture demand on the lower stream. Controlling the temperature of the heater
respiratory tract. As water is vaporized to increase prevents excessive water and gas temperatures. Most
inspired water vapor concentration and the inspired units have a control for varying the gas temperature;
gas is warmed by convection, tracheal mucosa loses servo-controlled units use a temperature sensor in the
heat and moisture. As the mucosa dries and its patient circuit for more reliable temperature control of
temperature drops, secretions thicken and ciliary the gas delivery to the patient.
activity is reduced, and the ability to clear mucus
and debris is diminished. The formation of thick
mucus plugs can result in atelectasis (i.e., collapse There is a risk of hyperthermia and respiratory
of the alveoli) or obstruction of the airway. tract burns if the inspired gas exceeds 40°C for an
extended period of time. Increases in temperature and
Using an artificial means to heat and humidify exposure time correspondingly increase this risk.
inspired gases minimizes the complications associated Thus, we recommend monitoring inspiratory air tem-
with artificial airways. Usually, an electrically perature during every heated humidifier application,
heated, water-filled humidifier is applied to the inspi- and we prefer units that regulate the temperature by
ratory gas line. The humidifier simultaneously sup- means of a patient circuit probe, rather than reading
plies heat and humidity when the gas passes over a water or heater surface temperature.
009073 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
431-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Citations from Health Devices and indicator, and the alarm capabilities. Also deter-
mine whether any special inspection or preventive
Heated humidifiers [Evaluation], 1987 Jul; 16:223-50. maintenance procedures or frequencies are recom-
Heated humidifiers can burn infants during CPAP mended by the manufacturer. Test the humidifier,
[Hazard], 1987 Dec; 16:404. temperature monitor, and alarm together.
Heated wires can melt disposable breathing circuits 1. Qualitative tests
[Hazard], 1989 May; 18:174. 1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condi-
Test apparatus and supplies tion. Check that plastic housings are intact with
Thermometer (bimetallic or electronic) accurate to no cracks or poor seals that spilled fluid can
at least 0.5°C over a range of 30° to 45°C penetrate, that necessary assembly hardware is
T-adapter for positioning a thermometer in series present and tight, and that there are no signs of
with the patient inspiratory temperature sensor of spilled liquids or other serious abuse. Check for
the humidifier discoloration, peeling, melted plastic, or swelling
that may indicate overheating.
Leakage current meter or electrical safety analyzer
1.2 Mount/Fasteners. Examine the mounting secu-
Ground resistance ohmmeter
rity of the humidifier and associated accessories.
Source of medical compressed air or oxygen capable
of providing a flow rate of approximately 10 L/min 1.4 AC Plug. Examine the AC power plug for signs
of damage. Attempt to wiggle the blades to de-
Distilled water for filling the humidifier termine that they are secure. Shake the plug
Patient circuit or tubing for use with the humidifier and listen for rattles that could indicate loose
Pressure gauges or meters with ranges of 0 to 30 cm screws. If any damage is suspected, open the
H2O and 0 to 100 cm H2O (such as those provided plug and inspect it.
by a pneumatic tester) with adapters for various 1.5 Line Cord. Inspect the line cord for signs of
humidifiers to be inspected (acceptance testing only) damage. If damaged, either replace the entire
Large syringe or sphygmomanometer bulb and cord or, if damage is near one end, cut out the
adapter that can be connected to the humidifier defective portion. Be sure to wire the new power
input for pressurizing it to 30 cm H2O (acceptance cord or plug with the same polarity as the old
testing only) one. Ensure that the line cord is sufficiently long
to preclude the need for extension cords.
Special precautions 1.6 Strain Reliefs. Examine the strain reliefs at
When inspecting heated humidifiers (and other both ends of the line cord. Be sure that they hold
thermostatically controlled equipment), verify that the the cord securely.
unit is not operating on its backup or secondary
thermostat. If the normal (primary) thermostat fails 1.7 Circuit Breaker/Fuse. If the unit has a switch-
in the on condition, the secondary thermostat will limit type circuit breaker, check that it moves freely. If
the temperature to protect the heater from burning the unit is protected by an external fuse, check its
out, but the heater may still generate a temperature value and type against that marked on the chassis,
excessive for the patient. Thus, if output temperature and ensure that a spare fuse is provided. If there
is high and the control thermostat does not appear to is no provision for a spare fuse, consider installing
adjust it properly, the unit may be operating on its a simple spring clip or old fuse holder. If the unit
backup thermostat. Most units do not have an alarm has a separate fuse for the heated circuit, be sure
to alert the user to this condition. to check it (its type and rating are critical).
CAUTION: Heater surfaces may be hot. 1.8 Tubes/Hoses. Check the condition of all tubing
and hoses in the unit. Be sure that they are not
Procedure cracked, kinked, brittle, or dirty. Check for any
evidence of leaking.
Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and 1.9 Cables. Inspect the controller and temperature
service manuals; be sure that you understand how to sensor cables, if any, as well as their strain reliefs,
operate the equipment, the significance of each control for general condition. Check reusable heated
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Heated Humidifiers
wires for cracks, kinks, and brittleness. Verify 1.22 Labeling. Check that all necessary placards, la-
that the wires are compatible with this unit. bels, flow rate and temperature calibration
charts, and instruction cards are present and
1.10 Fittings/Connectors. Examine all gas and liq- legible.
uid fittings and connectors (e.g., patient circuit,
water supply, electrical cable connectors) for 1.23 Accessories. Confirm the presence and condition
general condition. of such accessories as separate controllers, tem-
perature sensors, and water supplies. Make
1.11 Transducers/Temperature Sensor. Check that sure all necessary parts are present (e.g., valve
the patient inspiratory temperature sensor is flaps, removable stoppers).
present and properly fitted into the center of its
adapter for use in the patient circuit. 1.24 Flow/Output. With distilled water in the humi-
difier, connect it to a source of medical com-
1.13 Controls/Switches. Before moving any controls pressed air and its output to the patient circuit
and alarm limits, check their positions. If any of tubing. Set the unit for a mid-range temperature
them appear inordinate (e.g., temperature con- and the gas source for 10 L/min, and turn on the
trol at maximum, alarm limits at the ends of humidifier and gas source. Confirm that the gas
their range), consider the possibility of inappro- flow in a bubble-type unit actually bubbles up
priate clinical use or of incipient device failure. through the water. Also check that gas is being
Record the settings of those controls that should humidified after the unit has warmed up, as
be returned to their original positions following evidenced by condensation in the output hose.
the inspection. (During major procedures, perform Items 2.1
and 2.2 before this test, so that it will be possible
Examine all controls and switches for physical
to proceed directly to 2.10 after this test.)
condition, secure mounting, and correct motion.
Where a control should operate against fixed-
limit stops, check for proper alignment, as well
2. Quantitative tests
as positive stopping. Check membrane switches Perform the following tests (except Item 2.1) with
for membrane damage (e.g., from fingernails, distilled water added to the unit before applying power
pens). During the course of the inspection, be to the heater.
sure to check that each control and switch per-
forms its proper function. 2.1 Grounding Resistance. Measure and record the
resistance between the grounding pin of the
1.14 Heater. Examine the heater or heat transfer power cord and all exposed metal on the unit
surface for physical condition (e.g., corrosion or (including heater sheath or surface) except
pitting of its sheath, deteriorated insulation). small external trim pieces. Tug and flex both
ends of the line cord and any connected acces-
1.16 Fluid Levels. Check that the maximum fluid
sory cords while making the measurement. We
level is marked and clearly visible.
recommend that the resistance not exceed 0.5 Ω.
1.18 Indicators/Displays. During the course of the Grounding resistance and leakage current
inspection, confirm the operation of all lights, measurements are not required if the unit is
indicators, and visual displays. If the unit has a constructed primarily of plastic and has no ex-
digital temperature display, be sure that all its posed metal surfaces.
segments function.
2.2 Leakage Current. Measure chassis leakage cur-
1.20 Alarms. Operate the unit in such a way as to rent with the grounding connection temporarily
activate audible and visual alarms. High-tempera- opened. Obtain measurements with the unit off
ture alarms may need to be checked during Item and on and with the unit on and the heater cycle
2.11. If the unit has a probe-disconnect alarm, on and off, and record the maximum leakage
verify that it is activated and that the heater is current. Leakage current should not exceed
turned off when the probe is disconnected. 300 µA. (Since only water vapor and condensate
reach the patient through the inspiratory hose,
1.21 Audible Signals. Operate the unit to activate special measurements of leakage current from
any audible signals. Confirm appropriate vol- the water reservoir are not required. However, if
ume, as well as the operation of a volume control, the water supply is readily accessible for leakage
if so equipped. current measurement, this will provide further
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
assurance of heater insulation integrity, espe- 3. Preventive maintenance
cially if the sheath or heater surface is not of a
grounded design.) 3.1 Clean the exterior and heat transfer surface with
a damp cloth. (Be sure that the heat transfer
surface is cool.)
2.3 Low-Temperature Alarms. Verify the functions
and the accuracy of low-temperature alarms and 4. Acceptance tests
indicators. Some units alarm if they detect
Conduct major inspection tests for this procedure
room-temperature gas (although this may not
and the appropriate tests in the General Devices Pro-
occur until after several minutes of operation on
cedure/Checklist 438. In addition, perform the follow-
some units); other units have a user-selectable
ing tests.
low-temperature alarm.
4.1 Pressure Drop. With a T-adapter in the humidi-
2.10 Output Temperature. Connect the humidifier fier input, connect the 0 to 10 cm H2O pressure
input to a medical compressed-air source and the gauge or meter to measure the input pressure to
output to the patient circuit or tubing. Attach the the unit. Measure the pressure drop with 10
test thermometer adapters and the humidifier’s L/min gas flow exhausting to the atmosphere.
temperature sensor at the patient Y as close to The pressure drop should be less than 5 cm H2O
each other as the adapters will permit. for bubble-type humidifiers and much less for
other units. (This measurement can be per-
formed while the humidifier is warming up for
Set the temperature controller to low or mid the output temperature tests.) This test need not
range (35° to 40°C), set the gas source for 10 be performed on units that use disposable hu-
L/min, and turn on the humidifier and the gas midity chambers or units that allow complete
source. When the thermometer equilibrates, visual inspection of the flow path, since the ab-
record the output temperature and the tem- sence of any constriction can be verified.
perature indicated by the unit’s temperature
monitor or controller. Also, record the control- 4.2 Leaks. Attach the syringe or sphygmomanome-
ler or thermostat setting. Repeat the test at the ter bulb and 0 to 100 cm H2O pressure gauge or
maximum temperature setting. Verify that meter to the input and the output to seal the
the output temperature changes when the set- humidifier. Pressurize it to 30 cm H2O and ob-
ting is changed to maximum. If it does not, the serve the pressure drop over 1 min. The pres-
primary temperature control may not be func- sure drop multiplied by the unit’s internal
tioning, and the unit may be operating on its compliance (specified by the manufacturer)
backup thermostat. should not exceed 6 mL. For example, if the
unit’s internal compliance is 0.4 mL/cm H2O and
the pressure drop over 1 min is 10 cm H2O, the
Temperature monitor and temperature settings
leakage is 4 mL and within the 6 mL limit.
(if so equipped) should be accurate within 1°C for
servo-controlled units (other units are not cali- To determine nonspecified internal compli-
brated). The maximum temperature of any unit ance, occlude one end of the humidifier, inject 50
should not be higher than that specified by the mL of air through the open humidifier port with
manufacturer. (We believe that the maximum a syringe, and measure the increase in pressure
obtainable temperature should not exceed 40°C. in cm H2O. The internal compliance equals 50
However, many units are capable of delivering mL divided by the pressure increase. Record this
gases at considerably higher temperatures.) value for future use.
2.11 High-Temperature Alarms. Using the same Before returning to use
setup as in 2.10, verify that the high-tempera- Adjust the temperature setting to minimum or nor-
ture alarm activates whenever the output gas mal. Empty or remove the water reservoir. If the unit
temperature exceeds the alarm set point by more is equipped with an adjustable alarm volume, ensure
than 1°C. If the unit has an adjustable high-tem- that the volume is appropriate for a clinical setting.
perature alarm, verify alarm function at a low Return the unit for processing (e.g., cleaning, steriliz-
and high alarm setting. ing) to prepare it for patient use.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 413-0595
Hemodialysis Units
Used For:
Dialysate Delivery Systems, Multipatient [11-211]
Dialysate Delivery Systems, Single-Patient [11-213]
Hemodialysis Units [11-218]
Also Called: Dialysis machines, dialysis units, artificial kidney machines, hemodialyzers (which more appro-
priately applies to the dialyzer component of the machine)
Commonly Used In: Hemodialysis departments, critical care units, freestanding hemodialysis treatment
centers, patient homes
Scope: Primarily applies to single-patient hemodialysis units, although portions may be applied to central
hemodialysis systems; also see Peritoneal Dialysis Units Procedure/Checklist 455
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval* By Hospital Time Required
Major 12 months months . hours
Minor 3 months months . hours
* Temperature, conductivity, and pH (if applicable) monitors should be checked by the operator before each
dialysis.
Overview blood, or a special single-needle access catheter. Hepa-
rin is infused into the arterial (inflow) side of the blood
Hemodialysis is used to remove accumulated waste circuit to prevent clotting.
products, organic salts, and water from the blood of a
patient with impaired kidney function or to remove Blood pressure sensors on the venous side of the
toxins in cases of blood poisoning. Hemodialysis units dialyzer (and sometimes also on the arterial side) may
consist of an extracorporeal blood delivery unit (blood alarm and stop the blood pump when pressure is
circuit), a dialysate delivery unit (dialysate circuit), a outside preset limits. Most units have an air-bubble
dialyzer, and monitoring units. and/or foam detector or blood-level detector, which
clamps the venous blood line and stops the blood pump
Blood circuit. In the blood circuit, blood is taken if air is detected in the venous line to prevent infusing
from an artery, circulated through the dialyzer by a air emboli into the patient. Newer units may combine
blood pump, cleansed, and returned to a vein. Usually, air-bubble, foam, and blood-level detectors in one
one or two needles inserted in an arteriovenous (A-V) monitor unit.
fistula (the linking of an artery and vein) in the pa-
tient’s arm provide access to the circulatory system. Dialyzer. In the dialyzer, a semipermeable mem-
The single-needle technique halves the number of brane separates the blood from the dialysate solution.
punctures but requires either a Y connection and a Substances from the blood pass through the membrane
controller to alternate withdrawal and infusion of into the dialysate solution by diffusion, ultrafiltration,
009068 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
413-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
and osmosis. The dialysate solution initially contains Citations from Health Devices
none of the waste substances to be removed from the
blood. The resulting concentration gradients across Single-patient hemodialysis machines [Evaluation],
the membrane promote selective diffusion from the blood 1980 Feb-Mar; 9:87-130.
to the dialysate solution. Substances that should remain
Update: Gambro dialysis unit, 1980 Apr; 9:162.
in the blood are present in equivalent concentrations in
the dialysate solution. The dialysate solution has a lower Reusing dialyzers and tubing sets: Pros and cons, 1980
hydrostatic pressure than the blood to promote removal Nov; 10:22-4.
of excess water from the blood by ultrafiltration.
Improper dialysate [Hazard], 1983 Oct; 12:315-8.
Dialysate circuit. Dialysate solution, a mixture of
treated (purified) water and concentrated dialysate, is Electrical safety of subclavian catheters used in
pumped through the dialyzer at a prescribed tempera- hemodialysis, 1983 Nov; 13:18-20.
ture, concentration, and flow rate. Dialysate solution is Peritoneal dialysis compared with hemodialysis, 1986
prepared continuously in some machines by a propor- Feb-Mar; 15:34-5.
tioning system that meters and mixes precise propor-
tions of concentrated dialysate and treated water (a Hemodialysis water purification [User Experience
common ratio is 1 part dialysate to 34 parts water). This NetworkTM], 1988 Aug; 17:247.
proportioning system may be a fixed ratio (i.e., propor-
tioning a known volume of concentrate and water) or may Cobe Centry 2 and Centry 2Rx hemodialysis units
be servocontrolled, using a control sensor to regulate the [Hazard], 1988 Oct; 17:313-4.
flow of dialysate concentrate. A built-in conductivity Air embolism associated with hemodialysis [Hazard],
meter continuously monitors the solution before it 1989 Nov; 18:406-7.
reaches the dialyzer. Newer machines may have special
proportioning and monitoring systems for different types Technical overview: Hemodialysis machines, 1991
of dialysate (e.g., variable bicarbonate, variable sodium). Jun; 20:187.
The dialysate solution for other machines is prepared
by the simple “batch” method, but enough solution for the
Test apparatus and supplies
entire procedure must be mixed before the start of dialy- Ground resistance ohmmeter
sis. Portable conductivity meters are used to check batch Leakage current meter
mixtures of dialysate solution. The formulation of the
dialysate solution is prescribed by the physician and may Thermometer accurate to at least 0.1°C over a range
be varied to meet each patient’s needs. of at least 30° to 45°C; a temperature monitoring
device made of a thermometer sealed into one leg of
The dialysate circuit may be housed in a single-pa- a Y or T connector may also be used (similar fixtures
tient unit or divided between a central unit and a are used for hypothermia unit testing, although a
number of bedside stations. A central unit may allow separate fixture should be used for dialysis testing
the bedside apparatus to be smaller and less costly to avoid possible contamination)
than single-patient units. However, a central unit Stopwatch or watch with a second hand
does not permit individual prescription of dialysate
solution concentration. Syringe of the type used in the heparin pump
Syringe (at least 30 cc) to generate pressure of 300
Depending on the unit used, monitoring devices in
mm Hg
the dialysate circuit may sense dialysate temperature,
conductivity, flow rate, negative pressure, ultrafiltra- Pressure gauge or meter capable of reading vacuum
tion rate, and blood circuit leaks. Some monitors and and pressure over a range of about -600 to +400 mm
alarms include fail-safe controls that interrupt the Hg; accuracy should be at least 5 mm Hg over the
dialysis procedure to prevent injury. -100 to +100 mm Hg range and 5% over the remain-
der; necessary range depends on type of hemodia-
For more detailed information on dialysis, consult lysis unit being inspected
the Health Devices citations, particularly the 1980
evaluation of hemodialysis machines and the improper Graduated cylinder with a 1,000 mL capacity for
dialysate hazard, as well as Review of Hemodialysis for checking flowmeter and blood pump
Nurses and Dialysis Personnel (Gutch CF, Stoner MH, Conductivity meter, accurate to at least 1% or stand-
Corea AL. 5th ed. St. Louis, MO: C.V. Mosby, 1993). ard solution to check concentration monitor
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Hemodialysis Units
Expendable supplies for the device being inspected, Some components covered by the following proce-
including isolators or fluid barriers for pressure dure (e.g., blood pump) are not built into certain older
gauges or meters, blood lines, syringes, clamps, dia- models of dialysis machines but are accessories that
lyzers, and dialysate solution (some of these supplies must be supplied by the user. Note the serial numbers
are expensive; to reduce costs, a single set of expend- of these components on the inspection form.
able supplies can be used repeatedly for inspections,
except for units dedicated for isolation patients or that Record the time elapsed indicated on the hour me-
are suspected of having been used on patients with ter, if so equipped. This will help indicate appropriate-
hepatitis or AIDS; expendables used with such units ness of preventive maintenance frequency and what
should be properly disposed of after use) preventive maintenance procedures to do.
Assorted fittings for connecting tubing and gauges 1. Qualitative tests
Vacuum cleaner 1.1 Chassis/Housing. Examine the exterior of the
pH meter or standard test solutions if unit under unit for cleanliness and general physical condi-
test has pH monitor tion. Be sure that plastic housings are intact,
that all assembly hardware is present and tight,
Special precautions and that there are no signs of spilled liquids or
other serious abuse. Dialysate has a high salt
For some hemodialysis units, especially the more
concentration that will corrode and tarnish.
sophisticated ones, it will be impossible to perform
quantitative checks on all monitoring and alarm cir- 1.2 Mount. If the device is mounted on a stand or
cuits. Refer to the service manual for suggestions when cart, examine the condition of the mount. If it is
the procedures described below cannot be carried out attached to a wall or rests on a shelf, check the
in a straightforward manner. security of this attachment.
Dialysis-grade water should be used for all inspec- 1.3 Casters/Brakes. If the device moves on casters,
tion and preventive maintenance procedures. check their condition. Look for accumulations of
lint and thread around the casters, and be sure
CAUTION: For protection against HBV and HIV,
that they turn and swivel, as appropriate. Check
wear rubber gloves, a long-sleeved gown, and safety
the operation of brakes and swivel locks, if the
glasses or goggles when disassembling or testing dialy-
unit is so equipped.
sis units. Contact the infection control practitioner
responsible for the hemodialysis unit to review insti- 1.4 AC Plug/Receptacles. Examine the AC power
tutional policies and procedures regarding protection plug for damage from abuse. Attempt to wiggle
from HIV and HBV. Treat machines as though they the blades to determine that they are secure.
were contaminated, and consider maintaining sepa- Shake the plug and listen for rattles that could
rate, dedicated tool sets for servicing. To minimize the indicate loose screws. If any damage is sus-
chance of oral contamination, do not eat or smoke in pected, open the plug and inspect it.
the test area. (For more information on infection con-
trol during IPM activities, see the article in this binder Hospital Grade plugs are strongly recom-
titled “IPM Safety.”) mended for hemodialysis units. Base selection of
plugs on their resistance to fluid infiltration;
Since there may be water on the floor of mainte- Hospital Grade plugs molded onto the line cord
nance areas, consider using ground fault circuit inter- might be considered.
rupters for electric shock protection in areas where this
equipment will be tested and serviced. If the device has electrical receptacles for ac-
cessories, insert an AC plug into each and check
Procedure that it is held firmly. If accessories are frequently
plugged and unplugged, consider a full inspection
Before beginning an inspection, carefully read this of the receptacle. Check for corrosion.
procedure and the manufacturer’s instruction and
service manuals; be sure that you understand how to 1.5 Line Cord. Inspect the cord for signs of damage.
operate the equipment, the significance of each control If damaged, replace the entire cord or, if the
and indicator, and the alarm capabilities. Also deter- damage is near one end, cut out the defective
mine whether any special inspection or preventive portion. Be sure to wire a new power cord or plug
maintenance procedures or frequencies are recom- with the same polarity as the old one. Also check
mended by the manufacturer. line cords of battery chargers.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
1.6 Strain Reliefs. Examine the strain reliefs at them appear inordinate (e.g., a conductivity or
both ends of the line cord. Be sure that they hold flow control at maximum, alarm limits at the
the cord securely. ends of their range), consider the possibility of
inappropriate clinical use or incipient device fail-
1.7 Circuit Breaker/Fuse. If the device has a ure. Record the settings of those controls that
switch-type circuit breaker, check that it moves should be returned to their original positions
freely. If the device is protected by an external following the inspection.
fuse, check its value and type against that
marked on the chassis and ensure that a spare Examine all controls and switches for physical
is provided. condition, secure mounting, and correct motion.
1.8 Tubes/Hoses. It may be necessary to disassem- Where a control should operate against fixed-
ble the unit to examine all tubing and connectors limit stops, check for proper alignment, as well
to ensure that they fit correctly. The tubing as positive stopping. Check membrane switches
should not be kinked or mounted near rotating for membrane damage (e.g., from fingernails,
components, sharp edges, and fastener ends. If pens). During the course of the inspection, check
deaerators are used, check them for proper fluid that each control and switch performs its proper
levels and venting. Check that all seals, grom- function.
mets, gaskets, and couplings are in good condi-
1.14 Heater. Examine the heater for physical condi-
tion and are correctly installed. Tubing and fluid
tion (e.g., corrosion of its sheath, deteriorated
connectors should not show signs of aging, fa-
insulation). Operate it to ensure that its controls
tigue, or stress (e.g., discoloration, cracks);
function properly (e.g., that a variable tempera-
should not contain foreign material; and should
ture control does, in fact, determine the amount
not leak. Look for signs of leaks (e.g., corrosion
of heating; that on/off controls work).
or dried dialysate near a connector). Make re-
pairs if any of the above defects are present.
1.15 Motor/Pump/Fan. Check all pumps (e.g., dia-
Ensure that all fluid path components are se-
lysate, recirculating, drain, proportioning, blood,
curely mounted to the unit.
heparin) for proper operation. Make sure they
1.9 Cables. Inspect the cables (e.g., sensor) and deliver fluid properly and are not excessively hot
their strain reliefs for general condition. Exam- to the touch while operating. Motors should have
ine cables carefully to detect breaks in the insu- smooth and free-running bearings and should not
lation and to ensure that they are gripped be excessively noisy. Check for leaks around pump
securely in the connectors at each end to prevent seals and coupling, and make sure that pump
rotation or other strain. heads and motors are clean. Clean and lubricate
pumps, fans, motors, and other moving parts ac-
1.10 Fittings/Connectors. Examine all gas and liq- cording to manufacturer’s recommendations, and
uid fittings and connectors, as well as all electri- note this on Lines 3.1 and 3.2 of the form.
cal cable connectors, for general condition.
Electrical contact pins or surfaces should be On batch-type units, make sure the drain
straight, clean, and bright. Color-coded or spe- screen of the dialysate delivery pump is intact
cial connectors may be used to avoid inappropri- and clean. Replace it if damaged.
ate connections (e.g., a “bicarbonate” dialysate
concentrate to a “sodium” concentrate circuit). 1.16 Fluid Levels. Check all fluid levels. Test the
Verify that these safeguards have not been ig- water-loss alarm by momentarily turning off the
nored or violated by the use of adapters. water while the unit is running.
1.11 Transducers. Confirm that any necessary 1.17 Battery. Inspect the physical condition of batter-
transducers are on hand, and check their physi- ies and battery connectors, if readily accessible.
cal condition. Check operation of battery-operated power-loss
1.12 Filters. Check the condition of all liquid and gas alarms, if so equipped. The power-loss alarm
(air) filters. Clean or replace and indicate this on should sound if the plug is pulled out during
Line 3.1 or 3.4 of the inspection form. operation or when the unit is off and is then
turned on. Check power-loss alarm batteries.
1.13 Controls/Switches. Before moving any controls When it is necessary to replace a battery, label
and alarm limits, check their positions. If any of it with the date.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Hemodialysis Units
1.18 Indicators/Displays. During the course of the 2.2 Leakage Current. Measure chassis and patient
inspection, confirm the operation of all lights, lead leakage current to ground with the ground-
indicators, flowmeters, temperature/pressure ing conductor temporarily opened. Operate the
gauges or meters, and visual displays or indica- device in all normal modes, including on,
tors on the unit and charger, if so equipped. standby, and off, and record the maximum leak-
Ensure that all segments of any digital displays age current. Obtain a reading with the heater
function. cycled on and with it cycled off. Chassis leakage
current should not exceed 300 µA.
1.20 Alarms/Interlocks. Operate the device in such
a way as to activate each audible and visual Measure chassis leakage current with all ac-
alarm. Check that any associated interlocks cessories normally powered from the same line
function. If the device has an alarm-silence fea- cord connected and turned on and off. This in-
ture, check that it silences the alarm only for the cludes other equipment that is plugged into the
period of time specified by the manufacturer. primary device’s accessory receptacles, as well as
equipment plugged into a multiple-outlet strip
Verify that venous line clamps apply enough (“Waber strip”) so that all are grounded through
force to completely occlude the line. a single line or extension cord.
1.21 Audible Signals. Operate the device to activate Hemodialysis is sometimes performed
all audible signals. Confirm appropriate volume, through a subclavian catheter. Ideally, any
as well as the operation of a volume control. hemodialysis machine connected to a subclavian
catheter should have an isolated patient connec-
1.22 Labeling. Check that all necessary placards, la- tion due to the risk of microshock from accidental
bels, conversion charts, and instruction cards migration of the catheter tip into the heart.
are present and legible. However, most units are not designed for this
application; thus, we have not included a test of
1.23 Accessories. Verify that an emergency hand
fluid path isolation. For subclavian hemodia-
crank for the blood pump is supplied with the unit.
lysis, we recommend using hemodialysis units
1.24 Deaeration. It is difficult to quantitatively assess with leakage current levels below 50 µA or modi-
deaeration ability in dialysis machines. One of fied units with redundant grounding or an isola-
the primary components of the deaeration system tion transformer.
is the deaeration (vacuum) pump; deterioration of
2.3 Air/Foam (Blood-Level) Detector. Check this de-
its performance can adversely affect deaeration.
tector for proper operation. Ensure that all visual
To check vacuum pumps used in deaeration sys-
and audible alarm indicators operate properly.
tems, we suggest measuring the vacuum gener-
Clean sensors according to manufacturer’s recom-
ated by the pump with a pressure gauge or meter.
mendations, and follow the suggested test proce-
Consult the manufacturer for the best measur-
dure. Other interlocked functions (e.g., venous
ing point and acceptable vacuum levels or for
line clamp, shutoffs, bypasses) should operate
other recommended tests.
properly when an alarm is indicated. Check sen-
sitivity based on manufacturer’s information, and
2. Quantitative Tests verify proper operating range. If the unit has an
alarm-test switch, check that it works correctly,
2.1 Grounding Resistance. Using an ohmmeter, but be aware that it does not test the sensor.
electrical safety analyzer, or multimeter with
good resolution of fractional ohms, measure and Some blood-level, air, or foam detectors may
record the resistance between the grounding pin require opaque fluid in the lines in order to
of the power cord and exposed (unpainted and not function. Check the manufacturer’s recommen-
anodized) metal on the chassis. Verify that a low dations for testing these units.
resistance exists from the ground pin to various
points on the unit, including all accessory mod- 2.4 Blood-Leak Detector. Check this detector for
ules, to ensure that interconnections are ade- proper operation. Ensure that all visual and audi-
quate. We recommend a maximum of 0.5 Ω. ble alarm indicators operate properly. Clean sen-
sors according to manufacturer’s recommen-
If the device has an accessory outlet, check its dations, and follow the suggested test procedure.
grounding to the main power cord. Other interlocked functions (e.g., venous line
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
clamp, shutoffs, bypasses) should operate prop- perature, and compare alarm temperatures
erly when an alarm is indicated. Check sensitiv- with the manufacturer’s specifications. (On
ity based on manufacturer’s information, and units where this cannot be done, it may be
verify proper operating range. If the unit has an possible to test temperature alarms qualita-
alarm-test switch, check that it works correctly, tively by infusing a bolus of hot or cold water
but be aware that it does not test the sensor. into the dialysate line.) Verify proper function
of high-temperature indicators and any other
On some units, the blood-leak alarm can be
interlocked function (e.g., dialysate bypass).
tested by injecting air or milk past the photocell
Return the temperature control to the normal
detector. Check the manufacturer’s recommen-
operating temperature.
dations for testing these units.
2.6 Conductivity.
2.5 Temperature.
Accuracy. Set the temperature to 37°C on units CAUTION: Incorrect dialysate conductivity
with a temperature control. Set the flow rate may be fatal (see Health Devices 1983 Oct; 12:315).
to 500 mL/min or according to manufacturer’s Accuracy. Examine and clean the conductivity
recommendations. Record the reading of the probe, and ensure that the monitor is
unit’s temperature indicator and that indi- mounted correctly according to the manufac-
cated by the precision thermometer (actual turer’s recommendations.
temperature) after the unit equilibrates. On Although conductivity readings can be most
units with a coil dialyzer, measure the tem- accurately verified by laboratory tests, this is
perature of the dialysate in the canister. For inconvenient on a routine basis. Comparison
units with parallel-flow or hollow-fiber capil- to a conductivity meter or standard solutions
lary dialyzers, connect the temperature moni- is an acceptable alternative. The conductivity
toring device to the dialysate line at the meter used for this test should have an accu-
entrance to the dialyzer (a T connection allows racy of at least 1% and should be checked
dialysate to keep flowing during the measure- frequently against a standard solution. Moni-
ment). tors are calibrated in milliequivalents/L of
When the heaters are initially turned on, chloride (although they measure total ionic
the temperature in some units may overshoot concentration), percent deviation, or mil-
the desired setting and trigger a high-tem- liohms/cm. If the unit is calibrated in percent
perature alarm. Allow 15 min for temperature deviation, be aware that this corresponds to
stabilization. Remember that dialysate cools only one concentration of dialysate. If physi-
between the heater and the dialyzer; some cians at your hospital prescribe other concen-
units may compensate for this cooling by in- trations, check for appropriate deviation
creasing the temperature of the dialysate in readings.
the unit above the set temperature. The tem- While the unit is running at normal oper-
perature control and/or indicator should be ating temperature, use the manufacturer’s
accurate within 0.5°C or within the manufac- recommended method to take samples. Be
turer’s specifications. sure to flush the conductivity meter several
Alarms. Keep the precision thermometer in the times with the solution to be tested before
same position as it was for the previous test. taking readings, and take the average con-
Test low-temperature alarms by turning the ductivity of three samples. If the conductiv-
heaters off and allowing the dialysate to cool ity monitor error is greater than the
or by adjusting the limits to cause an alarm. manufacturer’s specification, verify that it is
Record the temperature at which the alarm not due to temperature effects before adjust-
occurs. Verify the operation of the low-tem- ing the conductivity meter. A fill line
perature alarm and any other interlocked should be marked on the batch tank. If not,
functions. establish the line and mark it on the tank.
Test the high-temperature alarm functions Alarms. Verify that low- and high-conductivity
by setting the temperature control to a value alarm indicators function properly. See the in-
higher than the alarm limits or by the over- struction or service manual on how to conduct
shoot when the heaters are initially turned on this test, or test the high-conductivity alarm by
(see Accuracy). Record the actual alarm tem- infusing a bolus of dialysate into the water line
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Hemodialysis Units
and test the low alarms by disconnecting the rect size tubing in the pump, immerse both ends
dialysate supply. Verify that all other inter- of the tubing in a tank of saline solution or water
locked alarms function properly. and start the pump. Check the accuracy of the
pump at a mid-range flow rate by setting it to
2.7 Blood Circuit Pressure. deliver 200 to 250 mL/min and collecting the
Monitor. Check the accuracy of blood circuit volume in a 1,000 mL graduated cylinder for a
pressure monitors by connecting an accurate specified interval. Also check operation at low
pressure gauge or meter and the existing pres- and high flow settings. Flows should be accurate
sure monitor to a T or Y connector (see Sphyg- to within 10% or the manufacturer’s specifica-
momanometers Procedure/Checklist 424). tions.
Connect the sphygmomanometer bulb to the
remaining port of the connector, increase the On pumps without direct reading of flow rate,
pressure, and read the pressure on both the it may be useful to draw a graph of flow rate
monitor and the test gauge or meter. The moni- versus dial setting and placard it on the pump.
tor should be tested at three different pres- Indicate tubing size and brand on the graph.
sures to ensure that it is accurate over the
entire range. The monitor should be accurate Ensure that an emergency hand crank is at-
within 10 mm Hg or 10% of the reading, which- tached to the unit. Disconnect the power and
ever is greater, or within manufacturer’s speci- verify that the hand crank will turn the pump.
fications. If there is more than one monitor,
repeat the test for the other monitors. 2.11 Dialysate Flow Rate. Check that all markings
are legible. Check the accuracy of the flowmeter
Alarms. With the pressure gauge or meter still by setting it to deliver a known flow rate
connected, verify that the appropriate audible (vol/min) and collect the dialysate flow via the
and visual alarms function when the low and drain line in a 1,000 mL graduated cylinder for
high blood pressure alarm limits are reached. a specified period. Machines with fixed flow
Confirm that other interlocked functions op- rates or single-pass converters may be checked
erate properly. Record the values at which similarly. Check dialysate flow rate at low (mini-
the alarms occur, and check that they are mum), medium, and high (maximum) flow set-
within the manufacturer’s specifications. tings. Flowmeter accuracy should be within 10%
or within the manufacturer’s specifications.
2.8 Heparin Pump. Check heparin pump accuracy
with a saline-, water-, or heparin-filled syringe 2.12 Negative Pressure.
of the type actually used with the unit. Set the
pump to a rate typical of actual use, and operate Monitor. Check the negative pressure monitor at
it for a measured time interval. Calculate the low, medium, or high levels with a vacuum
delivery rate from the syringe graduations. Ac- gauge or pressure meter and a Y or T connector
curacy should be within 10%. Check that the (some units have a sampling port in the dia-
pump alarms and turns off when the plunger lysate line that can be used). The reading
reaches the end of its travel. should be accurate within 10 mm Hg or within
the manufacturer’s specifications. Refer to the
2.9 Blood Pump Occlusion. Check tube occlusion by
manufacturer’s manual to determine where to
connecting a T fitting to the outflow end of the
place the gauge or meter for this test. The
tubing. On one side of the T connect a pressure
position of the gauge or meter relative to the
gauge or meter. Occlude the tubing segment
dialyzer is important, since elevation errors
with one roller of the pump, and pressurize the
are approximately 20 mm Hg/ft. To prevent
tubing to 300 mm Hg with a syringe attached to
contamination, use a standard transducer
the remaining port of the T or Y fitting. Any drop
protector (isolator) when making these meas-
in pressure should be within the manufacturer’s
urements.
specifications. Repeat this procedure for the
other roller.
Alarms. Verify that the appropriate audible and
2.10 Blood Pump Flow Rate. Check rollers to make visual alarms function when the dialysate
sure that they function smoothly and that there pressure exceeds the preset high and low lim-
are no unusual noises from the bearings or other its. Verify that other interlocked functions
indications of excessive bearing wear. With cor- operate properly.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
2.13 Additional Features. Test additional features 3.2 Lubricate where appropriate. Lubricate motor
(e.g., ultrafiltration [UFR], variable sodium and and pump heads according to the manufac-
bicarbonate features, pH meters, single-needle turer’s specifications.
controllers) according to the manufacturer’s
specifications. If quantitative testing of UFR me- 3.4 Replace any tubing segments or other items ac-
ters is not possible, confirm that they are func- cording to the manufacturer’s recommendations.
tioning. Testing of the ultrafiltration control is Replace lights if necessary.
essential for high-flux machines. Test the pH
monitor in a manner similar to Item 2.6. The 4. Acceptance tests
variable sodium and bicarbonate features may Conduct major inspection tests for this procedure
be inconvenient to test, but both of these parame- and the appropriate tests in the General Devices Pro-
ters of prepared dialysate may be compared to cedure/Checklist 438.
values obtained by a laboratory blood gas/elec-
trolyte analyzer. (Use reverse side of inspection Before returning to use
form to record test results.)
Disinfect the device as recommended by the manu-
3. Preventive maintenance facturer. Make sure controls are set at normal posi-
tions and alarm volumes, if adjustable, are set loud
3.1 Clean the exterior and interior of the unit. Vac- enough to be heard in the clinical use area.
uum air vents and cooling fans, if so equipped.
Clean or replace fan filters. Clean flowmeters, if Place a Caution tag in a prominent position so that
required, according to the manufacturer’s in- the next user will be careful to verify control settings,
structions. setup, and function before use.
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 465-0595
Ho:YAG Surgical Lasers
Used For:
Lasers, Surgical, Holmium:YAG [16-943]
Also Called: Ho:YAG lasers, YAG lasers (incorrectly), holmium lasers, surgical lasers, arthroscopic lasers,
urology lasers, angioplasty lasers, thulium:YAG lasers, orthopedic lasers
Commonly Used In: Operating rooms, short procedure areas, cystoscopy rooms, catheterization labora-
tories, endoscopy laboratories, orthopedic operating rooms
Scope: Applies to general-purpose holmium:YAG surgical lasers that include contact and/or noncontact
flexible fiberoptic delivery systems (either reusable or disposable), emit near-infrared energy at 2,100 nm, and
can provide sufficient power output to coagulate and vaporize tissue; applies to low- and high-power
holmium:YAG surgical lasers that are typically used for general surgery, orthopedic surgery, urology, cardio-
vascular surgery, gastroenterology, bronchopulmonary, neurosurgery, gynecology, and ENT surgery proce-
dures; does not apply to holmium:YAG lasers used solely for ophthalmic surgery; also does not apply to other
ophthalmic lasers or to CO2 lasers, Nd:YAG lasers, argon lasers, or other surgical lasers; however, many of
the tests listed herein can be used or modified for these other lasers
Risk Level: ECRI-recommended, High; Hospital assessment,
ECRI-Recommended Interval
Type Interval Used By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview density to cause vaporization and/or coagulation. The
2,100 nm, mid-infrared Ho:YAG energy is preferen-
Ho:YAG lasers are normally checked before each use tially absorbed by water and is typically absorbed
by the laser’s power-on self-test and by user examina- within 0.5 mm of the tissue surface. Ho:YAG surgical
tion of the aiming beam and the delivery system to be laser fibers are most often used in contact with or close
used. This minimizes the need for frequent additional to tissue to cause vaporization. Moving the fiber tip
periodic testing. Manufacturers or outside service ven- away from the tissue lowers the power density, causing
dors often maintain lasers for hospitals. The extent less tissue to be vaporized and allowing some coagula-
and frequency of inspection by hospital personnel tion effect.
should be coordinated with these outside services.
Failure of a Ho:YAG surgical laser can cause patient In addition, Ho:YAG lasers emit a train of energy
or staff injury, abrupt interruption of a surgical proce- pulses; both the energy per pulse and pulse rate are
dure, or damage to the laser system. These lasers must user settable. Cutting hard tissue may require high
be meticulously maintained to ensure proper and safe energy per pulse, while a smooth cut may require a fast
operation. pulse rate. However, the range of energy per pulse and
the number of pulse rate combinations are limited by
Ho:YAG surgical lasers affect tissue by delivering the laser’s power capability. The output power of the
invisible, mid-infrared energy at a sufficient power laser is the product of the energy per pulse times the
232619 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
465-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
pulse rate — for example, 0.5 J × 10 Hz and 1.0 J × 5 beam pattern introduced by an accessory would be
Hz are both 5 watts. A 5-watt laser may allow both of apparent by examining the visible aiming beam.
these settings, but not 1.0 J and 10 Hz, which would
require a 10-watt laser. This differs from most other Citations from Health Devices
lasers, which deliver a range of power through a vari-
able energy and fixed pulse rate that is faster than Laser use and safety [Guidance article], 1992 Sep;
Ho:YAG’s. 21:306-10.
General-purpose Ho:YAG surgical lasers have a la- Ho:YAG surgical lasers [Evaluation], 1995 Mar; 24:92-
ser cavity that houses an yttrium-aluminum-garnet 122.
(YAG) crystalline rod doped with holmium (Ho). (In
most Ho:YAG lasers, the YAG crystal is also doped Test apparatus and supplies
with thulium [Tm] and chromium [Cr], which improve
Leakage current meter or electrical safety analyzer
the laser’s efficiency.) Energy leaving the laser tube
through a partially reflecting mirror is typically di- Ground resistance ohmmeter
rected into a flexible optical fiber that transmits the New, unused fiber delivery system
laser energy to the tissue. The fiber may be used with
additional devices (e.g., through an endoscope), with Black Delrin block 1⁄2″ or more thick, 1″ or more wide,
special tips, and/or with a laser handpiece or a laser about 3″ to 4″ long; tongue depressors; or firebrick
micromanipulator (used to interface the laser with the Laser radiometer (power meter)
surgical microscope). These attachments can be used
to focus the energy into a small spot size at a known Laser safety signs
working distance and or a specific beam direction to Laser safety eyewear specifically designed for use
accomplish a special task (e.g., focused energy emis- with Ho:YAG surgical lasers and of sufficient optical
sion at a right angle to the fiber for sclerostomy). density to protect the wearer’s eye from laser injury
Because the mid-infrared energy emitted by the Vise with padded jaws or ring stand with padded
Ho:YAG laser is invisible, a second, nontherapeutic clamp
aiming helium-neon (He-Ne) laser or laser diode,
Pressure gauges and coolant system tee fitting
which emits visible light (typically red), simultane-
ously traverses the fiber and is coincident (i.e., travels Outlet test fixture (optional)
the same path) with the Ho:YAG laser beam. Insulating gloves, high voltage (optional)
Like most lasers, Ho:YAG lasers are inefficient in Grounding strap (optional)
converting electrical energy into laser energy. As a
result, excess heat is generated in the laser cavity,
requiring a cooling system. Most Ho:YAG lasers use
Special precautions
water/air cooling systems that are self-contained, con- Inspecting and maintaining lasers is a dangerous as
nected to a freestanding chiller system, or connected well as necessary process, and far greater care is
to a water supply and drain. required than with most devices. Personnel who in-
spect or service lasers should receive special training
With Ho:YAG lasers, unlike those lasers that use from the manufacturer or from a qualified alternative
mirror delivery systems (e.g., articulating arms on CO2 training source.
lasers), it is not necessary to periodically verify coinci-
dence of the aiming and therapeutic beam or to assess Laser energy can cause serious injury, particularly
the therapeutic beam pattern (e.g., TEM00) within the when the internal interlock is overridden or in any
beam or spot. Since the therapeutic and aiming laser other situation in which the energy does not diverge
beams are transmitted through a single optical fiber, significantly over long distances. Under some circum-
these two beams are coincident as they exit the fiber. stances, the beam may not diverge significantly, even
Any beam pattern distortion at the fiber entrance a full room length or more away from the laser (and
would be eliminated as the laser beams travel through can harm tissue or burn material even at this dis-
the fiber because of internal reflections within the tance). Therefore, exercise great care whenever a laser
fiber. Misalignment of the beam at the fiber entrance beam is accessible. Area security and use of personnel
would result in decreased power output or loss or protective devices and practices should be consistent
distortion of the aiming beam. In a well-aligned sys- with hospitalwide laser safety procedures and/or
tem, any significant problem with the therapeutic should be approved by the laser safety committee.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Ho:YAG Surgical Lasers
In addition, windows should be covered with nonre- enter the laser cabinet. When possible, disconnect the
flective material to prevent transmission of laser en- laser from line voltage before entering the laser cabi-
ergy to other areas. net, and use insulated gloves for those procedures in
which contact with a high-voltage source is possible
Users should wear appropriate laser safety eyewear (and the gloves are not otherwise contraindicated).
at all times whenever the laser is in the Operating Ensure that equipment intended to be used to meas-
mode. WARNING: Laser safety eyewear does not pro- ure, drain, or insulate high voltages carries the appro-
tect the wearer from the aiming system light. Do not priate insulation rating (e.g., above 20 kV).
stare directly into the aiming system beam or the thera-
peutic laser, even when wearing laser safety eyewear. Where possible, perform tests with the unit turned
Avoid placing the laser beam path at eye level (i.e., off. Because of the presence of high voltage, perform
when kneeling, sitting, or standing). the Grounding Resistance test (Item 2.1) before any
other test that requires operation of the laser.
Do not perform these procedures when a patient is
present or clinical staff is working, and do not aim the Report any laser accident immediately to the laser
laser across a path that a person might normally use safety officer or equivalent, as well as to the hospital
as a thoroughfare. Furthermore, at minimum, post risk manager.
doors to the room with appropriate laser safety signs
stating that the laser is in use and that it is unsafe to Procedure
enter the room without authorization by the service Before beginning the inspection, carefully read this
person performing the procedure. A second person procedure and the manufacturer’s operator instruc-
should be present, especially during procedures of rec- tions and service manual; be sure that you understand
ognized risk, to summon help in case of an accident. how to operate the equipment, the significance of each
control and indicator, and precautions needed to en-
The laser should remain in the Off position when
sure safety and avoid equipment damage. Also, deter-
not in use. When in use, it should be in the
mine whether any special inspection or preventive
Standby/Disabled mode. Do not switch it to the Oper-
maintenance procedures or frequencies are recom-
ating mode until the procedure is about to begin and
mended by the manufacturer.
the laser and its delivery system are properly posi-
tioned. If the procedure must be interrupted, discon-
1. Qualitative tests
nect the laser from line voltage, and remove the laser
operation key and store it in a controlled location. 1.1 Chassis/Housing.
Do not use the laser in the presence of flammable General. Verify that the key has not been left in
anesthetics or other volatile substances or materials the laser. (Remove it if it has been, and inform
(e.g., alcohol), or in oxygen-enriched atmospheres, be- users of the importance of storing the key in a
cause of the serious risk of explosion and fire. Remove controlled location.) Examine the exterior of
from the working area or cover with flame-resistant the unit for cleanliness and general physical
opaque material all reflective surfaces likely to be condition. Be sure that all housings are intact
contacted by the laser beam. Whenever possible, use a and properly aligned, that assembly hard-
firebrick or other nonflammable material behind the ware is present and tight, that any retractable
target material (e.g., black Delrin) when the laser is to parts slide easily and lock in place if so con-
be activated. Target materials will ignite when ex- structed, that there are no signs of spilled
posed to high laser energies; use short durations when liquids or other evidence of abuse, and that
practical. A CO2 fire extinguisher should be readily there are no obvious signs of water or oil
available. leakage.
Shutters. If manual shutters for the aiming sys-
Some surgical lasers use high voltages (e.g., 20 kV), tem or the therapeutic laser are accessible,
which can be lethal. Capacitors may store charges long ensure that they operate smoothly and cor-
after the device has been disconnected from line volt- rectly. Be sure to leave the shutter in the
age. Consult the manufacturer’s recommended proce- proper position for normal operation.
dures for servicing high-voltage laser circuits, and
avoid contact with any portion of the high-voltage 1.2 Mounts/Holders. Check that mounts or holders
circuit until you are certain that the charge has been intended to secure the fiber to the fiber support
drained. In such cases, a good ground must be present; (to protect the fiber when in use) are present, in
preferably, use a redundant ground strap if you must good working order, and being used. Similarly,
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
check mounts or holders for other devices Electrical contacts should be straight, clean, and
(e.g., external power meters, footswitch). bright.
If the device is mounted on a stand or a cart, There should be no visible dirt or residue in
examine the condition of the mount. Verify that the optical path of the laser aperture. Ensure
the mounting apparatus is secure and that all that any mechanism to close off the laser aper-
hardware is firmly in place. ture (fiber port) is clean, operates smoothly, and
1.3 Casters/Brakes. Check that the casters roll and is in use.
swivel freely. Check the operation of brakes and
1.12 Filters. Check the condition of all liquid and air
swivel locks.
filters. Some Ho:YAG surgical lasers require
1.4 AC Plug/Receptacle. Examine the AC power deionized water, and most require special filtra-
plug for damage. Wiggle the blades to deter- tion. Measuring the pressure drop across a liquid
mine whether they are secure. Shake the plug, filter can be helpful in determining whether the
and listen for rattles that could indicate loose filter should be replaced. Clean or replace filters
screws. If you suspect damage, open the plug according to the manufacturer’s recommenda-
and inspect it. tions (e.g., replace if the pressure drop is >5 psi),
and indicate this in the preventive maintenance
1.5 Line Cords. Inspect line cords for signs of dam- section of the inspection form. Clean or replace
age. If a cord is damaged, replace the entire cord air filters and radiators that are obviously dirty.
or, if the damage is near one end, cut out the
defective portion. Be sure to wire a new power 1.13 Controls/Switches.
cord or plug with the correct polarity.
General. Before moving any controls, check and
1.6 Strain Reliefs. Examine the strain reliefs at record their positions. If any position appears
both ends of the line cord. Be sure that they grip inordinate, consider the possibility of inappro-
the cord securely. priate use or of incipient device failure. Exam-
1.7 Circuit Breakers/Fuses. If the device has a ine all controls and switches for physical
switch-type circuit breaker, check that it moves condition, secure mounting, and correct mo-
freely. If the device is protected by an external tion. If a control has fixed-limit stops, check
fuse(s), check its value and type against what is for proper alignment as well as positive stop-
marked on the chassis or noted in the instruction ping. Check membrane switches for tape resi-
or service manual. Ensure that a spare is pro- due and for membrane damage (e.g., from
vided or readily available. fingernails, pens, surgical instruments). If
you find such evidence, notify users to avoid
1.8 Tubes/Hoses. Check the condition of all cooling- using tape and sharp instruments. During the
system hoses and any other hoses or tubing the inspection, be sure that each control and
laser may have (e.g., drain). Check that they are switch works properly.
of the correct type; that they have not become
cracked and do not show other signs of significant Remote. Examine the exterior of the control for
abuse; that they are connected correctly and po- cleanliness and general physical condition. Be
sitioned so that they will not leak, kink, trail on sure that housings are intact, that assembly
the floor, or be caught in moving parts; and that hardware is present and tight, and that there
they are secured adequately to any connectors. are no signs of spilled liquids or other serious
1.9 Cables. Inspect all cables and their channels or abuse. If the remote control is attached by
strain reliefs for general physical condition. Ex- cable to the laser, ensure that the cable and
amine cables carefully to detect breaks in insu- any connectors are in good condition. Examine
lation and to ensure that they are gripped all controls and switches for general physical
securely in the connectors at each end to prevent condition, secure mounting, correct motion,
strain on the cable. and intended range of settings. Where a con-
trol should operate against fixed-limit stops,
1.10 Fittings/Connectors. Examine all optical (e.g., check for proper alignment as well as positive
fiber), liquid, and electrical fittings and connec- stopping. During the course of the inspection,
tors for general physical condition. Liquid fit- be sure to check that each control and switch
tings should be tight and should not leak. performs properly.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Ho:YAG Surgical Lasers
Footswitch. Examine the footswitch for general If primary and remote-control indicators and
physical condition, including evidence of displays can be used at the same time or if control
spilled liquids. Footswitches for lasers include can be switched from one to the other during the
an internal switch that activates according to course of a procedure, verify that the same infor-
the depth of pedal depression. It is usually mation (e.g., settings, displays) is indicated on
possible to feel the vibration caused by closure both control panels during laser operation.
of the switch, even through a shoe. Check that
the internal switch is operating and that the If display screens or digital displays are pro-
footswitch does not stick in the On position. vided for user prompts or for viewing accumu-
Some footswitches include two internal lated information (e.g., pulse or accumulated
switches; in this case, verify the operation of energy counter), ensure that each display pro-
both. vides the information expected. Ensure that user
prompts occur in the proper sequence. Store
During the procedure, check to be sure that some sample information, and verify that it is
the laser activates consistently when the foot- correct. If a feature to manually reset this infor-
switch is depressed. Flex the cable at the mation is available, ensure that it works.
entry to the switch, and using an ohmmeter,
check for internal wire breaks that cause in- 1.19 Laser Delivery System Calibration. Some hol-
termittent operation. Confirm that strain re- mium:YAG surgical lasers include a user-acces-
liefs are secure. sible calibration port or power meter that allows
output calibration and/or testing of the laser
Examine the male and female connectors fiber. This feature is provided because transmis-
for attaching the footswitch to the laser cabi- sion of laser energy through a fiber may change
net to be sure that no pins are bent and that as a result of fiber use. Based on the measure-
no other damage is present. Ensure that the ment from the calibration power meter, the laser
connector secures acceptably to the laser may automatically recalibrate itself and/or ad-
cabinet. just the displays so that the power indicated to
1.15 Motors/Pumps/Fans/Compressors. Check the be delivered to the patient will be correct, or it
physical condition and proper operation of these may require the user to do this manually. Verify
components, if present. If lubrication is required, that this feature is functioning by using the
note this in the preventive maintenance section manufacturer’s recommended calibration proce-
of the inspection form. Clean any obvious dust dure to test one delivery system (e.g., fiber, hand-
from these components. piece) that the manufacturer indicates can be
acceptably calibrated using these procedures. A
1.16 Fluid Levels. Check all fluid (e.g., coolant) lev- good-quality (e.g., >85% transmissibility, un-
els. Refill or change the fluid according to the damaged sheath) fiber or handpiece should be
manufacturer’s recommendations, and note this used for this test.
in the preventive maintenance section of the
inspection form. 1.20 Alarms/Interlocks. Operate the device in a
manner that will activate the self-check feature,
1.17 Battery. Inspect the physical condition of batter- if present, and verify that all visual and audible
ies and battery connectors, if readily accessible. alarms activate according to the manufacturer’s
If a remote control or display is battery powered, documentation. If no self-check feature is pre-
check or replace the battery (periodic prophylac- sent, operate the laser in a manner that will
tic battery replacement is often preferred to risk- activate each audible and visual alarm; be sure
ing battery failure during use). When it is to test only those alarms that will not cause
necessary to replace a battery, label it with the damage to the laser or present an unnecessary
date. risk of laser beam exposure to yourself or by-
standers.
1.18 Indicators/Displays. During the course of the
inspection, verify proper operation of all lights, If a door or window interlock is used, ensure
indicators, meters, gauges, and visual displays that it deactivates the laser properly. (Do not
on the unit and remote control. Ensure that all disassemble major parts of the laser to test in-
segments of a digital display function. Note any ternal interlocks.) After deactivating the laser
error messages displayed during the power-on and reclosing the door or window, check to be
self-test. sure that the laser will restart. Be sure to check
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
the interlocks in all locations where the laser is Handpieces. Examine each handpiece compo-
used. (For some lasers, the function of the inter- nent (e.g., body, tips, lenses) for cleanliness
locks can be checked using an ohmmeter.) and general physical condition. Examine indi-
vidually only those components that are in-
If the laser is equipped with an emergency tended for removal during normal use and
“kill” switch, test this feature to be sure that it storage. (Do not remove other parts that are
deactivates the laser and that the laser will press-fit or attached by screws, bolts, or snap-
subsequently restart. rings.) If lenses are detachable, be sure not to
1.21 Audible Signals. Operate the device to activate touch the lens surface; handle lenses by the
any audible signals (e.g., laser emission, setting edges only. Consult the manufacturer’s rec-
change). Check for proper operation, and verify ommendations for the procedures and clean-
that the signal can be heard in the environment ing agents to use to clean lenses.
in which the laser will be used. Ensure that major subcomponents of the
handpiece, when assembled, are secure. En-
1.22 Labeling. Check that all placards, labels, and
sure that the mechanisms used to connect the
instruction cards noted during acceptance test-
handpiece(s) to the fiber are in good working
ing (see Item 4.3) are present and legible. Check
order and that they reliably secure each hand-
to see that an instruction manual is kept with
piece to the fiber.
the laser or is readily available.
Microscope micromanipulator. Examine the
1.23 Accessories. microscope micromanipulator for cleanli-
General. Verify that all necessary accessories ness and general physical condition. Be sure
are available and in good physical condition. to handle it by the main body; do not hold it
Set up reusable accessories with the laser to by the joystick, and do not touch the reflect-
ensure compatibility and proper functioning. ing surfaces or lenses in the body. Inspect
micromanipulators provided by both the la-
Checking all fibers or accessories during a ser manufacturer and the laser accessory
single inspection and preventive mainte- manufacturer.
nance procedure is unnecessary as long as
accessories are routinely checked by the per- Ensure that the reflecting surfaces and
son(s) responsible for laser setup and opera- lenses are intact and clean. Consult the
tion. In addition, many of the accessories are manufacturer’s recommendations for the pro-
sterile and require resterilization before use, cedures and cleaning agents to use to clean
making the laser potentially unavailable. Be reflecting surfaces and lenses.
sure to check with the person responsible for Examine the joystick to ensure that it is
scheduling the use of the laser before begin- firmly attached and that it freely moves the
ning the procedure. reflecting lens. If a finger rest is present,
Fibers. For the test fiber or before each use, ensure that it is firmly attached and properly
examine the connector, cable, and tip of each oriented.
fiber to be used, as well as the fiber support, If a zoom focus feature is present, be sure
for cleanliness and general physical condi- that it turns easily and does not slip. Examine
tion. Be sure that all hardware (e.g., coolant each objective lens to ensure that it is intact
channels) is present, in good condition, and and clean. Do not touch the lens surface. Con-
firmly attached. Ensure that the connector sult the manufacturer’s recommendations for
properly seats into the laser aperture of the the procedures and cleaning agents to use to
laser cabinet. Examine the distal end of fibers clean the objective lenses. Carefully insert
to ensure that any connecting mechanisms each lens into the micromanipulator, and en-
(e.g., threads) are in proper working order. sure that it fits snugly.
If a fiber appears to be dirty or damaged, Inspect the mechanism used to attach the
remove it from service. If a fiber is reusable, micromanipulator to the microscope to ensure
notify the person(s) responsible for fiber re- that all parts are present and that it is in good
pair. The fiber should be repaired and/or working order. Connect the micromanipula-
cleaned according to the manufacturer’s rec- tor to the microscope to check for a secure
ommendations. Verify fiber performance. connection.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Ho:YAG Surgical Lasers
Safety filters. Verify operation of safety filters However, if the laser power meter does not meas-
in the microscope and endoscope delivery ure pulse duration, use the following less prefer-
systems. able alternative.
1.24 Aiming Beam. Activate the aiming beam (with- Place and secure the laser fiber, handpiece, or
out the therapeutic beam), and verify that it micromanipulator with the aiming system fo-
produces a round, uniformly bright spot, with no cused on the target material (e.g., black Delrin
halo. For handpieces that provide adjustable or a tongue depressor). With the laser set to
spot sizes, verify that the spot size changes as about 10 W and the exposure set at minimum
expected and still remains uniform. Check that duration, activate the laser and create a burn.
the intensity control, if present, does change the Carefully move the target material to expose a
brightness of the aiming beam. Similarly, check clean area, maintaining the same distance. Ad-
pulsing controls to verify that the aiming beam just the exposure setting in increments of 0.1 sec
can be pulsed. If several color choices are avail- or the next longest duration, and activate the
able for the aiming beam, verify that each color laser at each setting. Continue this process until
is present and working properly. you have tested all exposure settings, except
continuous, and have developed a series of
1.25 Laser Aperture.
burns. Compare the burns to verify that progres-
WARNING: Make this inspection with the la- sively larger burns occurred as the exposure
ser powered off. Remove and inspect the protec- duration increased.
tive window (e.g., blast shield) behind the laser
aperture. It should be clean and undamaged; 2.4 Repeat Pulse. If the unit includes a Repeat Pulse
clean or replace if needed. There should be no feature, which repeats the pulse at a fixed or
visible dirt or residue in the optical path of the adjustable rate, test this feature with the laser
laser aperture. set at the minimum, median, and maximum
repeat pulse settings, if adjustable. Some laser
2. Quantitative tests power meters can react quickly enough to be
used to test this feature of the laser. If you are
2.1 Grounding Resistance. Use an ohmmeter, elec- using such a power meter, test the laser to be
trical safety analyzer, or multimeter with good sure that the correct power is repeatedly deliv-
resolution of fractional ohms to measure and ered over the correct time period.
record the resistance between the grounding pin
on the power cord and exposed (unpainted and If your laser power meter cannot be used for
not anodized) metal on the chassis, accessory this test, use the following alternative test
outlet, ground pins, and footswitch. We recom- method. Set the laser to about 10 W and a 0.1 sec
mend a maximum of 0.5 Ω. (If the footswitch is exposure duration with the fiber, handpiece, or
of low voltage, grounding is not required.) micromanipulator attached, and verify that the
repeat pulse feature operates as expected by
2.2 Leakage Current.
moving the target material slightly between
WARNING: Do not reverse power conductors each pulse. Be extremely careful to keep hands
for this or any other test. Improper attachment of out of the laser beam path. If the number or
conductors may damage the laser. duration between repeat pulses is adjustable,
test that setting changes made throughout the
With the laser attached to a grounded power- range result in the expected performance.
distribution system, measure the leakage cur-
rent between the chassis and ground with the 2.5 Footswitch Exposure Control. Set the output
unit grounded and ungrounded. The leakage cur- time for about 5 sec, activate the unit, and
rent on the chassis should not exceed 300 µA; in release the footswitch after about 1 sec. Verify
no case should it exceed 500 µA. Where it is that the beam turns off when the footswitch is
greater than 300 µA, ensure that appropriate released.
grounding is present.
2.6 Pulse Rate. This test can be done in conjunction
2.3 Exposure Duration. Some laser power meters with power output measurements with some
can measure pulse duration. If the power meter power meters. Should your power meter be inca-
can react to pulse duration (this is the preferred pable of measuring pulse rates, output from a
circumstance), test the laser at each setting. high-speed IR photodiode circuit and oscilloscope
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
can be used to measure the number of pulses per 3. Preventive maintenance
second. Alternately, low-power illumination of
thermal paper in a chart recorder will create Verify that all daily preventive maintenance proce-
marks on the paper that can be compared to the dures recommended by the manufacturer are carried
laser pulse rate. out.
3.1 Clean the exterior. Clean accessible optical com-
With the laser set at minimum and maximum ponents (e.g., blast shield, microscope lenses), if
pulse rates and at one mid-range setting between necessary, using techniques and cleaning solu-
the minimum and maximum pulse rates, activate tions recommended by the manufacturer.
the laser at its minimum power setting for a
sufficient period to acquire acceptable readings. 3.2 Lubricate any motor, pump, fan, compressor, or
Compare the reading with the pulse rate display printer components as recommended by the
of the laser; the measured and displayed values manufacturer.
should all be within 10% of one another. In addi-
3.3 Calibrate/adjust any components (e.g., printer)
tion, compare the reading obtained with the read-
according to the manufacturer’s recommenda-
ing taken on incoming acceptance testing, at the
tions. Only appropriately trained personnel
last preventive maintenance procedure, or after
should attempt laser adjustments. Ensure that
the last service procedure.
all hoses and tubes are tight.
2.10 Power Output. Select one delivery system (e.g., 3.4 Replace filters if needed. Check all fluid levels,
fiber, handpiece, micromanipulator), and per- and supplement or replace fluids if needed.
form the manufacturer’s recommended user cali-
bration procedure. Secure the delivery system at 4. Acceptance Tests
the appropriate distance from the detector of the
Conduct major inspection tests for this procedure
laser power meter to meet spot-size require-
and the appropriate tests in the General Devices Pro-
ments specified in the instructions for the meter.
cedure/Checklist 438.
(Do not focus the beam to a small spot on the
power meter. Some power meters require that WARNING: Lasers may be damaged by switching
the unfocused or a defocused laser beam be pro- between normal and reverse polarity while the device is
jected into the detector to cover the majority of on. If reverse-polarity leakage current measurements
the absorber surface. If the laser beam is focused are made, turn off the unit being tested before switching
on the detector, it may be damaged.) polarity. Also, lasers powered by three-phase electrical
systems may be damaged if proper electrical phase
WARNING: Accessing the unfocused laser connections are not made initially and maintained
beam may require defeating internal interlocks. thereafter. Thus, do not switch conductor connections
Because of the heightened risk associated with an or wiring configuration for any tests, including leakage
unfocused, nondiverging laser beam, exercise current measurement. Do not conduct electrical leakage
great care if the interlocks are to be defeated. current tests with reversed-polarity wiring.
With the laser set at low (e.g., 10% of full scale),
medium (e.g., 50% of full scale), and maximum Also test the ability of the laser to deliver laser
output, activate the laser for a sufficient period energy as expected in all configurations and with all
to acquire acceptable readings. (Power meters provided laser accessories. In addition, perform the
use different time constants to acquire an accept- following tests.
able reading, and you must know and meticu- 4.1 Areas of Use. Visit the area(s) in which the laser
lously follow the power meter’s instructions for is to be used, and ensure that laser signs,
use.) Compare the reading with the power dis- eyewear, and window coverings are available
play of the laser; the measured and displayed and being used and that safety interlocks for
values should all be within 10% of one another. doors or windows, if present, are functioning
In addition, compare the reading obtained with properly.
the reading taken on incoming acceptance test-
ing, at the last preventive maintenance proce- 4.2 Casters/Mounts/Holders. Ensure that the as-
dure, or after the last service procedure. If the sembly is stable and that the unit will not tip
laser includes a low-power (e.g., mW) feature, over when pushed or when a caster is jammed on
test it in a similar fashion with a power meter of an obstacle (e.g., a line cord, threshold), as may
appropriate resolution in the low-power range. occur during transport. If the device is designed
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Ho:YAG Surgical Lasers
to rest on a shelf, ensure that it has nonslip legs 4.7 Repeat Pulse. If the unit includes a Repeat Pulse
or supports. feature, test this feature as described in Item 2.4,
but over the full range of available settings.
4.3 Labeling. Examine the unit and note the pres-
ence, location, and content of all labels. Labeling 4.8 Power Range. Using the technique described
information is typically found in the laser’s op- in the Power Output test, test the power output
erator manual. accuracy at several low, medium, and high
settings.
4.4 Electrical Wiring Configuration. Ensure that
the branch circuits and the outlets for the laser 4.9 Laser Delivery System Calibration. Use the
are properly wired and rated for use with the manufacturer’s recommended calibration proce-
laser. Examine the receptacles at each location dure to test each new reusable delivery system
where the laser is to be used to ensure that the (e.g., fiber, handpiece) that the manufacturer
proper electrical configuration (e.g., proper neu- indicates can be acceptably calibrated using
tral and ground connections, proper phase rota- these procedures. Note the fiber transmission for
tion) has been installed. Connect the laser to each delivery system tested if this information is
each receptacle and confirm that the laser oper- provided by the laser. Or you can calculate it
ates properly, specifically confirming that mo- using the following formula:
tors are operating in the proper direction. Delivered power
% Transmission = × 100%
Power entering the fiber
4.5 AC Plug. Verify that the plug is acceptable for
Delivery systems with less than the manufac-
use with the maximum current and voltage
turer-recommended transmission (typically
specifications for operating the laser. (Consult
>80%) should be returned to the manufacturer.
National Electrical Manufacturers Association
[NEMA] configurations for general-purpose non-
locking and locking connectors if in doubt.)
Before returning to use
Be sure to return controls to their starting position,
4.6 Pulse Duration. Verify that progressive in- and place a Caution tag in a prominent position so that
creases in pulse duration throughout its range of the next user will be careful to verify control settings,
adjustment result in progressively larger burns. setup, and function before using the unit.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Procedure/Checklist 414-0595
Hypo/Hyperthermia Units
Used For:
Hyperthermia Units, Circulating-Fluid [17-648]
Hypothermia Units [12-078]
Hypo/Hyperthermia Units, Central [12-074]
Hypo/Hyperthermia Units, Mobile, General-Purpose [12-075]
Hypo/Hyperthermia Units, Mobile, Heart-Lung Bypass [17-206]
Also Called: Hypothermia units, hyperthermia units, heating pads, heater/cooler units
Commonly Used In: Special care units, operating rooms, general medical/surgical areas, emergency departments
Scope: Applies to mobile units that provide both heating and cooling; adaptable for devices that provide heat
only and for central hypo/hyperthermia units; does not apply to smaller circulating-fluid pump/heating pad units,
which should be inspected using Circulating-Fluid Pumps Procedure/Checklist 412
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
*Flush and refill reservoir, if necessary, at a six-month interval.
Overview Automatic (servo). The operator selects the desired
patient temperature. The machine senses the actual
Hypo/hyperthermia units are used primarily to raise patient temperature through a rectal, skin, or esopha-
the body temperature of victims of accidental hy- geal temperature probe and delivers heated or cooled
pothermia, maintain normal temperature (normother- fluid accordingly. The machine displays actual and
mia) in patients during and after surgery, lower the selected patient and fluid temperatures in this mode.
body temperature for certain surgical procedures, and (See Health Devices 1988 Nov; 17:320-46 for additional
lower and stabilize the body temperature of febrile information on applications and operation of hypo/
patients. The utility of hypo/hyperthermia units for hyperthermia units.)
some of these applications has been questioned.
Hypo/hyperthermia units are relatively complex
Hypo/hyperthermia units can typically operate in devices. They are among the heaviest and bulkiest
the following two modes: pieces of mobile hospital equipment and are often
subjected to rough handling. The water or antifreeze
Manual. The operator selects the temperature of solutions used in them can corrode interior parts if the
fluid to be delivered to the blanket for heating or units are treated carelessly. All too often, patients
cooling the patient. The selected and actual fluid tem- being heated or cooled by units that use an automatic
peratures are displayed. Some units also monitor control mode are not observed as carefully as those
patient temperature. whose temperature is being controlled manually.
009075 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
414-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Thus, accurate and reliable operation of hypo/ hyper- Such a device does not normally limit water tempera-
thermia units, particularly in the automatic mode, is ture to a clinically safe level, but it should not be
crucial. deactivated since unit damage can result.
Hypo/hyperthermia units have been implicated Some of the items in this procedure differ from most
in a number of cases of patient injury or death. other procedures in that they may require opening the
Investigation of these incidents reveals that some unit and temporarily modifying the wiring. We hesi-
could have been avoided with adequate inspection tate to recommend such wiring modifications as part
and maintenance. of a routine inspection procedure because unskilled
personnel may inadvertently damage the unit; how-
Citations from Health Devices ever, there is no other way to determine whether the
Hypo/hyperthermia machines and blankets [Evalu- backup thermostats are functional. Personnel respon-
ation], 1988 Nov; 17:320-46. sible for inspecting hypo/hyperthermia units who lack
the technical expertise to perform this test must rec-
Test apparatus and supplies ognize their own limitations and seek qualified help.
Performing the fluid temperature indicator test (Item
Ground resistance ohmmeter
2.10) after the high- and low-temperature protection
Leakage current meter or electrical safety analyzer tests (Items 2.3 and 2.4) will help ensure that the
Calibration thermometer, accurate to at least device has been correctly returned to its proper oper-
±0.3°C over the range of the hypo/hyperthermia ating condition.
unit’s electronic thermometer, and cups of hot and
cold water (a temperature probe simulator suitable Procedure
for use with the hypo/hyperthermia unit to be in- Before beginning an inspection, carefully read this
spected may be used instead of the thermometer and procedure and the manufacturer’s instruction and
the cups of water, but the water and the thermome- service manuals; be sure that you understand how to
ter will be required to check temperature probes) operate the equipment, the significance of each control
Temperature-monitoring device that consists of an and indicator, and the alarm capabilities. Also deter-
accurate dial thermometer to check the tempera- mine whether any special inspection or preventive
ture of the circulating fluid, some clear tubing, and maintenance procedures or frequencies are recom-
appropriate connectors for installing the device in mended by the manufacturer.
series with the blanket. (These devices, sometimes
1. Qualitative tests
referred to as shunt thermometers, are available
from some hypo/hyperthermia unit manufacturers, 1.1 Chassis/Housing. Examine the exterior of the
or they can be constructed; see User-constructed unit for overall condition. The chassis should be
Test Equipment behind the Test Equipment and clean and free of rust and corrosion. Exterior
Supplies Tab.) screws should be tight.
Hydrometer with scales suitable for the type of 1.2 Mount. If the unit is mounted on a stand or cart,
antifreeze used in the unit (required only if the unit examine the condition of the mount.
circulates an alcohol or ethylene glycol solution
through the blanket); inexpensive antifreeze testers 1.3 Casters/Brakes. If the unit moves on casters,
are available from automotive parts suppliers. check their condition. Look for accumulations of
lint and thread around the casters, and be sure
Short-circuited patient temperature probe plug (re-
that they turn and swivel, as appropriate. Check
quired only if the unit has an automatic control
the operation of brakes and swivel locks, if the
mode and circulates an alcohol or ethylene glycol
unit is so equipped.
solution through the blanket)
Cup of saline solution and strip of aluminum foil for 1.4 AC Plug. Examine the AC power plug for dam-
measuring probe leakage current (acceptance test- age. Attempt to wiggle the blades to determine
ing only) that they are secure. Shake the plug, and listen
for rattles that could indicate loose screws. If
Special precautions any damage is suspected, open the plug and
inspect it.
Some units have undertemperature and/or
overtemperature protection to avoid damage to the 1.5 Line Cord. Inspect the cord for signs of damage.
heating element compressor or other parts of the unit. If damaged, replace the entire cord or, if the
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Hypo/Hyperthermia Units
damage is near one end, cut out the defective function properly (e.g., that a variable tempera-
portion. Be sure to wire a new power cord or plug ture control does, in fact, determine the amount
with the correct polarity. of heating; that on/off controls function).
1.6 Strain Reliefs. Examine the strain reliefs at 1.15 Motor/Pump/Fan/Compressor. Check the
both ends of the line cord. Be sure that they hold physical condition, and verify proper operation
the cord securely. of these components. Lubricate them if re-
quired, and note this on Line 3.2 of the form
1.7 Circuit Breaker/Fuse. If the unit has a switch- (but do not check 3.2 until you have completed
type circuit breaker, check that it moves freely. all necessary lubrication).
If the unit is protected by an external fuse, check
its value and type (as well as those of any spares 1.16 Fluid Levels. Check the circulating fluid level in
provided) against that marked on the chassis. the reservoir with a blanket connected, and add
fluid as needed. Consult the operator’s manual
1.8 Tubes/Hoses. Check the condition of all tubing to determine the proper level. If fluid is needed,
and hoses. Be sure that they are not cracked, add distilled water or the manufacturer’s recom-
kinked, or dirty. mended alcohol-and-water or antifreeze-and-
1.10 Fittings/Connectors. Attach a blanket to each water mixture. If the unit uses distilled water,
pair of connectors on the unit to ensure that the add a disinfectant according to the manufac-
unit operates smoothly and does not leak. Exam- turer’s instructions. If it uses antifreeze, check
ine all fittings and connectors, as well as all its specific gravity with a hydrometer, with the
electrical cable connectors, for general condition. fluid at about room temperature.
Electrical contact pins or surfaces should be 1.18 Indicators/Displays. During the course of the
straight, clean, and bright. inspection, confirm the operation of all lights,
1.11 Probes. Confirm that patient temperature indicators, meters, gauges, and visual displays
probes are on hand, and check that they are on the unit and charger, if so equipped. Be sure
clean and are not cracked, brittle, or otherwise that all segments of a digital display function.
deteriorated. 1.20 Alarms. Operate the unit in such a way as to
1.12 Filters. Check the condition of the fluid filters, activate each audible and visual alarm. Check
if so equipped. Clean or replace them as needed, that any associated interlocks function. If the
and indicate this on Line 3.1 or 3.4 of the inspec- unit has an alarm-silence feature, check the
tion form. method of reset (e.g., manual or automatic)
against the manufacturer’s specifications. It will
1.13 Controls/Switches. Before moving any controls not be possible to check out all alarms at this
or alarm limits, check their positions. If any of time, since some of them require abnormal oper-
them appear inordinate (e.g., a temperature con- ating conditions that will be simulated later in
trol that is at the end of its range), consider the Items 2.3 and 2.4.
possibility of inappropriate clinical use or of in-
cipient device failure. Record the settings of 1.21 Audible Signals. Operate the unit to activate
those controls that should be returned to their any audible signals. Confirm appropriate vol-
original positions following the inspection. ume, as well as the operation of the volume
control, if so equipped.
Examine all controls and switches for physical
condition, secure mounting, and correct motion. 1.22 Labeling. Check that all necessary placards, la-
Where a control should operate against fixed- bels, conversion charts, and instruction cards
limit stops, check for proper alignment, as well are present and legible.
as positive stopping. Check membrane switches 1.23 Accessories.
for membrane damage (e.g., from fingernails or
pens). During the course of the inspection, be Blankets. Check each reusable blanket for leaks,
sure to check that each control and switch per- connector operation, and general cleanliness.
forms its proper function. Since blankets do not usually have serial
numbers on them and may be interchanged
1.14 Heater. Examine the heater for physical condi- between units, it is not possible to associate the
tion (e.g., corrosion of its sheath, deteriorated blanket inspection with any one unit. Never-
insulation). Operate it to verify that its controls theless, the hospital should know how many
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
reusable blankets it owns and should inspect the maximum reading of the temperature-moni-
each one regularly. Check for leaks with the toring device, and note any overheating or high-
blanket connected to an operating hypo/hy- temperature alarms. If the unit has a secondary
perthermia unit because this produces the backup device, bypass the primary high-tem-
highest pressure within the blanket tubing. perature backup and repeat the test. The maxi-
Blankets that pass inspection should be mum temperature(s) should agree with the
tagged “Inspected,” with the date and inspec- manufacturer’s specification for the primary
tor’s initials noted. Roll, rather than fold, (and secondary) backup device, but should not
stored blankets to prolong their life. exceed43°C.
2. Quantitative tests Caution: Remove any bypasses installed for
this test.
2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with Repeat the test with the patient temperature
good resolution of fractional ohms, measure and probe unplugged. The temperature should go no
record the resistance between the grounding pin higher than before; some units will indicate the
of the power cord and exposed (unpainted and failure with a Probe Open alarm, and the unit
not anodized) metal on the chassis. If a redun- will not operate.
dant ground is provided, either as a second plug 2.4 Low-Temperature Protection. This test is simi-
or an alligator clip, check its resistance to the lar to Item 2.3, except that it confirms the opera-
chassis. We recommend a maximum of 0.5 Ω. tion of the primary low-temperature backup (and
If the device has an accessory outlet, check its secondary backup, if present) and should be per-
grounding to the main power cord. formed only if the unit circulates alcohol or eth-
ylene glycol through the blanket and has an
2.2 Leakage Current. Measure the maximum leak- automatic control mode. Low-temperature
age current between the chassis and ground with backup cutoffs are intended to protect the pa-
the ground wire temporarily opened and any tient against excessive cooling if the tempera-
redundant ground removed. Check the follow- ture-control circuitry or probe fails. Before
ing operating modes with the grounding conduc- performing this test, obtain a schematic of the
tor interrupted: off, manual cooling, manual hypo/hyperthermia unit and determine whether
heating, and circulate only. Record the highest the unit has low-temperature backup protection
leakage current; it should not exceed 300 µA. (a thermostat or other cutoff).
2.3 High-Temperature Protection. This test con- Install a jumper across the main thermostat.
firms the operation of the high-temperature Check the service manual for information on how
backup (and secondary backup, if present) and to do this. Operate the hypo/hyperthermia unit
should be performed on all units regardless of in the automatic mode with a temperature-moni-
the type of circulating fluid. Identify the backup toring device connected in series with the input
thermostats or other devices. If the unit does not line to a blanket. Set the control temperature to
have an automatic mode, consult the manufac- its lowest value, and expose the patient tempera-
turer to determine how to test backup protection. ture probe to room air. The hypo/hyperthermia
If the unit has an automatic mode with two unit should cool the circulating fluid until it is
backup high-temperature cutoffs, check both. limited by the backup cutoff. Record the lowest
temperature indicated by the temperature-
Install a jumper across the thermostat; monitoring device, and note any alarms. If the
check the service manual for information on unit has a secondary low-temperature backup,
how to do this. Operate the hypo/hyperther- bypass the primary low-temperature backups
mia unit in the automatic mode with a tem- and repeat the test. The recorded temperature(s)
perature-monitoring device connected in series should agree with the manufacturer’s specifica-
with the input line to the blanket. Set the tion for the primary backup (and secondary
control temperature to room air, and expose backup) device (usually ≥1°C).
the patient temperature probe to a value above
room ambient temperature. The hypo/ hyper- Repeat the test with a shorted patient tem-
thermia unit should heat the circulating fluid perature probe plug substituted for the probe
until it is limited by the backup cutoff. Record itself. Observe the operation of a Probe Shorted
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Hypo/Hyperthermia Units
alarm, if so equipped. If the machine operates at cup of 41°C water used in the last test, and
all, the minimum fluid temperature should be operate the unit in the automatic mode with the
limited by the primary backup cutoff. temperature-monitoring device in the input line
to a blanket and the control point set to 37°C.
Caution: Remove any bypasses installed for The temperature of the circulating fluid should
this test. drop to the low level recorded in Item 2.10. Next,
2.10 Fluid Temperature Indicator. Operate the unit transfer the patient temperature probe to the
in the manual mode with the temperature-moni- cup of cooler water saved from the previous test
toring device in the input line to the blanket. (it is not necessary to recheck the temperature
Select the lowest blanket temperature setting, of that water), and observe both the temperature
and wait until the temperature stabilizes (this indicator and the Heat and Cool indicators (if so
should take 3 to 10 min). Record the setting of equipped) on the unit. Note the reading on the
the control knob, the reading of the fluid tem- patient temperature indicator when the unit
perature indicator, and the reading of the tem- switches from cooling to heating. It should be
perature-monitoring device; it should not drop within 0.5°C of the 37°C set-point temperature.
below 1°C. The first two should be within 1°C of If the unit lacks indicators for the heating and
the temperature-monitoring device. Repeat this cooling modes, listen for a change in sound as the
test with the manual control set at its highest cooling compressor stops. The circulating fluid
temperature; it should not exceed 43°C. temperature should equilibrate at the high value
recorded in Item 2.10. This test can also be
2.11 Patient Temperature Indicator and Probe. This performed using a patient temperature probe
test applies only to units with an automatic mode simulator, if available.
of operation. Fill a cup with tap water at about
30°C, as measured with the calibration ther- 3. Preventive maintenance
mometer. Be sure that the thermometer is im- 3.1 Clean the exterior, interior, and fluid filter, if
mersed to an adequate depth to provide an necessary. Remove dirt that has accumulated in
accurate reading. Place the calibration ther- vents and cooling fans within the unit with a
mometer and the unit’s patient temperature vacuum cleaner or compressed air hose. This will
probe in the water near each other. Record the usually require removal of a chassis panel.
two readings on the form. (It may be necessary to
operate the unit in order to read the thermome- 3.2 Lubricate the circulating pump, if required.
ter.) Repeat the test with cups of water at tem- 3.3 Calibrate, if needed.
peratures of about 37°C and 41°C. The
temperatures, in all cases, should be within 1°C. 3.4 Flush/refill the reservoir and replace the fluid
Repeat this test with each probe. Save the warm- filter, if necessary.
est and coldest cups of water for the next test.
4. Acceptance tests
A patient temperature probe simulator, if
Conduct major inspection tests for this procedure
available, is more convenient for determining the
and the appropriate tests in the General Devices Pro-
accuracy of the patient temperature indicator.
cedure/Checklist 438. In addition, perform the follow-
However, because the simulator tests only the
ing tests.
circuitry and not the probe itself, probe accuracy
must also be verified. A convenient test method 4.1 Probe Leakage Current. If the unit has a patient
is to dip all probes simultaneously into one body- temperature probe, measure leakage current
temperature water bath, allow them to equili- from all available probes in every operating
brate, and successively plug each into the same mode. Wrap the probe loosely with aluminum foil,
pretested temperature unit or module. All clip the lead from the leakage current meter to
probes should give the same temperature read- the foil, and immerse the probe and foil in a salt
ing. (Some variation is normal because the water water solution (normal saline or about a teaspoon
temperature varies slightly with location in the of table salt per cup of water). Leakage current
bath and the water gradually cools with time.) greater than 100 µA suggests a damaged probe.
2.12 Automatic Controller Switching. This test ap- Alternatively, measure probe circuit leakage
plies only to units with an automatic mode. Keep current directly from each probe electrical lead
the patient temperature probe immersed in the contact (using an appropriate plug) on units that
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
do not use ground-referenced probe circuits. If that the water is being warmed. Watch the
the leakage current to ground from each lead of water temperature indicator and the Heat light,
the connector is less than 100 µA in each operat- and record the water temperature reading at
ing mode, then it is unnecessary to check leakage which the Heat light goes out. This is the set-
current from the probe itself. (An appropriate point temperature of the primary high-tempera-
resistance to simulate the thermistor may be ture thermostat. This temperature should agree
required on some units that have protective cir- with the manufacturer’s specification.
cuits to turn off heater power in the event of a
probe malfunction.) However, thoroughly exam- Allow the unit to continue running in the
ine the probe for defects (Item 1.11). manual mode with the water temperature selec-
tor set to its highest setting. The water tempera-
4.2 Hysteresis. This test will determine the differ- ture will begin to slowly drop. Observe the water
ence between the set-point temperature and the temperature indicator, and record the tempera-
reset temperature of the high-temperature ture at which the Heat light comes back on; this
thermostat. This test need be performed only in is the reset temperature of the thermostat. The
the manual mode. If a problem is found in this difference between the set-point temperature
mode, it would consequently also be present in and the reset temperature is the hysteresis. The
the automatic mode. maximum hysteresis should be 3°C. Thus, the
reset temperature range will typically be 39° to
Connect a blanket and/or test hose shunt to the
41°C.
unit. (Some units require that fluid circulate while
the unit is operating.) Allow the unit to warm up
for at least 15 min in the manual mode with the Before returning to use
water temperature set to 40°C. After warm-up, Verify that any control circuits that were bypassed
set the water temperature selector to its highest or deactivated for testing purposes have been returned
setting. The Heat light should come on, indicating to their normal operating conditions.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 415-0595
Infant Incubators
Used For:
Incubators, Infant, Mobile [17-432]
Incubators, Infant, Transport [12-114]
Commonly Used In: Delivery rooms, neonatal ICUs, nurseries, ambulances, and aircraft
Scope: Does not apply to radiant warmers or transport radiant warmers (see Procedure/Checklist 419)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA* months . hours
* Minor intervals for transport incubators should be every 3 months.
Overview and presented electrical shock hazards, and poor
transport incubator performance or power failure due
Infant and transport incubators provide warmth to to improperly maintained batteries or unreliable bat-
help an infant maintain a normal body temperature tery-charge-level indicators. Because incubators are
and are often essential for an infant’s survival. Most bulky and mobile, they routinely receive rough han-
incubators warm the infant by a forced or natural flow dling (especially transport units) that may degrade
of heated air. One type, no longer in production, sup- performance and physical condition. Periodic inspec-
plements air convection with radiant infrared energy tion may reveal hazardous deficiencies that could
from heated bassinet and hood walls. harm patients.
Infant incubators are designed primarily for in-hos-
pital use at specific locations, operate on AC line power Citations from Health Devices
in a temperature-controlled indoor environment, and Mercury contamination in incubators and elsewhere,
rest on relatively high movable stands. Transport 1981 Dec; 11:65-8.
incubators provide thermal support during transfer
within the hospital or by car, ambulance, or aircraft to Transport incubators [Evaluation], 1982 May; 11:
another hospital. Transport incubators are both port- 179-91.
able and mobile; operate from a variety of power Infant incubators [Evaluation], 1982 May; 11:191-9.
sources, including self-contained batteries; have
stands that are relatively low or adjustable in height Update: Transport incubators, 1982 Sep; 11:301.
to fit into vehicles with restricted overhead clearance;
Air-Shields C-300-1, C300-2, and TI-100 infant incu-
and may be required to operate in ambient conditions
bators [Hazard], 1986 Jul; 15:212-3.
much colder than those found in a hospital.
Air-Shields Vickers C100 and C200 infant incubators
Deaths and injuries to neonates have occurred in [Hazard], 1987 Jul; 16:253-4.
incubators. Reports include thermostat failures that
caused incubator overheating and infant hyperther- Air-Shields C-86, C-100, and C-200 infant incubators
mia, malfunctions or design defects that produced fires [Hazard], 1987 Nov; 16:376-7.
009078 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
415-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Air-Shields Vickers C-86 infant incubators [Hazard], operate the equipment, the significance of each control
1988 Oct; 17:314-5. and indicator, and the alarm capabilities. Also deter-
mine whether any special inspection or preventive
Mallinckrodt incuTemp 4 skin temperature probes and maintenance procedures or frequencies are recom-
Air-Shields Vickers C-100 incubators [Hazard], mended by the manufacturer.
1990 Jul; 19:245.
If it is necessary to inspect several incubators that
Thermometer holders detaching from hoods of Oh-
have patient probes, it may be convenient to use a
meda Air-Vac transport incubators, 1994 Oct-Nov;
patient-probe simulator to test indicator accuracy and
23:457-8.
temperature control effectiveness of all probes simul-
taneously. The procedure is essentially the same as
Test apparatus and supplies that used in Temperature Monitors Procedure/Check-
Ground resistance ohmmeter list 425. It may be necessary to use different connec-
Leakage current meter or electrical safety analyzer tors to accommodate the probes of the incubators being
inspected.
Patient-probe simulator capable of simulating a
range of temperatures as well as open- and short- If an incubator to be inspected is in use, ask clinical
circuited probe conditions (for incubators that use personnel if they can use a temporary substitute, or
patient temperature probes) request that they notify you when the incubator is free
Plastic 6 to 8 oz cup for inspection.
Source of varied-temperature water; a temperature 1. Qualitative tests
simulator will simplify some device tests, but at
least one cup of water will be needed to verify probe 1.1 Chassis/Housing. Examine the overall exterior
accuracy and probe leakage current condition of the chassis. Check that the control
Calibrated glass or electronic thermometer accurate unit is clean, that all labels and markings are
to within 0.1°C in the clinical range legible, and that no adhesive tape or tape residue
is present. Remove any tape. Check all rubber
Oxygen source and flowmeter or plastic gaskets in the incubator for signs of
Hot-air gun or hair dryer deterioration (e.g., cracks).
For transport incubators with lead-acid batteries: The hood condition is important for proper
hydrometer to measure specific gravity of the bat- control of the infant’s environment. Ensure that
teries; float markings should cover the range from the hood is free of cracks, warping, or other signs
1.240 to 1.280 to within 0.001 accuracy (available of deterioration. Determine whether any parts
from any scientific apparatus supplier) (Note: auto- are missing or incorrectly assembled. Examine
motive hydrometers that indicate only GOOD or all ports for proper alignment and sealing.
BAD without numerical specific gravity indications
are not suitable.) Consult the instruction manual for a general
exploded diagram of the incubator; remove the
Special precautions hood, bed, baffle, main deck, and other parts and
thoroughly inspect the interior for foreign objects,
Examine all mercury-in-glass thermometers and
deterioration, or misassembly of internal compo-
high-temperature thermostats. If broken, replace and
nents that could interfere with performance. Look
clean the unit carefully using appropriate precautions
for contamination of the air supply and blocked air
for mercury spills (see Health Devices 1981 Dec; 11:65
and/or humidity passages caused by improper
and the “IPM Safety” article behind the Guidance Tab
placement of the humidity tray or gaskets.
in this binder). ECRI recommends replacing all mer-
cury-containing components in infant incubators. Examine the humidity apparatus for deterio-
CAUTION: Mercury and its vapors are toxic. Do not ration, contamination, and missing or incor-
allow mercury to contact an open cut. rectly assembled parts.
1.2 Mount/Fasteners. Check that all screws, nuts,
Procedure and fasteners are tight. Sometimes a loose screw
Before beginning an inspection, carefully read this may not be easy to detect visually. Use a screw-
procedure and the manufacturer’s instruction and driver and systematically try to tighten every
service manuals; be sure that you understand how to screw on the hood.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Infant Incubators
Operate iris-type port closures to ensure make sure that they are clear and free of foreign
proper function. Examine the iris diaphragms matter.
and port sleeves for tears. A torn or otherwise
damaged iris reduces the integrity of the closed- 1.9 Cables. Inspect the cables (e.g., sensor, elec-
chamber system. Consult the manual to deter- trode, remote control) and their strain reliefs for
mine if the irises are disposable types that should general condition. Examine cables carefully to
be discarded after each incubator use. You need detect breaks in the insulation and to ensure
not replace torn disposable irises, since they will that they are gripped securely in the connectors
be routinely replaced when the interior is steril- of each end to prevent rotation or other strain.
ized for the next incubator application. Verify 1.10 Fittings/Connectors. Examine all electrical ca-
with clinical personnel that this practice is en- ble connectors for general condition. Electrical
forced and that disposable irises are not reused. contact pins or surfaces should be straight,
clean, and bright.
1.3 Casters/Brakes. If the device moves on casters,
check their condition. Remove accumulations of 1.11 Probes. Examine all patient probes to ensure
lint and thread from around the casters, and be that they are clean and are not cracked, brittle,
sure that they turn and swivel, as appropriate. or otherwise deteriorated. If the hospital has
Check the operation of brakes and swivel locks more than one type of infant incubator, ensure
if the unit is so equipped. Conductivity checks, that probe labels clearly identify the associated
where appropriate, are usually done more effi- units. Improperly interchanged probes of differ-
ciently as part of a check of all equipment and ent types or from different manufacturers may
furniture in an area. adversely affect temperature control.
1.4 AC Plug/Receptacles. Examine the AC power 1.12 Filters. Inspect the air filter for signs of clog-
plug for damage. Attempt to wiggle the blades to ging; if the filter looks dirty, replace it and note
determine that they are secure. Shake the plug this on Line 3.4 of the inspection form. Check the
and listen for rattles that could indicate loose air-filter assembly to ensure that airflow is un-
screws. If any damage is suspected, open the impeded. Clogged or improperly installed filters
plug and inspect it. can raise the oxygen concentration above safe
levels. Change filters regularly according to the
If the device has electrical receptacles for ac- manufacturer’s recommendations, and record
cessories, insert an AC plug into each and check the date you install a new filter.
that it is held firmly. If accessories are plugged
and unplugged often, consider a full inspection Attach an oxygen source with a flowmeter to
of the receptacle. each oxygen port and use your hand to feel that
gas is flowing into the chamber. Vary the oxygen
1.5 Line Cord. Inspect the cord for signs of damage. flow and check that manufacturer-specified
If damaged, replace the entire cord or, if the maximum and minimum flow rates can be
damage is near one end, cut out the defective achieved.
portion. Be sure to wire a new power cord or plug
with the same polarity as the old one. Check line 1.13 Controls/Switches. Before moving any controls
cords of battery chargers. and alarm limits, check their positions. If any of
them appear inordinate (e.g., a temperature con-
1.6 Strain Reliefs. Examine the strain reliefs at trol turned to the end of its range), consider the
both ends of the line cord. Be sure that they hold possibility of inappropriate clinical use or incipi-
the cord securely. ent device failure. Record the settings of those
controls that should be returned to their original
1.7 Circuit Breaker/Fuse. If the device has a circuit positions following the inspection.
breaker, check that it operates freely. If the
device is protected by an external fuse, check its Examine all controls and switches for physical
value and type against that marked on the chas- condition, secure mounting, and correct motion.
sis, and ensure that a spare is provided. Where a control should operate against fixed-
limit stops, check for proper alignment, as well
1.8 Tubes/Hoses. Check the condition of all tubing as positive stopping. Check membrane switches
and hoses. Be sure that they are not cracked, for membrane damage (e.g., from fingernails,
kinked, or dirty. Inspect all oxygen orifices to pens). During the course of the inspection, be
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
sure to check that each control and switch per- accurate log of operating time, recharges, serv-
forms its proper function. ice, and inspections to permit early detection of
deteriorating performance. Operate the unit on
1.14 Heater. Disassemble the heating unit enough to battery power for several minutes to check that
expose the heating element. Examine the ele- the battery is charged and can hold a charge.
ment for severe discoloration or foreign deposits. Check remaining battery capacity by activating
Heating elements normally change color with the battery test function. Check the condition of
use, but dark, distinct surface spotting may in- the battery charger, and to the extent possible,
dicate that material has come into contact with confirm that it does, in fact, charge the battery.
the element, possibly after falling through the When it is necessary to replace a battery, label
air duct. Foreign matter touching the hot surface it with the date.
could cause a fire or the generation of noxious
fumes. If you find such discoloration, examine A liquid-electrolyte lead-acid battery located
the control unit compartment for signs of over- in the same case as the charging circuitry can
heating (e.g., darkening, blistering). If screw cause problems unless the battery is kept clean.
terminals connect the heating element to the Wash off acid and other materials that may
control circuitry, check that they are tight. collect on top of the battery. If there is electrolyte
or a yellow-white powder on the battery, check
Operate the heater to verify that heater con- for contaminating deposits on components of the
trols function properly (e.g., that a variable tem- charging circuit; these may cause rapid deterio-
perature control does, in fact, cycle the heater off ration. Wipe components clean, or replace the
and on as the set point is varied). charging circuit if it appears corroded. Check for
1.15 Motor/Fan. Inspect the fan blades for deterio- obstructions in the vent caps and associated
ration or damage, such as melting (if plastic), venting system. If necessary, clear the venting
warping, or lost blades. Ensure that the fan is system with a stiff wire, or blow out the tubes
securely attached to its drive shaft and that the through a straw inserted into the vent hole.
coupling is present and intact. Check that clear- 1.18 Indicators/Displays. During the course of the
ance between the fan and its housing is adequate inspection, confirm the operation of all lights,
by looking for signs of rubbing. In some cases, indicators, meters, gauges, and visual displays
an improperly inserted control module and on the unit and charger, if so equipped. Verify
heater assembly in the incubator base has bent that all segments of a digital display function.
and disabled the fan, preventing air circulation
and causing overheating. 1.19 User Calibration/Self Test. Verify operation of
these features, where applicable.
Check the service manual to determine if the
fan motor requires lubrication. Oil as recom- 1.20 Alarms. Operate the device in such a way as to
mended and note on Line 3.2 of the inspection activate each audible and visual alarm. Check
form. Check the sound level inside the incubator; that any associated interlocks function.
noisy operation may indicate that the fan motor
or housing assembly needs service. Check the action of the disconnected-probe
alarm, if the unit is so equipped. Also, if it has
In some incubators, the fan is visible at the alarms for open- or short-circuited patient tem-
back of the control module if the module is re- perature probes, test these with open- and short-
moved. If possible, expose the fan and operate circuited probe plugs. If the device has an
it, and watch for wobbling or excessive vibration. alarm-silence feature, check the method of reset
If possible, spin the fan with your finger (with the (i.e., manual or automatic) against the manufac-
power off) and make sure that it turns smoothly. turer’s specifications.
1.16 Fluid Levels. Check all fluid levels, including 1.21 Audible Signals. Operate the device to activate
those in lead-acid batteries. any audible signals. Confirm appropriate vol-
ume, as well as operation of volume controls.
1.17 Battery/Charger. Inspect the physical condi-
tion of batteries and battery connectors if readily 1.22 Labeling. Check that labels clearly and con-
accessible. Check operation of battery-operated cisely identify the functions of all controls,
power-loss alarms if so equipped. Each battery switches, and connectors. Because incubators
should have an identification number and an may administer supplemental oxygen, they
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Infant Incubators
should carry a WARNING — FIRE HAZARD If the device has an accessory outlet, check its
placard, since textiles, oils, and other combusti- grounding to the main power cord.
bles ignite easily and burn intensely in oxygen-
enriched air. Exposing an infant to high oxygen 2.2 Leakage Current. Measure the leakage current
concentrations may cause retrolental fibroplasia to ground from the incubator chassis and, if the
and possible blindness. Thus, incubator labeling unit has a battery charger, from the charger
should also include the following: WARNING: chassis in all operating modes, including off, and
EXPOSING INFANTS TO ELEVATED OXY- during battery operation. Measure while all ac-
GEN CONCENTRATIONS MAY CAUSE cessories (e.g., examining and phototherapy
BLINDNESS. lamps) are operating. Chassis leakage should
not exceed 300 µA. (Note that the chassis leak-
1.23 Accessories. age of transport incubators may vary with the
state of battery charge.)
Hood thermometer. Check the hood thermome-
ter for cracked glass and separation of the
Measure chassis leakage current with all ac-
liquid column. If the liquid column has sepa-
cessories normally powered from the same line
rated, it might be possible to consolidate it by
cord connected and turned on and off. This in-
removing the thermometer and carefully dip-
cludes other equipment that is plugged into the
ping it in hot water. If the thermometer has
primary device’s accessory receptacles, as well as
an expanded space at the top, the liquid will
equipment plugged into a multiple-outlet strip
pool in the small reserve chamber. When the
(“Waber strip”), so that all are grounded through
gap in the column disappears into the pool,
a single line or extension cord.
cool the thermometer and recheck it for col-
umn separations. Repeat the process if neces- 2.3 Temperature Control. Check the action of the
sary. If the thermometer does not have primary and safety thermostats with the incuba-
reserve space at the top, the heated liquid will tor fully assembled. Although this is time-con-
expand until it completely fills the thermome- suming, it is essential, since proper thermostatic
ter, after which pressure will build up. The operation depends on the presence of normal
pressure may eliminate the column separa- airflow patterns. Test the thermostats accord-
tion, but it may also break the thermometer. ing to the manufacturer’s instructions, and re-
Even with a reserve space, overheating the cord on the form the temperature at which the
thermometer may break it. In either case, do safety or backup thermostat turns off the heater.
not heat the thermometer too fast or to too If the manufacturer does not provide instruc-
high a temperature while attempting to con- tions, use the following methods, which test both
solidate the column. Replace the thermometer manual and automatic temperature controls.
if it is cracked.
In the manual mode, the primary thermostat
Mattress. If the mattress position is adjustable,
cycles the heater on and off or provides propor-
check the ease of motion and security of the
tional heating to maintain a constant hood tem-
locking mechanism. Examine the mattress for
perature. The operator can adjust the
cleanliness. If the unit is to be used in the
temperature by changing a setting. In the auto-
presence of flammable anesthetics, check that
matic mode, a patient probe senses the infant’s
a conductive mattress cover is being used.
skin temperature, and electronic circuits control
the heater to keep the skin temperature constant
2. Quantitative tests at a clinically desirable level.
2.1 Grounding Resistance. Using an ohmmeter, To test manual controls, position the cali-
electrical safety analyzer, or multimeter with brated glass or electronic thermometer 10 cm
good resolution of fractional ohms, measure and (4 in) above the center of the mattress, close the
record the resistance between the grounding pin hood, set the temperature control to mid range,
of the power cord and exposed (unpainted and allow the incubator to warm up to thermal equi-
not anodized) metal on the chassis. We recom- librium, and record the hood thermometer read-
mend a maximum of 0.5 Ω. If the system is ing and the true mid-hood air temperature in
modular, verify grounding of the mainframe and Item 2.7. Then, alternately raise and lower the
each module. temperature setting. If the primary thermostat
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
is operating properly, the heater will turn on and is because the safety thermostat is often at some
off, respectively. distance from the mid-hood area, downstream in
the airflow, so that its temperature lags behind
To check automatic controls, first test the the mid-hood air temperature. Also, avoid blow-
accuracy of the patient-probe temperature indi- ing hot air directly at the thermometers. If a
cator. Place the probe and a calibrated ther- blower is used, deliver intermittent bursts of
mometer into a cup of water preheated to heat and pause for thermal stabilization. Recon-
approximately 35°C. Stir to reduce temperature nect the primary thermostat that had been dis-
gradients, allow the temperature readings to abled in the above procedure (consult the
stabilize, and record the patient-probe tempera- operator’s manual to determine the necessary
ture indication and the true bath temperature in procedure).
Item 2.8. If the two readings do not agree within
0.3°C, the probe may be defective. Substitute a 2.6 Air-Temperature Alarms. If the incubator is
probe known to be accurate, and repeat the test. equipped with high and low air-temperature
If the two readings still disagree, the measuring alarms other than those that are controlled by a
circuit or meter is defective and requires recali- secondary temperature controller, verify that
bration or repair. the alarms are functional. Adjust the air-tem-
perature set point to 36°C and allow the air
Confirm the operation of the temperature con- temperature to stabilize. Verify that the low
trol circuit by alternately dipping the probe into air-temperature alarm (if so equipped) activates
cold and hot water, well below and above the when the incubator hood is opened.
skin-temperature set point, respectively. The
heater should activate when the probe is cold and To verify the high air-temperature alarm, set
turn off when the probe is hot. the air-temperature set point to 36°C and slowly
increase the air temperature with an external
2.4 Skin-Temperature Alarms. If the incubator is heat source (e.g., hair dryer or heat gun). Note
equipped with high and low skin-temperature when the high alarm responds.
alarms, verify that these alarms function. Adjust
the skin temperature set point to 36°C. Place the 2.7 Hood Air Temperature. The mid-hood air tem-
sensor in the incubator and allow the tempera- perature and hood thermometer readings taken
ture to stabilize. Remove the sensor from the in Item 2.3 should agree within 1°C.
incubator, and verify that the low skin-tempera-
2.8 Patient Probe. The patient-probe temperature
ture alarm activates.
indication and true water bath temperature, also
To verify the high skin-temperature alarm, recorded during performance of Item 2.3, should
place the sensor in a water bath set at 36°C and agree within 0.3°C.
gradually increase the water bath temperature.
2.9 Portable Power Supply (transport incubators
Note the point at which the high alarm responds. only). The portable power supply usually con-
2.5 Safety Thermostat To test the operation of the sists of a rechargeable battery, a recharging cir-
safety thermostat and the high-temperature cuit, and associated wiring and connectors. It is
alarm, disable the primary thermostat or discon- essential to keep all parts in good condition to
nect it from the control circuit (consult the man- ensure the safe, effective operation of the trans-
ual to determine the necessary procedure) so port incubator.
that the heater remains on continuously. In Battery types vary, and each requires a differ-
some cases, this can be achieved by turning the ent inspection and preventive maintenance pro-
temperature control to its maximum setting. It cedure. Types commonly used are lead-acid with
is possible to speed up the air-temperature rise a liquid or sealed gelled-electrolyte, nickel-cad-
by supplementing the incubator heater output mium, and alkaline batteries. Sealed batteries
with a hot-air gun or hair dryer. Record the hood require less maintenance than types to which
thermometer indication and the true mid-hood fluid must occasionally be added to compensate
air temperature at which the safety thermostat for evaporation.
and high-temperature alarm respond. Be careful
not to heat the hood air too rapidly with the Measure the specific gravity of lead-acid bat-
hot-air blower, or the mid-hood air temperature teries with a hydrometer, but not while the bat-
at the alarm point will be erroneously high. This tery is charging. If the battery is charging at
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Infant Incubators
inspection time, disconnect the charger and wait heater on after the batteries are fully charged,
at least 15 min before testing the battery. Before and measure the voltage under load initially and
taking a reading, rapidly fill and empty the hy- after 15 min of operation. Record the two values.
drometer several times to thoroughly mix the elec- If the voltage decreases more than 10% during
trolyte, taking care to avoid splashing or spilling. this period, replace the battery.
The specific gravity of a fully charged battery
should be 1.265. (It may be necessary to check the 3. Preventive maintenance
electrolyte level and measure the specific gravity
of lead-acid batteries as frequently as every two 3.1 Clean the exterior and interior.
weeks, depending on use and age of battery.) 3.2 Lubricate the fan assembly if required.
If the liquid level is low, add distilled or
3.3 Calibrate if needed.
demineralized water to bring the level to the split
ring in each cell. Do not overfill. Excess water 3.4 Replace filter and battery if needed.
may boil over and damage the battery case and
nearby charging circuits. If the battery has been 4. Acceptance tests
on a constant trickle charge and the specific
gravity is too low and battery voltage is lower Conduct major inspection tests for this procedure
than 12.6 V, then the battery is defective or the and the appropriate tests in the General Devices Pro-
charger circuit is at fault. The charging circuit cedure/Checklist 438.
may need readjustment.
If the incubator uses nickel-cadmium or
Before returning to use
gelled-electrolyte lead-acid batteries, turn the Set all controls to their normal positions.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Procedure/Checklist 416-0595
Infusion Devices
Used For:
Infusion Controllers [11-010]
Infusion Pumps, Ambulatory [16-491]
Infusion Pumps, General-Purpose [13-215]
Infusion Pumps, Micro [16-722]
Infusion Pumps, Multichannel [17-634]
Infusion Pumps, Patient-Controlled Analgesic [16-924]
Infusion Pumps, Syringe [13-217]
Pumps, Enteral Feeding [13-209]
Commonly Used In: All patient care areas, homes
Scope: Applies to most types of electromechanical devices that regulate the delivery of fluids to a patient,
including general-purpose infusion pumps, multichannel pumps, microinfusion pumps, patient-controlled
analgesic (PCA) pumps, syringe pumps, ambulatory pumps, enteral feeding pumps, infusion controllers
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview infuse small volumes at rates less than 100 mL/hr by
depressing the plunger or sliding the barrel of a con-
Infusion devices are often used when accurate delivery ventional syringe installed in the pump. Ambulatory
rates are required over long periods of time. General- pumps are small and do not rely on line power or
purpose infusion pumps and controllers are used for gravity for operation. They are commonly used to in-
many of the same applications and have similar alarm fuse antibiotics, analgesics, chemotherapeutic agents,
features. However, infusion pumps infuse under pres- and total parenteral nutrition solutions. Enteral feed-
sure, whereas controllers regulate a gravity infusion. ing pumps are typically used to deliver enteral solution
Most general-purpose infusion pumps have a flow or food mixtures to a patient’s stomach or small intes-
range of 1 to 999 mL/hr, while most controllers regulate tine through an enteral feeding tube.
flow in a range of 3 to 300 mL/hr. Multichannel infusion
devices consist of two or more general-purpose pumps
and/or controllers within one chassis. Microinfusion
Citations from Health Devices
pumps are similar to general-purpose pumps but have Enteral feeding pumps [Evaluation], 1984 Nov; 13:9-30.
greater flow resolution and lower flow settings; they are
commonly used in neonatal critical care areas. PCA Infusion controllers [Evaluation], 1985 May; 14:219-56.
pumps deliver pain medication on patient demand by Undetected upstream occlusions in volumetric infu-
handswitch activation; they are programmed for drug sion pumps [Hazard], 1986 Jun; 15:182-4.
concentration and dose volume, lockout interval, and
maximum dose. Syringe pumps are typically used to Syringe infusion pumps [Evaluation], 1987 Jan; 16:3-32.
009060 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
416-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Ambulatory insulin infusion pumps [Evaluation], 1987 1. Qualitative tests
Nov; 16:351-76.
1.1 Chassis/Housing. Examine the unit for overall
Patient-controlled analgesic pumps [Evaluation], 1988 condition. The chassis should be clean and free
May; 17:137-66. from IV or enteral solution residue, especially
near moving parts (e.g., thumbwheel switches,
General-purpose infusion pumps [Evaluation], 1989 pump or controller mechanisms). Also check for
Mar-Apr; 18:92-133. dried solution deposits on accessible air-in-line
sensors, pressure sensing mechanisms, and in-
Ambulatory infusion pumps [Evaluation], 1991 Sep;
fusion set/cassette locking mechanisms. Check
20:324-58.
that labels and markings are legible.
IV free-flow — still a cause for alarm [Perspectives], 1.2 Mount. Screws and brackets that attach the
1992 Sep; 21:323-8. unit to an IV pole should be secure and function-
ECRI responds to FDA Public Health Advisory on IV ing. If the device is mounted on a stand or cart,
free-flow [Hazard], 1994 Jun; 23:256-7. examine the condition of the mount. Also exam-
ine the pole, stand, or cart.
Test apparatus and supplies 1.3 Casters/Brakes. If the unit is mounted on a
dedicated IV pole, stand, or cart that moves on
General: casters, check their condition. Look for accumu-
Ground resistance ohmmeter lations of lint and thread around the casters and
Leakage current meter or electrical safety analyzer be sure that they turn and swivel, as appropri-
ate. Check the operation of brakes and swivel
At least one IV tubing set, cassette, syringe, and/or locks, if the unit is so equipped.
other disposable specified for the pump or controller
being inspected 1.4 AC Plug/Receptacles. Examine the AC power
plug for damage. Attempt to wiggle the blades
Fluid container of outdated (i.e., clinically unusable)
to determine that they are secure. Shake the
IV solution or degassed water
plug and listen for rattles that could indicate
IV pole loose screws. If any damage is suspected, open
the plug and inspect it.
Pressure meter (0 to 50 psi)
U-100 insulin syringe and needle If the device or its IV pole has electrical recep-
tacles for accessories, inspect them by inserting
For determining flow accuracy at settings ≥1 mL/hr: an AC plug into each and checking that it is held
50 mL graduated cylinder with 1 mL graduations firmly. If accessories are plugged and unplugged
and stopwatch or watch with a second hand, or often, consider a full inspection of the receptacle.
Infusion pump analyzer 1.5 Line Cord. Inspect the cord for signs of damage.
For determining flow accuracy at settings <1 mL/hr: If damaged, either replace the entire cord or, if
the damage is near one end, cut out the defective
Electronic balance with a 200 g range and resolution
portion. Be sure to wire the new power cord or
to 0.1 mg and small beaker, or
plug with the correct polarity.
10 mL pipette with 0.1 mL graduations and vertical
mounting stand 1.6 Strain Reliefs. Examine the strain reliefs at
both ends of the line cord. Be sure that they hold
the cord securely.
Procedure
1.7 Circuit Breaker/Fuse. If the unit has a switch-
Before beginning an inspection, carefully read this type circuit breaker, check that it moves freely.
procedure and the manufacturer’s instruction and If the unit is protected by an external fuse, check
service manuals; be sure that you understand how to its value and type against that marked on the
operate the equipment, the significance of each control chassis, and ensure that a spare fuse is provided.
and indicator, and the alarm capabilities. Also deter-
mine whether any special inspection or preventive 1.9 Cables. Inspect drop sensors and remote air-in-
maintenance procedures or frequencies are recom- line detector cables for general condition. Exam-
mended by the manufacturer. ine cables carefully to detect breaks in the
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Infusion Devices
insulation. Ensure that they are gripped se- the instruction manual to see how the alarm
curely in the connectors at each end to prevent should work. When an alarm occurs, check to see
rotation or other strain. that both audible and visual alarms are acti-
vated and that flow stops or is reduced to a
1.10 Fittings/Connectors. Examine any electrical ca- keep-vein-open rate (e.g., <5 mL/hr). Confirm
ble connectors (e.g., drop sensor, nurse call) for appropriate alarm volume, as well as the opera-
general condition. Electrical contact pins or sur- tion of any volume control.
faces should be straight and clean. Check any
spill-protection connector caps for signs of damage. Set up the infusion device according to the
manufacturer’s instructions, using an IV pole, a
1.13 Controls/Switches. Before moving any control container of outdated IV solution or degassed
switches, dials, or knobs, check their positions. water, and the specified IV set. Be sure that the
If any appear inordinate (e.g., volume-infused set is properly primed and that bubbles are re-
counter or audible alarm level at the end of its moved.
range), consider the possibility of inappropriate
clinical use or of incipient device failure. Record Air-in-line. In some units, this alarm is the
the settings of those controls (e.g., occlusion pres- same as the empty-container alarm. Test its
sure limits) that should be returned to their function by introducing a small air bubble into
original positions following the inspection. Ex- the system by righting the fluid container
amine all controls and switches for physical con- briefly or by injecting air into an injection port
dition, secure mounting, and correct motion. of the IV tubing with a syringe between the
Where a control should operate against fixed- container and the air-in-line detector. (Sensi-
limit stops, check for proper alignment, as well tivity to air volumes of less than 50 µL is likely
as positive stopping. Check membrane switches to result in nuisance alarms; most devices will
for membrane damage (e.g., from fingernails, trigger an alarm for greater than 100 µL air;
pens). During the course of the inspection, be 50 and 100 µL volumes can be approximated
sure to check that each control and switch per- by 5 and 10 units, respectively, from a U-100
forms its proper function. insulin syringe.)
Empty container. Simulate an empty fluid con-
1.17 Battery. Inspect the physical condition of batter-
tainer while the device is infusing. The simu-
ies and battery connectors, if readily accessible.
lation method will depend on the type of
Operate the unit on battery power during its
sensor that is used in the alarm system. For
entire inspection to check that the battery has
most units, turning the fluid container up-
been charged and can hold a charge. If a low-bat-
right will cut off the supply, empty the tubing
tery alarm occurs, check to ensure that it is
leading from the container, and trigger the
properly displayed and then continue the inspec-
alarm. For units that rely on a drop sensor or
tion using line power. Note how long the unit has
an empty container detector to determine
been operating and the conditions under which
fluid depletion, simply remove the sensor de-
the low-battery alarm occurred. Fully charge the
tector from the drop chamber.
battery before returning the unit to use. When it
is necessary to replace a battery, label it with the Occlusion. See Item 2.11.
date.
Infusion complete. If the total volume to be in-
1.18 Indicators/Displays. During the course of the fused can be preset, set it to a low volume (e.g.,
inspection, confirm the operation of all lights, 10 mL), and operate the pump at a high-flow
indicators, meters, gauges, visual displays, and setting.
display backlighting, if so equipped. Be sure Open door/misloaded infusion set. Check this
that all segments of a digital display function. alarm during setup and operation.
(Many infusion devices automatically check in-
dicator and display function when turned on or Nurse call. Some pumps have a relay contact
during a manually activated self-test.) closure that activates a nurse-call system
when an alarm condition occurs. This re-
1.20 Alarms. Many of the alarm capabilities of infu- quires a special cable that connects the pump
sion pumps and controllers can be checked quali- to the nurse-call system. If the unit has this
tatively. The following procedures include tests capability and it is used in any clinical loca-
for the most common alarm conditions. Check tion, connect the cable, and simulate one or
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
more of the above alarm conditions to deter- 2.2 Leakage Current. Measure leakage current be-
mine whether they activate the nurse call. tween the chassis and ground with the ground-
Alternatively, use an ohmmeter to check that ing conductor temporarily opened. Measure
a change in resistance (either low to high or chassis leakage current with all accessories nor-
high to low) occurs between the two conduc- mally powered from the same line cord connected
tors of the cable when an alarm condition is and turned on and off. This includes other equip-
created. ment that is plugged into the primary device’s
accessory receptacles, as well as equipment
1.21 Audible Signals. Operate the device (e.g., press plugged into a multiple-outlet strip (“Waber
rate switches) to activate any audible signals. strip”) so that all are grounded through a single
Confirm appropriate volume, as well as the op- line or extension cord.
eration of the volume control, if so equipped.
Chassis leakage current to ground should not
1.22 Labeling. Check that all necessary placards, la- exceed 300 µA.
bels, conversion charts, and instruction cards
are present and legible. 2.10 Flow Accuracy. It may be desirable to record the
type of tubing, pump chamber or syringe brand
1.23 Accessories. Check the condition of external air-
and size (where user selectable), solution used,
in-line and drop sensors, if so equipped. Clean
and any other test variables to facilitate the
sensors according to the manufacturer’s instruc-
comparison of results with those obtained during
tions. After cleaning the drop sensor, confirm
future inspections.
operation by passing a pen or finger between the
sensor while watching for activation of the drop Flow settings ≥1 mL/hr: Use an infusion pump
indicator, if present. analyzer or collect the output in a graduated
cylinder. Determine the flow accuracy at two
1.24 Flow-Stop Mechanism(s). Turn the power off or more typical clinical flow settings (e.g., 10
with the infusion set primed and loaded in the and 100 mL/hr). (Choose the correct fluid code
device. With all tubing clamps open and the fluid when testing volumetric controllers.) Use a
container two feet or more above the device, stopwatch or a watch with a second hand to
verify that no fluid flows out of the set. time the delivery into the graduated cylinder
until at least 10 mL is collected. Record the
If the device incorporates a mechanism that
time interval and volume collected, and calcu-
automatically closes the set or requires the set to
late the delivery rate in mL/hr.
be manually closed before it is removed from the
device, verify the operation of this mechanism.
Flow settings <1 mL/hr: If an electronic bal-
1.25 Lockout Interval. (This test applies only to PCA ance is available, gravimetrically determine
pumps.) Program the unit for its minimum lock- device accuracy by weighing a small beaker
out interval (typically 1 to 5 min). Activate a (covered with a film of plastic wrap to mini-
dose, and then verify that a second dose cannot mize evaporative losses) before and after col-
be activated until the programmed lockout time lecting a mass of at least 1.5 g. Convert the
has elapsed. mass to volume (1 g H2O = 1 mL; 1 g/mL can
be used for most other test solutions [e.g.,
2. Quantitative tests normal saline], although the mass per unit
volume of some fluids may differ signifi-
2.1 Grounding Resistance. Measure and record the cantly). Divide the calculated volume by the
resistance between the grounding pin of the collection time in hours (e.g., 1.5 mL ÷ 15 hr
power cord and exposed (unpainted and not ano- = 0.1 mL/hr). Follow this procedure to deter-
dized) metal on the chassis with an ohmmeter, mine bolus volume accuracy of PCA pumps;
electrical safety analyzer, or multimeter with for pumps programmed in volume units (e.g.,
good resolution of fractional ohms. We recom- mL), collect and determine the average value
mend a maximum of 0.5 Ω. of three 1.5 mL boluses; for pumps pro-
grammed in mass units (e.g., mg), select a
If the device or its IV pole has an accessory concentration of 1.0 mg/mL and a 1.5 mg
outlet, check its grounding to the main power bolus, and then collect and determine the
cord. average value of three boluses.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Infusion Devices
If an electronic balance is not available, use a alarm pressure(s). The maximum pressure of
small length of rubber hose to connect the infusion newer pumps is typically 20 psi or less.
set to the base of a vertically mounted, graduated
5 mL pipette (resolution to 0.1 mL). Divide the Connect the distal end of the primed admini-
collected volume (1.5 mL, minimum) by the collec- stration set to a pressure meter, and start the
tion time to calculate the infusion rate. infusion. Test alarm pressures at two commonly
used flow settings (e.g., 10 and 100 mL/hr). If the
To calculate flow error, use the following pressures are outside the unit’s specifications,
formula: consult the service manual for making the nec-
essary corrections. For units that have adjust-
Actual rate − Desired rate
% Error = × 100% able occlusion alarm pressures, test at high and
Desired rate
low settings.
Exercise extreme care during measuring to
ensure accurate test results. Although most in- If the device delivers from an external fluid
travenous infusion pumps are specified to de- container, verify upstream occlusion detection
liver within 5% of the flow setting, 10% is by activating infusion with the tubing clamped
acceptable for most applications; for critical ap- just below the container. (Some pumps do not
plications, the error should not exceed 5%. (Note: have this capability; see Health Devices 1986
Negative and positive flow error represents un- Jun; 15:182-4.)
derdelivery and overdelivery, respectively.) Ex-
pect greater delivery errors (up to 15%) with 3. Preventive maintenance
enteral feeding pumps. Infusion controllers are 3.1 Clean the exterior and the interior of the unit, if
typically specified to deliver within 10% of the required. Pay particular attention to solution
flow setting or drop rate. Be sure that infusion deposits on mechanical infusion control mecha-
devices are used appropriately (e.g., infusion nisms, drop and air-in-line detectors, and occlu-
controllers should not be used for critical intra- sion or pressure-sensing mechanisms.
venous infusions).
3.3 Calibrate per the manufacturer’s specifications.
If the unit is designed to count drops and the
delivery rate can be set only in drops/min, do not 3.4 Replace the battery, if necessary.
attempt to convert to mL/hr. Converting drops to
milliliters is complex and only grossly assesses 4. Acceptance tests
the device’s ability to deliver fluid volumes. In-
Conduct major inspection tests for this procedure
stead, operate the device for 3 to 5 min at a
and the appropriate tests in the General Devices Pro-
midrange rate setting, and then count the drops
cedure/Checklist 438. In addition, perform the follow-
falling into the drip chamber for 2 min. Operate
ing test.
the device for several more minutes, and repeat
the count. Calculate the number of drops per 4.1 Flow Accuracy. Determine flow accuracy at
minute for each trial, and average the two rates minimum and maximum flow settings, following
if they are different. (Slight variations may be the procedures in Item 2.10.
due to the control circuitry correcting for errors.)
2.11 Maximum Pressure/Occlusion Alarms. (Exclude Before returning to use
infusion controllers from these tests because of Ensure that the unit’s battery is fully charged and
their inherently low operating pressures.) Deter- that the case is properly reassembled to minimize the
mine the unit’s specified downstream occlusion risk of fluid entry.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 432-0595
Intra-Aortic Balloon Pumps
Used For:
Circulatory Assist Units, Intra-Aortic Balloon [10-846]
Also Called: IABPs, counterpulsation units
Commonly Used In: Critical care units, catheterization labs, operating rooms
Scope: Applies to all intra-aortic balloon pumps; ECG and pressure monitors in these units should be inspected
using the appropriate Inspection and Preventive Maintenance Procedures
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 6 months months . hours
Minor NA months . hours
Overview Intra-aortic balloon pumps [Evaluation], 1987 May;
16:135-76. (See also 1987 Jun; 16:216.)
An intra-aortic balloon is placed in the descending
aorta and controlled by a complex electromechanical Inaccurate blood pressure readings on IABP patients
system in an attempt to lower the pressure the heart [Hazard], 1989 Mar-Apr; 18:138.
has to work against and to provide better coronary and
systemic perfusion. Test apparatus and supplies
Intra-aortic balloon pumps have been used for sev- Aortic simulator (see the “Test Equipment” section
eral types of heart disease. Their most frequent and of this binder)
successful use has been with cardiac surgery, applied
as a preoperative, intraoperative, or postoperative aid Transducer simulator (or pressure transducer and
to open-heart surgery; for patients with unstable an- accurate pressure source); these devices were evalu-
gina who are not responding to medication and who ated in Health Devices 1980 Jan; 9:59
may be helped by revascularization surgery; as a pre- ECG simulator
caution before revascularization surgery after arte-
riography has indicated a coronary lesion; in high-risk Leakage current meter or electrical safety analyzer
patients (patients with left main coronary artery occlu- Ground resistance ohmmeter
sion or poor left ventricular function); and for weaning
patients with low cardiac output from cardiopulmon- Expendable supplies such as a stopcock and syringe
ary bypass. and other tubing and fittings for connecting test
equipment
Citations from Health Devices Leak-detecting solution
Intra-aortic balloon pumps [Evaluation], 1981 Nov; Transducer connector (may be required to gain access
11:3-39. to monitor terminals) (acceptance inspection only)
093755 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
432-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Isolation test supply; this feature may be included accessories are plugged and unplugged often,
in some electrical safety analyzers (acceptance in- consider a full inspection of the receptacle.
spection only)
1.5 Line Cord. Inspect the cord for signs of damage.
If damaged, replace the entire cord, or if the
Procedure damage is near one end, cut out the defective
Before beginning an inspection, carefully read this portion. Be sure to wire a new power cord or plug
procedure and the manufacturer’s instruction and with the same polarity as the old one. Also check
service manuals; be sure that you understand how to line cords of battery chargers.
operate the equipment, the significance of each control
and indicator, and the alarm capabilities. Also deter- 1.6 Strain Reliefs. Examine the strain reliefs at
mine whether any special inspection or preventive both ends of the line cord. Be sure that they hold
maintenance procedures or frequencies are recom- the cord securely.
mended by the manufacturer.
1.7 Circuit Breaker/Fuse. If the device has a
Since available intra-aortic balloon pumps differ switch-type circuit breaker, check that it moves
considerably and are relatively complicated life-sup- freely. If the device is protected by an external
port devices, be familiar with the operation of the unit fuse, check its value and type against that
to be inspected. Inspection test methodology and cri- marked on the chassis, and ensure that a spare
teria may vary from unit to unit; customize this proce- fuse is provided.
dure as required. For specific instructions on how to
1.8 Tubes/Hoses/Moisture. Check the condition of
perform tests or inspections, consult the operator’s
all tubing in the unit. Be sure that tubing is not
manuals or manufacturers. Record the hour meter
cracked, kinked, or dirty. Check that tubing is
reading and (when applicable) note the software ver-
secured away from any elements that may be-
sion before beginning the inspection.
come hot and that it has proper strain relief.
Clean or replace as necessary.
1. Qualitative tests
1.1 Chassis/Housing. Examine the exterior of the Be sure no moisture has accumulated in the
unit for cleanliness and general physical condi- pneumatic pathway. Inspect the patient isola-
tion. Be sure that plastic housings are intact, tion system, where applicable, for moisture. If
that all assembly hardware is present and tight, the isolation system is not transparent, briefly
and that there are no signs of spilled liquids or operate the balloon pump with the tubing at-
other serious abuse. tached to determine if there is moisture in the
unit. See the operator’s manual for specific in-
1.2 Mount/Fasteners. If unit components (e.g., structions on how to clear moisture. If moisture
ECG, blood pressure monitors) are independent is in the tubing, either dry it or replace the
modules on the console, check mounting of mod- tubing. After clearing moisture, inform IABP
ules to ensure that they are securely attached. users that moisture has accumulated during use
and instruct them to clear the system of moisture
1.3 Casters/Brakes. If the device moves on casters, after each use.
check their condition. Look for accumulations of
lint and thread around the casters, and be sure 1.9 Cables. Inspect ECG electrode and pressure
that they turn and swivel, as appropriate. Check transducer cables and any interconnecting ca-
the operation of brakes and swivel locks, if the unit bles between modules for neat and secure rout-
is so equipped. Conductivity checks, where appro- ing, condition, and strain reliefs. If additional
priate, are usually done more efficiently as part of cables are provided for slaving pressure or ECG
a check of all equipment and furniture in an area. signals to other units, check their function and
condition. Spare ECG and pressure cables
1.4 AC Plug/Receptacles. Examine the AC power should be kept with the unit. Check cable (ECG
plug for damage. Attempt to wiggle the blades and blood pressure ports) on consoles to ensure
to determine that they are secure. Shake the that connectors are in good condition (e.g., no
plug and listen for rattles that could indicate bent pins or cracked connectors).
loose screws. If any damage is suspected, open
the plug and inspect it. If the device has electrical 1.10 Fittings/Connectors. Check the condition of all
receptacles for accessories, insert an AC plug gas manifolds, fittings, and connectors in the
into each and check that it is held firmly. If pneumatic pathway. Examine all gauges and
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Intra-Aortic Balloon Pumps
valves for general condition. If leaks are sus- may prove to be cost-effective, since it eliminates
pected, check tubing and high-pressure regula- most battery failures and the problems of un-
tor connections for leaks using a leak-detecting scheduled battery replacement. This is particu-
solution. If pneumatic systems pass near elec- larly true for transport models.) Where
tronic portions of the units, be careful not to spill appropriate, check the specific gravity of lead-
or drip the solution on electronic components. acid batteries.
1.11 Electrodes/Transducers. Verify that ECG elec- Operate the unit on battery power for several
trodes and pressure transducers and disposable minutes to check that the battery is charged and
domes, if used, are on hand and in good physical can hold a charge. Check that charging lights or
condition. battery status meters are operative. Verify
1.12 Filters. Check the condition of air filters in the automatic switchover to battery power, if pro-
pneumatic pathway associated with the com- vided. Check the condition of the battery
pressor or vacuum pump and filters associated charger, and to the extent possible, confirm that
with fans for cooling electronic components. it charges the battery. When not in use, always
Clean or replace as required and indicate this on leave the unit plugged in so that batteries may
Lines 3.1 and 3.4 of the form. charge. The unit should be placarded LEAVE
PLUGGED IN AT ALL TIMES.
1.13 Controls/Switches. Before moving any controls
and alarm limits, check their positions. If any of To further assess rechargeable battery capac-
them appear inordinate, consider the possibility of ity, most of the inspection procedure can be
inappropriate clinical use or incipient device fail- performed with the unit operating on battery
ure. Record the settings of those controls that power. Before operating the unit on battery
should be returned to their original positions fol- power for a prolonged period, be sure there is
lowing the inspection. Examine all controls and adequate time for recharging or that an alter-
switches for physical condition, secure mounting, nate unit is available.
and correct motion. Where a control should oper-
ate against fixed-limit stops, check for proper If required, replace the batteries during the
alignment, as well as positive stopping. Check inspection procedure (unless the operator’s man-
membrane switches for membrane damage (e.g., ual requires more frequent replacement). When
from fingernails, pens). During the course of the it is necessary to replace a battery, label it with
inspection, be sure to check that each control and the date.
switch performs its proper function. 1.18 Indicators/Displays. During the course of the
1.15 Motor/Pump/Fan. Inspect and confirm the inspection, confirm the operation of all lights,
physical condition and proper operation of vac- indicators, meters, gauges, and visual displays.
uum and pressure pumps, drive solenoids, and If the unit has digital displays, be sure that all
cooling fans. Replace pump diaphragms, valves, segments of the display function properly. Ex-
or gaskets, lubricate as required, and note this amine all regulators and pressure gauges or
on Lines 3.2 and 3.4 of the inspection form. meters for signs of damage or abuse.
1.16 Fluid Levels. Check fluid levels in lead-acid bat- 1.19 User Calibration. Confirm that the ECG and
teries where appropriate. Check the fluid level pressure monitors’ calibration functions operate
in the dome and syringe of the Mansfield (now properly.
Boston Scientific) unit, and refill with distilled
or sterile water, if necessary. (The dome should 1.20 Alarms/Interlocks. Operate the device in such
be full when the syringe is empty.) a way as to activate audible and visual alarms
(e.g., heart rate, leak detectors, trigger loss, vac-
1.17 Battery/Charger. Inspect the physical condi- uum or pressure loss, trigger change, balloon
tion of batteries and battery connectors, if read- disconnect). Check the function of any associated
ily accessible. Check operation of interlocks (e.g., balloon deflation).
battery-operated power-loss alarms, if so
equipped. Check the battery date code, if pro- 1.21 Audible Signals. Operate the device to activate
vided, for expiration. (Depending on how heav- any audible signals. Confirm appropriate vol-
ily your hospital relies on rechargeable batteries ume, as well as operation of the volume control,
for IABP operation, annual battery replacement if so equipped. If audible alarms have been si-
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
lenced, alert clinical personnel to the importance that the diameter of the orifice through the T-
of keeping alarms at the appropriate level. piece is not significantly smaller than the cathe-
ter diameter; otherwise, the back pressure
1.22 Labeling. Check that all necessary placards, la- created by the restriction may trigger alarms on
bels, timing adjustment charts, and instruction some units. The test method will vary with the
cards are present and legible. model being tested. The following describes tests
1.23 Accessories. Confirm the presence and condition appropriate for units currently in common use.
of safety chambers, patient isolator, and magnet Aries and Datascope pumps. Operate in Auto
(i.e., for Mansfield [now Boston Scientific] “Tele- mode. (Operation of the Aries in Manual and
wire” transmitter). the Datascope 90 in Manual-fill mode will
1.24 Gas Supplies. Check pressure of gas tanks; disable leak alarms.)
make sure that the location of spares is pla- Datascope and Mansfield (now Boston Scientific)
carded on the unit. If helium pressure is below pumps. Withdraw gas in 1 cc increments until
250 psi or if the IABPs indicate that the gas is a leak alarm sounds. Typically, 11 to 12 cc of
low, replace the gas tanks with full tanks and gas must be withdrawn before the units will
arrange to have them refilled. If CO2 is used alarm. The Aries leak alarm circuitry is de-
with your unit, tanks should be replaced if the signed to trigger if the system detects a gas
pressure is below 850 psi. (Since CO2 maintains leak rate exceeding 3 cc per min. Test the unit
a constant pressure of 850 psi at room tempera- by withdrawing gas at a rate of approximately
ture until all the liquid is converted to gas, a 4 cc per min to verify that the alarm is operat-
pressure of less than 850 indicates that replace- ing. (At leak rates of 3 cc per min or less, the
ment is required.) Recheck the pressure after a Aries will automatically compensate for the
new tank is installed to verify that it is full and gas loss by repriming the system with helium.
that the gauge or meter is functioning properly. Kontron IABPs are also designed to detect
leakage by leak rate; contact Kontron or con-
2. Quantitative tests sult the operator’s manual to determine the
2.1 Grounding Resistance. Using an ohmmeter, appropriate rate for the model being tested.)
electrical safety analyzer, or multimeter with
2.6 Frequency Weaning. Check the operation of the
good resolution of fractional ohms, measure and
weaning control by applying a simulated ECG
record the resistance between the grounding pin
signal and setting the unit for 1:1 pumping;
of the power cord and exposed (unpainted and
observe the response when the setting for pump-
not anodized) metal on the chassis. We recom-
ing frequency is changed to alternate settings
mend a maximum of 0.5 Ω. If the system is
(e.g., 1:2, 1:3). Verify that the frequency is what
modular, verify grounding of the mainframe and
is indicated on the control knob position.
each module. If the device has an accessory out-
let, check its grounding to the main power cord. 2.7 Triggering/Timing. Using the aortic simulator
and an ECG simulator, confirm the proper op-
2.2 Leakage Current. Measure chassis current to
eration of the controls for timing and triggering
ground with the grounding conductor temporar-
of the balloon pumping on each unit. Set the
ily opened. Operate the device in all normal
ECG simulator to a heart rate of 90 bpm and
modes, including on, standby, and off, and record
observe the ECG signal on a monitor. Set timing
the maximum leakage current. Leakage current
controls for several settings and confirm changes
should be 300 µA or less.
in the balloon inflation point, inflation duration,
2.3 Pressure Monitor. Follow Item 2.10 in Blood and the deflation point.
Pressure Monitors Procedure/Checklist 434.
2.8 Driving System. Using a 40 cc balloon in the
2.4 ECG Monitor. Follow ECG Monitors Procedure/ aortic simulator, confirm proper vacuum and
Checklist 409. (If a pacemaker is incorporated pressure levels during operation at high heart
and is intended to be used, also follow External rates. Balloon should completely deflate and
Pacemakers Procedure/Checklist 418.) inflate (depending on timing control position)
even at high rates (e.g., 120 bpm).
2.5 Leak Detector. Using the aortic simulator, insert
a T-piece in the balloon catheter and connect a 2.10 Volume Displacement. Set the IABP to fully in-
25 cc syringe to the third port on the T. Be sure flate the 40 cc balloon in the simulator. Leave
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Intra-Aortic Balloon Pumps
the chamber open to the atmosphere, start the 434, External Pacemakers Procedure/Checklist 418).
pump, and observe the fluid displaced in the In addition, perform the following test.
simulator. It should be within 10% of the set-
ting. Check displacement again at volumes of 30 4.1 Compatibility with ECG and BP monitors. We
and 20 cc. (Run the test with a low trigger rate have received several reports of difficulties users
to aid in measuring the displacement.) Close the have experienced when trying to interface moni-
chamber to the atmosphere and increase pres- tors with IABPs. While we generally recommend
sure in the simulator to 40 and then to 60 mm against slaving IABPs off separate patient moni-
Hg. Observe the displaced volume when fully toring systems, we recognize that this is a rela-
inflating the balloon. If significant decreases in tively common practice. If your hospital
displaced volume occur (40%), the unit may not interfaces IABPs with monitors, verify that the
pump effectively. Contact the manufacturer. IABPs purchased are compatible with the moni-
tors to which they may be connected. Using an
3. Preventive maintenance ECG or arterial pressure waveform simulator,
3.1 Clean the exterior. connect IABPs to monitors as they are commonly
connected in your hospital and attempt to trigger
3.2 Lubricate per the manufacturer’s instructions. the pump. (This type of test will not guarantee
equipment compatibility, but should identify
3.4 Replace pump diaphragms, valves, gaskets, gas
units that are grossly incompatible. As further
line filters, ventilation filters, safety chambers,
verification, contact the IABP manufacturer to
and diaphragm isolators, if needed.
obtain its recommendations.)
Check the number of hours of use since the last
inspection and the hours of use on safety chambers
(Datascope), VLDs (Aries), or diaphragm isolators
Before returning to use
(Mansfield/Boston Scientific). Replace these accord- Make sure controls are set at normal positions and
ing to the manufacturer’s recommendations (Aries that alarm volumes, if adjustable, are set loud enough
every 2,000 hours or every year; Datascope every 1,000 to be heard in the clinical setting. Verify that cooling
hours or by the expiration date; Mansfield/Boston Sci- fans are drawing air through the console housing once
entific every 250 hours). On the inspection form, note the panels are back in place. Be sure that the battery
the date installed and the hour meter reading at instal- is charged or the unit is charging. (Note: After running
lation. Be sure clinical personnel know how to change the unit on battery during this inspection procedure,
these components. it is prudent to allow the IABP to fully recharge before
returning the unit to use. Be sure that an alternate
4. Acceptance tests IABP is available during the interim for clinical use.)
In addition to the tests described in the major in- Place a CAUTION tag in a prominent position so that
spection procedure, conduct the appropriate tests in the next user will be careful to verify control settings,
the General Devices Procedure/Checklist 438 and ac- setup, and function before using. If any gas hoses were
ceptance tests for ECG and blood pressure monitors removed or replaced during inspection or servicing, be
and pacemakers (ECG Monitors Procedure/Checklist sure to verify that the unit works properly by attaching
409, Blood Pressure Monitors Procedure/Checklist and pumping a 40 cc balloon in the aortic simulator.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Form 439-0595
Isolated Power Systems
Used For:
Isolated Power Systems [15-817]
Line Isolation Monitors [12-361]
Also Called: Isolated power centers
Commonly Used In: Operating rooms and special care areas
Scope: Applies to isolated power systems with dynamic line isolation monitors; in addition, most items are
applicable to older static ground fault detectors, which usually do not have meters to monitor the total hazard
index but which will give audible and/or visual indication after the limit has been exceeded (exceptions noted
in the text)
Risk Level: ECRI Recommended, Low; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 6 months months . hours
Minor NA months . hours
Overview required for all installed systems, even in areas in
which they are not currently required.
Isolated power systems are nonspecialized power dis-
Once isolated power systems are installed, their
tribution systems in which neither load conductor is
performance is generally taken for granted, and deg-
directly grounded and a detection device (a line isola-
radation in isolation can go unnoticed. The front-panel
tion monitor [LIM] or ground fault detector) is incor-
test button and the alarms on many systems will
porated to determine the extent of degradation of
indicate certain faults. However, we have examined
isolation. These systems have been widely installed in
isolated power systems in which even these features
operating rooms and may also be found in other areas
were not functioning properly.
of the hospital (e.g., critical care units, special proce-
dures laboratories, emergency rooms). Until recently, NFPA requirements call for a monthly test that can
codes and standards have required their installation be easily accomplished using the front-panel test button.
in all anesthetizing locations. The requirements also call for a more thorough inspec-
tion when the systems are first installed, after any
Although appropriate applications of isolated power required maintenance, and semiannually thereafter.
systems continue to be debated, these systems are Our inspection procedure meets these requirements.
currently required in operating rooms only if the oper-
ating room is not designated as a nonflammable anes- The term “total hazard index” is used throughout this
thetizing location. Isolated power systems or procedure to refer to the meter reading on the LIM. This
alternative protective mechanisms are also required in term is commonly used to denote the current that the
“wet” (as defined in NFPA 99, 1993 Edition, Section meter predicts will flow through a line-to-ground short,
3-5.2.4) locations (such as hydrotherapy areas). Peri- should one develop. The total hazard index is the greater
odic inspection and appropriate record keeping is of the currents measured when a leakage current meter
009081 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
439-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
is connected, in turn, between each load conductor and and in areas distant from the testing site, any device
ground. used to determine ground quality or grounding re-
sistance on occupied patient care areas must limit
The terms “Line 1” and “Line 2” are used to refer to the output to 500 mV RMS [1.4 V peak-to-peak] or
the power-carrying (load) conductors of an isolated 1.4 VDC; several test devices using different meas-
system. The designation is strictly arbitrary and may urement methodologies are available; any of these
not appear on the wiring itself within the system. It special-purpose devices, or simply an ohmmeter, is
serves merely to establish a polarity convention. In satisfactory, so long as it meets the above output
newer systems, one line is wired with orange insulated limits and has adequate resolution and accuracy for
wire; the other line has brown insulation. the test; for periodic measurement in existing con-
struction, the measurement current can be either
Citations from Health Devices AC or DC; an AC measuring source is required for
Isolated power systems [Evaluation], 1974 Aug-Sep; postconstruction tests)
3:243-58.
Parallel-blade receptacle tension tester (optional)
Electrical safety analyzers [Evaluation], 1988 Oct; Long lead with probe (long enough to reach from a
17:283-309. control grounding point to all areas of the room)
Isolated power systems [User Experience NetworkTM],
1988 May; 17:170-1. Special precautions
Electrical outlets in anesthetizing locations, 1993 Aug- Because checking isolated power requires that
Sep; 22:420. measurements be made on energized power lines, it is
possible for personnel to contact full line voltage. Iso-
Test apparatus and supplies lated power systems deliver substantial currents
Isolated power system analyzer (optional for routine through line-to-line contacts, and, depending on the
inspections); can be a stand-alone device or one that condition of the system, contacts from line to ground
connects to a leakage current meter, electrical may yield hazardous currents. Exercise the same pre-
safety analyzer, or voltmeter (see Special Precau- cautions used when testing or working with a conven-
tions and Health Devices 1988 Oct; 16:283-309); if tional grounded system. We strongly recommend that
used, many of the following items will not be neces- isolated power systems be inspected by a team of at
sary; for routine major inspections, a safely con- least two people so that, in the event of an accident,
structed test fixture with a single resistor (2W) and a one can summon help or begin CPR. The second per-
three-position switch — Line 1 to ground; off; Line 2 son will also prove invaluable for testing remote indi-
to ground — can be used (resistance value specified cator panels and circuit breakers.
in Item 7)
In the past, it was necessary to use separate meters
AC voltmeter for measuring line voltage and variable resistances that were interconnected
Leakage current meter or voltmeter capable of through a variety of test leads and adapters with the
measuring 10 to 500 mV isolated power system by the person(s) doing the in-
spection. Several manufacturers currently make de-
Adapters that plug into the power receptacles (e.g., vices that can be used in conjunction with electrical
parallel blade, twist-lock, explosion proof, x-ray) safety analyzers, leakage current meters, and volt-
used in the systems to be inspected, and allow safe meters to inspect isolated power systems. The use of
connection to test equipment without exposed con- such devices significantly decreases the risk of shock,
ductive surfaces that could pose a shock hazard expedites the inspection process, and alleviates the
Adapters that plug into the power receptacles (e.g., need for many of the previously required extra wires
twist-lock, explosion proof, x-ray) used in the system and adapters. Hospitals that intend to inspect isolated
that have an exposed ground connection and can be power systems on a regular basis should purchase and
hooked to a trouble light or some other load to verify use these types of devices.
the presence of AC power (120-240 V)
Never test isolated power supplies that serve oper-
Grounding cable that plugs into special grounding ating rooms, catheterization labs, or special proce-
receptacles used in the system to be checked dures rooms while procedures are underway. If it is
Ground resistance ohmmeter (to avoid risk to pa- necessary to test systems in other areas of the hos-
tients in the area in which testing is being conducted pital while patients are present, check with clinical
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Isolated Power Systems
personnel to ensure that tripped circuit breakers will pivots to nominal zero. (Note: The left end of the
not compromise patient support or safety in the area. scale corresponding to the de-energized meter
may not be labeled “0.”)
Procedure 4. Alarms and Silencing Feature. Most LIMs have at
The Universal Inspection Form is not applicable to least two buttons or switches — one to test the
this procedure. Use the special Isolated Power System alarms and one to silence the audible alarms.
Form 439. Actuate both to verify proper function. Record the
reading on the LIM when the alarm test button is
For new installations, fill in the required identifica-
actuated. This value can be helpful in diagnosing
tion information at the top of the form. This includes
failures in the LIM (normally, it should advance to
nameplate data on the isolated power system, location
the trip level). When the alarm-silence button is
of remote indicators and alarms, and type of power
actuated, there should be a visible indication
receptacle. In addition, list all fixed or permanently
either that the system is still in alarm or that the
connected equipment (e.g., overhead lighting, x-ray
alarm is silenced. Remember to test all remote
view boxes, clocks) that is powered by the isolated
indicators. Be sure that the audible and visual
power system. A box is provided on the form to sketch
alarms reset following this test. The audible alarm
the layout of the room or area served by the isolated
may or may not automatically reset upon resolu-
power system to identify the location of defective com-
tion of the alarm condition.
ponents or receptacles. The sketch should provide
some orientation (e.g., location of bed or operating 5. Fuses. If the LIM has accessible fuses, examine
table, doors). (An otherwise blank form, with this in- them for condition and rating. Their rating
formation filled in, can be copied for routine inspec- should be placarded near the fuseholder. If it is
tions; verify that no changes have been made since the not placarded, do not assume that a fuse of the
acceptance inspection. The sketch is not required if correct value is installed; check the specifica-
receptacles are assigned identification numbers and tions for the LIM. Be sure that the fuseholders
labeled during acceptance testing.) are in good condition.
Items 1 through 9 constitute a simple operational 6. Circuit Breakers. Examine and manually oper-
check of the system to be performed routinely. These ate each primary and secondary circuit breaker
and the remaining items constitute an acceptance pro- associated with the isolated power system. If the
cedure. Although they are listed separately for clarity, circuit-breaker panel is usually locked, deter-
checks of several items (e.g., lights, meters, alarms) mine whether this is a necessary precaution. In
can be performed simultaneously. most cases, especially if the breakers are located
in the same room that they serve, a locked
Qualitative and quantitative tests breaker panel is inappropriate because it will
1. Physical Condition. Check the physical condi- delay restoration of power following a fault.
tion of display and circuit-breaker panels, in- 7. Confirmation of LIM Function. (Note: This test
cluding indicators, meters, and circuit breakers. does not confirm LIM accuracy and does not need
Verify that they are not cracked or broken, that to be performed during acceptance testing when
they do not show signs of fluid entry, and that Item 10 is conducted.) Connect a 24 kΩ resistance
viewing and access are not obstructed. (for 120 V system or 48 kΩ for a 240 V system)
2. Lights. Check all indicator lights, including any between Line 1 and ground. Repeat the test with
remote indicators, to verify that they are func- this same resistance connected between Line 2
tioning. It may be necessary to actuate the test and ground. (An isolated power analyzer or a
feature to check certain lights. Ensure that col- calibrated, adjustable resistance can be used for
ored lenses over the indicator lights are intact. this test. However, it may be more convenient to
If a light is burned out, replace it or note the type make a test fixture by wiring an appropriate plug
on the inspection form to facilitate replacement. with a 24, or 48, kΩ resistor that can be switched
from ground to Line 1 or Line 2.) Confirm that
3. Meters. Be sure that the LIM meter is in good the visual and audible alarm indicators are acti-
condition. The needle should not be bent and vated for each of these connections. This test
should advance smoothly when the test button confirms that an alarm will occur for a fault
is pressed. If it is possible to disable the LIM that would result in a 5 mA hazard current. A
(e.g., by removing its fuse), check that the needle proportionately higher resistance may be used
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
for confirmation at the 2 mA level (e.g., 60 kΩ Verify that each receptacle has power by plug-
for 120 V systems, 120 kΩ for 240 V systems). If ging a lamp or trouble light into the receptacle
an analyzer with adjustable trip point adjust- (a 240 V bulb is needed for x-ray outlets). Check
ment is used, the alarm should activate at resis- the grounding contact of each receptacle. A du-
tances at or above those specified here. If leakage plex to locking receptacle adapter (or duplex to
readings are used, the alarm should activate at x-ray) may be required. It may be possible to
readings no greater than 5 mA (or 2 mA for combine the grounding contact test with the
2 mA LIM). power test if a light with an accessible grounding
point is used.
8. Receptacles. Check explosion-proof and x-ray
receptacles. Replace chipped or broken recepta- For new construction, NFPA 99 requires
cles and cracked faceplates. Parallel-blade du- that the voltage limit between a reference
plex receptacles can be checked either as part of point and grounding contact of each receptacle
the isolated power inspection procedure or dur- in the patient vicinity not exceed 20 mV. In
ing routine inspection of duplex receptacles in existing construction, the voltage should not
that area of the hospital (see Electrical Recepta- exceed 500 mV in general care areas and 40 mV
cles Procedure/Form 437). in critical care areas. However, voltages in
modern construction are usually <10 mV; volt-
It is only necessary to record any defective ages >20 mV may indicate a deteriorating con-
outlets that are found. If all outlets are satisfac- dition and should be investigated. It should be
tory, check Pass. If the test is postponed because understood that these limits are not precise,
it will be included as part of the receptacle in- and differences of <20% should be considered
spection procedure, put a line through both the insignificant.
Pass and Fail columns.
Measure the retention force of parallel- Measure ground potentials with a voltmeter
blade outlets with a receptacle tension tester. or leakage current meter. Leakage current read-
Be sure that withdrawal of the tester from the ings can be converted to millivolts (mV) if the
outlet is straight and smooth. Retention force leakage current meter’s impedance is known.
on the ground prong must be 4 oz or more. (Most leakage current meters have a 1,000 Ω
Although measurement of retention force on impedance at line frequency; the reading in µA
the power-carrying prongs is not required, we is then numerically equivalent to the voltage in
recommend that this be measured. A reten- mV.) Connect one lead of the meter to a reference
tion force of 4 oz is also adequate for these ground point that is known to be securely
prongs, and forces of 2 to 4 oz are satisfactory grounded. It is usually most convenient to use
if the plug brand in use tends to stabilize at the ground contact of one receptacle, but a
this value and does not continue to deteriorate. ground plug or structural member can also be
Replace any outlet with less than 2 oz reten- used. Do not use the cover plate screw, because
tion force on any prong. (See Procedure/ Form this may not be adequately grounded. Connect
437 for additional information.) the other lead to the ground contact of each
receptacle in turn.
A quantitative test of contact quality cannot
be made in most locking receptacles. Instead, Measure the resistance between the ground-
make a qualitative test of the power contacts ing terminal of the receptacle (accessed through
by plugging a movable floor lamp or trouble the adapter) and ground, and verify that it is <0.2
light into the receptacle, either directly or Ω (or 0.1 Ω in new construction) and does not
through an adapter (a 240 V bulb will be vary as the plug is jiggled in the receptacle.
needed for x-ray outlets). Jiggle the plug and
pull on it after it has been inserted and notice 9. Grounding Jacks. Examine all installed
whether the light flickers. The insertion and grounding jacks for general physical condition.
removal of the plug should be smooth. If the Insert a cable intended for that type of receptacle
receptacle is explosion proof, check that the to make sure that there are no obstructions (e.g.,
lamp does not go on until the appropriate ac- broken locking pins) in the receptacle or other
tion is taken (e.g., twisting the plug in the damage that prevents insertion or retention of
receptacle, rotating the cover plate). the plug.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Isolated Power Systems
Check ground potentials and resistance as (24 to 48 kΩ for a 5 mA, 120 V system). If a
described in Item 8; the same criteria apply. resistance higher than this value activates an
alarm, it is indicative of inadequate isolation. This
Acceptance tests can result in nuisance alarms.
Items 10-14 should be done only after the system is If resistances significantly below the expected
first installed or if major modifications or repair have value are required to generate an alarm, then
been performed on the system. malfunction or miscalibration of the line isola-
tion monitor is likely; this condition should be
10. Line Voltage. Line voltage tests are not required
corrected before the inspection continues.
by NFPA 99. These tests should be performed
following new construction, renovations, or ma- Static LIMs may not alarm until the resis-
jor repairs to the electrical distribution system tance is about 20 kΩ, and LIMs with other alarm
to ensure that voltage taps are set correctly. levels may be encountered. Examine the speci-
Testing after typical loads are applied or testing fications of these special systems; the systems
in existing facilities may indicate poor wiring or should operate within those specifications.
inadequate system capacity.
(If the hazard index is above 5 mA, do not
Measure and record the output voltage of the attempt the next step [measuring total hazard
system between Line 1 and Line 2. The meas- current] unless your meter is protected against
ured value should conform, within reasonable line voltage.) Measure the resulting total hazard
limits, to the value specified on the nameplate. current with the resistance in place on Line 1 by
Any significant deviation requires further inves- switching the analyzer meter to read from Line
tigation. However, it may reflect the relatively 2 to ground (the LIM meter will go to full scale).
poor accuracy of many AC voltmeters, so check Record this current reading. This current
your meter before blaming the system. should not exceed 2 mA (5 mA on 5 mA systems)
and should agree, within 20%, with the LIM
11. Alarm Levels. This test verifies that the alarm
meter reading before the leakage current meter
will function when a suitable fault from one line
was connected. To satisfy current codes, it
to ground occurs, verifies the accuracy of the LIM
should not be, under any circumstances, signifi-
meter, and provides a measure of the degree of
cantly higher than 5 mA.
isolation from each line to ground.
Static ground fault detectors may have alarm
Unplug all cord-connected equipment and
levels above 5 mA or more and may be beyond
turn off all fixed equipment (e.g., x-ray view box)
the range of some meters. In addition, static
from the system. Connect the analyzer and set it
detectors do not recognize balanced faults.
to apply a resistance between Line 1 and ground.
Reduce the resistance from a high value (e.g., Older dynamic line isolation monitors scan
200 kΩ) until the alarm sounds. Record this between Lines 1 and 2 at rates that can introduce
resistance value and the total hazard index (LIM marked fluctuations in meter readings. When
meter reading). the scanning rate is slow enough that two dis-
tinct readings can be distinguished on the meter,
If the analyzer does not indicate the actual record the greater of the two values. Otherwise,
resistance used during this particular test, it is record the average current.
not imperative that this value be obtained and
recorded. However, it is important to perform Repeat this sequence of tests, connecting the
the procedure for determining system leakage resistance from Line 2 to ground, adjusting it
(Item 12) and to record system leakage values. until the alarm sounds, and measuring the total
The resistance between a single power line and hazard current from Line 1 to ground with a
ground that can cause an alarm varies, depend- leakage current meter.
ing on the isolation of that line. The resistance
required to cause an alarm and the system leak- 12. System Leakage. These measurements check
age current are both indications of the isolation system integrity and give further information on
of the system, and either value is sufficient. LIM meter accuracy. While not essential if Item
10 is performed, the information obtained may
For a 2 mA, 120 V system, resistance values be helpful in assessing a new installation and in
between 60 and 120 kΩ indicate adequate isolation future troubleshooting. Comparing the readings
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
with values obtained in previous inspections mA for a 120 V system (1.2 mA for a 240 V
may indicate degradation of the isolation of system).
transformers, wiring, or other components.
13. Grounding of Exposed Metal. NFPA 99-1993
Record the hazard index indicated on the LIM calls for testing of installed, permanently at-
with the isolated power system on, all cord-con- tached, electrically conductive surfaces that
nected devices unplugged, and individual branch might become electrically energized and that
circuit breakers or switches integral to the unit might be touched by the patient or persons
turned on. Installed lighting powered by the touching the patient. Testing is required follow-
system (e.g., overhead surgical lights, x-ray view ing significant modifications and is recom-
boxes) should be turned on or off, whichever mended (but not required) at one-year intervals.
yields the higher hazard index. However, NEC (1993) no longer requires ground-
ing of such surfaces. We recommend performing
Measure the system leakage with the line this test after new construction and significant
isolation monitor connected. Connect the leak- modifications.
age current meter between Line 1 and ground Tests and criteria are the same as for Item 8.
and note the reading. This represents leakage It is not necessary to be concerned about resis-
caused by impedance from Line 2 to ground. tance to ground of isolated exposed metal as long
Repeat the measurement with the meter con- as the potentials measured above are accept-
nected between Line 2 and ground. Record the ably low.
two values and compare the greater one to the
reading recorded for the LIM meter. A signifi- 14. Circuit Breaker Function and Labeling. Deter-
cant difference suggests a line isolation moni- mine the correspondence between circuit break-
tor malfunction. To ensure that there will be ers and receptacles. Turn off all secondary
adequate leeway on the system to cope with circuit breakers and plug a light, voltmeter, or
connected loads, this value should be <1 mA for other indicating device into one receptacle. Mo-
2 mA systems and <2.5 mA for 5 mA systems. mentarily turn on one breaker at a time until the
breaker controlling the receptacle is identified.
If the fuses of the LIM can be removed, if the Repeat this for all receptacles served by the
grounding wire of the LIM can be disconnected, isolated power system. As you go through the
or if the breaker serving the LIM can be turned area, check that the receptacles and breakers are
off, repeat system leakage measurements. This labeled (preferably by numbering) to indicate the
value measures the collective leakage of in- relationship between them. This can facilitate
stalled wiring, transformer, and associated restoration of power should a breaker trip. If
components, but without the degradation of they are not labeled, arrange to permanently tag
isolation caused by the LIM; thus, it is a better each receptacle with the number of the circuit
indication of wiring degradation. NFPA 99 breaker that controls it. If more than one recep-
states that the isolation must be >200,000 Ω; tacle is served by a breaker, use letter suffixes
therefore, system leakage (mA) should be <0.6 (e.g., 8A, 8B).
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Isolated Power Systems
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 466-0595
Laparoscopic Insufflators
Used For:
Insufflators, Laparoscopic [16-849]
Also Called: CO2 Insufflators
Commonly Used In: Operating rooms, short procedure and ambulatory surgery areas
Scope: Applies to pneumatically and electronically controlled insufflators intended for introduction of CO2
or N2O gas into the peritoneal space. Does not apply to insufflators for hysteroflation (i.e., insufflation of the
uterus).
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview can stabilize, allowing the pressure in the transducer
inside the insufflator to equalize with the abdominal
Insufflators are used to establish and maintain the pressure. Both pneumatic and electronic insufflators
pneumoperitoneum during laparoscopic procedures. feature controls for setting the pressure and maximum
Gas, typically CO2, introduced into the peritoneal cav- flow rate. They feature displays, gauges, or other indi-
ity distends the abdominal wall to provide a viewing cators for set and detected abdominal pressure and
and working space within the abdomen. flow, volume of gas consumed, and external gas cylin-
der pressure or volume remaining. In pneumatic insuf-
The primary function of the insufflator is to act as flators, flow is typically specified as high or low. In
a pressure-controlled gas flow regulator. The insuffla- electronic insufflators, flow rates are specified either
tor takes in compressed gas from a supply cylinder as a time-averaged flow or as an instantaneous flow.
(700 to 850 psi) or wall outlet (50 to 100 psi) and The maximum flow possible from a given insufflator
delivers it to the patient, typically at 10 to 15 mm Hg varies depending on flow resistance introduced by in-
(0.2 to 0.3 psi). In pneumatic insufflators, abdominal line tubing filters and by the stopcock connection
pressure control is accomplished by limiting the pres- through which the insufflator is connected to the
sure of gas delivered to the patient. Electronic insuf- patient.
flators typically deliver gas at a pressure higher than
that desired in the pneumoperitoneum; these units
limit abdominal pressure by slowing and then sus- Citations from Health Devices
pending flow when intermittent abdominal pressure
measurements approach and reach a user-selected Laparoscopic insufflators [Evaluation], 1992 May;
pressure. For electronic insufflators to accurately 21:143-73.
measure abdominal pressure, flow is briefly sus-
pended so that pressure in the abdomen, insufflator Entry of abdominal fluids into laparoscopic insuffla-
tubing, and the patient outlet port of the insufflator tors [Hazard], 1992 May; 21:180-1.
234107 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
466-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Fatal gas embolism caused by overpressurization dur- damage is near one end, cut out the defective
ing laparoscopic use of argon enhanced coagulation portion.
[Hazard], 1994 Jun; 23:257-9.
1.6 Strain Reliefs. Examine the strain reliefs at
High-flow laparoscopic insufflators [Evaluation], 1995 both ends of the line cord. Be sure that they hold
Jul; 24:252-85. the cord securely. If the line cord is detachable
(by the user), affix the cord to the unit so that it
Test apparatus and supplies cannot be removed by the operator. (See Health
Devices 1993 May-Jun; 22:301-3.)
Leakage current meter or electrical safety analyzer
Ground resistance ohmmeter 1.7 Circuit Breaker/Fuse. If the device has an ex-
ternal circuit breaker, check that it operates
Pressure meter or gauge (range 0 to 75 mm Hg; freely. If the device is protected by an external
mercury manometers are not suitable) fuse, check its value and type against that
Large-bore (20 ga or larger) hypodermic needle marked on the chassis and ensure that a spare
is provided.
Empty 500 mL and 3 L (one each) IV and/or anes-
thesia solution bags with at least two ports 1.8 Tubes/Hoses. Check the condition of reusable
Trocar cannula or IV stopcock patient tubing and gas-supply hoses. Be sure
that they are not cracked, kinked, or dirty.
Stopwatch or watch with second hand
1.10 Pneumatic Connectors. Verify that the high-
Procedure pressure hose is pin-indexed for the appropriate
gas (e.g., CO2 or N2O).
Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and Examine all external gas fittings and connec-
service manuals; be sure that you understand how to tors, as well as electrical cable connectors, for
operate the equipment, the significance of each control general condition. Electrical contact pins or sur-
and indicator, and the alarm capabilities. Also deter- faces should be straight, clean, and bright. Verify
mine whether any special inspection or preventive that leads and electrodes are firmly gripped in
maintenance procedures or frequencies are recom- their appropriate connectors. Gas fittings should
mended by the manufacturer. be tight and should not leak.
1. Qualitative tests 1.11 Electrodes/Transducers. Confirm that any nec-
essary electrodes and/or transducers are on
1.1 Chassis/Housing. Examine the exterior of the hand, and check their physical condition.
unit for cleanliness and general physical condi-
tion. Be sure that plastic housings are intact, 1.12 Filters. Check the condition of internal gas fil-
that all hardware is present and tight, and that ters. Clean or replace as appropriate, and indi-
there are no signs of spilled liquids or other cate this in Section 3 of the inspection form.
serious abuse. Inspect the gas outlet port for Follow the manufacturer’s recommended inter-
evidence of fluid entry, which can indicate con- val for service of internal filters (typically 2
tamination by body fluids. years) and instructions for replacement.
1.2 Mount/Fasteners. If the device is mounted on a 1.13 Controls/Switches. Before changing any con-
stand or cart, examine the condition of the trols or alarm limits, check their positions. If any
mount. If it is attached to a wall or rests on a settings appear inordinate (e.g., a pressure con-
shelf, check the security of this attachment. trol at maximum), consider the possibility of
inappropriate clinical use or of incipient device
1.4 AC Plug/Receptacles. Examine the AC power failure. Record the setting of those controls that
plug for damage. Attempt to wiggle the blades to should be returned to their original positions
check that they are secure. Shake the plug and following the inspection.
listen for rattles that could indicate loose screws.
If any damage is suspected, open the plug and Examine all controls and switches for physical
inspect it. condition, secure mounting, and correct motion.
Check that control knobs have not slipped on
1.5 Line Cord. Inspect the cord for signs of damage. their shafts. Where a control should operate
If damaged, replace the entire cord or, if the against fixed-limit stops, check for proper
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Laparoscopic Insufflators
alignment, as well as positive stopping. During ment temporarily opened. Operate the device in
the course of the inspection, be sure to check that all normal modes, including on, standby, and off;
eachcontrol andswitchperformsitsproperfunc- record the maximum leakage current.
tion.
Measure chassis leakage current with all ac-
1.18 Indicators/Displays. During the course of the cessories normally powered from the same line
inspection, confirm the operation of all lamps, cord connected and turned on and off. This in-
indicators, meters, gauges, and visual displays cludes other equipment that is plugged into the
on the unit. Be sure that all segments of a digital primary device’s accessory receptacles, as well as
display function. equipment plugged into a multiple outlet strip
(“Waber strip”) so that all are grounded through
1.19 User Calibration. Verify that any calibration a single line or extension cord.
function operates.
Chassis leakage current to ground should be
1.20 Alarms. Induce alarm conditions to activate 300 µA or less.
audible and visual alarms. Check that any asso-
ciated interlocks function. If the unit has an 2.3 Set Pressure Accuracy. Connect the insufflator
alarm silence feature, check the method of reset to an empty 3 L solution bag. Introduce a large-
(e.g., manual or automatic) against the manufac- bore hypodermic needle through an injection
turer’s specifications. It may not be possible to port on the bag. Connect the pressure meter or
check out all alarms at this time, since some may gauge to the hypodermic needle, and measure
require abnormal operating conditions that will the gas pressure in the bag after it has stabilized.
be simulated later in this procedure. Measurements should be taken at maximum,
minimum, and a pressure setting in the range of
1.21 Audible Signals. Operate the device to activate 12 to 15 mm Hg and should be within 3 mm Hg
any audible signals. Confirm appropriate vol- of the pressure setting.
ume, as well as the operation of a volume control
if so equipped. If audible alarms have been si- 2.4 Displayed Pressure Accuracy. During the pre-
lenced or the volume set too low, alert clinical ceding test (Item 2.3), compare the displayed
staff to the importance of keeping alarms at the pressure with pressure measured with the
appropriate level. pressure meter or gauge; displayed pressure
should be within 3 mm Hg of the measured
1.22 Labeling. Check that all necessary placards, la- pressure. Manually compress the bag to pro-
bels, conversion charts, and instruction cards duce pressure in excess of the set pressure, and
are present and legible. verify that displayed pressure remains within
3 mm Hg or 10% of measured pressure, which-
2. Quantitative tests
ever is greater.
2.1 Grounding Resistance. For line-powered units,
use an ohmmeter, electrical safety analyzer, or 2.5 Pressure Relief Mechanism. An insufflator
multimeter with good resolution of fractional should limit delivered pressure to a manufac-
ohms to measure and record the resistance be- turer-specified maximum value. In addition to a
tween the grounding pin of the power cord and pressure-relief valve, some units also have vents
exposed (unpainted and not anodized) metal on that are electronically opened if the detected
the chassis. We recommend a maximum of 0.5 Ω. pressure exceeds a threshold value (e.g., 30 mm
If the system is modular or composed of separate Hg) or if the detected pressure exceeds the se-
components, verify grounding of the mainframe lected pressure by a certain value. In many
and each module or component. If the device is cases, these vents activate after a delay of sev-
double insulated, grounding resistance need not eral seconds. With the insufflator connected to a
be measured; indicate “DI” instead of the ground filled 3 L solution bag, manually compress the
resistance value. bag so that pressure is slowly increased 5 mm Hg
at a time until pressure relief is activated. Note
If the device has an accessory receptacle, the bag pressure at which pressure relief occurs
check its grounding to the main power cord. as indicated by the pressure meter or gauge also
connected to the bag.
2.2 Leakage Current. For line-powered units, meas-
ure chassis leakage current to ground with the 2.6 High-Pressure Alarms. During the preceding
grounding conductor of plug-connected equip- two tests (Items 2.4 and 2.5), note the bag
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
pressures at which intermittent and continuous set intended for use with the insufflator, and
audible alarms and visual indicators are acti- compare it to the flow established for that unit
vated. during acceptance testing. Insufflators should
have a setting that delivers flow in the range of
2.10 Maximum Flow. With the insufflator set to its 1 to 2 L/min. For this test, compute the flow using
maximum flow setting, measure the time re- the following formula:
quired to fill a 3 L solution bag to a typical
pressure setting (e.g., 15 mm Hg) through the (0.5 L) × (60 sec⁄min)
flow (L⁄min) =
tubing/filter set intended for use with the insuf- fill time (sec)
flator, and compare it to the flow established for
that unit during acceptance testing. For this test, 3. Preventive Maintenance
compute the flow using the following formula: 3.1 Clean the exterior (interior, if required).
(3 L) × (60 min)
sec⁄
3.2 Lubricate per the manufacturer’s instructions.
flow (L⁄min) =
fill time (sec)
3.3 Calibrate pressure settings, if required.
(This measurement may differ markedly from
the manufacturer’s specified maximum flow rate 3.4 Replace filters, if required.
if it is specified as an instantaneous flow or is not
4. Acceptance tests
adjusted for flow resistance of the tubing set and
filter. It is important to minimize flow resistance Conduct major inspection tests for this procedure
in the connection between the insufflator tubing and the appropriate tests in the General Devices Pro-
set and the reservoir bag [e.g., do not use a cedure/Checklist 438.
Veress or hypodermic needle for this connection].
If a trocar cannula or IV stopcock is used for this Before returning to use
connection, it should be maintained as a perma- Ensure that all controls are set properly. Set alarms
nent test device because flow resistance of stop- loud enough to alert personnel in the area in which the
cocks and cannulae varies significantly.) device will be used. Other controls should be in their
normal pre-use positions.
2.11 Low Flow. With the insufflator set to minimum
flow setting, measure the time required to fill a Attach a Caution tag in a prominent position so that
500 mL IV reservoir bag to a typical pressure the user will be aware that control settings may have
setting (e.g., 15 mm Hg) through the tubing/filter been changed.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 467-0595
Mammography Units
Used For:
Radiographic Units, Mammographic [12-425]
Commonly Used In: Radiology departments, breast clinics
Scope: Applies to mobile and stationary screening x-ray mammography units that use a screen-film receptor;
xeroradiographic and digital receptor systems are not covered here specifically, although many of the following
tests will apply to these systems; biopsy systems are also not covered in this procedure
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview beam from the cathode and emits x-rays. Mo, alumi-
num (Al), and/or Rh filters are placed in the path of
Mammography units use x-rays to produce a film image the x-ray beam to absorb unwanted x-rays. The x-rays
of the breast (a mammogram) that provides informa- that pass through the filter are shaped by a collima-
tion about breast morphology, normal anatomy, and tor or by cone apertures. Currently, five target/filter
gross pathology. Mammography is primarily used to combinations for screen-film mammography are
detect and diagnose breast cancer, as well as to evaluate available: Mo/Mo, W/Mo, W/Rh, Mo/Rh, and Rh/Rh.
palpable masses and nonpalpable breast lesions. The target/filter combination selected for imaging
depends on the thickness and density of the breast
A mammographic radiographic system consists of after compression.
an x-ray generator, an x-ray tube, a positioning assem-
bly, a compression system, a Bucky grid to reduce
An automatic exposure control (AEC) device is
scatter radiation, a radiation shield, and an image
used to terminate x-ray generation when a radiation
recording system. X-ray generators for mammography
sensor behind the film cassette senses the proper
are usually high-frequency (they convert the 50- or
exposure. AEC devices can automatically compen-
60-cycle input voltage to a frequency as high as 100
sate for technique variance and patient anatomy
kilohertz) or constant-potential (they supply a ripple-
(breast thickness), thereby reducing radiation expo-
free, continuous voltage to the x-ray tube, regardless
sure and retakes.
of the input power). For screen-film mammography,
the kilovoltage (kV) settings range from 20 to 35 kV;
this narrow range accentuates the subtle density dif- The positioning assembly is capable of vertical and
ferences in breast tissue. rotational movement to adjust for different patient
heights and breast sizes and to permit the acquisition
X-rays are produced by the x-ray tube, which usually of images from various angles around the breast
has a rotating anode that dissipates heat produced dur- (e.g., craniocaudal, mediolateral). A compression sys-
ing exposure. A molybdenum (Mo), tungsten (W), or tem, either automatic or manually operated, is used to
rhodium (Rh) target on the anode receives the electron uniformly reduce the thickness of the breast to facilitate
237588 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
467-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
x-ray beam penetration and maximize the amount of Special precautions
tissue imaged.
Wear a lead apron during all radiation testing and
In screen-film mammography, the image recording maintain a safe distance between yourself and the
system uses high-detail fluorescent screens that con- x-ray tube. It should not be necessary to place hands
vert x-rays to light photons and that are in contact with or fingers in the x-ray beam; if this is unavoidable,
a single- or double-emulsion film. Xeromammography, wear lead gloves. For repeated exposures, as required
a method of electrostatic image recording using by some of the tests in this procedure, allow adequate
charged photoconductive plates, is still available on time between exposures to prevent the x-ray tube from
some mammography units. overheating. Do not remove high-voltage cables from
the wells with the power on. When removing them,
Citations from Health Devices ensure that the cables are completely discharged by
repeatedly contacting the conductor to the ground as
Mammography units [Evaluation], 1989 Jan; 18(1):3-53.
soon as the cables are removed from the wells.
Quality assurance in screening mammography [Clini-
For tests of the AEC and of image quality, it is
cal perspective], 1990 May-Jun; 19(5-6):152.
imperative that an optimally performing film proces-
Mammography units [Evaluation], 1990 May-Jun; sor be used. This film processor should be the one that
19(5-6):153-98. is normally used to process all mammograms. Also, the
technical tests should be undertaken using the same
Test apparatus and supplies screen-film combination that is used for acquiring
mammograms.
Ground resistance ohmmeter
Leakage current meter or electrical safety analyzer Procedure
Noninvasive mammographic kVp meter Before beginning an inspection, carefully read this
Noninvasive timer (may be included with the kVp procedure and the manufacturer’s instruction and
meter) service manuals; be sure that you understand how to
operate the equipment, the significance of each control
Ionization chamber with electrometer, or a combi- and indicator, and the alarm capabilities. Also deter-
nation exposure meter, capable of making exposure mine whether any special inspection or preventive
measurements in the mammography energy range maintenance procedures or frequencies are recom-
and specifically calibrated for this purpose mended by the manufacturer.
Five high-purity (>99%) aluminum filters measur-
This procedure is intended to ensure adequate sys-
ing 10 cm × 10 cm × 0.1 cm
tem performance and maintenance. It should not be
10 cm of stiff wire construed as providing full compliance with the re-
Four coins or lead markers quirements of all governmental regulations and ac-
creditation standards of professional associations.
One dozen sheets of 18 cm × 24 cm mammography Such regulations and standards may include testing
film from same batch beyond that provided below and may also require docu-
One dozen sheets of 24 cm × 30 cm mammography mentation by a certified medical physicist.
film from same batch
For acceptance testing, we strongly recommend con-
One 18 cm × 24 cm mammography cassette with tracting with a medical physicist. Acceptance testing
screen is crucial because it generates data on baseline per-
formance of the device.
One 24 cm × 30 cm mammography cassette with
screen
1. Qualitative tests
Densitometer
1.1 Chassis/Housing. Examine the exterior of the
Ten pieces of 15 cm × 15 cm × 1 cm plexiglass mammography unit for cleanliness and general
American College of Radiology (ACR) accreditation physical condition. Be sure that all hardware is
mammography phantom present and secure and that there are no signs of
serious abuse. Check the movements of the C-
Oscilloscope (calibration only) arm assembly, both for rotation and vertical
High-voltage divider (calibration only) movements, ensuring that all of its movements
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Mammography Units
are smooth and that the locks function ade- rotation or other strain. Verify that there are no
quately. Also check during these tests that the intermittent faults by flexing electrical cables
film cassette is retained securely but that it is near each end and looking for erratic operation
not difficult to insert or remove. Check the con- or by using an ohmmeter.
dition of the operator shield and the patient face
1.10 Fittings/Connectors. Examine all electrical ca-
shield.
ble connectors for general condition. Electrical
1.2 Mounts/Fasteners. Ensure that the mammog- contact pins or surfaces should be straight,
raphy unit is securely mounted on the floor so clean, and bright. Verify that leads and elec-
that it is not likely to become unstable when a trodes are firmly gripped in their appropriate
patient is leaning on the breast platform or when connectors. If keyed connectors are used, make
the technologist is moving the C-arm assembly. sure that no pins are missing and that the keying
is correct. Also, check the mechanical connec-
1.3 Casters/Brakes. For mobile mammography tions, particularly of the compression paddles
units, verify that the wheels turn and swivel, as and of the magnification platforms. Ensure that
appropriate, and look for accumulations of dirt the connections permit safe and adequate at-
and grime around the wheels. Also, check the tachment of these devices.
operation of brakes and the adequacy of the park
positions of the C-arm assembly and of any other 1.13 Controls/Switches. Before changing any con-
components likely to move during transport. trols or alarm limits, check their positions. If any
settings appear inordinate (e.g., very large preset
1.4 AC Plug/Receptacles. For line-powered mam- density change or a kVp that is too low), consider
mography units, examine the AC power plug for the possibility of inappropriate clinical use or of
damage. Attempt to wiggle the blades to check incipient device failure. Record the setting of
that they are secure. Shake the plug and listen those controls that should be returned to their
for rattles that could indicate loose screws. If any original positions following the inspection.
damage is suspected, open the plug and inspect
it. If the unit has electrical receptacles for acces- Examine all controls and switches (x-ray in-
sories (e.g., printers), verify the presence of line itiation, technique selection, filter selection, focal
power and insert an AC plug into each and check spot selection, compression and decompression
that it is held firmly. If accessories are plugged switches, preset density change, etc.) for physi-
and unplugged often, consider a full inspection cal condition, secure mounting, and correct mo-
of the receptacles. tion. Check that control knobs, if present, have
not slipped on their shafts. Where a control
1.5 Line Cord. Inspect the cord for signs of damage. should operate against fixed-limit stops, check for
If damaged, replace the entire cord or, if the proper alignment, as well as positive stopping.
damage is near one end, cut out the defective During the inspection, be sure to check that each
portion. Be sure to wire a new power cord or plug control and switch performs its proper function.
with correct polarity. Also check line cords of
battery chargers. For the radiographic exposure switches, en-
sure that they do not stick and that continuous
1.6 Strain Reliefs. Examine the strain reliefs at pressure is required to continue exposure. Re-
both ends of the line cord. Be sure that they hold lease of pressure should immediately terminate
the cord securely. exposure. Also pay close attention to the opera-
tion of the compression and decompression
1.7 Circuit Breaker/Fuse. If the device has an exter-
switches. Ensure that, where provided, automat-
nal circuit breaker, check that it operates freely. If
ic decompression follows exposure.
the device is protected by an external fuse, check
its value and type against that marked on the 1.15 Motor/Pump/Fan/Compressor. Check the phys-
chassis and ensure that a spare is provided. ical condition of the motor-driven compression
mechanism. Also, ensure that the cooling fan in the
1.9 Cables. Inspect any cables (e.g., from the AEC
tube head assembly is clean and operates ade-
detectors to the generator, cable to footswitches)
quately. Clean and lubricate if necessary and note
and their strain reliefs for general condition.
this in Items 3.1 and 3.2 of the inspection form.
Carefully examine cables to detect breaks in the
insulation and to ensure that they are gripped 1.18 Indicators/Displays. During the inspection,
securely in the connectors at each end to prevent confirm the operation of all lamps, indicators,
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
meters, gauges, and visual displays on the unit. 2.2 Leakage Current. For mobile mammography
Examples of indicators and displays are tech- units, use a safety analyzer to measure leakage
nique settings, choice of focal spots, filter in use, current. The chassis leakage current to ground
breast thickness, source-to-image distance should not exceed 300 µA. Note that for existing
(SID), and C-arm rotation indicators. Include mobile units, leakage currents of up to 500 µA are
checks of the light field in this test. deemed not to pose a hazard, but, if the leakage
current is between 300 and 500 µA, a documented
1.20 Alarms. Induce conditions to activate audible and maintenance schedule should be implemented to
visual alarms (for example, x-ray exposure, backup ensure the integrity of the grounding connection.
timer activation). Check that any associated inter- Permanently wired equipment should be tested
locks (e.g., no exposure if there is no film cassette before installation. With all grounds lifted, leak-
in the Bucky) function. If the unit has an alarm age current should not exceed 5 mA.
silence feature, check the method of reset (e.g.,
manual or automatic) against the manufacturer’s 2.3 Accuracy of kVp. Use a noninvasive kVp meter
specifications. It may not be possible to check out capable of making measurements in the mam-
all alarms at this time, since some may require mographic energy range. The kVp meter should
abnormal operating conditions (e.g., long exposure have been previously calibrated against a high-
times). Instruct users to document activation of voltage divider on the type of generator that pow-
these alarms to ensure that they are functional. ers the mammography unit. Use the kVp meter in
accordance with the recommendations of the me-
1.21 Audible Signals. Operate the device to activate ter’s manufacturer (e.g., the distance at which the
any audible signals (for example, radiographic kVp meter has to be placed).
exposure). Confirm appropriate volume.
Make measurements at a minimum of three
1.22 Labeling. Check that all necessary certification kVp settings that span the range normally used
labels, warning labels, technique charts, and at your facility. For units that have two focal
instruction cards are present and legible. spots, measurements should be made using each
focal spot at the tube current setting appropriate
1.23 Accessories. Confirm the presence and condition
for the focal spot in use. After appropriate cor-
of accessories (e.g., full and spot compression
rections have been applied to the measured kVp
paddles, grids, magnification platform, dia-
readings (e.g., for filtration), the measured kVp
phragms, and cones).
should be within ±5% of the preset kVp.
2. Quantitative tests If a consistent significant error between the
preset kVp and the measured kVp is detected,
2.1 Grounding Resistance. Using an ohmmeter, further testing with a high-voltage divider may
electrical safety analyzer, or multimeter with be required to identify the problem.
good resolution of fractional ohms, measure and
record the resistance between the ground pin (or 2.4 Timer Accuracy. Use a noninvasive timer to
the ground for hard-wired systems) and the ac- measure the accuracy of the time settings. If the
cessible conductive surfaces on the mammogra- noninvasive kVp meter also displays exposure
phy unit. The resistance should not exceed times, it is acceptable for this test. Follow the
0.5 Ω. Handswitches and footswitches that are manufacturer’s recommended technique for
powered from low voltages need not be grounded. making time measurements.
Although confirmation of grounding integrity Measure at a minimum of three time settings
provides reasonable assurance of safety, NFPA spanning the range normally used at your facility.
99 calls for voltage measurements for installed For all measurements, use a fixed tube voltage
devices in the patient vicinity. Using a voltmeter, setting of 28 kVp. If the time settings are not
measure and record the voltage between a refer- displayed on the mammography unit, calculate
ence grounding point (e.g., the grounding pin of them from the mAs values by factoring out the mA
an electrical receptacle or some other known the unit uses at 28 kVp for that focal spot. Make
ground) and exposed (i.e., unpainted and not measurements for both focal spots, where avail-
anodized) metal on the chassis. A voltage read- able. The difference between the measured time
ing below 500 mV is acceptable for general care and the preset time should not exceed ±1 msec or
areas in existing construction. ±5% of the preset time, whichever is greater.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Mammography Units
2.5 Linearity of mAs. Use an ionization chamber mR with no added filters in the beam. These kVp,
with an electrometer (or a combination exposure mAs values should be held constant during the
meter) to measure the exposure in mR for this whole course of this test.
test. The devices should have been specifically
calibrated using mammographic energy ranges. Record the initial exposure value (in mR)
The ionization chamber should be placed centrally with nothing in the primary beam (i.e., 0 mm of
in the x-ray beam, with the compression paddle aluminum). Then add aluminum filters in 0.1
removed. mm steps up to a total of 0.5 mm, and obtain an
exposure reading for each 0.1 mm addition. Plot
Dial up a midrange kVp setting (e.g., 28 kVp). mR values against aluminum thickness on
Make radiographic exposures at this fixed kVp, semilog paper (mR vertically on log scale). Read
using a minimum of at least three mAs settings the amount of aluminum thickness required to
that span the range normally used. Record the drop the initial mR value by 50%. This is the
exposure values (in mR) from the electrometer or HVL. The measured HVL should comply with the
exposure meter for each exposure. Calculate the following equation:
mR/mAs for each exposure and average the cal-
culations. Each individual mR/mAs value should HVL ≥ [(kVp/100) + 0.03] mm Al
be within ±10% of the average mR/mAs value. For example, at 28 kVp, the HVL should be a
2.6 Exposure Reproducibility. Use one of the above minimum of 0.31 mm of aluminum. Previous
mR/mAs values at 28 kVp as the one value to be HVL values should be compared with the current
used for evaluating short-term and long-term measurement; a change in HVL may indicate
reproducibility of the mammography unit. For tube deterioration.
the short-term test, make a minimum of four 2.8 Collimation. Place an 18 cm × 24 cm film cassette
exposures at the same mAs over a span of 15 in the cassette tray. Place a larger nonscreen film
minutes. The mR/mAs values should have a co- (24 cm × 30 cm) on top of the cassette table, such
efficient of variation no larger than 5%. For that it extends beyond the patient edge of the
long-term reproducibility, simply mark the cur- cassette table by about 4 cm. Position a 10 cm stiff
rent average mR/mAs value on a trend chart wire on the larger film such that it is aligned with
together with values recorded at previous tests. the patient edge of the cassette table. Next, turn
It is critical that identical test conditions on the light field and place one coin at each of the
(e.g., same chamber-electrometer, chamber at other three sides of the field defined by the light
same distance from focal spot, same technique, field. The outer edges of the coins should mark the
absence of compression paddle) be maintained edges of the light field. Finally, place a fourth coin
for accurate assessment of long-term reproduci- in the bottom left corner of the light field to provide
bility. Long-term reproducibility should be orientation information. (See Figure 1 for wire
within ±5% of the average. and coin placement.)
2.7 Half-Value Layer (HVL). Use high-purity alu- Record the SID in use on the mammography
minum filters for this test. This test should be unit. Then make an exposure and process both
conducted with the compression paddle in place films. On the 18 cm × 24 cm film, ensure that no
and at a kVp setting commonly used to image a area beyond the outer edges of the coins can be seen
compressed breast 4 cm thick so that the derived on the film. On the larger film, measure the dis-
HVL may be used to calculate the average glan- tance from the wire edge to the edge of the x-ray
dular dose (see Item 2.14). Position the compres- field. This distance should be no greater than 2%
sion paddle as close as possible to the x-ray tube. of the SID. Note that this 2% criterion is valid only
Place the ionization chamber on the cassette for the side that is adjacent to the patient’s chest.
table, roughly 4 cm in from the patient edge of Repeat this test for the 24 cm × 30 cm film size
the table. Collimate the beam so that only the in the cassette table and for all collimators in use
sensitive area of the chamber is fully exposed. on the system. The same criteria apply to all film
Check this with the light field. Set the mammog- sizes and for all collimators.
raphy unit to operate at the kVp setting that
would be commonly used to image a compressed 2.9 AEC Object Thickness Compensation. Place 4 cm
breast 4 cm thick (e.g., 28 kVp). Select the mAs of 15 cm × 15 cm plexiglass on the cassette table.
value that produces an exposure of around 500 Ensure that it covers the AEC detectors. Bring the
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
compression paddle down to touch the top of the 2.10 AEC kVp Compensation. Place 4 cm of plexiglass
stack. Set the mammography unit to operate at on the cassette table. Ensure that it covers the
the commonly used kVp for imaging a com- AEC detectors. Bring the compression paddle
pressed breast 4 cm thick (e.g., 28 kVp). Use the down to touch the top of the plexiglass stack. Load
standard screen-film combination utilized at a standard film-screen cassette into the cassette
your facility as the receptor in the cassette holder for all checks in this test.
holder.
Make a series of AEC-controlled exposures
of the 4 cm thick plexiglass at different kVp
Make an AEC-controlled exposure. Process
values. At a minimum, use four kVp settings
the film on the standard film processor used to
that span the range commonly used. For each
process all mammography films, having
exposure at a given kVp, process the film on an
checked that it is performing optimally. Use a
optimally performing processor. Read the opti-
densitometer to measure the optical density of
cal density of the phantom image using a den-
the phantom image at a point about 4 cm in
sitometer. The optical density of all films at all
from the edge of the phantom. The optical
kVp settings checked should agree to within
density should measure in the range of 1.2-1.4
±0.3 OD. Repeat this test using the magnifica-
OD, or some other value that the radiologists
tion imaging mode.
have had programmed into the unit. Periodic
checks should result in optical density changes 2.13 Image Quality. Place the ACR accreditation
within ±0.1 OD. test phantom on the cassette table. Bring the
compression paddle down to touch the top of the
If the measured optical density falls within phantom. Load a standard screen-film cassette
the acceptable range, repeat the test using iden- into the Bucky. Dial up 28 kVp on the mammog-
tical setup conditions but with varying amounts raphy unit (or the kVp commonly used at your
of plexiglass on the cassette table. At a mini- facility for this thickness of compressed breast)
mum, check the optical density at 2 and 6 cm of and acquire an image using an AEC-controlled
plexiglass. All films used in this test should come exposure. Process the film using the standard
from the same batch, and for each check the film film processor used for all mammography films,
must be loaded into the same cassette for the having first ensured that it is performing opti-
whole test. The optical density of all processed mally. Once processed, the film should be
films should agree to within ±0.3 OD of the viewed on the viewbox normally used to display
optical density at 4 cm of plexiglass. Repeat this mammograms. It should be possible to see a
test using the magnification imaging mode on the minimum of four fibrils, three speck clusters,
mammography unit. The same criteria apply. and three masses.
Figure 1. Collimation test setup
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Mammography Units
TABLE 1. Glandular Dose (in mrad) for 1 Roentgen Entrance Exposure to a 4.2 cm Breast Thickness —
50% Adipose/50% Glandular Breast Tissue Using a Mo/Mo or W/Al Target Filter Combination
X-Ray Tube Voltage (kVp)
HVL 23 24 25 26 27 28 29 30 31 32 33 W/Al
Target-Filter
Combination
0.23 116
0.24 121 124
0.25 126 129 131
0.26 130 133 135 138
0.27 135 138 140 142 143
0.28 140 142 144 146 147 149
0.29 144 146 148 150 151 153 154
0.30 149 151 153 155 156 157 158 159 170
0.31 154 156 157 159 160 161 162 163 164 175
0.32 158 160 162 163 164 166 167 168 168 170 171 180
0.33 163 165 166 168 169 170 171 173 173 174 175 185
0.34 168 170 171 172 173 174 175 176 177 178 179 190
0.35 174 175 176 177 178 179 180 181 182 183 194
0.36 179 181 182 183 184 185 185 186 187 199
0.37 185 186 187 188 189 190 191 191 204
0.38 190 191 192 193 194 195 195 208
0.39 196 197 198 198 199 200 213
0.40 201 202 203 204 204 217
0.41 206 207 208 208 221
0.42 211 212 212 225
0.43 215 216 230
0.44 220 234
0.45 238
Source: American College of Radiology. Mammography quality control manual. Revised ed. 1994:163.
2.14 Average Glandular Dose to Standard Breast. compression paddle so that it is just in contact
The average glandular dose is determined by with the chamber and the phantom. Set the
using the HVL value measured in Item 2.7 to- mammography system at the kVp setting com-
gether with the entrance exposure measured in monly used to image a compressed breast 4 cm
air for imaging the ACR mammography accredi- thick (note that this kVp should match the value
tation phantom. used for measuring the HVL in Item 2.7), and
engage the AEC system. For a mammography
To measure the entrance exposure, place the system provided with a variable SID, record the
phantom on the cassette table, ensuring that the SID together with the technique settings.
phantom completely covers the sensitive area of
the AEC detectors. Next, set the ionization Make an exposure of the phantom and record
chamber at one side of the phantom such that its the mR value. This is the entrance exposure for
center is 4 cm in from the patient edge of the the mammography phantom. Using the HVL
cassette table and also vertically in alignment measured in Item 2.7 and the entrance exposure
with the top of the accreditation phantom. Se- measured in this test, the average glandular
cure the chamber in this position. Make sure dose may be calculated as follows:
that the x-ray field completely envelops both the a. Determine the target/filter combination of
phantom and the ionization chamber. Lower the the system under test. If it is a Mo/Mo system
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
TABLE 2. Glandular Dose (in mrad) for 1 Roentgen Entrance Exposure to a 4.2 cm Breast Thickness —
50% Adipose/50% Glandular Breast Tissue Using a Mo/Rh Target Filter Combination
X-Ray Tube Voltage (kVp)
HVL 25 26 27 28 29 30 31 32 33 34 35
0.28 149 151 154
0.29 154 156 158 159
0.30 158 160 162 162 163
0.31 163 164 166 166 167 167
0.32 167 169 171 171 171 172 172
0.33 171 173 175 176 176 176 176 177
0.34 176 178 179 179 180 180 180 181 181
0.35 180 181 183 183 184 185 185 186 187
0.36 185 186 187 187 188 188 189 190 191 191
0.37 189 190 191 191 192 193 193 194 195 195
0.38 193 194 196 196 197 197 197 198 199 199 200
0.39 198 199 200 200 201 201 202 202 203 203 204
0.40 202 203 204 204 205 205 206 207 208 208 208
0.41 206 207 208 208 209 209 210 211 212 212 212
0.42 211 211 212 212 213 213 214 215 216 216 217
0.43 215 216 217 217 218 218 219 219 220 220 221
0.44 220 220 221 221 222 222 223 223 224 224 225
0.45 224 224 225 225 226 226 227 227 228 228 229
0.46 228 229 229 230 231 231 232 233 233 234
0.47 233 233 234 235 235 236 237 237 238
0.48 238 238 239 240 240 241 241 242 242
0.49 242 243 243 244 244 245 245 246
0.50 247 247 248 248 249 250 251
0.51 251 252 253 254 254 255
0.52 257 257 258 258 259
0.53 261 261 262 263 264
0.54 265 266 267 268
0.55 269 270 271 272
0.56 275 276 276
0.57 279 280 281
0.58 284 285
0.59 288 289
0.60 293
Source: American College of Radiology. Mammography quality control manual. Revised ed. 1994:164.
or a W/Al system, use Table 1. For Mo/Rh and d. The value at the intersection of the HVL row
Rh/Rh systems, use Table 2 and Table 3, and the kVp column is the normalized glan-
respectively. dular dose (i.e., the dose that applies to an
entrance exposure of 1 R). Multiply the nor-
b. Go down the first column in the table until you malized glandular dose by the entrance expo-
find the HVL value measured in Item 2.7. sure measured in this test. The value
obtained is the average glandular dose for the
c. Progress along the row at this HVL until you system under test.
are in the column headed by the kVp setting
used to measure the entrance exposure in this The average glandular dose for the system
test. under test should not exceed 300 mrad (3 mGy).
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Mammography Units
TABLE 3. Glandular Dose (in mrad) for 1 Roentgen Entrance Exposure to a 4.2 cm Breast Thickness —
50% Adipose/50% Glandular Breast Tissue Using a Rh/Rh Target Filter Combination
X-Ray Tube Voltage (kVp)
HVL 25 26 27 28 29 30 31 32 33 34 35
0.28 150 155 159
0.29 155 160 164 168
0.30 160 164 168 172 176
0.31 165 168 172 174 180 182
0.32 169 173 177 181 184 186 188
0.33 174 178 181 185 188 190 192
0.34 179 183 186 190 193 195 196 199
0.35 184 187 190 194 197 199 201 203
0.36 189 192 195 198 201 204 205 207 209
0.37 193 196 199 202 205 207 209 211 213
0.38 198 201 204 207 209 211 213 215 217 219 221
0.39 203 206 208 211 214 216 217 219 221 223 224
0.40 208 211 213 216 218 220 221 223 224 226 228
0.41 213 215 217 220 222 224 225 227 228 230 232
0.42 218 220 222 224 226 228 229 231 232 234 236
0.43 222 224 226 228 230 232 233 235 236 238 240
0.44 227 229 231 233 235 237 238 239 240 242 243
0.45 232 234 235 237 239 241 242 243 244 246 247
0.46 239 241 243 245 246 247 248 250 251
0.47 247 249 250 251 252 254 255
0.48 251 253 254 255 256 258 259
0.49 257 258 259 260 261 262
0.50 261 262 263 264 265 266
0.51 266 267 268 269 270
0.52 270 271 272 273 274
0.53 275 276 276 277 278
0.54 279 280 280 281
0.55 283 284 284 285
0.56 288 288 289
0.57 292 293
0.58 296 297
0.59 300
0.60 304
Source: American College of Radiology. Mammography quality control manual. Revised ed. 1994:165.
As an illustration of the above method, assume 3.2 Lubricate according to the manufacturer’s in-
that on a Mo/Mo system, the HVL measured at structions (e.g., clean and lubricate casters, if
28 kVp was 0.33 mm Al and that the entrance needed).
exposure measured at 28 kVp was 500 mR (0.5
R). From Table 1, the normalized glandular dose 3.3 Calibrate the unit, if needed.
is 170 mrad. Multiplying the normalized dose by
3.4 Replace items on the unit, if needed.
the entrance exposure of 0.5 R provides the glan-
dular dose value of 85 mrad.
4. Acceptance tests
3. Preventive maintenance Acceptance testing is typically performed by a medi-
3.1 Clean exterior and interior, if needed. cal physicist.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Inspection and Preventive Maintenance System
Before returning to use home, ensure that all controls are set correctly before
it is returned to the patient.
Ensure that all controls are set properly. Set alarms
loud enough to alert personnel in the area in which the Attach a Caution tag in a prominent position so that
device will be used. Other controls should be in their the user will be aware that control settings may have
normal pre-use positions. If the unit is being used at been changed.
Inspection and Preventive Maintenance System
10 ©1995 ECRI. All Rights Reserved.
Procedure/Forms 440-0595
Medical Gas/Vacuum Systems
Used For:
Alarms, Central Gas System [15-824]
Medical Gas and Vacuum Systems [18-046]
Medical Gas Outlets [17-682]
Valves, Medical Gas and Vacuum [18-044]
Also Called: Piped medical gas systems, medical-surgical gas systems, nonflammable medical gas systems,
vacuum systems
Commonly Used In: Most patient care areas and some laboratories
Scope: Applies to any piped medical gas system (including oxygen, air, and nitrous oxide) and central vacuum
system; does not replace full testing according to NFPA 99, Standard for Health Care Facilities, which must be
conducted following any new construction or modification; does not apply to medical air compressors, dryers,
contaminant monitors, or purification systems, which must receive regular IPM for safe and reliable operation
(see Medical gas and vacuum systems, Health Devices [Guidance article], 1994 Jan-Feb; 23:4-41)
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major After any renovations, Months Approximately 100
modifications, and/or additions outlets/day in occupied
to the medical gas system areas; 250 outlets/day
in unoccupied areas
Minor 12 months* Months Same as above
* Although we recommend that a major inspection (Items 2, 3, 5, 6, 7, and 8) be performed annually for medical
gas and vacuum systems, we understand that, for some hospitals, this may not be practical. Increasing the
inspection interval up to but not more than two years is acceptable in these cases. However, some frequently
used outlets and inlets (e.g., in the emergency room) are subject to wear, and more frequent performance of
Items 5 and 6 should be considered to ensure their safe operation. Where alarm-system test buttons are
provided, audible and visual alarm indicators should be tested monthly (NFPA 99, Appendix C, Section C-4.2.17).
Overview multiple fatalities in some institutions, in at least 15
hospitals in North America.
In an actual case, workers renovating an emergency Piped gas systems present certain characteristic
room inadvertently cross-connected the nitrous oxide hazards, usually related to their original construction,
and oxygen supply lines. As a result, 20 outlets labeled modification, or repair. However, problems can de-
“oxygen” actually delivered nitrous oxide for more than velop during the working lifetime of the systems, par-
six months before the hospital’s chief anesthesiologist ticularly in medical compressed air systems, outlets,
discovered the error. We are also aware of other cases and vacuum inlets. The hazards include plumbing
in which similar incidents have occurred. Mix-ups in errors, as described above; use and degradation of
medical gas connections have caused deaths, including materials incompatible with the gases to be delivered;
241434 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
440-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
obstruction of flow by migration of material left in the on medications, requires that medications (i.e., drugs)
pipelines; gas contamination by residual debris or ac- be prepared, delivered, and administered according to
cumulated foreign matter (e.g., scale, hydrocarbons, appropriate laws and standards of practice, which
microorganisms, moisture, or dirt in medical com- again indirectly refers to NFPA 99.
pressed air pipelines); gas contamination due to chemi-
cal interaction, including fire and explosion, between Hospitals should insist that those responsible for
the gases and pipeline components or foreign matter; construction document the test methods and results as
and gas contamination due to a contaminated source required in NFPA 99; this documentation, as well as
(e.g., air intake near diesel exhausts). (See Cleaning documentation from analytical tests, should be kept on
contaminated MGVSs, Health Devices 1994 Jan-Feb; permanent record. Hospitals should also obtain docu-
23:34-5.) Problems related to how the system is used mentation verifying the purity of medical gases from
and maintained during its lifetime include leaking suppliers. In addition, the hospital should perform
outlet seals, clogged vacuum inlets and piping (e.g., by acceptance inspection and testing of the medical gas
dust or by body fluids), inadequate particulate filtra- and vacuum systems independently of tests conducted
tion, corrosion of automatic condensate drains, wear by the installing contractor. The hospital’s facility
or embrittlement of valve seals, physically damaged or engineering, anesthesia, clinical engineering, or respi-
loose outlets, wear of compressor or pump seals and ratory therapy department may perform this testing.
bearings, and pressure sensor drift. If adequate personnel, experience, or equipment is
lacking, an independent testing organization that spe-
NFPA 99, which is mandatory in some localities, cializes in this type of activity can be employed.
states in Chapter 4, the section on gas and vacuum
systems, that the piping systems must be tested fol- In a typical hospital, piped medical gas and vacuum
lowing new construction, addition, renovation, or re- systems are frequently repaired, modified, and ex-
pair. (In this procedure, references to NFPA 99 refer panded. These activities may include replacing defec-
to the 1993 edition, unless otherwise specified.) It tive outlets or inlets, valves, or piping; relocating
specifies tests for zone-valve and alarm-system func- outlets; and adding outlets to the existing system. Iden-
tion, leaks, and cross-connections (in addition to other tification plates and other labels are often removed
items) and provides specific criteria for gas analysis during this activity, increasing the probability of error.
and monitoring. Installers are required to perform Major changes to systems (e.g., construction of a build-
some testing of new or modified systems; independent ing addition) are not included in this category.
testing of these systems before they are used for pa-
tient care is recommended. NFPA 99 also calls for the ECRI knows of no procedure other than this one that
healthcare facility to develop and implement proce- enables the hospital to safely, easily, accurately, and
dures for testing medical gas and vacuum systems and completely inspect only the modified portion of the
their related alarm systems; this IPM procedure system. The procedures outlined in NFPA 99 are
should satisfy this requirement for piping and alarm clearly intended to test newly constructed systems
systems testing. The standard also requires that that have not yet been put into service. The process
proper medical gas concentration be verified and that described by that standard requires testing at differ-
the supply systems be tested after any breach of or ent stages of installation before proceeding with addi-
modification to the system. tional installation. For example, both the 150 psig
pressure test (Section 4-5.1.2.1) and the blow-down (or
Also, in its 1995 Accreditation Manual for Hospitals,
initial purging) test (Section 4-5.1.2.2) must be per-
the Joint Commission on Accreditation of Healthcare
formed before system components, such as pressure-
Organizations (JCAHO) requires that the hospital
actuating alarm switches, alarms, manifolds, pressure
have documented plans and procedures for routine
gauges, and pressure relief valves, are installed.*
testing, inspection, and maintenance of utility systems
(e.g., medical gas and vacuum systems) to ensure that Pressure testing and purging of the completed system
these systems operate properly and will continue to must also be performed. The hospital should have the
operate in an emergency. The JCAHO manual also contractor who installs the system and an outside testing
indirectly refers to NFPA 99 through NFPA 101, Life organization provide documentation of conformance
Safety Code, and the American Institute of Architects’
Guidelines for Construction and Equipment of Hospi- * Pressure is measured relative to one of two reference points: standard
atmospheric pressure (14.7 psia) or zero absolute pressure; psig refers
tal and Medical Facilities, which base design and to gauge pressure (i.e., the reference pressure to which the measuring
safety requirements on NFPA 99. Also, because medi- device is calibrated, typically standard atmospheric pressure), and psia
cal gases are drugs, the JCAHO manual, in its section refers to absolute pressure (i.e., reference pressure of zero).
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Medical Gas/Vacuum Systems
with all portions of NFPA 99, Chapter 4, for all new Pressure measuring devices, 0 to 100 and 0 to 400
medical gas and vacuum system construction. psig, with 5% accuracy
Performing certain portions of the NFPA 99 testing Flowmeter, 0 to 250 L/min, with 5% accuracy (flow-
procedure requires a complete shutdown of the system. meter manufacturers usually supply calibration
Thus, the hospital must provide a large number of curves for a range of common gases with each in-
alternative gas or vacuum sources (e.g., cylinders with strument); alternatively, if a flowmeter calibrated
regulators, portable suction systems) and may need to for the gas being measured is not available, use the
minimize gas or vacuum usage (e.g., by rescheduling following formula:
surgery) to test the entire medical gas or vacuum
√ Density (Design Gas)
system following modifications. Corrected Flow = Indicated Flow
Density (Test Gas)
Because of the difficulty and expense entailed and Flow control valve(s)
the possible compromise of patient care, hospitals are
reluctant to fully test modified systems, except after Test equipment that combines the functions of the
major modifications or additions. However, failure to above test devices or that automates the testing de-
fully test systems can allow serious problems scribed in this procedure is available and may be
(e.g., cross-connections, which are usually thought of substituted. Also, portable pneumatic calibrators or
as problems associated only with new systems) to go anesthesia machine calibrator/analyzers may be suit-
undetected. able alternatives.
ECRI has developed a simple technique that per- Note: Medical gas systems may contain contami-
mits testing and inspection both of existing systems nants that may affect test instruments; periodic clean-
and of modified portions without affecting the entire ing, in addition to calibration, may be needed.
hospital at once; this procedure also allows detection Source of oil-free dry nitrogen with a pressure regu-
of most problems that can develop during system modi- lator to supply a test gas (see the section on com-
fication or system operation. pressed gases in “IPM Safety” behind the Guidance
Tab of this binder)
Citations from Health Devices Hoses and adapters to connect the pressure or vac-
Restricted draw in Schrader-type vacuum inlets [User uum measuring device and test gas cylinder to each
Experience NetworkTM], 1993 Aug-Sep; 22:426-7. gas outlet
Color-coded compressed medical gas hose changes Hand tools, such as screwdrivers, wrenches (includ-
color [Hazard], 1986 Apr; 15:106-7. ing Allen wrenches), and pliers
Labels, such as “Do Not Use” and “System Under
Medical gas and vacuum systems [Guidance article],
Test”
1994 Jan-Feb; 23:4-41.
Sampling bottles and filters for collecting samples
Should vacuum pump effluent be treated? [User Expe- for analysis; typically, these are obtained from the
rience NetworkTM], 1994 Jul; 23:310. laboratory that will conduct the analysis
Use of filters on medical gas system outlets and vac-
uum system inlets [User Experience NetworkTM], Special Precautions
1994 Dec; 23:494-5. General. Before testing, alert clinical personnel,
and ensure that an adequate supply of appropriate gas
Soldered medical gas piping [User Experience Net- cylinders and/or vacuum sources is available in the
workTM], 1995 Mar; 24:127. immediate area as a backup for piped gases. Provide
ample preparation time, especially if a system or zone
Test Apparatus and Supplies must be shut down for testing.
Oxygen analyzer that will remain accurate in the Never disconnect or test any medical gas outlet,
presence of and not be damaged by nitrous oxide vacuum inlet, or system serving a patient or patient
(analyzers used with anesthesia units are probably care area without the approval of clinical personnel.
satisfactory)
Do not perform any test that may interfere with the
Vacuum measuring device, 0 to 30 inches of mercury gas supply to patients (e.g., turn off zone valves,
(in Hg; 0 to 760 mm Hg), with 5% accuracy pressurize with another gas or to a pressure different
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
from the usual supply pressure) while that section Limit purging and flow measurement times from
of the system is in use for patients. each outlet to 10 sec. (About 200 ft of piping can be
Never use oxygen as a test gas (e.g., pressure purged in this time; correspondingly shorter purge
test) — use only oil-free dry nitrogen. times can be used for shorter piping runs.)
Do not allow smoking or other open sources of igni- Purge the nitrous oxide system last, and leave the
tion in the immediate test area, especially in the room after turning off the outlets. Restrict person-
presence of nitrous oxide or oxygen. nel from entering the room to allow the exhausted
gas to dissipate. In a typical operating room, 15 min
Because of high pressure, take special care when is adequate. In smaller rooms with lower ventilation
inserting and disconnecting adapters from the out- room-air exchange rates, such as delivery rooms,
let under test. Also, before testing, make certain dissipation may require 1 hr. Restrict unnecessary
that the adapter is securely locked into the outlet. entry into the room during this time; the room may
Never pressurize (i.e., apply a test gas to) a vacuum be used if essential for patient care.
system with gauges in the section of the system to
be pressurized; this could damage the vacuum Procedure
gauges. Overpressurizing compressed gas lines, as This procedure was developed to help hospitals find
required for certain sensors (e.g., newly installed or and correct hazards associated with existing and modi-
modified systems), can also damage certain sensors, fied piped medical gas and vacuum systems. It does not
alarm switches, and outlets in these systems. Cer- replace the full testing required by NFPA 99; it con-
tain pressure tests must be conducted before these firms safe operation and is recommended for use by the
components are installed in the system per NFPA hospital for independent confirmation of safety and
99, Section 4-5.1.2.1. performance only after the construction, tests, and
Purging. When using the test gas (oil-free dry nitro- inspection per NFPA 99 have been completed and on
gen) to inspect an alarm panel or to pressurize a piping an annual basis thereafter.
system, purge the test gas from the system before
You must perform all items in the procedure on any
using it for patients. With the appropriate zone valve
portion of the system that is repaired or modified
closed, open an outlet to depressurize the system. After
before that portion of the system is put into service.
depressurization, close that outlet; then open the zone
valve and each outlet in the zone in order, starting with Before beginning the inspection, carefully read this
the outlet nearest the zone valve. You can turn off an procedure; be sure you understand how the gas system
outlet before opening the next outlet in the line. Where and associated equipment are intended to operate, the
appropriate (e.g., with oxygen and medical compressed significance of all controls and indicators, and the
air pipelines), use an oxygen analyzer to verify proper alarm capabilities. Begin the inspection procedure by
oxygen content at each outlet, or flush each outlet with identifying the area to be tested. This may be a room,
its labeled gas for approximately 1 min (except nitrous a special care area, or an area with many outlets. We
oxide — see the precautions below — and also note recommend that each gas outlet be identified with a
that an oxygen analyzer, by definition, will not detect numbered label or an engraved number on the face-
nitrogen or nitrous oxide). plate. One systematic numbering method consists of
starting to the left of a given doorway from a position
Nitrous Oxide. Take special precautions when test-
facing into the room and proceeding clockwise, num-
ing or purging nitrous oxide systems to minimize ex-
bering the outlet stations in the room (see Figure 1).
posure to the exhausted gas. Although occasional acute
Include ceiling columns (e.g., as in an operating room),
exposure to nitrous oxide, which might occur during
as well as surface-mounted stations. Each outlet at a
annual testing, has not been shown to be hazardous,
given station is then numbered from left to right.
we recommend that you still take reasonable precau-
tions to minimize exposure. For example: Disconnect equipment from each outlet before per-
Women of childbearing age should not routinely forming the inspection of that outlet station. If you are
perform this procedure or be in the area during the inspecting a system that is already in operation, con-
procedure. sult clinical personnel before disconnecting any pa-
tient care equipment being used. Inspect every outlet
Use a length of corrugated tubing (about one inch in at each station in the area.
diameter) to direct the exhausted gas away from
personnel and, where practical, into a ventilation Because the Universal Inspection Form is not ap-
return duct or out a window. plicable, use the special three-part Medical Gas and
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Medical Gas/Vacuum Systems
1. Pressure Testing. All new or modified systems
should be pressure tested per NFPA 99, Sections
4-5.1.2.1 and 4-5.1.2.3. We recommend that the
following acceptance test be performed by the
hospital or an independent agency before a new
system or modified portion of the existing system
is put into use.
When all components of the system have been
installed and the system is ready to be used, pres-
surize the appropriate section of the medical gas
or vacuum system to 100 psig with oil-free dry
nitrogen. On additions and modifications, close the
appropriate zone valve before pressurizing so that
the section to be tested is isolated from the rest of
the system. We recommend using 100 psig (instead
of 150 psig, as required by NFPA 99 during the
initial pressure test) for testing to reduce the risk
of damaging system components. (Verify that com-
Figure 1. Sample room with 6 stations, numbered clock- ponents [e.g., pressure sensors] will not be dam-
wise from left, and 18 outlets. aged by this test pressure.) However, this does not
substitute for pressure testing according to NFPA
Vacuum System Inspection Form provided. Part A of
99 during installation. Measure the pressure im-
the form is for alarm-panel and zone-valve inspections,
mediately after pressurization to 100 psig and
and Part B is for medical gas outlet and vacuum inlet
again 1 hr later. After correcting for any tempera-
inspections. Part C is for documenting medical gas
ture changes, confirm that there has been no
purity analysis.
change in line pressure after the 1 hr period. To
On the appropriate part of the inspection form (on correct for temperature changes, use the following
Parts A and B), record the test data and the actions formula:
needed and taken. If deficiencies detected during the PInitial × TFinal
inspection are serious enough to preclude using an PFinal =
TInitial
outlet until it is repaired, check both the Action Needed
and the Do Not Use columns; label the outlet so that it where T = absolute temperature measured in
will not be used and so that it can be quickly identified kelvins or degrees Rankine*
for future repairs. If the outlet is in an area being used,
2. Area Pressure Alarms. Area pressure alarms
inform clinical personnel, and make sure that an ade-
should be activated when line pressure varies
quate alternative gas supply is available. If the outlet
20% from normal system pressure.
is usable, check only the Action Needed column. To
clearly identify defective outlets on the inspection To test the high-pressure alarm, close the
form, circle unacceptable values, or note specific de- appropriate zone valve, and apply oil-free dry
fects in the Comments section at the bottom of the nitrogen through a pressure measuring device to
form. one outlet in the zone until the alarm is acti-
vated. Measure and record the alarm pressure.
The Status box in the upper right corner of each To test the low-pressure alarm, bleed system
form provides a quick indication of the condition of the pressure with the zone valve closed until the
outlets or alarms and valves listed. Check the appro- low-pressure alarm is activated. Measure and
priate box after completing the inspection. If even one record the alarm activation pressures on the top
outlet, alarm, or valve on the sheet requires servicing, portion of Part A of the Medical Gas/Vacuum
check the Service Required box. The individual who Systems Inspection Form. (Note: This test can
completes the repairs should record the date and his be performed in conjunction with Item 3.)
or her initials in the Action Taken column; check the
OK column after confirming the satisfactory condition Check area signal panels, remote indicators
and performance of that item. Check the Passed box in (if present), and appropriate gauges for proper
the Status area only after all repairs for all items on * To obtain a temperature in kelvins or degrees Rankine, add 273.2
that form are complete. to degrees Celsius and 459.7 to degrees Fahrenheit, respectively.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
labeling and function or accuracy. Also check With appropriate adapters (which should match
audible alarm-silence systems during alarm ac- outlet labels), check each individual outlet of
tivation — a visual alarm light should remain each gas and vacuum system to determine that
on. In addition, check signal panels for deactiva- test gas is not present at any outlet other than
tion after returning the system to normal pres- the one connected to the pressurized supply.
sure. Before placing the system in service, purge Disconnect the source of the test gas, and reduce
it as described in the Special Precautions section the first system to atmospheric pressure. Repeat
and in accordance with NFPA 99, Section this test by pressurizing each additional piping
4-5.1.3.9. (Other testing may be completed with system, one at a time, including vacuum (unless
the test gas before purging; see the precautions gauges are present). Purge all tested systems in
regarding nitrous oxide.) accordance with NFPA 99, Section 4-5.1.3.9, and
the special precautions noted previously.
If the alarm panel has test buttons, retesting
of audible and visual alarms should be done To avoid disrupting patient care when testing
monthly. modifications to existing systems that are in use,
use the oxygen concentration measuring proce-
3. Zone Valves. Zone valves are tested to ensure dure described in Item 5.
that the branch served by the zone valve will be
closed and isolated in the event of an emergency. 5. Medical Gas Outlets (medical compressed air,
nitrogen, nitrous oxide, oxygen, carbon dioxide,
Check each zone valve for a label or placard that
and other gases if piped). Examine the condition
lists the gas it controls and the area it serves. Also
of the outlet. Check that each outlet is properly
check that a line-pressure gauge is present down-
labeled with the name of the dispensed gas and
stream of the zone valve and that it correctly reads
that its cover plate is securely fastened. Ensure
the system pressure by comparing it with a pres-
that color coding is consistent with standards for
sure measuring device at an outlet in that area.
the gas supplied to each outlet (e.g., green for
Close the valve, and bleed the branch to zero
oxygen, yellow for medical compressed air).
pressure. Confirm that the system gauge and pres-
Make sure that the adapter specific for the gas
sure measuring device read zero. Record findings
dispensed locks securely into the outlet, that the
on the bottom portion of Part A of the Medical
outlet does not leak with the adapter installed,
Gas/Vacuum System Inspection Form.
that the adapter is easily removed, and that the
Perform a leakage test on all threaded compo- valve closes when the adapter is removed. Listen
nents of the pressurized zone valve using a test for leaks before and after inserting adapters.
solution listed as safe for use with oxygen. Leaks may be corrected by replacing seals
(e.g., O-rings, gaskets) in the valve assembly.
4. Cross-Connection Testing. This test should only
be performed on new systems or following any Attach an oxygen analyzer, a pressure meas-
system modifications. The test must be per- uring device, and a flowmeter or pneumatic ana-
formed after all outlets are completely installed, lyzer to the outlet; measure and record the flow
including labels, cover plates, and fittings. This and pressure at that flow on Part B of the Medi-
will ensure that outlets are connected to and cal Gas/Vacuum System Inspection Form. NFPA
labeled for the appropriate gas system. Do not 99 requires that piping systems be able to deliver
rely on testing done before final attachment of flows at the pressures listed in Table 1, Recom-
labels and other identification plates that iden- mended Pressures and Flows.
tify gas outlets. Open the flow-control valve until a flow of 100
To test new systems or major modifications L/min is seen. Pressure at that outlet should not
to existing systems where gas sources can be
shut down without disrupting existing patient Table 1. Recommended Pressures and Flows*
care, use the following procedure. Reduce all Medical Gas Pressure, psig Flow, L/min
pipelines to atmospheric pressure. Disconnect Oxygen 50 to 55 ≥100
all sources of test gas from all of the systems Nitrous Oxide 50 to 55 ≥100
with the exception of the one system to be Medical Air 50 to 55 ≥100
Carbon Dioxide 50 to 55 ≥100
checked. Pressurize this system to 50 psig with Nitrogen ≥160 ≥145
oil-free dry nitrogen to avoid disruption to and *Pressures and flows per NFPA 99, Section 4-5.1.3.8.
possible contamination of the existing services.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Medical Gas/Vacuum Systems
drop below 50 psig for all gases except nitrogen, label. This problem may also arise if you use
which should not drop below 160 psig at a flow extension hoses to connect equipment to a wall
of at least 145 L/min. Some older systems may or ceiling outlet. Recheck each time service per-
not be able to meet these requirements. However, sonnel remove a hose for repair, maintenance, or
if the pressure drops to below 80% of the listed replacement.
values in older systems or below the required
values in newer systems or if the required flows Gas hoses should have appropriate connectors
cannot be obtained, corrective action is required. for attachment to equipment. Avoid using spe-
Unacceptable pressure or flow may indicate a cial adapters for connecting hoses (e.g., DISS to
blockage in either the distribution piping or the quick-connect fittings) to minimize problems
outlet check valve(s). Blowing the piping clear such as gas leaks at the connectors. Color-coded
with the outlet removed and cleaning the outlet hoses are recommended for this application to
check valve(s) will usually resolve this problem. reduce the risk of misconnection. Be aware that
(Minimize exposure to nitrous oxide; see Special the color of gas hoses can change over a period of
Precautions.) If the above measures do not re- time (see Color-coded compressed medical gas
solve the problem, the outlet may have to be hose changes color [Hazard], Health Devices
replaced or, depending on the severity of the 1986 Apr; 15:106-7.) Replace any hoses that have
restriction, a portion of the system may need to changed color or faded.
be modified. Consult with clinical staff to deter- 6. Vacuum Inlets (vacuum and evacuation vac-
mine the minimum acceptable flow for clinical uum). Inspect the condition of each inlet, as
needs, including the safe operation of life-sup- described in Item 5.
port equipment. Also consider whether simulta-
neous use of multiple outlets will further Attach the vacuum measuring device to an
degrade performance. ECRI can provide advice inlet and a flowmeter to an adjacent inlet. Meas-
on the most appropriate action to take should a ure and record the pressure and flow on Part B
flow-restriction problem exist. of the Medical Gas/Vacuum System Inspection
Form. NFPA 99, Section 4-11.2.1.3, requires that
Measure and record (on Part B of the Medical the vacuum pressure be at least 12 in Hg (305
Gas/Vacuum Systems Inspection Form) the oxy- mm Hg) while 85 L/min (3 standard cubic feet
gen concentration to determine that the outlet is per minute) flow is being drawn at an adjacent
delivering the proper medical gas. The oxygen inlet. We recommend that, where practical, the
concentration should be 100% at oxygen outlets two inlets be on the same branch and that the
and 21% at medical compressed air outlets. pressure be measured at an inlet beyond the
NFPA 99, Section 4-5.1.3.9, requires the use of inlet at which the flow is established. In addition,
gas-specific analyzers for initial testing of new we recommend noting the maximum flow. Most
and renovated systems, but for routine testing of newer systems will be able to provide 85 L/min
installed systems, nitrogen, nitrous oxide, and at an inlet, although such high flows may not be
carbon dioxide outlets should read 0% on an required for many applications. Some older sys-
oxygen analyzer. Note that, in an operating sys- tems may not be able to meet these criteria; it is
tem, nitrogen will be at a higher pressure than then necessary to determine whether corrective
nitrous oxide. This test can also serve to check action (e.g., cleaning the pipeline) is required to
for cross-connection in existing systems. meet clinical needs.
In some hospitals, hoses extend from ceiling For inlets that have reduced vacuum draw,
connectors to outlets that are suspended at a inspect the interior of each vacuum inlet for
lower, more accessible height. Although the ceil- accumulated dust or other debris from leaking
ing connector and suspended outlets may have seals or poor suctioning procedures. Clean the
proper labels and unique fittings for each gas to inlet, if necessary, by removing the inlet valve
prevent incorrect connections, the end connec- assembly and washing it in warm soapy water
tions of the hoses and the pipelines to the gas (see the section on infection control in “IPM
fittings and outlets may be identical. Thus, it Safety” behind the Guidance Tab in this binder).
may be possible to attach an outlet or connector Using a piece of tubing, suck about a liter of the
to the wrong hose. If you have such an installa- wash water into the disassembled inlet to clean
tion, make sure that the ceiling connector and debris from the inlet section of the pipeline.
outlet linked by a given hose have the same gas Rinse the inlet valve assembly with clean water
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
and reassemble the inlet. Remeasure vacuum compressors must also be monitored for liquid
pressure and flow at the cleaned inlet. Inade- (continuously) and gaseous (quarterly) hydro-
quate flow may indicate other problems in the carbons. Piped medical compressed air systems
vacuum system (e.g., a clogged pipe). should also be tested annually for particulates.
Independent dew point and carbon monoxide
7. Master Alarm Panel. Refer to NFPA 99, Section
tests should be conducted at least annually for
4-4.1.1.2 and Appendix C-4, for required compo-
all medical compressed air systems, preferably
nents and recommended test intervals. Section
in the summer when these contaminants are
4-6.2.3.9 of NFPA 99 requires periodic retesting
most prevalent, to verify monitor performance.
of audible and visual alarms to determine
More frequent analyses may be warranted in
whether they are functioning properly, and Sec-
hospitals with medical compressed air problems
tion C-4.2.16 recommends annual testing of all
until those problems are resolved.
components of warning systems if testing can be
performed without changing system line pres- For medical compressed air analysis, obtain
sure. Refer to the manufacturer’s instructions sampling bottles (as well as instructions for their
for component testing. use) from an analytical laboratory. For annual
inspections, sampling can be done at an outlet
8. Medical Gas Analysis. Acceptance testing of
close to the source. To determine the cause of any
medical gas purity is not usually required if
problem, it may be necessary to monitor the
purity testing required by NFPA 99 is conducted
quality of the outside air at the medical air com-
by an independent test organization when the
pressor intake. For all other analyses, take a
system is completed.
sample at the farthest outlet locations from the
Obtain certificates of purity showing all test- compressor in the piped medical compressed air
ing performed by the gas manufacturer for each system.
shipment of gas.
Enter the results of the medical air analysis
For oxygen, nitrous oxide, nitrogen, and carb- on Part C of the inspection form. Compare the
on dioxide, verify that certificates of purity have results to the values listed in Table 2, in which
been received and filed for each gas shipment, most allowable values meet or exceed the con-
and note this on the Confirmation of Purity taminant limits of most of the various concerned
section of the inspection form. Include the source agencies. ECRI chose the values listed in the
of any certificate of purity and the date of the table because we believe they are reasonable to
certificate. After installation of a new system, obtain and safe for the particular gas and con-
the piping system for these gases should also be taminant based on our review of the several
tested for gaseous and liquid hydrocarbons, as documents that define the composition of medi-
well as for particulates and gas concentration. cal gases.
We recommend taking gas samples from an out-
Judging the level of a particular contaminant
let nearest the gas source and at the outlet most
relative to this table should be done with caution.
remote from the source. Refer to Table 2 for
Such factors as the measurement accuracy, the
recommended maximum allowable levels of con-
sampling location, the sampling technique, and
taminants for these gases.
the contaminant itself will affect what should be
NFPA 99, Section 4-3.1.9.8, requires that the done. Regardless, a second test, independent of
quality of the medical compressed air generated the first, should be made to verify any suspected
on-site be monitored continuously for dew point contamination. Determination of the source of
and carbon monoxide. A gas sampling port the contamination will direct the course of cor-
downstream of the system pressure regulators rective action (e.g., change of source, purge of
is used for this purpose. Reciprocating (oil-less) pipeline).
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Medical Gas/Vacuum Systems
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Inspection and Preventive Maintenance System
Inspection and Preventive Maintenance System
10 ©1995 ECRI. All Rights Reserved.
Medical Gas/Vacuum Systems
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 11
Inspection and Preventive Maintenance System
Inspection and Preventive Maintenance System
12 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 463-0595
Mobile C-arms
Used For:
Radiographic/Fluoroscopic Units, Mobile [11-758]
Also Called: Portable C-arms, surgical C-arms
Commonly Used In: Critical care areas, emergency departments, and operating rooms
Scope: Applies to mobile C-arms capable of fluoroscopy and radiography
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommende Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview the physician’s office, the industrial site, and the ath-
letic field. The user can quickly acquire projections of
C-arms provide radiographic and fluoroscopic imag- the patient’s anatomy from various angles while con-
ing in surgical, orthopedic, critical care, and emer- tinuously viewing the fluoroscopic images. Radio-
gency care procedures. They are used to image graphic imaging capability may not be provided.
patients in radiolucent beds, stretchers, or tables
when it is not feasible to transport the patient to the
radiology department. The fluoroscopic feature allows
Citations from Health Devices
real-time imaging, which permits quick diagnoses and Mobile C-arm units [Evaluation], 1990 Aug; 19: 251-91.
minimal patient time under anesthesia during surgi-
cal procedures. International Medical Systems Exposcop Plus mobile
C-arm system [Evaluation], 1993 Mar; 22:103-21.
C-arms are used in a variety of general surgical,
cardiac, and neurological applications, including aneu- FluoroScan Mini C-arm unit [Evaluation], 1995 Feb;
rysm repair, pacemaker implantation, hip replace- 25:44-70.
ment, fracture reduction, foreign-body location, needle
biopsy, catheter placement, percutaneous lithotripsy, Test apparatus and supplies
and brachytherapy. These devices also enable special
studies, such as the diagnosis of swallowing disorders Ground resistance ohmmeter
in patients who cannot readily sit on a standard fluoro- Leakage current meter or electrical safety analyzer
scopic table or stand on a footboard. Mobile C-arms can
also be equipped with a variety of digital hardware and Noninvasive kVp meter (compatible with the x-ray
software options for use in angioplasty, interventional generator being inspected)
neuroradiology, neurosurgery, and trauma care. Noninvasive timer (may be included with kVp
meter)
Compact, scaled-down fluoroscopic imaging sys-
tems called mini C-arms are designed for extremity Ionization chamber with electrometer or a combina-
imaging in the emergency room, the operating room, tion exposure meter
241477 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
463-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Five filters of 10 cm × 10 cm × 1 mm Type 1100 maintenance procedures or frequencies are recom-
aluminum mended by the manufacturer.
Ruler with leaded 1 cm or 1⁄2″ markers This procedure is intended to ensure adequate sys-
Large-format x-ray film (30 cm × 30 cm) tem performance and maintenance. It should not be
construed as providing full compliance with the re-
Patient simulator material (e.g., 8 pieces of 30 × 30 quirements of all governmental regulations and ac-
× 2.5 cm plexiglass, or appropriate thickness of creditation standards of professional associations.
aluminum or copper) to bring the unit to midrange Such regulations and standards may include testing
technique under automatic brightness stabilization beyond that provided below and may also require docu-
(ABS) control mentation by a certified medical physicist.
Six pieces of 30 cm × 30 cm × 1 mm lead
For acceptance testing, we strongly recommend con-
High-contrast resolution line-pair phantom to 5 tracting with a medical physicist. Acceptance testing
lp/mm minimum is crucial because it generates data on baseline per-
Low-contrast phantom consisting of two 3/4″ (2 cm) formance of the device.
aluminum plates, 7 × 7″ (18 × 18 cm), and one sheet
1. Qualitative tests
of 1.0 mm aluminum, 7 × 7″ (18 × 18 cm), with two
sets of four holes of the following sizes: 1/16″, 1/8″, 1.1 Chassis/Housing. Examine the exterior of all
3/16″, and 1/4″ (1.0, 3.0, 5.0, and 7.0 mm) (using an components of the C-arm for cleanliness and
alternative low-contrast phantom is acceptable pro- general physical condition. Be sure that all hard-
vided that it can be reproducibly used for assessing ware is present and tight and that there are no
long-term performance; use the criterion applicable signs of spilled liquids or other serious abuse.
to the phantom selected) External collimators should be checked for pool-
ing of blood and be cleaned, if necessary. The grid
Oscilloscope (calibration only)
and image intensifier housing should be checked
High-voltage divider (calibration only of rotating for blood and cleaned, if necessary.
anode type x-ray tubes)
Check the mechanical operation of the C-arm,
Special precautions including up/down motion, rotation, and
wig/wag, ensuring that all movements are
Wear a lead apron and thyroid shield at all times smooth; ensure that the arm locks securely at
during x-ray exposure. Maintain the greatest possible each position.
reasonable distance from the x-ray source and all scat-
tering material. It should not be necessary to place 1.3 Casters/Brakes. Verify that the casters turn
hands or fingers in the x-ray beam; if unavoidable, wear and swivel freely. Check the ease of steering of
lead gloves. Keep x-ray exposure time to a minimum. the C-arm stand and the display cart. Ensure
that caster brakes secure the stand from move-
Do not remove the high-voltage cables from the ment.
wells with the power on. Ensure that high-voltage
cables are completely discharged by repeatedly touch- 1.4 AC Plug/Receptacles. Examine the AC power
ing the conductor to ground as soon as it is removed plug for damage. Attempt to wiggle the blades to
from the well. Wear rubber gloves or other appropriate check that they are secure. Shake the plug, and
protection when exposed to blood or other body fluids. listen for rattles that could indicate loose screws.
If any damage is suspected, open the plug and
For repeated exposures, allow adequate time be- inspect it.
tween exposures to prevent overheating of the x-ray
tube. If the device has electrical receptacles for ac-
cessories, verify the presence of line power. In-
Procedure sert an AC plug into each receptacle, and check
that it is held firmly. If accessories are plugged
Before beginning an inspection, carefully read this and unplugged often, consider a full inspection
procedure and the manufacturer’s instructions and of the receptacles.
service manuals; ensure that you understand how to
operate the equipment, the significance of each control 1.5 Line Cord. Inspect the cord for signs of damage.
and indicator, and the alarm capabilities. Also deter- If damaged, replace the entire cord or, if the
mine whether any special inspection or preventive damage is near one end, cut out the defective
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Mobile C-arms
portion. Ensure that the remaining length is proper alignment, as well as positive stopping.
adequate. Be sure to wire a new power cord or During the course of the inspection, be sure to
plug with correct polarity. check that each control and switch performs its
proper function. For the fluoroscopic and radio-
1.6 Strain Reliefs. Examine the strain reliefs at graphic exposure switches, ensure that they do
both ends of the line cord. Be sure that they hold not stick and that continuous pressure is re-
the cord securely. quired to continue exposure. Release of pressure
1.7 Circuit Breaker/Fuse. If the device has an ex- should immediately terminate exposure.
ternal circuit breaker, check that it operates 1.18 Indicators/Displays. During the course of the
freely. If the device is protected by an external inspection, confirm the operation of all lamps,
fuse, check its value and type against that indicators, meters, gauges, and visual displays
marked on the chassis, and ensure that a spare on the unit. Examples of indicators and displays
is provided. are technique settings, image modes, fluoro-
1.9 Cables. Inspect any cables (e.g., between the scopic exposure time, x-rays on, display monitor
C-arm stand and display cart, from the C-arm, text, and image storage numbers.
connecting the footswitch) and their strain re- 1.20 Alarms. Induce conditions to activate audible
liefs for general condition. Carefully examine and visual alarms (e.g., x-rays on). Check that
cables to detect breaks in the insulation and to any associated interlocks (e.g., fluoroscopy inhi-
ensure that they are gripped securely in the bition) function. If the unit has an alarm silence
connectors at each end to prevent rotation or feature, check the method of reset (e.g., manual
other strain. Verify that there are no intermit- or automatic) against the manufacturer’s speci-
tent faults by flexing cables for the display near fications. It may not be possible to check out all
each end and looking for erratic operation. alarms at this time, since some may require
For units with rotating anode tubes, the high- abnormal operating conditions (e.g., long expo-
voltage cables should be removed from the wells, sure times). Instruct users to document activa-
and the ends and the wells should be cleaned, tion of these alarms to ensure that they are
coated with high-voltage compound, reinserted, functional.
and tightened securely. 1.21 Audible Signals. Operate the device to activate
1.10 Fittings/Connectors. Examine all electrical ca- any audible signals (e.g., radiographic exposure,
ble connectors for general condition. Electrical boost or high-level control fluoroscopy). Confirm
contact pins or surfaces should be straight, appropriate volume. If audible alarms have been
clean, and bright. Verify that leads and elec- silenced or the volume set too low, adjust alarm
trodes are firmly gripped in their appropriate volume to the appropriate level.
connectors. If keyed connectors are used, make 1.22 Labeling. Check that all necessary certification
sure that no pins are missing and that the keying labels, warning labels, technique charts, and
is correct. instruction cards are present and legible.
1.13 Controls/Switches. Before changing any con- 1.23 Accessories. Confirm the presence and condition
trols or alarm limits, check their positions. If any of accessories (e.g., film cassette holder, digital
setting appears inordinate (e.g., high mA set- acquisition systems, multiformat cameras, video
ting), consider the possibility of inappropriate printers).
clinical use or of incipient device failure. Record
the settings of those controls that should be 2. Quantitative tests
returned to their original positions following the
inspection. 2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with
Examine all controls and switches (x-ray in- good resolution of fractional ohms, measure and
itiation, collimation, image manipulation, tech- record the resistance between common ground
nique selection, size of image, etc.) for physical and exposed metal on the C-arm, the control
condition, secure mounting, and correct motion. stand, and the display cart. We recommend a
Check that control knobs, if present, have not maximum resistance of 0.5 Ω. The footswitch
slipped on their shafts. Where a control should does not need to be grounded if it operates from
operate against fixed-limit stops, check for low voltages.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
2.2 Leakage Current. Measure chassis leakage cur- calculated from the mAs values. Conduct meas-
rent to ground with the grounding conductor of urements at typically used low, medium, and
plug-connected equipment temporarily opened. high time settings. As a general rule, the differ-
Operate the device in all normal modes, includ- ence between the measured time and the preset
ing on, standby, during exposure, and off; record time should not exceed 1 ms or 5%, whichever is
the maximum leakage current. Chassis leakage greater.
current should be 300 µA or less. For older C-
arms, leakage current up to 500 µA is acceptable, 2.5 Linearity of mAs. Use an ionization chamber
provided that a documented maintenance sched- with an electrometer (or a combination exposure
ule is established to ensure grounding integrity; meter) to measure the exposure in mR for this
a three-month interval is a nominal period, but test. The ionization chamber should be placed
may be adjusted depending on intensity of use centrally in the x-ray beam. The image intensi-
and previous experience. fier should be covered with a lead plate to protect
it from excessive radiation.
2.3 Accuracy of kVp. Use a noninvasive kVp meter
that has previously been calibrated against a Dial up a midrange kVp setting (e.g., 80 kVp)
high-voltage divider on the type of generator with the C-arm set to operate in the radiographic
that powers the C-arm system. Use the kVp mode. Make radiographic exposures at this fixed
meter in accordance with the recommendations kVp, and record the exposure values (in mR)
of the manufacturer of the kVp meter. (These from the electrometer or exposure meter at a
may include the kind of filters to use and the minimum of three settings that span the range
distance at which the kVp meter has to be placed. typically used. Calculate the mR/mAs at each
Some meters require that the user specify the setting, and average the calculations. Each indi-
type of generator being tested and the amount of vidual mR/mAs value should be within 10% of
filtration present in the primary x-ray beam.) the average.
Take measurements in the radiographic and 2.6 Exposure Reproducibility. Use one of the above
fluoroscopic modes of operation of the C-arm at mR/mAs values as the one value to be used for
low, medium, and high settings (e.g., 60, 80, and evaluating short-term and long-term reproduci-
100 kVp). After the appropriate corrections have bility of the x-ray tube and the generator combi-
been applied to the measured kVp readings (e.g., nation. For the short-term test, make a
for filtration), the difference between the meas- minimum of four exposures at the same mAs
ured kVp and the preset kVp should not exceed over a span of approximately 15 minutes. The
5% of the preset kVp. If a consistent significant mR/mAs value should have a coefficient of vari-
error between the preset kVp and the measured ation no larger than 10%. For long-term repro-
kVp is detected, further testing with a high-volt- ducibility, simply record the current average
age divider may be required to identify the prob- mR/mAs value from the four values above and
lem. compare this with the value recorded during the
preceding inspection. It is critical that identical
2.4 Timer Accuracy. Use a noninvasive timer to test conditions be used for assessing reproduci-
measure the accuracy of the timer settings avail- bility. For example, the same chamber-to-source
able on the C-arm system when it is operated in distance should be used, and the technique (kVp,
the radiographic mode. Most noninvasive kVp mAs) should be the same. Long-term reproduci-
meters also display exposure times. Follow the bility should be within ±10% of the average.
manufacturer’s recommended technique for
making time measurements. Cover the image 2.7 Half-Value Layer (HVL). Use an ionization
intensifier with 6 mm thick lead plate to protect chamber, electrometer, and Type 1100 alumi-
the image intensifier and TV camera system. num filters for this test. Place the ionization
chamber on the image intensifier or at about 60
Once the unit has been appropriately set up, cm from the focal spot. Under fluoroscopic guid-
dial up a midrange kVp setting (e.g., 70 kVp). ance, adjust the collimation on the C-arm so that
The mobile C-arm may have a display only of the x-ray field just encompasses the ionization
mAs rather than exposure time. If this is the chamber.
case, consult the C-arm manuals to find out what
mA is being used at 70 kVp in the radiographic Set the C-arm to operate in the radiographic
mode. The exposure time readings can then be mode at 80 kVp. Select a midrange mAs value.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Mobile C-arms
These kVp and mAs values should be held con- inspections. The typical exposure rate is 1 R/min
stant during the whole course of this test. (with a range of 0.5 to 2.0 R/min). If the exposure
rate has increased from that of previous inspec-
Record the initial exposure value (in mR) with tions, further testing should be performed to
nothing in the primary beam (i.e., 0 mm of alu- determine the reason for the required increase
minum). Then record the exposure reading with in radiation.
aluminum thickness of 2 mm and 4 mm. The
thickness of aluminum required to reduce the 2.12 Maximum Fluoroscopic Exposure Rate. Use an
initial exposure reading by half is the half-value ionization chamber with an electrometer (or a
layer of the beam. The HVL is most accurately combination exposure meter) capable of measur-
read by plotting the measurements on semilog ing exposure rate. Place a thick lead plate (at
graphing paper. Plot the exposure values on the least 6 mm thick) over the image intensifier
logarithmic scale against the thickness of alumi- housing. Ensure that the whole input face of the
num on the linear scale. At 80 kVp, the HVL image intensifier is covered by the lead plate.
should be a minimum of 2.3 mm of aluminum. Place the ionization chamber 30 cm above the
The HVL measurement should be compared to image intensifier input plane.
measurements from previous inspections, since
a change in HVL may indicate tube deteriora- Record the exposure rate on the electrometer
or exposure meter during a fluoroscopic expo-
tion.
sure in the automatic mode, as well as in the
2.8 Collimation. Place a ruler with leaded 1 cm or manual mode at the highest technique. If the
1/2″ markers on the image intensifier housing, C-arm also has a “boost” or “high-level” control
and measure the visual field size (length and mode, record the exposure rate during a fluoro-
width) of the image intensifier on the display scopic exposure in this mode. For units that have
monitor during a fluoroscopic exposure using the only manually selectable kVp and mA settings,
largest available mode on the image intensifier. the exposure rate at the highest settings should
Next, place a large-format x-ray film (30 cm by not exceed 5 R/min. For units that have automat-
30 cm minimum) on the image intensifier hous- ic kVp and mA control, the exposure rate should
ing and make a fluoroscopic exposure, still using not exceed 10 R/min.
the largest available mode on the image intensi-
There are no governmental regulations that
fier. A fluoroscopic exposure of about five sec-
limit exposure rates under boost mode for de-
onds is likely to provide sufficient film
vices in use now. However, for devices manufac-
darkening. After the film has been processed,
tured in 1996 and after, the exposure rate in the
ensure that the dimensions of the x-ray beam
boost or high-level control mode should not ex-
measured on the film do not differ from the
ceed 20 R/min.
dimensions of the fluoroscopic image measured
with the lead ruler by more than 3% of the 2.13 Image Quality.
source-to-image distance (SID).
High-Contrast Resolution. Place the line-pair
2.11 Standard Fluoroscopic Exposure Rate. In addi- phantom on the grid. It should be placed at a
tion to verifying that the unit meets exposure 45-degree angle to the grid lines and raster
requirements, this test also verifies functioning lines of the TV system. At low kVp (ABS with
of the ABS system. nothing other than the line-pair phantom in
the field), determine the maximum line-pair
Use an ionization chamber with an electrome- resolution for all available field sizes. It may
ter (or a combination exposure meter) capable of be necessary to alter the brightness and con-
measuring exposure rate. Place the chamber or trast settings on the TV monitor to optimize
the meter 30 cm above the image intensifier the display for the visualized object. Resolu-
input plane. Place sufficient patient simulator tion should be at or above 1.2 lp/mm for a 22
material on the image intensifier that the tech- cm (9″) field of view (FOV) and 1.7 lp/mm for
nique tracks to about midrange (e.g., 70 kVp) in a 15 cm (6″) FOV.
the automatic fluoroscopic mode.
Low-Contrast Resolution. Ensure that the 1 mm
Run a fluoroscopic exposure, and record the piece of aluminum is next to the grid. Place the
exposure rate. Check for consistency of the expo- low-contrast phantom on the grid. The thicker
sure rate with those made during previous aluminum pieces should be on top of the 1 mm
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
thick plate. Initiate a fluoroscopic exposure 4. Acceptance Tests
under ABS control. On the 15 cm (6″) FOV,
Acceptance testing is typically performed by a medi-
the three smallest holes should be visible. It
cal physicist.
may be necessary to alter the brightness and
contrast settings on the TV monitor to opti-
mize the display for the visualized object.
Before returning to use
Ensure that all controls are set properly. Set alarms
3. Preventive Maintenance loud enough to alert personnel in the area in which the
device will be used. Other controls should be in their
3.1 Clean the exterior, as well as the interior if needed.
normal pre-use positions.
3.2 Lubricate per the manufacturer’s instructions.
Attach a Caution tag in a prominent position so that
3.3 Calibrate per the manufacturer’s instructions. the user will be aware that control settings may have
Adjust caster brakes and arm locks, if needed. been changed.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 468-0595
Mobile X-ray Units
Used For:
Radiographic Units, Mobile [13-272]
Also Called: Mobile radiographic systems, portable x-ray machines
Commonly Used In: Patient rooms, surgical suites
Scope: Applies to portable radiographic systems powered from or charged by a standard 115 VAC receptacle
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview exposure, the capacitor(s) must be recharged. In a
battery-powered generator, line power is used to
Mobile x-ray units are used for radiographic imaging charge lead-acid batteries; the fully charged unit can
of patients who cannot be moved to the radiology then be operated independently of an outside power
department and who are in areas, such as intensive source until the batteries need to be recharged. Bat-
care units or emergency rooms, that lack standard, tery-powered generators supply a constant kV and
fixed radiographic equipment. These units consist of current throughout the exposure.
an x-ray generator, an x-ray tube and tubestand, colli-
mators, and a film cassette storage drawer. Battery- The x-ray tube assembly, which includes the x-ray
powered units also contain a battery and charging tube and collimator, is attached to a tubestand that
system, and self-propelled units contain a motor drive. can be rotated about its base or moved horizontally and
vertically. The x-ray tube anode is either stationary or
One of three different types of x-ray generators can rotating. Filters are placed in the path of the x-ray
be used: a line-powered transformer, a capacitor-dis- beam to absorb the less penetrating x-rays. After the
charge generator, or a battery-powered transformer. beam passes through the filters, a set of collimators
Line-powered transformers use 120 or 220 VAC for confines the primary beam to the size and shape that
x-ray production. A step-up transformer increases the will cover the area of diagnostic interest.
voltage, and a rectifier converts the AC to the DC
required by the x-ray tube. In a capacitor-discharge Because of design constraints, tube current in
generator, 110 or 220 VAC power is fed into a step-up mobile units is often lower than in stationary radio-
transformer; the output is then rectified and used to graphic systems. Therefore, radiographs taken with
charge a large capacitor or group of capacitors, which mobile units are usually of poorer quality. Further-
are then discharged through a grid-controlled x-ray more, because patient positioning and film placement
tube. Because the capacitors are charged to the same are more difficult with bedside radiography, the over-
potential, each exposure begins at the same peak kilo- all image quality is lower, as well. Mobile radiographic
voltage (kVp), but the kV will decrease during expo- units are designed for use only when patient transport
sure as the capacitor discharges. At the end of each is contraindicated; the radiology department, with
241473 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
468-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
fixedradiographic equipment, offers a more controlled, maintenance procedures or frequencies are recom-
optimal setting for imaging. mended by the manufacturer.
Test apparatus and supplies This procedure is intended to ensure adequate sys-
tem performance and maintenance. It should not be
Ground resistance ohmmeter construed as providing full compliance with the re-
Leakage current meter or electrical safety analyzer quirements of all governmental regulations and ac-
Noninvasive kVp meter (compatible with the x-ray creditation standards of professional associations.
generator being inspected) Such regulations and standards may include testing
beyond that provided below and may also require docu-
Noninvasive timer (may be included with the kVp mentation by a certified medical physicist.
meter)
For acceptance testing, we strongly recommend us-
Ionization chamber with electrometer or a combina-
ing a medical physicist. Acceptance testing is crucial
tion exposure meter
because it generates data on baseline performance of
Five filters of 10 cm × 10 cm × 1 mm Type 1100 the device.
aluminum
Collimator alignment template marked in centime- 1. Qualitative tests
ters or inches 1.1 Chassis/Housing. Examine the exterior of all
Medium-format x-ray film (25 cm × 30 cm or 10″ × 12″) components of the portable x-ray unit for clean-
liness and general physical condition. Be sure
Ten pieces of 30 cm × 30 cm × 2.5 cm plexiglass (or
that all hardware is present and tight, and that
another patient-simulating material for testing the
there are no signs of spilled liquids, deep
automatic exposure control [AEC])
scratches, dents, or other serious abuse. Check
Densitometer the mechanical operation of all moving parts to
Oscilloscope (calibration only) include any film storage compartment, as well as
all movements of the x-ray tube, x-ray tube sup-
High-voltage divider (calibration only)
port, and collimator, ensuring that all move-
ments are smooth with no binding or undue
Special precautions resistance.
Wear a lead apron and thyroid shield. Maintain the
greatest possible reasonable distance from the x-ray 1.3 Casters/Brakes. Verify that the casters turn
source and all scattering material during all x-ray and swivel freely. Look for accumulations of dirt
exposures. It should not be necessary to place hands or and grime around the casters. Check the ease of
fingers in the x-ray beam. If this is unavoidable, wear steering. Check the brake or locking device for
lead gloves. each movement of the x-ray tube, x-ray tube
support, and collimator. Ensure that all locks
Do not remove the high-voltage cables from the function properly and hold securely.
wells with the power on. Ensure that high-voltage
cables are completely discharged by repeatedly touch- 1.4 AC Plug/Receptacles. Examine the AC power
ing the conductor to ground as soon as it is removed plug for damage and ensure that the AC plug is
from the well. clamped securely to the line cord. If you find
evidence that the plug is being removed from the
Wear rubber gloves or other appropriate protection receptacle by pulling on the cord, caution users
when exposed to blood or other body fluids. against this practice. Attempt to wiggle the
Allow adequate time between repeated exposures to blades to check that they are secure. Shake the
prevent overheating of the x-ray tube. plug and listen for rattles that could indicate
loose screws. If any damage is suspected, open
Procedure the plug and inspect it.
Before beginning an inspection, carefully read this 1.5 Line Cord. Inspect the cord for signs of damage.
procedure and the manufacturer’s instruction and If damaged, replace the entire cord or, if the
service manuals; ensure that you understand how to damage is near one end, cut out the defective
operate the equipment, the significance of each control portion. Ensure that the remaining length is
and indicator, and the alarm capabilities. Also deter- adequate. Be sure to wire a new power cord or
mine whether any special inspection or preventive plug with correct polarity.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Mobile X-ray Units
1.6 Strain Reliefs. Examine the strain reliefs at stick, that continuous pressure is required to
both ends of the line cord. Be sure that they hold continue exposure, and that release of pressure
the cord securely. immediately terminates exposure. Ensure the
proper operation of the two-position exposure
1.7 Circuit Breaker/Fuse. If the device has an exter- switch (i.e., ensure that the x-ray exposure is not
nal circuit breaker, check that it operates freely. If released by the first trigger only), if present.
the device is protected by an external fuse, check
its value and type against that marked on the 1.17 Battery/Charger. Using a multimeter, measure
chassis and ensure that a spare is provided. the battery voltage. (Consult the manufacturer’s
documentation for appropriate measuring
1.9 Cables. Inspect any cables (e.g., collimator ca- points.) Verify that the level of charge is accu-
bles, high-voltage cables) and their strain reliefs rately represented by the level-of-charge indica-
for general condition. Carefully examine cables tor on the operator’s panel. Verify that the
to detect breaks in the insulation and to ensure battery charger automatically stops charging
that they are gripped securely in the connectors when the appropriate state of charge is reached.
at each end to prevent rotation or other strain. Ensure that any cooling or ventilation fans oper-
For cables other than high-voltage cables, verify ate properly.
that there are no intermittent faults by flexing
electrical cables near each end and looking for 1.18 Indicators/Displays. During the inspection,
erratic operation. Use an ohmmeter if a problem confirm the operation of all lamps, indicators,
is suspected. High-voltage cables should be re- meters, gauges, and visual displays on the unit.
moved from the wells (at the x-ray tube ends), Examples of indicators and displays are tech-
cleaned, coated with high-voltage compound, re- nique settings, exposure time, and x-ray on. In-
inserted, and tightened securely. The high-volt- spect the source-to-image distance (SID)
age transformer end should not require routine indicator (usually a tape measure). Ensure that
inspection if the wells are vertical and high-volt- it is present, operates smoothly, and is accurate.
age oil is used.
1.20 Alarms. Induce conditions to activate audible and
1.10 Fittings/Connectors. Examine all electrical cable visual alarms (e.g., x-ray on). Check that any asso-
connectors for general condition. Electrical contact ciated interlocks (e.g., x-ray tube park) function. If
pins or surfaces should be straight, clean, and the unit has an alarm silence feature, check the
bright. If keyed connectors are used, make sure method of reset (e.g., manual or automatic) against
that no pins are missing and that keying is correct. the manufacturer’s specifications. It may not be
possible to check out all alarms at this time, since
1.12 Filters. Check the condition of any air filters some may require abnormal operating conditions.
present in the systems. Clean or replace as Instruct users to document activation of these
needed. alarms to ensure that they are functional.
1.13 Controls/Switches. Before changing any con- 1.21 Audible Signals. Operate the device to activate
trols or alarm limits, check their positions. If any audible signals (e.g., radiographic exposure,
any settings appear inordinate (e.g., high mA audible signal during motorized drive if applica-
setting), consider the possibility of inappropri- ble). Confirm appropriate volume. If audible
ate clinical use or of incipient device failure. alarms have been silenced or the volume set too
Record the setting of those controls that should low, adjust alarm volume to the appropriate level.
be returned to their original positions following
the inspection. Examine all controls and 1.22 Labeling. Check that all necessary certification
switches (x-ray initiation, collimation, tech- labels, warning labels, technique charts, and
nique selection, etc.) for physical condition, se- instruction cards are present and legible.
cure mounting, and correct motion. Check that 1.23 Accessories. Confirm the presence and condition
control knobs, if present, have not slipped on of accessories (e.g., film cassette holder).
their shafts. Where a control should operate
against fixed-limit stops, check for proper align- 1.24 Drive Mechanism (for motor-powered units only).
ment, as well as positive stopping. During the Ensure that the drive system operates smoothly,
inspection, be sure to check that each control does not pull to one side or the other, and makes
and switch performs its proper function. Ensure no unusual noises (e.g., apparent binding,
that radiographic exposure switches do not squeaking). If there are variable-speed controls
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
present, test their operation. Verify that the been appropriately set up, dial up a midrange
bumper switches disable the drive circuitry for kVp setting (e.g., 80 kVp). The unit may have a
both forward and reverse motions. Verify that display only of mAs rather than exposure time.
any interlocks associated with the drive circuitry If this is the case, consult the instruction and
are functional (e.g., that an x-ray tube not in service manuals to find out what mA is being
park position allows slow drive only, that the used at 80 kVp. The exposure time readings can
main drive handle must be depressed or then be calculated from the mAs values. Conduct
squeezed to allow movement). measurements at typical low, medium, and high
settings. The difference between the measured
2. Quantitative tests time and the preset time should not exceed ±1
msec or ±5%, whichever is greater.
2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with 2.5 Linearity of mAs. Use an ionization chamber
good resolution of fractional ohms, measure and with an electrometer (or a combination exposure
record the resistance between common ground meter) to measure the exposure in mR for this
and exposed metal on the portable x-ray unit. We test. The ionization chamber should be placed
recommend a maximum resistance of 0.5 Ω. centrally in the x-ray beam at a known standard
2.2 Leakage Current. Measure chassis leakage cur- distance from the focal spot (e.g., 100 cm). Dial
rent to ground with the grounding conductor of up a midrange kVp setting (e.g., 80 kVp). Make
plug-connected equipment temporarily opened. radiographic exposures at this fixed kVp and
Operate the device in all normal modes, includ- record the exposure values (in mR) from the
ing on, standby, exposure, and off, and record the electrometer or exposure meter at a minimum of
maximum leakage current. Chassis leakage cur- three mA settings that span the range commonly
rent should be 300 µA or less. For older portable used for a generator with variable mA. Also use
x-ray units, up to 500 µA is acceptable, provided three mAs settings for constant mA generators.
that a documented maintenance schedule is es- Calculate the mR/mAs at each setting and aver-
tablished to ensure grounding integrity; three age the calculations. Each individual mR/mAs
months is an acceptable interval, but may be value should be within 10% of the average.
adjusted depending on the intensity of use and
2.6 Exposure Reproducibility. Use one of the above
on previous experience.
mR/mAs values as the one value to be used for
2.3 Accuracy of kVp. Use a noninvasive kVp meter evaluating short-term and long-term reproduci-
that has previously been calibrated against a high- bility of exposure. For the short-term test, make
voltage divider on the type of generator that pow- a minimum of four exposures at the same mAs
ers the portable x-ray unit. Use the meter in over a span of 15 minutes. The mR/mAs values
accordance with the manufacturer’s recommenda- should have a coefficient of variation no larger
tions. (These may include the kind of filters to use than 10%. For long-term reproducibility, simply
and the distance at which the kVp meter has to be record the current average mR/mAs value, and
placed. Some meters require that the user specify compare it with the value recorded during the
the type of generator being tested and the amount preceding inspection. It is critical that identical
of filtration present in the primary x-ray beam.) test conditions be used for assessing reproduci-
Make measurements at low, medium, and high bility. For example, the same chamber-to-source
settings (e.g., 60, 80, 100 kVp). After the appropri- distance should be used, and the technique (kVp,
ate corrections have been applied to the measured mAs) should be the same. Long-term reproduci-
kVp readings (e.g., for filtration), the difference bility should be within ±10% of the average.
between the measured kVp and the preset kVp
should not exceed ±5% of the preset kVp. 2.7 Half-Value Layer (HVL). Use an ionization
chamber, electrometer, and Type 1100 alumi-
2.4 Timer Accuracy. Use a noninvasive timer to num filters for this test. Place the ionization
measure the accuracy of the time settings avail- chamber in the center of the x-ray beam at about
able on the unit when it is operated in the 100 cm from the focal spot. Collimate so that the
radiographic mode. Most noninvasive kVp me- x-ray field just encompasses the ionization
ters also display exposure times. Follow the chamber. Set the unit to operate at 80 kVp.
manufacturer’s recommended technique for Select a midrange mAs value. These kVp, mAs
making time measurements. Once the unit has values should be held constant during the whole
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Mobile X-ray Units
course of this test. Record the initial exposure the processed film. The sum of W1 + W2 + L1
value (in mR) with nothing in the primary beam + L2 is the total misalignment between the
(i.e., 0 mm of aluminum). Then record the expo- light field and the x-ray field. This sum must
sure reading with aluminum thicknesses of 2 mm not exceed 2% of the SID; that is, at an SID of
and 4 mm. The thickness of aluminum required 100 cm, the misalignment should not exceed
to reduce the initial exposure reading by half is 2 cm. See Figure 1.
the HVL of the beam. The HVL is most accurately
Field size indicators versus actual exposed area.
read by plotting the measurements on semilog
Measure the length and width of the exposed
graphing paper. Plot the exposure values on the
area on the exposed film. Compare the actual
logarithmic scale against the thickness of alumi-
size of the exposed area to the readout of the
num on the linear scale. At 80 kVp, the HVL
exposure area size indicators noted earlier.
should be a minimum of 2.3 mm of aluminum.
The dimensions of the exposed area must be
The HVL measurement should be compared to
within 2% of the SID — that is, 2 cm at an SID
measurements from previous inspections since a
of 100 cm.
change in HVL may indicate tube deterioration.
2.8 Collimation. Place a medium-format x-ray film 2.9 AEC Object Thickness Compensation (for units
(25 cm × 30 cm or 10″ × 12″), at an SID of 100 cm provided with an AEC system). This test is to be
(40″). Ensure that the x-ray film is perpendicular conducted on each available radiographic image
to the x-ray beam. Precisely center the collimator receptor holder (e.g., spot-film, table Bucky, wall
alignment tool on the cassette. Turn on the col- Bucky). Place 20 cm of 30 cm × 30 cm plexiglass
limator light and collimate to an area of 20 cm × on the table or support it up against the wall
20 cm. Ensure that the light beam is exactly Bucky. (It is acceptable to use another patient
centered on the collimator alignment tool. Note simulating material for AEC tests, such as alu-
the exact readout of the exposure area size indi- minum.) Ensure that the plexiglass covers the
cators. Record the exact size of the illuminated AEC detectors. Set the unit to operate at 80 kVp
boundaries from the collimator alignment tool. (or some other setting commonly used to image a
Make an x-ray exposure (for a film/screen speed medium-sized patient). Load a cassette of a size
of 400, a technique of 55 kVp and 5 mAs should commonly used with the standard film used at
be sufficient), and process the x-ray film. the facility, and place this into the receptor holder
being tested. Then make an AEC-controlled ex-
Congruence of the light field to the x-ray field. posure. Process the film on a processor that has
Measure the distances L1, L2, W1, and W2 on previously been verified as operating optimally.
″ ″
Figure 1. Schematic showing misalignment of the light field with respect to the x-ray field
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
Use a densitometer to measure the optical den- The optical density of the films at all kVp set-
sity of the radiograph in the center of the image. tings checked should agree to within ±0.3 OD.
If the optical density falls within the range cho-
sen by the radiologists (typically 1.2-1.4 OD), 3. Preventive maintenance
repeat the test using identical setup conditions 3.1 Clean the exterior and interior. Take precau-
but with varying amounts of plexiglass in the tions when dealing with body fluids.
beam. At a minimum, check the optical density
at 15 cm and 25 cm of plexiglass. All films used 3.2 Lubricate per the manufacturer’s instructions.
in this test should come from the same batch,
3.3 Calibrate the system to ensure performance
and only one cassette is to be used for all expo-
within the manufacturer’s specifications, at in-
sures. The optical density of all the processed
tervals recommended by the manufacturer or as
films should agree to within ±0.3 OD of the
indicated by inspection results. Adjust all brakes
optical density at 20 cm.
and locks to ensure proper performance.
2.10 AEC kVp Compensation (for units provided with
3.4 Replace components if needed.
an AEC system). This test should also be con-
ducted on each available radiographic image re- 4. Acceptance Tests
ceptor holder (spot-film, table Bucky, and wall
Bucky). Place 20 cm of plexiglass (or some other Acceptance testing is typically performed by a medi-
patient simulating material) on the table or sup- cal physicist.
port it up against the wall Bucky. Ensure that
the AEC detectors are covered by the plexiglass. Before returning to use
Use the most common size of films in the same Ensure that all controls are set properly. Set alarms
cassette holder for all checks in this test. Make loud enough to alert personnel in the area in which the
a series of AEC-controlled exposures of the 20 cm device will be used. Other controls should be in their
of plexiglass at different kVp values. At a mini- normal pre-use positions. Attach a Caution tag in a
mum, use three kVp settings (e.g., 60, 80, 100 prominent position so that the user will be aware that
kVp). For each exposure, process the film on an control settings may have been changed. Recharge
optimally performing processor. Read the optical battery-powered devices or equip them with fresh bat-
density of the radiograph using a densitometer. teries, if needed.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 447-0595
Nd:YAG Surgical Lasers
Used For:
Lasers, Surgical, Nd:YAG [16-943]
Also Called: YAG lasers (incorrectly), continuous-wave YAG lasers, surgical lasers, urology lasers,
angioplasty lasers, bronchopulmonary lasers, gastroenterology lasers, neurosurgical lasers, photocoagulator
lasers
Commonly Used In: Operating rooms, short procedure areas, cystology rooms, catheterization labora-
tories, endoscopy laboratories, radiology areas
Scope: Applies to general-purpose Nd:YAG surgical lasers that include contact (e.g., sapphire tip) and/or
noncontact flexible fiberoptic delivery systems (either reusable or disposable), emit near-infrared energy at
1,064 nm, and can provide sufficient power output to coagulate and vaporize tissue; applies to low- and
high-power Nd:YAG surgical lasers that are typically used for general surgery, urology, cardiovascular surgery,
gastroenterology, bronchopulmonary, neurosurgery, gynecology, ENT, and plastic surgery procedures; applies
to the Nd:YAG portion of units that combine the Nd:YAG wavelength with other wavelengths (e.g., KTP or
CO2); does not apply to ophthalmic Nd:YAG lasers or to Nd:YAG lasers that are, for example, frequency-
doubled and do not emit energy for delivery to the patient at 1,064 nm (frequency-doubled units are covered
in Procedure/Checklist 464); also does not apply to CO2 lasers, argon lasers, or other ophthalmic lasers;
however, many of the tests listed herein can be used or modified for these other lasers
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview sers must be meticulously maintained to ensure proper
and safe operation.
Nd:YAG lasers are normally checked before each use
by the laser’s power-on self-test and by user examina- Nd:YAG surgical lasers affect tissue by delivering
tion of the aiming beam and calibration of the system invisible near-infrared energy at a sufficient power den-
with the delivery system to be used. This minimizes sity to cause photocoagulation, thermal denaturation,
the need for frequent additional periodic testing. and/or vaporization of tissue. The 1,064 nm Nd:YAG
energy is not well absorbed by any tissue and is typically
Manufacturers or outside service vendors often scattered over a 5 mm depth within tissue. Nd:YAG
maintain lasers for hospitals. The extent and fre- surgical lasers are frequently used to cause photocoagu-
quency of inspection by hospital personnel should be lation or thermal denaturation of tissue in the noncon-
coordinated with these outside services. tact mode or with quartz or sapphire contact tips.
Failure of an Nd:YAG surgical laser can cause pa- General-purpose Nd:YAG surgical lasers have a
tient or staff injury, abrupt interruption of a surgical laser cavity that houses an yttrium-aluminum-garnet
procedure, or damage to the laser system. These la- (YAG) crystalline rod that is doped with neodymium
046828 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
447-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
(Nd). Energy leaving the laser tube through a partially beam pattern introduced by an accessory would be
reflecting mirror is typically directed into a flexible opti- apparent by examining the visible aiming beam.
cal fiber that transmits the laser energy to the tissue. The
fiber may be used with additional connectors (e.g., Citations from Health Devices
through an endoscope), with contact tips or contact-tip Lasers in medicine: An introduction, 1984 Jun;
fibers connected, and/or with a laser handpiece or a laser 13:151-78.
micromanipulator (used to interface the laser with the
surgical microscope) connected. These attachments can Lasers as investigational devices: Appendix A, 1984
focus the energy into a small spot size at a known Jun; 13:167-9.
working distance or a specific beam pattern to accom-
Lasers: Model policy and procedures statement: Ap-
plish a specific task. In a few cases (e.g., the Trimedyne
pendix B, 1984 Jun; 13:169-71.
Laserprobes SLT contact tips), the laser energy is trans-
formed into thermal energy to heat a catheter tip, which Loss of metal nozzle on Nd:YAG surgical laser fibers
then causes the clinical effect; in this case, no or very little [User Experience NetworkTM], 1987 Mar-Apr; 16:115.
direct laser irradiation of tissue occurs.
Fatal gas embolism associated with intrauterine laser
Because the near-infrared energy emitted by the surgery [Hazard], 1989 Sep; 18:325-6.
Nd:YAG laser is invisible, a second, nontherapeutic Surgical lasers [Evaluation], 1991 Jul-Aug; 20:239-316.
aiming helium-neon (He-Ne) laser — which emits vis-
ible red light — a red diode laser, or a xenon lamp with Test apparatus and supplies
filters to emit white or blue light simultaneously trave-
rses the fiber and is coincident (i.e., travels the same Leakage current meter or electrical safety analyzer
path) with the Nd:YAG laser beam. Ground resistance ohmmeter
New, unused fiber delivery system
Like most lasers, Nd:YAG lasers are inefficient in
converting electrical energy into laser energy of 0 to 140 Black Delrin block ≥1⁄2″ thick, ≥1″ wide, about 3″ to
W. As a result, excess heat is generated in the laser 4″ long; tongue depressors; or firebrick
tube, requiring a cooling system. Some Nd:YAG lasers Laser radiometer (power meter)
use internal water/air cooling systems, while others
require external connection to a water source and drain Laser safety signs
or to a freestanding cooling system. Most Nd:YAG laser Laser safety eyewear specifically designed for use
fibers require gas or liquid cooling as well for certain with Nd:YAG surgical lasers and of sufficient opti-
applications. As a result, gas compressors/regulators cal density to protect the wearer’s eyes from laser
and/or fluid pumps are typically integral or attached to injury
these lasers. Because Nd:YAG laser fibers may be used Vise with padded jaws or ring stand with padded
in body cavities (e.g., during gastroscopy), some lasers clamp
may include a gas recirculation system that inserts gas
to cool the fiber and/or insufflate the cavity and with- Pressure gauges and coolant system tee fitting
draw gas to limit pressure and avoid distension. Outlet test fixture (optional)
Insulating gloves, high voltage (optional)
With Nd:YAG lasers, unlike those lasers that use
mirror delivery systems (e.g., articulating arms on CO2 Grounding strap (optional)
lasers), it is not necessary to periodically verify coinci- Calibrated flowmeter
dence of the aiming and therapeutic beam or to assess
the therapeutic beam pattern (e.g., TEM00) within the Special precautions
beam or spot. Since the therapeutic and aiming laser Inspecting and maintaining lasers is a dangerous as
beams are transmitted through a single optical fiber, well as necessary process, and far greater care is
these two beams are coincident as they exit the fiber. required than with most devices. Personnel who in-
Any beam pattern distortion at the fiber entrance spect or service lasers should receive special training
would be eliminated as the laser beams travel through from the manufacturer or from a qualified alternative
the fiber because of internal reflections within the training source.
fiber. Misalignment of the beam at the fiber entrance
would result in decreased power output or loss or Laser energy can cause serious injury, particularly
distortion of the aiming beam. In a well-aligned sys- when the internal interlock is overridden or in any
tem, any significant problem with the therapeutic other situation in which the energy does not diverge
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Nd:YAG Surgical Lasers
significantly over long distances. Under some circum- Some surgical lasers use high voltages (e.g., 20 kV),
stances, the beam may not diverge significantly, even which can be lethal. Capacitors may store charges
a full room length or more away from the laser (and long after the device has been disconnected from line
can harm tissue or burn material even at this dis- voltage. Consult the manufacturer’s recommended
tance). Therefore, exercise great care whenever a laser procedures for servicing high-voltage laser circuits,
beam is accessible. Area security and use of personnel and avoid contact with any portion of the high-voltage
protective devices and practices should be consistent circuit until you are certain that the charge has been
with hospitalwide laser safety procedures and/or be drained. In such instances, a good ground must be
approved by the laser safety committee. present; preferably, use a redundant ground strap if
you must enter the laser cabinet. When possible, dis-
In addition, windows should be covered with nonre- connect the laser from line voltage before entering the
flective material to prevent transmission of laser en- laser cabinet, and use insulated gloves for those proce-
ergy to other areas. dures in which contact with a high-voltage source is
possible (and the gloves are not otherwise contraindi-
Wear appropriate laser safety eyewear at all times cated). Ensure that equipment intended to be used to
whenever the laser is in the Operating mode. WARN- measure, drain, or insulate high voltages carries the
ING: Laser safety eyewear may not protect the wearer appropriate insulation rating (e.g., above 20 kV).
from the aiming system light. Do not stare directly into
the aiming system beam or the therapeutic laser beam, Where possible, perform tests with the unit turned
even when wearing laser safety eyewear. Avoid placing off. Because of the presence of high voltage, perform
the laser beam path at eye level (i.e., when kneeling, the Grounding Resistance test (Item 2.1) before any
sitting, or standing). other item that requires operation of the laser.
WARNING: Do not use an anesthesia or other simi-
Do not perform these procedures when a patient is
lar bag that may have a mold-release agent (e.g., starch,
present or clinical staff is working, and do not aim the
talc) on its inside surface because the agent could
laser across a path that a person might normally use
contaminate the gas recirculation system of the laser
as a thoroughfare. Furthermore, at minimum, post
and ultimately contaminate a patient wound during a
doors to the room with appropriate laser safety signs
subsequent procedure.
stating that the laser is in use and that it is unsafe to
enter the room without authorization by the service Report any laser accident immediately to the laser
person performing the procedure. A second person safety officer or equivalent, as well as to the hospital
should be present, especially during procedures of rec- risk manager.
ognized risk, to summon help in case of an accident.
Procedure
The laser should remain in the Off position when Before beginning the inspection, carefully read this
not in use. When in use, the laser should be in the procedure and the manufacturer’s instruction and serv-
Standby/Disabled mode. Do not switch it to the Oper- ice manual; be sure that you understand how to operate
ating mode until the procedure is about to begin and the equipment, the significance of each control and indi-
the laser and its delivery system are properly posi- cator, and precautions needed to ensure safety and avoid
tioned. If the procedure must be interrupted, discon- equipment damage. Also determine whether any special
nect the laser from line voltage, and remove the laser inspection or preventive maintenance procedures or fre-
operation key and store it in a controlled location. quencies are recommended by the manufacturer.
Do not use the laser in the presence of flammable 1. Qualitative tests
anesthetics or other volatile substances or materials
(e.g., alcohol), or in an oxygen-enriched atmosphere, be- 1.1 Chassis/Housing.
cause of the serious risk of explosion and fire. Remove General. Verify that the key has not been left in
from the working area or cover with flame-resistant the laser. (Remove it if it has, and inform
opaque material all reflective surfaces likely to be con- users of the importance of storing the key in a
tacted by the laser beam. Whenever possible, use a controlled location.) Examine any external
firebrick or other nonflammable material behind the gas tanks that may be in use with the laser,
target material (e.g., black Delrin) when the laser is to and ensure that they have been turned off
be activated. Target materials will ignite when exposed after the last use. Examine the exterior of the
to high laser energies; use short durations when practi- unit for cleanliness and general physical con-
cal. A CO2 fire extinguisher should be readily available. dition. Be sure that all housings are intact
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
and properly aligned, that assembly hardware kink, trail on the floor, or be caught in moving
is present and tight, that any retractable parts parts; and that they are secured adequately to
slide easily and lock in place if so constructed, any connectors.
that there are no signs of spilled liquids or other
evidence of abuse, and that there are no obvious 1.9 Cables. Inspect all cables and their channels or
signs of water or oil leakage. strain reliefs for general physical condition. Ex-
amine cables carefully to detect breaks in insu-
Shutters. If manual shutters for the aiming sys- lation and to ensure that they are gripped
tem or therapeutic laser are accessible, en- securely in the connectors at each end to prevent
sure that they operate smoothly and correctly. strain on the cable.
Be sure to leave the shutter in the proper
position for normal operation. 1.10 Fittings/Connectors. E xam ine all optical
(e.g., fiber), gas, liquid, and electrical fittings
1.2 Mounts/Holders. Check that the mounts se- and connectors for general physical condition.
curely contain any gas cylinders that may be in Gas and liquid fittings should be tight and not
use. Be sure that mounts or holders intended to leak. Electrical contacts should be straight,
secure the fiber to the fiber support (to protect clean, and bright.
the fiber when in use) are present, in good work-
ing order, and being used. Similarly, check There should be no visible dirt or residue in
mounts or holders for other devices (e.g., exter- the optical path of the laser aperture. Ensure
nal power meters, footswitches). that any mechanism to close off the fiber laser
aperture (fiber port) is clean, operates smoothly,
1.3 Casters/Brakes. Check that the casters roll and
and is in use.
swivel freely. Check the operation of brakes and
swivel locks. If external gas tanks or wall-supply outlets
can be used, gas-specific connectors should be
1.4 AC Plug/Receptacle. Examine the AC power
present. Be sure that no pins are missing from
plug for damage. Wiggle the blades to deter-
yokes and that the keying and indexing of con-
mine whether they are secure. Shake the plug,
nectors for each gas to be used is correct. A laser
and listen for rattles that could indicate loose
that connects to a central piped medical gas
screws. If you suspect damage, open the plug
system or to a freestanding medical gas system
and inspect it.
should have the matching DISS or quick-connect
1.5 Line Cords. Inspect line cords for signs of dam- fitting for the gas that it is to be used with.
age. If a cord is damaged, replace the entire cord, Verify that suitable connectors are supplied so
or, if the damage is very near one end, cut out that adapters are not required.
the defective portion. Be sure to wire a new
power cord or plug with the correct polarity. 1.12 Filters. Check the condition of all liquid and air
filters. Some Nd:YAG surgical lasers require
1.6 Strain Reliefs. Examine the strain reliefs at deionized water, and most require special filtra-
both ends of the line cord. Be sure that they grip tion. Measuring the pressure drop across a liquid
the cord securely. filter can be helpful in determining whether the
filter should be replaced. Clean or replace filters
1.7 Circuit Breakers/Fuses. If the device has a
according to the manufacturer’s recommenda-
switch-type circuit breaker, check that it moves
tions (e.g., replace if the pressure drop is >5 psi),
freely. If the device is protected by an external
and indicate this in the preventive maintenance
fuse(s), check its value and type against what is
section of the inspection form. Clean or replace
marked on the chassis or noted in the instruction
air filters and radiators that are obviously dirty.
or service manual. Ensure that a spare is pro-
vided or readily available. 1.13 Controls/Switches.
1.8 Tubes/Hoses. Check the condition of all cool- General. Before moving any controls, check and
ing-system hoses and any other hoses or tubing record their positions. If any position ap-
the laser may have (e.g., drain, gas). Check that pears unusual, consider the possibility of in-
they are of the correct type; that they have not appropriate use or of incipient device failure.
become cracked and do not show other signs of Examine all controls and switches for physical
significant abuse; that they are connected cor- condition, secure mounting, and correct mo-
rectly and positioned so that they will not leak, tion. If a control has fixed-limit stops, check
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Nd:YAG Surgical Lasers
for proper alignment, as well as positive stop- 1.15 Motors/Pumps/Fans/Compressors. Check the
ping. Check membrane switches for tape resi- physical condition and proper operation of these
due and for membrane damage (e.g., from components, if present. If lubrication is required,
fingernails, pens, surgical instruments). If note this in the preventive maintenance section
you find such evidence, notify users to avoid of the inspection form. Clean any obvious dust
using tape and sharp instruments. During the from these components.
inspection, be sure that each control and
1.16 Fluid Levels. Check all fluid (e.g., coolant) levels.
switch works properly.
Refill or change the fluid according to the manu-
Remote. Examine the exterior of the control for facturer’s recommendations, and note this in the
cleanliness and general physical condition. preventive maintenance section of the inspection
Be sure that housings are intact, that assem- form. If an external water supply is in use, ensure
bly hardware is present and tight, and that that the water pressure is properly regulated and
there are no signs of spilled liquids or other at the appropriate pressure and that the supply
serious abuse. If the remote control is at- and drain system is properly configured (e.g.,
tached by cable to the laser, ensure that the filters are oriented for proper flow, drain hoses
cable and any connectors are in good condi- are positioned in a sink or drain).
tion. Examine all controls and switches for
general physical condition, secure mounting, 1.17 Battery. If a remote control or display is battery
correct motion, and intended range of set- powered, check or replace the battery (periodic
tings. Where a control should operate against prophylactic battery replacement is often pre-
fixed-limit stops, check for proper alignment, ferred to risking battery failure during use).
as well as positive stopping. During the in- Other batteries, such as those used to provide
spection, be sure to check that each control additional power for 110 VAC Nd:YAG lasers,
and switch performs properly. should be inspected according to the manufac-
turer’s recommendations. When it is necessary
Footswitch. Examine the footswitch for general
to replace a battery, label it with the date.
physical condition, including evidence of
spilled liquids. Footswitches for lasers in- 1.18 Indicators/Displays. During the course of the in-
clude an internal switch that activates accord- spection, verify proper operation of all lights, indi-
ing to the depth of pedal depression. It is cators, meters, gauges, and visual displays on the
usually possible to feel the vibration caused unit and remote control. Ensure that all segments
by closure of the switch, even through a shoe. of a digital display function. Note any error mes-
Check that the internal switch is operating sages displayed during the power-on self-test.
and that the footswitch does not stick in the
On position. Some footswitches include two If primary and remote-control indicators and
internal switches; in this case, verify the op- displays can be used at the same time or if
eration of both. Some footswitches also in- control can be switched from one to the other
clude a switch to operate the liquid- or during a procedure, operate the laser in a way
gas-cooling system. Check to be sure that this that will verify that the same information (e.g.,
switch operates reliably. settings, displays) is indicated on both controls.
During the procedure, check to be sure that If display screens or digital displays are pro-
the laser activates and deactivates consistently vided for user prompts or for viewing accumu-
when the footswitch is depressed and that the lated information (e.g., pulse or accumulated
fiber-coolant system operates properly when energy counter), ensure that each display pro-
the fiber-coolant switch is activated and deacti- vides the information expected. Ensure that user
vated. Flex the cable at the entry to the switch, prompts occur in the proper sequence. Store
and, using an ohmmeter, check for internal wire some sample information, and verify that it is
breaks that cause intermittent operation. Con- correct. If a feature to manually reset this infor-
firm that strain reliefs are secure. mation is available, ensure that it works.
Examine the male and female connectors for 1.19 Laser Delivery System Calibration. Nd:YAG surgi-
attaching the footswitch to the laser cabinet to cal lasers typically include a user-accessible calibra-
be sure that no pins are bent and that no other tion port leading to an internal power meter that
damage is present. Ensure that the connector allows output calibration and testing of the laser
secures acceptably to the laser cabinet. fiber. This feature is provided because transmis-
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
sion of laser energy through a fiber can change Set up reusable accessories with the laser to
in response to fiber use. Based on the measure- ensure compatibility and proper functioning.
ment from the calibration power meter, the laser
Checking all fibers or accessories during a
may automatically recalibrate itself and/or ad-
single inspection and preventive mainte-
just displays so that the power indicated to be
nance procedure is unnecessary as long as
delivered to the patient will be correct; or it may
accessories are routinely checked by the per-
require the user to do this manually. Verify that
son(s) responsible for laser setup and opera-
this feature is functioning by using the manufac-
tion. In addition, many of the accessories are
turer’s recommended calibration procedure to
sterile and would require resterilization be-
test one delivery system (e.g., fiber, handpiece)
fore use, making the laser potentially un-
that the manufacturer indicates can be accept-
available. Be sure to check with the person
ably calibrated using these procedures. (Contact
responsible for scheduling the use of the laser
tips cannot be calibrated using the laser’s cali-
before beginning the procedure.
bration power meter.)
Fibers. For the test fiber and before each use,
1.20 Alarms/Interlocks. Operate the device in a man- examine the aperture connector, cable, and
ner that will activate the self-check feature, if tip of each fiber to be used, as well as the fiber
present, and verify that all visual and audible support, for cleanliness and general physical
alarms activate according to the manufacturer’s condition. Be sure that all hardware (e.g.,
documentation. If no self-check feature is present, laser gas tubing channels) is present, in good
operate the laser in a manner that will activate condition, and firmly attached. Ensure that
each audible and visual alarm; be sure to test only the aperture connector properly seats into the
those alarms that will not cause damage to the laser aperture of the laser cabinet. Examine
laser or present an unnecessary risk of laser beam the distal end of fibers to ensure that any
exposure to yourself or bystanders. connecting mechanisms (e.g., threads) are in
If a door or window interlock is used, ensure proper working order.
that it properly deactivates the laser. (Do not If a fiber appears to be dirty or damaged,
disassemble major parts of the laser to test in- remove it from service. If a fiber is reusable,
ternal interlocks.) After deactivating the laser notify the person(s) responsible for fiber re-
and reclosing the door or window, check to be pair. The fiber should be repaired and/or
sure that the laser will restart. Be sure to check cleaned according to the manufacturer’s rec-
the interlocks in all locations where the laser is ommendations. Verify fiber performance.
used. (For some lasers, the function of the inter-
locks can be checked using an ohmmeter.) Contact tips. Examine each tip that may be used
with the laser fibers for cleanliness and gen-
If the laser is equipped with an emergency eral physical condition. Be sure that the
“kill” switch, test this feature to be sure that it mechanism to connect a tip to a fiber is in
deactivates the laser and that the laser will proper working order and forms a secure con-
subsequently restart. nection. If a tip appears to be dirty or dam-
aged, remove it from service and notify the
1.21 Audible Signals. Operate the device to activate person(s) responsible for tip repair or replace-
any audible signals (e.g., laser emission, setting ment. Some tips may look dirty after a single
change). Check for proper operation, and verify use, but remain acceptable for use; if you are
that the signal can be heard in the environment unsure about the need to clean or repair a tip,
in which the laser will be used. consult with the person(s) responsible for tip
1.22 Labeling. Check that all placards, labels, and repair or replacement and with the manufac-
instruction cards noted during acceptance testing turer, if necessary.
(see Item 4.3) are present and legible. Check to Handpieces. Examine each handpiece component
see that an instruction manual is kept with the (e.g., body, tips, lenses) for cleanliness and gen-
laser or is readily available. eral physical condition. Examine individually
only those components that are intended for
1.23 Accessories.
removal during normal use and storage. (Do
General. Verify that all necessary accessories not remove other parts that are press-fit or
are available and in good physical condition. attached by screws, bolts, or snap-rings.) If
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Nd:YAG Surgical Lasers
lenses are detachable, be sure not to touch the brightness of the aiming beam. Similarly, check
lens surface; handle lenses by the edges only. pulsing controls to verify that the aiming beam
Consult the manufacturer’s recommenda- can be pulsed. If several color choices are avail-
tions for the procedures and cleaning agents able for the aiming beam, verify that each color
to use to clean lenses. is present and working properly.
Ensure that major subcomponents of the 1.25 Laser Aperture.
handpiece, when assembled, are secure. En-
sure that the mechanisms used to connect the WARNING: Make this inspection with the la-
handpiece(s) to the fiber are in good working ser powered off. Remove and inspect the protec-
order and that they reliably secure each hand- tive window (e.g., blast shield) behind the laser
piece to the fiber. aperture. It should be clean and undamaged;
clean or replace if needed. There should be no
Microscope micromanipulator. Examine the mi-
visible dirt or residue in the optical path of the
croscope micromanipulator for cleanliness
laser aperture.
and general physical condition. Be sure to
handle it by the main body; do not hold it by 1.26 Gas Regulators. Examine any gas regulators for
the joystick, and do not touch the reflecting cleanliness and general physical condition. En-
lenses in the body. Inspect micromanipulators sure that the gauges on the regulators are not
provided by both the laser manufacturer and broken. During the procedure, ensure that the
the laser accessory manufacturer. regulator and the gauge operate as expected.
Ensure that the reflecting surfaces and Verify that the correct gas is attached to each
lenses are intact and clean. Consult the regulator. Be sure that a key or wrench to facili-
manufacturer’s recommendations for the pro- tate changing the gas supply is with the unit or
cedures and cleaning agents to use to clean readily available.
reflecting surfaces and lenses.
If the laser includes a gas recirculation system,
Examine the joystick to ensure that it is ensure proper operation by allowing it to control
firmly attached and that it freely moves the the gas supply into and out of a sealed plastic bag.
reflecting lens. If a finger rest is present, ensure
that it is firmly attached and properly oriented. WARNING: Do not use an anesthesia or other
similar bag that may have a mold-release agent
If a zoom focus feature is present, be sure (e.g., starch, talc) on its inside surface because the
that it turns easily and does not slip. Examine agent could contaminate the gas recirculation
each objective lens to ensure that it is intact system of the laser and ultimately contaminate a
and clean. Do not touch the lens surface. Con- patient wound during a subsequent procedure.
sult the manufacturer’s recommendations for
the procedures and cleaning agents to use to If proper operation is questionable, consider
clean the objective lenses. Carefully insert using a calibrated flowmeter to measure actual
each lens into the micromanipulator, and en- gas flow.
sure that it fits snugly.
Inspect the mechanism used to attach the 2. Quantitative tests
micromanipulator to the microscope to ensure WARNING: In general, do not use liquid fiber cooling
that all parts are present and that it is in good for tests unless specifically described in the item. Use of
working order. Connect the micromanipulator to this kind of cooling rather than gas fiber cooling may
the microscope to check for a secure connection. damage test equipment or cause erroneous test results.
Safety filters. Verify operation of safety filters in
microscope and endoscope delivery systems. 2.1 Grounding Resistance. Use an ohmmeter, elec-
trical safety analyzer, or multimeter with good
1.24 Aiming Beam. Activate the aiming beam (with- resolution of fractional ohms to measure and
out the therapeutic beam), and verify that it record the resistance between the grounding pin
produces a round, uniformly bright spot, with no on the power cord and exposed (unpainted and
halo. For handpieces that provide adjustable not anodized) metal on the chassis, accessory
spot sizes, verify that the spot size changes as outlet, ground pins, and footswitch. We recom-
expected and still remains uniform. Check that mend a maximum of 0.5 Ω. (If the footswitch is
the intensity control, if present, does change the of low voltage, grounding is not required.)
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
2.2 Leakage Current. Pulse feature operates as expected by moving the
target material slightly between each pulse. Be
WARNING: Do not reverse power conductors extremely careful to keep hands out of the laser
for this or any other test. Improper attachment beam path. If the number or duration between
of conductors may damage the laser. repeat pulses is adjustable, test that setting
changes made throughout the range result in the
With the laser attached to a grounded power-
expected performance.
distribution system, measure the leakage cur-
rent between the chassis and ground with the 2.5 Footswitch Exposure Control. Set the output
unit grounded and ungrounded. The leakage time for about 5 sec, activate the unit, and release
current on the chassis should not exceed 300 µA; the footswitch after about 1 sec. Verify that the
in no case should it exceed 500 µA. Where it is beam turns off when the footswitch is released.
greater than 300 µA, ensure that appropriate
grounding is present. 2.10 Power Output. Select one delivery system (e.g.,
fiber, handpiece, micromanipulator), and per-
2.3 Exposure Duration. Some laser power meters form the manufacturer’s recommended user cali-
can measure pulse duration. If the power meter bration procedure. Secure the delivery system at
can react to pulse duration (this is the preferred the distance from the laser power meter to meet
circumstance), test the laser at each setting. spot-size requirements specified in the instruc-
However, if the laser power meter does not meas- tions for the meter. (Do not focus the beam to a
ure pulse duration, use the following less prefer- small spot on the power meter. Some power
able alternative. meters require that the unfocused or a defocused
laser beam be projected into the power meter to
Place and secure the laser fiber, handpiece, or cover the majority of the absorber surface. If the
micromanipulator with the aiming system fo- laser beam is focused on the receiver of such
cused on the target material (e.g., black Delrin meters, the meter may be damaged.)
or a tongue depressor). With the laser set to
about 10 W and the exposure set at minimum WARNING: Accessing the unfocused laser
duration, activate the laser and create a burn. beam may require defeating internal interlocks.
Carefully move the target material to expose a Because of the heightened risk associated with an
clean area, maintaining the same distance. Ad- unfocused, nondiverging laser beam, exercise
just the exposure setting in increments of 0.1 sec great care if the interlocks are to be defeated.
or the next longest duration, and activate the
With the laser set at low (e.g., 10% of full scale),
laser at each setting. Continue this process until
medium (e.g., 50% of full scale), and maximum
you have tested all exposure settings, except
output, activate the laser for a sufficient period to
continuous, and have developed a series of
acquire acceptable readings. (Power meters use
burns. Compare the burns to verify that progres-
different time constants to acquire an acceptable
sively larger burns occurred as the exposure
reading, and you must know and meticulously
duration increased.
follow them.) Compare the reading with the power
2.4 Repeat Pulse. If the unit includes a Repeat Pulse display of the laser; the measured and displayed
feature, which repeats the pulse at a fixed or values should all be within 10% of one another. In
adjustable rate, test this feature with the laser addition, compare the reading obtained with the
set at the minimum, median, and maximum reading taken on incoming acceptance testing, at
Repeat Pulse settings, if adjustable. Some laser the last preventive maintenance procedure, or af-
power meters can react quickly enough to be ter the last service procedure. If the laser includes
used to test this feature of the laser. If you are a low-power (e.g., mW) feature, test it in a similar
using such a power meter, test the laser to be fashion with a power meter of appropriate resolu-
sure that the correct power is repeatedly deliv- tion in the low-power range.
ered over the correct time period.
3. Preventive maintenance
If your laser power meter cannot be used for Verify that all daily preventive maintenance proce-
this test, use this alternative test method. Set dures recommended by the manufacturer are carried out.
the laser to about 10 W and a 0.1 sec exposure
duration with the fiber, handpiece, or microma- 3.1 Clean the exterior. Clean cooling system fibers
nipulator attached, and verify that the Repeat and accessible optical components (e.g., blast
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Nd:YAG Surgical Lasers
shield, microscope lenses), if necessary, using 4.4 Electrical Wiring Configuration. Ensure that
techniques and cleaning solutions recommended the branch circuits and the outlets for the laser
by the manufacturer. are properly wired and rated for use with the
laser. Examine the receptacles at each location
3.2 Lubricate any motor, pump, fan, compressor, or where the laser is to be used to ensure that the
printer components as recommended by the
proper electrical configuration (e.g., proper neu-
manufacturer. tral and ground connections, proper phase rota-
3.3 Calibrate/adjust any components (e.g., printer) tion) has been installed. Connect the laser to
according to manufacturer recommendations. each receptacle and confirm that the laser oper-
Only appropriately trained personnel should at- ates properly, specifically confirming that mo-
tempt laser adjustments. Ensure that all hoses tors are operating in the proper direction.
and tubes are tight.
4.5 AC Plug. Verify that the plug is acceptable for
3.4 Replace filters if needed. Check all fluid levels use with the maximum current and voltage
and supplement or replace fluids if needed. specifications for operating the laser. (Consult
National Electrical Manufacturers Association
4. Acceptance tests [NEMA] configurations for general-purpose non-
Conduct major inspection tests for this procedure locking and locking connectors if in doubt.)
and the appropriate tests in the General Devices Pro- 4.6 Pulse Duration. Verify that progressive in-
cedure/Checklist 438. creases in pulse duration throughout its range of
WARNING: Lasers may be damaged by switching adjustment result in progressively larger burns.
between normal and reverse polarity while the device is 4.7 Repeat Pulse. If the unit includes a Repeat Pulse
on. If reverse-polarity leakage current measurements feature, test this feature as described in Item 2.4,
are made, turn off the unit being tested before switching but over the full range of available settings.
polarity. Also, lasers powered by three-phase electrical
systems may be damaged if proper electrical phase 4.8 Power Range. Using the technique described in
connections are not made initially and maintained Item 2.10, test the power output accuracy at
thereafter. Thus, do not switch conductor connections several low, medium, and high settings.
or wiring configurations for any tests, including leak-
age current measurement. Do not conduct electrical 4.9 Laser Delivery System Calibration. Use the manu-
leakage current tests with reversed-polarity wiring. facturer’s recommended calibration procedure to
test each new reusable delivery system (e.g., fiber,
Also test the ability of the laser to deliver laser handpiece) that the manufacturer indicates can be
energy as expected in all configurations and with all acceptably calibrated using these procedures.
provided laser accessories. In addition, perform the (Contact tips cannot be calibrated using the laser’s
following tests. calibration power meter.) Note the fiber transmis-
sion for each delivery system tested if this infor-
4.1 Areas of Use. Visit the area(s) in which the laser
mation is provided by the laser. Or, you can
is to be used and ensure that laser signs, eyewear,
calculate it using the following formula:
and window coverings are available and being
used and that safety interlocks for doors or win- Delivered power
% Transmission = × 100%
dows, if present, are functioning properly. Power entering the fiber
4.2 Casters/Mounts/Holders. Ensure that the as- Delivery systems with less than the manufac-
sembly is stable and that the unit will not tip over turer-recommended transmission (typically
when pushed or when a caster is jammed on an 80%) should be discarded if they are disposable,
obstacle (e.g., a line cord threshold), as may occur or repaired if they are reusable and intended for
during transport. If the device is designed to rest repair.
on a shelf, ensure that it has nonslip legs or
supports. Before returning to use
4.3 Labeling. Examine the unit and note the pres- Be sure to return controls to their starting position,
ence, location, and content of all labels. Labeling and place a Caution tag in a prominent position so that
information is typically found in the laser’s op- the next user will be careful to verify control settings,
erator manual. setup, and function before using the unit.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 9
Procedure/Checklist 444-0595
Oxygen-Air Proportioners
Used For:
Oxygen-Air Proportioners [12-876]
Also Called: Oxygen blenders, oxygen controllers, oxygen-air mixers
Commonly Used In: Critical care units, NICUs; occasionally used in operating rooms and most other patient
care areas
Scope: Applies to external oxygen-air proportioners; can be adapted for proportioners that are built into
ventilators
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview them to preset levels at or below inlet supply levels.
At these matched or preset pressures, air and oxygen
Oxygen-air proportioners are designed to mix com- enter a mixing valve that regulates their proportions
pressed air and oxygen to user-selectable oxygen con- as they flow out of the unit.
centrations varying from 21% to 100% at high- or
low-output flows. Their mixed-gas output is often When input pressures drop too low or differ greatly,
passed through a humidifier or a nebulizer and deliv- proportioners cannot deliver accurate concentrations.
ered to patients through ventilators, tracheostomy For this reason, proportioners have built-in reed
tubes, endotracheal tubes, oxygen tents, oxygen hoods, alarms that sound when there are large pressure dif-
or masks at flows ranging from 1 to more than 100 ferentials at the gas inlets or when there are low inlet
L/min. Oxygen-mixing devices are built into ventila- or outlet pressures.
tors or supplied as stand-alone units. This procedure
covers the stand-alone units but can be adapted for The most common problems related to these units
other units. involve the contamination of oxygen or air sources due
to backflow of the other gas and the delivery of inaccu-
Oxygen-air proportioners operate by receiving air rate oxygen concentrations. These problems are most
and oxygen from central gas pipelines in the hospital often caused by buildup of moisture or particulates
or from other compressed-gas sources, such as tanks inside the units from the compressed-gas lines. Along
or portable air compressors. Ideally, the two input gas with regular preventive maintenance schedules, hos-
sources are regulated at equal pressures (usually 50 pitals can maintain accuracy and reliability by install-
psi). However, because this is often not the case, ing water-trap filters at the gas inlets and using gas
proportioners have their own pressure-regulating filtration and drying systems at compressed-gas
mechanisms to match input supply pressures or adjust sources.
022999 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
444-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Citations from Health Devices
Oxygen-air proportioners [Evaluation], 1985 Jul;
14:263-76.
Using a double flowmeter assembly in lieu of an oxygen
blender [User Experience NetworkTM], 1985 Nov;
14:401.
Inaccurate O2 concentrations from oxygen-air propor-
tioners [User Experience NetworkTM], 1989 Oct;
18:366.
Test apparatus and supplies
Although this procedure can be performed using
only the common tools and materials listed below,
some manufacturers sell special service kits for their
units. This procedure, as well as service and repair,
may be facilitated by these kits; consult your service
manual to determine if a kit is available. See Figure 1
for a typical test setup.
High-flow flowmeters with a range of 0 to 100 L/min
(accurate to within 10% of reading)
Flowmeters with ranges of approximately 0 to
50 mL/min and 1 to 15 L/min with 10% accuracy
Hoses and adapters for connecting pressure gauges
and flowmeters to equipment being inspected
Cylinders of oxygen and air with pressure gauges
that can be regulated between 0 and 100 psi; cylin-
der pressures should be at least 1,000 psi
Nondisposable corrugated breathing hose (dispos-
able tubing may be used only if it provides reliable
connections) Figure 1. Typical test setup
Oxygen analyzer with at least ±3% accuracy and
with a “T” adapter for sensor head the equipment, the significance of each control and
Flow-control valve indicator, and the alarm capabilities. Also, determine
if any special inspection or preventive maintenance
Teflon tape
procedures are recommended by the manufacturer.
Cleaning solvent recommended by the manufac-
turer
1. Qualitative tests
Lubricant specified by the manufacturer
Special precautions 1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condi-
All testing should be done with pressure gauges and tion. Be sure that plastic housings are intact,
flowmeters specified for oxygen or medical gas use that all connectors are present and tight, and
only. Turn off all pressurized gas sources when they that there are no signs of spilled liquids or other
are no longer in use. serious abuse.
Procedure 1.2 Mount/Fasteners. If the device is mounted on a
Before beginning an inspection, carefully read this stand or cart, examine the condition of the
procedure and the manufacturer’s instruction and serv- mount. If it is attached to a wall or rests on a
ice manuals; be sure that you understand how to operate shelf, check the security of this attachment.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Oxygen-Air Proportioners
1.8 Tubes/Hoses. Check the condition of all tubing 2. Quantitative tests
and hoses. Be sure that they are not cracked,
kinked, or dirty and that they do not leak. 2.3 Maximum Flow Rate. Using a high-flow flow-
meter, measure the maximum flow rate out of
1.10 Fittings/Connectors. Examine the condition of all the proportioner. If the proportioner has two
gas fittings. They should be tight and should not outlets, measure the flow from its high-flow out-
leak. If keyed connectors (e.g., DISS gas connectors) let. Unless designed specifically to deliver low
are used, make sure that the keying is correct. flows (e.g., below 15 L/min), the proportioner
should be able to deliver at least 80 L/min from
1.12 Filters. Clean or replace inlet gas filters where its high-flow outlet when the concentration is set
appropriate, and indicate this on Lines 3.1 and at 60%. Also, measure the maximum flow rate
3.4 of the form. Replace filters if their time of use when the concentration is set to 21% and 100%.
has exceeded the manufacturer’s recommended The flows at these concentration settings should
interval or if the proportioner’s performance in- not differ by more than 10 L/min. Flow differ-
dicates that they need to be changed (see Item ences greater than 10 L/min indicate a restric-
2.3). Use Teflon tape to ensure sealing when tion at one of the inlets and probably the need to
replacing any pipe-thread fittings that were re- replace an inlet filter.
moved for filter replacements.
2.4 Alarms. Adjust input pressures to the propor-
1.13 Controls/Switches. If the proportioner has ad- tioner’s specified alarm conditions. Verify that
justments for anything other than O2 concentra- the alarms can be heard clearly and that the unit
tion (e.g., alarm limits, output pressure), check delivers accurate concentrations before the
their positions. If they appear to be set to un- alarm sounds.
usual values, consider the possibility of inappro-
priate clinical use. Record the settings of those 2.5 Flow with Loss of an Input Source. Turn off one
controls that should be returned to their original of the input supplies and verify that the unit
positions following the inspection. continues to alarm and deliver adequate flows
at all concentration settings. With the loss of an
Examine all controls and switches for physical input source, the proportioner should be able to
condition, secure mounting, and correct motion. deliver at least 30 L/min from its high-flow
Check that control knobs have not slipped on their output and 15 L/min from its low-flow output.
shafts. Where a control should operate against Note that not all proportioners have the same
fixed-limit stops, check for proper alignment as alarm conditions; check the manufacturer
well as positive stopping. During the course of the alarm specifications.
inspection, be sure to check that each control and
switch performs its proper function. 2.6 Check-Valve Leakage. Apply 5 psi to one input
source and attach a flowmeter to the second
1.18 Indicators/Displays. During the course of the source. With the output disconnected, no more
inspection, confirm the operation of all gauges than 0.1 L/min should leak from the second input
and visual displays on the unit. source. Repeat this procedure with the other
input source.
1.22 Labeling. Check that all necessary placards and
labels are present and legible. 2.10 Accuracy. Adjust input pressures to 50 psi; us-
ing an oxygen analyzer, measure the concentra-
1.23 Accessories. Confirm the presence and condition tion from the proportioner output at settings of
of accessories, including high-pressure hoses, 21%, 60%, and 100% with the flowmeters ad-
flowmeters, and water-trap filters. High-pres- justed to deliver flows over the range that would
sure hoses should be supplied with the appropri- typically be used (e.g., 5 and 30 L/min). Accuracy
ate oxygen and air DISS fittings to match their should be within 3%.
outlet fittings. Water-trap filters should be
clean and drained of all fluid. 3. Preventive maintenance
1.24 Low-Flow Bleeds. Some proportioners have low- 3.1 Clean the exterior and interior, if needed.
flow continuous bleeds to the atmosphere to im- 3.2 Lubricate per the manufacturer’s instructions.
prove accuracy. Inspect the proportioners to Never use lubricants that will react with oxygen.
ensure that the bleed outputs are not blocked or
clogged by tape or dirt. 3.3 Calibrate per the manufacturer’s instructions.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
3.4 Replace tubing, hoses, dirty filters, and damaged Before returning to use
components if needed.
Depressurize all external gas supplies and make sure
that alarms and controls are set to appropriate levels.
4. Acceptance tests Where appropriate, attach a Caution tag in a promi-
nent position to alert users that alarm or control set-
Conduct major inspection tests for this procedure. tings may have been changed.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 417-0595
Oxygen Analyzers
Used For:
Oxygen Analyzers [12-858]
Oxygen Monitors [12-863]
Also Called: Oxygen monitors
Commonly Used In: Operating rooms and critical care units
Scope: Applies to oxygen analyzers/monitors intended to monitor the level of oxygen being delivered to a
patient, which may be measured at or near the airway (e.g., endotracheal tube) or in the oxygen delivery device
(e.g., oxygen hood); also applies to devices used to calibrate or verify the oxygen concentration in certain
medical gases, and to devices used to calibrate and verify performance of oxygen-mixing devices (see
Oxygen-Air Proportioners Procedure/Checklist 444)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview essential to collect and store data on the concentration
of inspired oxygen and the total time duration at each
For several years, ECRI has recommended that all level. An oxygen analyzer should also be used regu-
anesthesia patient circuits incorporate oxygen concen- larly to check the accuracy of ventilator settings.
tration analyzers/monitors (hereafter referred to sim-
ply as oxygen analyzers) with alarms. We consider Most oxygen analyzers for breathing circuits oper-
this essential to protect patients from hypoxia, since ate on electrochemical principles and use po-
the analyzer senses the oxygen concentration in the larographic electrodes or galvanic cells. Some
inspiratory line of the patient circuit rather than at the paramagnetic oxygen analyzers are also used. Oxygen
oxygen flowmeter or common gas outlet of the anesthe- analyzers can accurately measure oxygen concentra-
sia unit where oxygen concentration may be higher tions, as demonstrated in our evaluations of the de-
than in the patient circuit. Use of a properly function- vices. However, anesthesiology departments need to
ing oxygen analyzer in conjunction with the anesthe- realize that the instruments require more care and
siologist’s educated hand (on the reservoir bag) and ear maintenance than the anesthesia machines on which
(listening to breath sounds) greatly increases the like- they are used. The devices are too often found with
lihood that an adequately oxygenated mixture will be their batteries or sensors depleted. Daily checks by
directed into the patient’s lungs. the user are essential to ensure accuracy and response.
Continuous monitoring of oxygen concentration The reliability of oxygen sensors can also be affected
may also be required in applications of critical care by other factors. Nitrous oxide can be reduced by a
ventilators or other oxygen administration equipment. polarographic electrode, but at a higher voltage than
For example, when ventilating some infants, it is often that required by oxygen. In the past, some analyzers
010106 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
417-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
exhibited a sensitivity to nitrous oxide immediately 1.4 AC Plug. Examine the AC power plug for dam-
before battery depletion. (The voltage of mercury bat- age. Attempt to wiggle the blades to determine
teries peaks just before depletion and is then high that they are secure. Shake the plug and listen
enough to cause the reaction to proceed with nitrous for rattles that could indicate loose screws. If
oxide at the electrode.) Such interference resulted in any damage is suspected, open the plug and
indications of a higher-than-actual oxygen concentra- inspect it.
tion, but was corrected by limiting cell voltage to a
value where nitrous oxide interference was insignifi- 1.5 Line Cord. Inspect the cord for signs of damage.
cant. Early galvanic cells were also structurally dis- If damaged, replace the entire cord or, if the
torted by nitrous oxide and lost calibration. Newer damage is near one end, cut out the defective
galvanic cell designs resist this distortion and can be portion. Be sure to wire a new power cord or plug
used with anesthetic gas mixtures. with the same polarity as the old one. Also check
line cords of battery chargers.
Halothane can also be reduced by polarographic
electrodes and, if permitted to enter the cell, may 1.6 Strain Reliefs. Examine the strain reliefs at
generate significant error signals that increase over both ends of the line cord. Be sure that they hold
the duration of anesthesia administration. the cord securely.
1.7 Fuse. If the device is protected by an external
Citation from Health Devices fuse, check its value and type against that
Oxygen analyzers for breathing circuits [Evaluation], marked on the chassis and ensure that a spare
1983 Jun; 12:183-97. fuse is provided.
Test apparatus and supplies 1.9 Cables. Inspect the cables (e.g., sensor) and
Ground resistance ohmmeter (for line-operated their strain reliefs for general condition. Exam-
units only) ine carefully to detect breaks in the insulation
and to ensure that they are gripped securely in
Leakage current meter (for line-operated units only)
the connectors of each end to prevent rotation or
Oxygen source capable of providing about 4 L/min other strain.
flow
1.10 Fittings/Connectors. Examine all gas fittings
Gas manifold or T adapter
and connectors, as well as all electrical cable
Stopwatch or watch with a second hand connectors, for general condition. Electrical con-
tact pins or surfaces should be straight, clean,
Special precautions and bright. Confirm that the transducer fits
Do not touch or puncture the membrane surface. tightly into the manifold fittings.
Procedure 1.11 Electrodes/Transducers. Examine the sensor
for salt accumulation that might indicate elec-
Before beginning the inspection, carefully read this trode leakage. Check the condition and place-
procedure and the manufacturer’s instruction and serv- ment of O-rings. Check electrolyte level of
ice manuals; be sure you understand how to operate the polarographic electrodes; replenish it if needed
equipment, the significance of each control and indicator, and note this on Line 3.4 of the inspection form.
and the alarm capabilities. Also determine whether any
special inspection or preventive maintenance procedures 1.13 Controls/Switches. Before changing any con-
are recommended by the manufacturer. trols and alarm limits, check their positions. If
any of them appear inordinate (e.g., a calibration
1. Qualitative tests control at maximum, alarm limits at the ends of
1.1 Chassis/Housing. Examine the exterior of the their range), consider the possibility of inappro-
unit for cleanliness and general physical condi- priate clinical use or of incipient device failure.
tion. Be sure that plastic housings are intact, Record the settings of those controls that should
that all assembly hardware is present and tight, be returned to their original positions following
and that there are no signs of spilled liquids or the inspection.
other serious abuse.
Examine all controls and switches for physical
1.2 Mount/Fasteners. Check the security of the condition, secure mounting, and correct motion.
mounting mechanism. Where a control should operate against fixed-limit
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Oxygen Analyzers
stops, check for proper alignment, as well as 2. Quantitative tests
positive stopping. Check membrane switches for
membrane damage (e.g., from fingernails, pens). 2.1 Grounding Resistance. Using an ohmmeter,
During the course of the inspection, be sure to electrical safety analyzer, or multimeter with
check that each control and switch performs its good resolution of fractional ohms, measure and
proper function. record the resistance between the grounding pin
of the power cord and exposed (unpainted and
1.17 Battery/Charger. Inspect the physical condition not anodized) metal on the chassis. We recom-
of all batteries and battery connectors. Check mend a maximum of 0.5 Ω.
operation of battery-operated power-loss alarms,
if so equipped. Operate the unit on battery power 2.2 Leakage Current. Measure chassis leakage cur-
for several minutes to check that the battery is rent to ground with the grounding conductor of
charged and can hold a charge. Check remaining plug-connected equipment temporarily opened.
battery capacity by activating the battery test Operate the device in all normal modes, includ-
function or measuring the output voltage. Check ing on, standby, and off, and record the maxi-
the condition of the battery charger if so equipped mum leakage current. Leakage current should
and, to the extent possible, confirm that it does, not exceed 300 µA.
in fact, charge the battery. When it is necessary
2.3 Accuracy. The analyzer should indicate the oxy-
to replace a battery, label it with the date.
gen level in a dry gas mixture in the circuit to
1.18 Indicators/Displays. During the course of the within 3% oxygen. Check the accuracy at 21%
inspection, confirm the operation of all lights, (room air) or 100% oxygen concentration, which-
indicators, meters, and visual displays on the ever was not used in adjusting the unit’s calibra-
unit. Be sure that all segments of a digital tion (in Item 1.19). Use the gas manifold if 100%
display function. oxygen is needed.
1.19 User Calibration. Confirm that the calibration 2.4 Response Time. Analyzers should rapidly indi-
function operates. Calibrate the unit before pro- cate changes in oxygen concentration. The re-
ceeding to the quantitative tests. If it cannot be sponse time, including alarm delay, should be
adjusted according to manufacturers’ instruc- within the manufacturer-specified time, but
tions, it may need sensor replacement or renewal with a time constant (time for 63% of a change)
or battery replacement or recharging. Replace of less than 20 sec.
as needed and note this on Line 3.4 of the form.
An excessively long time constant usually in-
1.20 Alarms. Operate the unit in such a way as to dicates that the sensor needs replacement or
activate each audible and visual alarm. Where renewal.
the device has an alarm-silence feature, check
the method of reset (e.g., manual or automatic) With low alarms set at 50% oxygen, circulate
against the manufacturer’s specifications. An 100% oxygen until the reading stabilizes, then
oxygen analyzer for continuous monitoring terminate oxygen flow, remove the sensor, and
should have a low alarm that cannot be set below expose it to room air. (The 50% alarm setting
18% oxygen. If the device has a lower alarm represents approximately 63% of the change
limit, alert the user to this condition and con- from 100% to 21% oxygen.) Measure the time to
sider replacing the unit. indicate the change to 50% and alarm with a
stopwatch or watch with a second hand and
1.21 Audible Signals. Operate the device to activate record this value.
any audible signals. Confirm appropriate vol-
ume, as well as the operation of a volume control. 2.10 Alarms. Alarms should activate when the indi-
cated oxygen level is within 2% oxygen of the set
1.22 Labeling. Check that all necessary labels are alarm value for the range 15% to 40% oxygen,
present and legible. which is most critical for patient safety, and
within 5% oxygen for the range 40% to 100%
1.23 Accessories. Verify that replacement sensors, oxygen.
membranes, batteries, and electrolyte solution
or gel are available. Confirm that the expiration Vary the indicated oxygen concentration (by
date is current and that all packages are prop- varying the calibration adjustment) above or below
erly sealed. the alarm settings of 21% (low-alarm setting) and
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
50% (high-alarm setting) oxygen and record 4. Acceptance tests
whether the alarm points are within the re-
quired limits. If the unit’s design does not allow Conduct major inspection tests for this procedure
the above method to be used, then check the low and the appropriate tests in the General Devices Pro-
alarm by increasing the alarm setting from 21% cedure/Checklist 438.
(with the sensor exposed to room air) until the
alarm is activated. Test the high alarm simi-
Before returning to use
larly, but expose the sensor to 100% oxygen in If there are indications of improper daily mainte-
the manifold and decrease the alarm setting nance, misuse, or nonuse (e.g., deteriorated sensor,
from 100%. depleted battery, low alarm set below 20%), alert ap-
propriate clinical personnel (users and/or chief of an-
3. Preventive maintenance esthesiology). Stress the importance of daily
maintenance and monitoring oxygen concentrations
3.1 Clean the exterior. whenever inhalation anesthesia is administered. Pa-
3.3 Calibrate if required. tient deaths have occurred that could have been
averted if a properly operating oxygen analyzer had
3.4 Replace the battery and sensor, if needed. been used.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 418-0595
Pacemakers, External Invasive
Used For:
Pacemakers, Cardiac, External Invasive [12-912]
Also Called: Temporary pacemakers, transvenous pacemakers
Commonly Used In: Critical care units, emergency rooms, operating rooms, electrophysiology labs
Scope: Primarily applies to single- and dual-chamber external (transvenous) pacemakers used for temporary
demand or asynchronous pacing; does not apply to noninvasive (transcutaneous) pacemakers (see Pacemakers,
External Noninvasive Procedure/Checklist 460)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview battery-powered external pulse generator. An epicardial
lead can also be placed during open-heart surgery.
The heart has its own pacemaker — a group of special-
ized cells that produces a rhythmic train of electrical In the asynchronous, or fixed-rate, pacing mode, the
pulses. These pulses are carried by specialized con- pacemaker emits a stimulus at regular intervals, re-
ducting cells to cardiac muscle cells in the atria and gardless of cardiac activity. Asynchronous pacing is
ventricles, stimulating them to contract at the proper often used when a pacemaker is initially connected, or
times. In some patients, the intrinsic pacemaker or is used periodically to confirm that the signal ampli-
the conduction network fails. Unless the heart muscle tude is adequate to capture, or pace, the heart. The
is stimulated by some other means, the heart may beat asynchronous mode is also used for continuous pacing
erratically or stop. when the heart is unlikely to spontaneously revert to
a normal sinus rhythm during pacing.
A pacemaker is used to control these arrhythmias
(irregular heart rhythms) by applying a repetitive elec- If an asynchronous pacemaker is used, and the
trical stimulus to the heart. Temporary external pacing heart reverts to its own rhythm, competition may occur
is used to control the heart until it reverts (or is reverted between the pacemaker stimuli and the natural car-
through other therapy) to a satisfactory rhythm or until diac signals. This may cause ventricular fibrillation or
a permanent pacemaker can be implanted. Temporary a decrease in cardiac output. To avoid this possibility,
pacing is also used when patients with a history of certain the demand, or ventricular inhibited, mode of opera-
cardiac disturbances must undergo major surgery. tion can be used. In this mode, the pacemaker cir-
cuitry senses the heart’s intrinsic electrical signal and
The most common method of temporary pacing is attempts to pace the heart only if the intrinsic signal
through an electrical lead, or catheter, positioned in the is too infrequent or absent.
heart. The lead, which is usually inserted in a vein in
the arm or neck, has a metal tip and a metal ring that Although most temporary pacing is performed
act as electrodes to deliver a stimulus produced by a with demand or asynchronous ventricular pacing,
009018 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
418-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
dual-chamber pacemakers are also available for atrial- indicate a deficiency, they may not justify removing
ventricular (A-V) sequential pacing. In addition, some the pacemaker from use unless a replacement unit is
pacemakers are capable of fast-rate pacing for overrid- readily available. (For example, if the rate is inaccu-
ing certain cardiac rhythms. rate but still covers the necessary range, notify the
clinical staff of the problem, suggest that another unit
Citations from Health Devices be used if possible, and contact the manufacturer to
External pacemakers [Evaluation], 1974 Feb; 3:75-90. arrange for repair or replacement. However, if the
unit cannot be inhibited in the ventricular inhibited
External pacemakers [Evaluation], 1974 Aug-Sep; mode, immediately remove it from use.)
3:268-74.
Undetected pacemaker spike signals in IABP patients Procedure
[Hazard], 1989 Dec; 18:441. Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and
Test apparatus and supplies service manuals; be sure that you understand how to
A variable amplitude and rate ECG simulator with operate the equipment and the significance of each
at least several millivolts QRS output amplitude control and indicator, as well as the alarm capabilities.
and range of rates to 75 pulses per minute Also determine whether any special inspection or pre-
ventive maintenance procedures or frequencies are
500 Ω resistor recommended by the manufacturer.
Connector or connector pins to attach leads to pace-
maker 1. Qualitative tests
Oscilloscope (to be used to determine the rate accu- 1.1 Chassis/Housing. Examine the exterior of the
racy of the pacemaker and thus requiring an accu- unit for cleanliness and general physical condi-
rate sweep speed verified by periodic calibration; an tion. Be sure that plastic housings are intact,
ECG monitor or electrograph should not be used to that all assembly hardware is present and tight,
determine the output amplitude of a pacemaker, and that there are no signs of spilled liquids or
since the limited frequency response of these instru- other serious abuse.
ments may distort the waveform and result in erro-
1.9 Cables. Extension leads (cables) are sometimes
neous amplitude readings)
used to allow more remote placement of the pace-
Pacing system analyzer (optional) maker (e.g., during a surgical procedure). A cable
Note: A pacing system analyzer, used to test may be kept with the pacemaker, or all extension
pacemakers and leads during an implantation pro- cables may be kept in one central location.
cedure, has features that greatly facilitate inspec-
Inspect the cables and their strain reliefs for
tion of external (invasive) pacemakers. It may be
general condition. Examine cables carefully to
possible to borrow a pacing system analyzer from
detect breaks in the insulation and to ensure
the cardiology or surgery department for this in-
that they are gripped securely in the connectors
spection. Of course, a unit must always be available
of each end to prevent rotation or other strain.
for their use. As an alternative, a pacing system
The cable connectors should provide an insu-
analyzer may be purchased (see Health Devices
lated connection. Replace older, noninsulated
1993 May-Jun; 22:260). Pacemaker device analyz-
connectors, and avoid using alligator clip connec-
ers (for external pacemakers only) will perform
tors.
many of the qualitative tests and some of the quan-
titative tests in this procedure and may be useful for If cables are sterile, ensure that they are in-
quick confirmation of a pacemaker’s performance. spected with each use and have them resteril-
Although they may not directly perform all of the ized.
recommended tests, they may be equipped with an
oscilloscope output to facilitate these tests. 1.10 Terminals. Inspect the output terminal insula-
tion for cracks or signs of deterioration.
Special precautions 1.13 Controls/Switches. Before moving any controls
Before performing an inspection, notify clinical staff and alarm limits, check their positions. If any of
if the pacemaker will be removed from its normal them appear inordinate (e.g., a maximum rate
storage area or if the unit will be out of service for even setting), consider the possibility of inappropriate
a few minutes. While the results of a specific test may clinical use or of incipient device failure. Record
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Pacemakers, External Invasive
the settings of those controls that should be simulator to the pacemaker output terminal,
returned to their original positions following the adjust the ECG rate higher than the pacing rate,
inspection. observe the sensing indicator, and note the ces-
sation of the pacing indicator.
Examine all controls and switches for physical
condition, secure mounting, and correct motion. 1.22 Labeling. Check that all necessary placards, la-
Where a control should operate against fixed- bels, and instruction cards are present and leg-
limit stops, check for proper alignment, as well ible.
as positive stopping. During the course of the
inspection, be sure to check that each control and 1.23 Accessories. Verify that limb straps, a spare bat-
switch performs its proper function. tery, and a screwdriver (if one is needed to replace
the battery) are readily accessible for each unit.
1.17 Battery. Inspect the physical condition of batter- A sterile catheter and an extension cable may
ies and battery connectors. Open the battery also be kept with each unit. Insulating caps to
compartment and examine it for signs of corro- cover the lead connectors when the pacemaker is
sion. If corrosion residues are apparent, or if disconnected should also be included. Check that
there is evidence of spilled liquid in the battery straps are clean and untangled. Do not store
compartment, clean the compartment and re- spare batteries in areas with high temperatures
place the battery. or where the terminals could be shorted.
Discuss appropriate battery replacement in- 1.24 Battery Test Feature. Check the battery condi-
tervals and procedures with users. If the battery tion with the battery test feature of the unit.
has been in use for the maximum recommended This may be either a meter reading obtained by
time, or if it is time for routine replacement, pushing a button or an observation that the
install an appropriate new battery. Label it with pacing indicator is functioning when the unit is
the date, if appropriate. Most manufacturers turned on. Check the unit’s instruction manual
recommend alkaline, mercury, or lithium batter- for details.
ies, although some manufacturers state a pref-
erence. 2. Quantitative tests
Battery connectors should be clean and shiny. If a dual-chamber pacemaker is being tested, record
If they are dirty, clean them with a paper towel appropriate quantitative results for both pacemaker
or a rubber pencil eraser, and wipe them after- channels.
ward with a clean, soft cloth. Do not use emery
cloth, steel wool, or liquids to clean the contacts 2.3 Pulse Width. Use the test setup shown in Figure
because this may leave conductive residues that 1, or connect the pacemaker to a pacemaker
could interfere with pacemaker function. Check analyzer to determine the pacemaker output
that battery connectors securely grip the battery pulse width. Set the pacemaker to approxi-
and correct, if necessary. mately 5 mA (2.5 V) at 60 bpm. The oscilloscope
sweep speed should be about 0.2 msec per divi-
1.18 Indicators/Displays. Verify that all indicators sion, and the trace should be set to trigger at the
and markings are easy to read. The pacing indi- beginning of the pacemaker pulse so that the
cator should indicate pacing pulses when the waveform covers most of the oscilloscope’s view-
pacemaker is turned on. Verify that the pacing ing area. Use consistent start and end points
indicator rate varies as the pacing rate control is (i.e., manufacturer’s specifications or 90% ampli-
adjusted. tude points) when measuring pulse width. Typi-
cal pulse widths are 0.5 to 2.0 msec.
If the indicator is designed to show only pulse
currents delivered to the heart, provide a com- If pulse widths are user adjustable, select
plete current path by either connecting the pace- maximum and minimum settings and verify
maker to the 500 Ω load or short-circuiting the that they are within 10% of the manufacturer’s
output terminals of the pacemaker. If a shorted specifications.
lead is used, remove it following the test.
2.4 Atrial-Ventricular Delay. For dual-chamber
To verify that the QRS sensing indicator func- units with A-V delay, check the delay. Use the
tions, set the pacemaker to its maximum sensi- test setup shown in Figure 1 with the atrial and
tivity (lowest setting). Connect an ECG ventricular outputs connected together, or use a
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
pacing system analyzer with this capability. Us- Rate accuracy within 5% is considered to be
ing the same output settings as in Item 2.3, satisfactory.
measure and record the time delay between the
start of the atrial pulse output and the start of 2.11 Amplitude Accuracy. Using the test setup
the ventricular pulse output. If the delay is ad- shown in Figure 1, set the pacemaker rate to
justable, confirm that minimum and maximum about 60 bpm and the output amplitude to 1 mA
are within specification (±10%); record this addi- (0.5 V on those units calibrated in volts). Verify
tional result as Item 2.5 on the inspection form. that pulses are of the correct polarity. Calculate
the average amplitude as indicated in Figure 2.
2.6 Record either voltage or current amplitude. Re-
Direct Current Leakage. Connect a 500 Ω load peat this test with the pacemaker set to 5 mA
across the output terminals of the pacemaker as (2.5 V) and 10 mA (5 V) or maximum. Amplitude
shown in Figure 1. With the pacemaker turned off, accuracies should be within 10%.
measure the DC voltage with a voltmeter across
the 500 Ω load; it should not exceed 5 mV. Turn 2.12 Sensing Sensitivity. This test will determine the
the pacemaker on and, using an oscilloscope, pacemaker sensitivity to an externally applied
measure the voltage across the 500 Ω load during pulse. The external ECG test signal is not equiva-
the nonpaced activity period just before the output lent to the intracardiac electrical signal that
pulse. Again, it should not exceed 5 mV. These would appear on the pacemaker catheter; there-
tests should be repeated for both the atrial and fore, pacemaker response may not be identical to
ventricular channels in dual-chamber pacemak-
ers.
Additionally, for dual-chamber units, connect
two 500 Ω loads between the positive and negative
output and connect a third 500 Ω load between the
A+ and V+ terminals. Set the pacing mode to DDD,
and measure the voltage across this third resistor
during the nonpaced activity period using an oscil-
loscope; it should not exceed 5 mV.
2.10 Rate Accuracy. Use the pacemaker analyzer or
test setup shown in Figure 1. Set the pacemaker
output to approximately 5 mA (2.5 V) in the
asynchronous mode. Most pacemakers should
be checked at rates of 60 and 120 bpm (corre-
sponding to periods of 1.0 and 0.5 sec), although
special-purpose high-rate units should be
checked at higher rates. Measure and record
either the actual rate or period of the pacemaker.
To determine the rate, divide 60 by the period
(i.e., 60/period [sec]).
Figure 1. Pacemaker pulse width, rate, and amplitude setup. Figure 2. Pulse amplitude calculation.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Pacemakers, External Invasive
that obtained during actual use. A 40 or 20 msec
sine-squared pulse is often used (in pacing sys-
tem analyzers) to provide a standard signal for
comparison among units or between results of
tests at two different times; however, a variable-
amplitude ECG simulator is also adequate for
inspection purposes. Because ECG waveforms
may differ among simulators, note the model of
the simulator used, and use the same model
simulator when testing this and other pacemak-
ers in the future.
With the pacemaker in the ventricular inhib-
ited mode and at maximum sensitivity, connect Figure 3. Pacemaker sensitivity test setup.
the ECG simulator output to the pacemaker, and
monitor the signal on the oscilloscope (see Figure
pulse. It may be necessary to turn the pace-
3). Allow the oscilloscope sweep to free-run (auto-
maker off to accurately measure the pulse am-
matic trigger) at 1 sec per division. The pace-
plitude.
maker should be set at approximately 60 bpm
and 5 mA output. The ECG simulator should be 3. Preventive maintenance
set for a 75 bpm rate. Slowly increase the simu-
lator output from zero until the pacemaker is 3.1 Clean the exterior.
completely inhibited (pacemaker output is not 3.4 Replace the battery, if necessary.
observed on the oscilloscope or pacemaker out-
put indicator). From the oscilloscope display, 4. Acceptance tests
measure and record the QRS peak amplitude by
the scope at the pacemaker terminals. Repeat Conduct major inspection tests for this procedure.
the test at a midrange sensitivity to ensure that If a pacing system analyzer with appropriate test
the sensing control is functioning. functions is available, test the following feature.
Pacemaker sensitivity should meet the manu- 4.1 Refractory Period. Follow the analyzer manu-
facturer’s specifications. At maximum sensitiv- facturer’s instructions for performing this test.
ity, most units will begin to sense at 1 to 2 mV.
Some units have sensitivity knobs graduated in Before returning to use
millivolts; these are usually only approximate Ensure that all controls are set properly in their
because of the poor resolution provided. normal pre-use positions. Attach a Caution tag in a
prominent position on life-support equipment or any
To test units with a ventricular synchronous other device for which the user must be aware that
mode of operation, instead of looking for the pace- control settings may have been changed.
maker pulse to disappear, look for the pacemaker
pulse to coincide with each pulse generator pulse, Either recharge the battery, or equip the device with
and record the amplitude of the pulse generator fully charged batteries.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 460-0595
Pacemakers, External Noninvasive
Used For:
Defibrillator/Monitor/Pacemakers [17-882]
Pacemakers, Cardiac, External Noninvasive [16-516]
Also Called: Noninvasive pacemakers, temporary pacemakers, transcutaneous pacemakers, transthoracic
pacemakers
Commonly Used In: Critical care units, emergency rooms, operating rooms, ambulances
Scope: Applies to pacemakers used for temporary pacing through adhesive electrodes applied to the skin;
includes pacemakers that are integral to a defibrillator/monitor; does not apply to implanted, transesophageal,
or transvenous pacemakers. (See Procedure/Checklist 418 for Pacemakers, External Invasive.)
This procedure is intended to be used in conjunction with the procedures for ECG monitors and defibrilla-
tor/monitors. For noninvasive pacemakers with an integral monitor, see ECG Monitors Procedure/Checklist
409. For noninvasive pacemakers that are integral to a defibrillator/monitor, see Defibrillator/Monitors
Procedure/Checklist 408.
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview implanted. Temporary pacing is also used when
patients with a history of certain cardiac disorders
The heart has its own pacemaker — a group of special- must undergo major surgery. In addition, it can be
ized cells that produce a rhythmic train of electrical used to induce cardiac stress during diagnosis of car-
pulses. These pulses are carried by specialized con- diac ailments.
ducting cells to cardiac muscle cells in the atria and
ventricles, stimulating them to contract in a coordi-
Noninvasive pacemakers conduct pacing current
nated pumping action. In some patients, the intrinsic
through the patient’s thorax using a pair of adhesive
pacemaker or the conduction network fails. Under
electrodes placed on the chest or on the chest and back.
these circumstances, unless the heart muscle is stimu-
These are connected to the pacemaker with a cable.
lated by some other means, the heart may beat errati-
Most noninvasive pacemakers are integrated into a
cally, slow down, or stop.
defibrillator/monitor.
A pacemaker is used to control these arrhythmias
(irregular heart rhythms) by applying a repetitive In the fixed-rate pacing mode, the pacemaker emits
electrical stimulus to the heart. Temporary external a stimulus at regular intervals, regardless of cardiac
pacing is used to control the heart until it reverts (or activity. Fixed-rate pacing is sometimes used when a
is reverted through other therapy) to a satisfactory pacemaker is initially set up to confirm that the signal
rhythm or until a permanent pacemaker can be amplitude is adequate to capture, or pace, the heart.
249434 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
460-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
If fixed-rate pacing is used and the heart reverts to defibrillator/monitor/pacemaker units. While the re-
its own rhythm, competition may occur between the sults of a specific test may indicate a deficiency, they
pacemaker stimuli and the natural cardiac signals. may not justify removing the pacemaker from use
This may cause ventricular fibrillation or a decrease in unless a replacement unit is readily available. For
cardiac output. To minimize this possibility, the de- example, if the rate is inaccurate but still covers the
mand, or ventricular-inhibited, mode of operation is necessary range, notify the clinical staff of the prob-
usually used. In this mode, the pacemaker circuitry lem, suggest that another unit be used if possible, and
senses the heart’s intrinsic electrical signal and at- arrange for repair or replacement. However, if the unit
tempts to pace the heart only if the intrinsic signal is cannot be inhibited in the demand mode, immediately
too infrequent or absent. When the heart rate is above remove it from use.
the set pacing rate, pacemaker output is inhibited.
Caution should be used when the unit is delivering
Citations from Health Devices output. Noninvasive pacemakers can typically gener-
ate impulses of up to 300 V.
Pace*Aid Model 50C external transcutaneous pace-
maker [Evaluation], 1983 Nov; 13:3-13. Do not monitor through multifunction electrodes
during demand-mode and sensitivity tests. Monitoring
Transcutaneous pacemakers [Guidance article], 1988 through the output electrodes is not possible during
Feb; 17:39-47. pacing because the impulses will saturate the monitor.
Defibrillator/monitors and external noninvasive pace-
makers [Evaluation], 1993 May-Jun; 22:213-94. Procedure
Noninvasive pacemaker testers, 1993 May-Jun; Before beginning an inspection, carefully read this
22:260-1. procedure and the manufacturer’s instruction and
service manuals; be sure that you understand how to
Test apparatus and supplies operate the equipment, the significance of each control
and indicator, and the alarm capabilities. Determine
Ground resistance ohmmeter whether any special IPM procedures or frequencies are
Leakage current meter or electrical safety analyzer recommended by the manufacturer. Many units have
Noninvasive pacemaker tester (optional) self-test or service-mode functions that allow supple-
mental performance verification.
Note: Pacemaker analyzers can be used to per-
form many of the tests in this procedure and may be 1. Qualitative Tests
useful for quick confirmation of a pacemaker’s per-
formance. For some tests, it may be necessary to use 1.1 Chassis/Housing. Examine the exterior of the
an oscilloscope. Analyzers intended for implantable unit for cleanliness and general physical condi-
or transvenous pacemakers are not suitable for test- tion. Be sure that plastic housings are intact,
ing noninvasive pacemakers unless specifically de- that all assembly hardware is present and tight,
signed with this capability. The items listed below and that there are no signs of spilled liquids or
may not be required if an analyzer is available. other serious abuse.
ECG simulator with variable amplitude (≤0.5 mV) 1.2 Mount/Fasteners. If the device is mounted on
and rate settings (from 30 to 200 ppm) the wall or on a stand, IV pole, or cart, examine
Adapters for connecting pacing cable leads to test the condition of the mount. Verify that the
equipment (these can be easily made using the mounting apparatus is secure and that all hard-
connectors of an electrode pair) ware is firmly in place. Check for weld cracks.
Ensure that the assembly is stable.
200 to 1,000 Ω noninductive load, 5 W (see manu-
facturer’s specifications) 1.3 Casters/Brakes. If the device moves on casters,
Oscilloscope check their condition and make sure they roll
and swivel freely. Check the operation of brakes
Special precautions and swivel locks.
Before performing an inspection, notify clinical staff 1.4 AC Plug. Examine the AC power plug for dam-
if the pacemaker will be removed from its normal age. Attempt to wiggle the blades to determine
storage area or if the unit will be out of use for even a if they are secure. Shake nonmolded plugs, and
few minutes; this is particularly crucial in the case of listen for rattling, which could indicate loose
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Pacemakers, External Noninvasive
screws. If damage is suspected, open the plug controls that should be returned to their original
and inspect it. positions following the inspection. It is most ap-
propriate to set the output current (mA) and rate
1.5 Line Cord. Inspect all line cords, including the (ppm) controls of noninvasive pacemakers to
battery charger line cord, for signs of damage or zero or their minimum values to minimize the
inappropriate repairs (e.g., taped sections). If risk of inadvertent activation.
replacement is necessary, be sure to wire the
new power cord or plug with the correct polarity. Examine all controls and switches for physical
condition, secure mounting, and correct motion.
1.6 Strain Reliefs. Examine the strain reliefs at Check controls that should operate against fixed-
both ends of the line cord. Be sure that they hold limit stops for proper alignment, as well as posi-
the cord securely. tive stopping. During the course of the inspection,
be sure to check that each control and switch
1.7 Circuit Breaker/Fuse. If the device has a
performs its proper function.
switch-type circuit breaker, check that it moves
freely. If the device is protected by an external 1.17 Battery/Charger. Inspect the physical condi-
fuse, check the fuse’s current rating and type tion of batteries and battery connectors, if read-
against that marked on the chassis. ily accessible. For units with internal batteries,
open the battery compartment, and examine it
If the unit has a spare fuse holder, verify that
for signs of corrosion. If corrosion residues are
a fuse of the same rating and type is provided. If
apparent or if there is evidence of liquid spillage
the spare fuse is missing, advise clinical person-
in the battery compartment, clean the compart-
nel that it is important to have a spare fuse to
ment and replace the battery. Consult the unit’s
expedite the return of the device to operation
service manual for battery condition self-tests.
when a fuse blows. They should also be advised
to notify clinical engineering or another appro- Verify that the unit or charger is plugged into
priate department whenever a fuse is blown so line power and that all batteries are either
that the appropriate personnel can investigate charged or charging. Discuss appropriate bat-
the cause and provide another spare fuse. tery cycling and replacement intervals and pro-
cedures with users. For units with removable
1.9 Cables. Inspect the cables and their strain re-
batteries, verify that an adequate number of
liefs for general condition. Examine cables care-
batteries are being maintained at full charge.
fully to detect breaks in the insulation and to
ensure that they are gripped securely in the If the battery has been in use for the maxi-
connectors of each end to prevent rotation or mum recommended time or if it is due for routine
other strain. The cable connectors should pro- replacement, install an appropriate, fully
vide an insulated connection. Replace damaged charged, new battery. Label it with the date, if
cables (e.g., loose connectors). appropriate.
1.10 Connectors. Inspect the pacing output energy 1.18 Indicators/Displays. Verify that all visual indi-
port for insulation and signs of deterioration. cators and displays, including power, mode, pace
Connect the pacing and/or multifunction cables indicator, and leads-off message, are working.
to the appropriate output ports, and verify easy Verify that control labels and markings are easy
and secure connection to the unit. to read.
1.11 Electrodes. Confirm that an adequate supply of Connect the monitoring leads to an ECG
ECG and pacemaker electrodes is available. simulator or pacemaker analyzer. Connect the
Check the expiration dates of electrodes and pacing cable to an appropriate test load or a
replace as necessary. pacemaker analyzer, start the pacemaker, and
print a strip. Verify that a pacing pulse marker
1.13 Controls/Switches. Before adjusting any con- appears on the monitor and strip. Verify that the
trols and alarm limits, check their positions; pacing marker rate varies as the pacing rate
these settings will sometimes be stored in a control is adjusted.
setup menu. If any of them appear inordinate
(e.g., a maximum rate setting), consider the pos- 1.19 User Calibration/Self-Test. Activate self-test or
sibility of inappropriate clinical use or of incipi- service-mode functions that allow supplemental
ent device failure. Record the settings of those performance verification.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
1.21 Audible Signals. Activate all audible signals, 2.10 Rate Accuracy. Use the pacemaker analyzer or
including QRS detector, heart-rate alarm, and test setup shown in Figure 1. Set the pacemaker
lead faults. Verify that the signal can be easily output to approximately 100 mA in the fixed-rate
heard in the environment in which the device mode; for demand-mode-only units, either con-
will be used. nect ECG leads to an ECG simulator set to a rate
lower than the set pacing rate or short all moni-
1.22 Labeling. Check that all necessary placards, la- toring leads together, which will simulate
bels, and instruction cards are present and leg- asystole. Pacemakers should be checked at their
ible. maximum and minimum rates and at 60 ppm.
1.24 Demand-Mode Activation/Inhibition. The Measure and record either the actual rate or
pacemaker should inhibit demand-mode pacing period of the pacemaker. To determine the rate
whenever a heart rate greater than the set pac- in pulses per minute, divide 60 sec/min by the
ing rate is detected. With a test load across the period in sec/cycle (i.e., rate [in ppm] = 60/period
pacemaker output, use an ECG simulator to [in sec]). Rate accuracy within 5% is considered
apply a normal sinus rhythm to the ECG input. to be satisfactory.
Verify that pacing is inhibited when the simu- 2.11 Amplitude Accuracy. Use the pacemaker ana-
lated heart rate (bpm) exceeds the set pacing lyzer or the test setup shown in Figure 1. Set the
rate (ppm) and that pacing activates when the pacemaker rate to about 60 ppm and the output
simulated heart rate falls below the set pacing amplitude to 50 mA. If viewing the output on an
rate. A difference of up to 10 bpm between inhi- oscilloscope, also verify that no DC voltage is
bition and activation rates is common. present. Record the peak amplitude and either
voltage or current amplitude. Repeat this test
2. Quantitative Tests with the pacemaker set to 100 mA and its maxi-
mum current. Amplitude accuracies should be
2.1 Grounding Resistance. Using an ohmmeter,
within 10%.
electrical safety analyzer, or multimeter with
good resolution of fractional ohms, measure and
3. Preventive Maintenance
record the resistance between the grounding pin
of the power cord and exposed (unpainted and 3.1 Clean the exterior.
not anodized) metal on the chassis. We recom-
3.3 Calibrate per the manufacturer’s specifications.
mend a maximum grounding resistance of 0.5 Ω.
3.4 Replace the battery, if necessary.
2.2 Chassis Leakage Current. With the grounding
conductor of plug-connected equipment tempo- 4. Acceptance Tests
rarily opened, measure chassis leakage current
to ground. Operate the device in all normal Conduct major inspection tests for this procedure
modes, including on, standby, and off; record the and the appropriate tests in the General Devices Pro-
maximum leakage current. Chassis leakage cur- cedure/Checklist 438. In addition, perform the follow-
rent to ground should not exceed 300 µA. ing test.
2.3 Pulse Width. To determine the pacemaker out- 4.1 Demand-Mode Sensitivity. Pacemaker sensitivity
put pulse width, either use the test setup shown should meet the manufacturer’s specifications;
in Figure 1 or connect the pacemaker to a pace-
maker analyzer. Set the pacemaker to approxi-
mately 100 mA at 60 bpm. The oscilloscope
sweep speed should be at least 5 msec per divi-
sion, and the trace should be set to trigger at the
beginning of the pacemaker pulse so that the
waveform covers most of the oscilloscope’s view-
ing area. Use consistent start and end points
(i.e., manufacturer’s specifications or 90% ampli-
tude points) when measuring pulse width. Typi-
cal pulse widths are 20 and 40 msec. A pulse
width within 10% of the device’s specified width Figure 1. Pacemaker pulse width, rate, and amplitude setup.
is satisfactory.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Pacemakers, External Noninvasive
most units will begin to sense an ECG waveform simulated ECG waveform, and note the ampli-
with a QRS complex of 0.5 mV or less. Therefore, tude at which pacing is inhibited.
a variable-amplitude ECG simulator that gener-
ates waveforms with R-wave amplitudes less Before returning to use
than or equal to 0.5 mV should be used. Because Ensure that all controls are set properly. Set alarms
ECG waveforms may differ on different simula- loud enough to attract attention in the area in which
tors, note the model of the simulator used, and the device will be used. Other controls should be in
use the same model when testing all pacemak- their normal pre-use positions. It is most appropriate
ers, both in the present and in the future. to set the output current (mA) and rate (ppm) controls
Using the setup in Figure 1, connect the ECG of noninvasive pacemakers to zero or their minimum
cable to the simulator with its output set to mini- values to minimize the risk of inadvertent activation.
mum amplitude or asystole. Set the pacemaker for Attach a Caution tag in a prominent position on
demand mode, and adjust the monitor for maxi- life-support equipment or any other device for which
mum sensitivity or gain. Set the pacemaker to a the user must be aware that control settings may have
rate lower than that of the simulated heart rate, been changed.
and start pacing. Verify pacing output on the oscil-
loscope and pacing markers on the monitor and Either recharge the battery, or equip the device with
recorder. Gradually increase the amplitude of the fully charged batteries.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 455-0595
Peritoneal Dialysis Units
Used For:
Peritoneal Dialysis Units [11-226]
Also Called: Peritoneal dialysis cyclers, PD cyclers
Commonly Used In: Dialysis units, patient homes
Scope: Applies to automatic peritoneal dialysis cyclers that can be used in dialysis units and in the home
Risk Level: ECRI Recommended: High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview osmosis, solvents (e.g., water) move across the
semipermeable peritoneal membrane from an area of
Peritoneal dialysis (PD) is one of several therapies lesser solute concentration to one of greater solute
used to remove metabolic wastes from the blood in the concentration. To provide a concentration gradient for
treatment of renal failure. The purpose of dialysis is to diffusion and osmosis, the dialysate contains no me-
partially replace kidney function. Although dialysis tabolic wastes and a higher concentration of solute
does not perform the endocrine functions of healthy molecules (e.g., dextrose) than the blood.
kidneys and does not promote kidney function or heal-
PD can be administered by manual or automated
ing, it slows down the deterioration of other organ
means. Manual PD can be self-administered and is
systems by ridding the blood of metabolic wastes and
gravity dependent. Using aseptic technique, the pa-
excess water.
tient instills dialysate into the peritoneal cavity.
In PD, dialysate is infused directly into the perito- The dialysate remains in the peritoneum for 30 min
neal cavity through a catheter and a sterile disposable to 8 hr, depending on selected treatment protocol,
tubing system. Usually, a permanently implanted and is then drained by positioning the bag lower than
catheter provides access to the peritoneal cavity for a the abdomen. Automated PD requires the use of a
series of dialysis sessions, although temporary cathe- PD unit, but is still gravity dependent. This device
ters are used for acute dialysis. Diffusion of metabolic consists primarily of a dialysate heater and timing
wastes from the blood occurs within the abdominal mechanisms to actuate valves that start and stop the
cavity through the pores and intracellular channels of flow of fluid into and draining from the peritoneal
the peritoneum, the membrane covering the abdomi- cavity. Most current units include additional fea-
nopelvic walls and organs. PD is based on the princi- tures, such as electronic scales, drain alarms, tem-
ples of diffusion and osmosis. Through diffusion, perature alarms, and flow alarms.
solutes (e.g., toxic metabolic wastes, electrolytes)
readily move from an area of greater concentration Citations from Health Devices
(the blood) to an area of lesser concentration (the Peritoneal dialysis cyclers [Evaluation], 1986 Feb-
dialysate) until equilibrium is reached. Through Mar; 15:31-59.
085110 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
455-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Baxter PAC-X automated PD cyclers [User Experience there are no signs of spilled liquids or other
NetworkTM], 1988 May; 17:169. serious abuse.
Test apparatus and supplies 1.2 Mount/Fasteners. If the device is mounted on a
stand or cart, examine the condition of the
Leakage current meter or electrical safety analyzer mount. Also examine the stand or cart, includ-
Ground resistance ohmmeter ing examination of the height-adjustment
Thermometer accurate to at least 0.5°C over a range mechanism, if present.
of 30° to 43°C, or a temperature monitoring device 1.3 Casters/Brakes. If the device is mounted on a
made of a thermometer sealed into one leg of a Y or stand or cart that moves on casters, check their
T connector (see the Test Equipment and Supplies condition. Verify that they turn and swivel, as
Tab in this binder) appropriate, and look for accumulations of lint and
Stopwatch or watch with a second hand thread around the casters. Check the operation of
Large graduated cylinder (2 L capacity preferred) brakes and swivel locks, if the unit is so equipped.
Consumable supplies as required by machine type, 1.4 AC Plug. Examine the AC power plug for damage.
including a tubing set, one or two 2 L bags of dia- Attempt to wiggle the blades to check that they are
lysate solution (can be expired), and two drain bags secure. Shake the plug and listen for rattles that
(3 L or larger). (To reduce costs, a single set of could indicate loose screws. If any damage is sus-
consumable supplies can be used repeatedly for pected, open the plug and inspect it.
inspections. If expired dialysate solution is not
available, an empty dialysate bag can be filled with 1.5 Line Cord. Inspect the cord for signs of damage.
2 L of tap water. This may require the use of a If damaged, replace the entire cord or, if the
funnel connected to a piece of tubing with a spike on damage is near one end, cut out the defective
one end. Place the spike into the empty dialysate portion. Be sure to wire a new power cord or plug
bag, and connect the other end of the tubing to the properly. Also check line cords of battery charg-
funnel. The water can then be poured easily into ers, if present.
the bag. After the bag is filled, clamp it at the top,
1.6 Strain Reliefs. Examine the strain reliefs at
then remove the tubing and funnel. Conspicuously
both ends of the line cord. Be sure that they hold
mark the bag so that it will not be used for a patient.)
the cord securely.
Tubing clamp
1.7 Circuit Breaker/Fuse. If the device has a switch-
Procedure type circuit breaker, check that it operates freely.
If the device is protected by an external fuse,
Before beginning the inspection, carefully read this
check its value and type against that marked on
procedure and the manufacturer’s instruction and
the chassis, and ensure that a spare is provided.
service manuals; be sure that you understand how to
operate the equipment, the significance of each control 1.9 Cables. Inspect any cables (e.g., from heating
and indicator, and the alarm capabilities. Also deter- unit to main unit) and their strain reliefs for
mine whether any special inspection or preventive general condition. Carefully examine cables to
maintenance procedures or frequencies are recom- detect breaks in the insulation and to ensure that
mended by the manufacturer. they are gripped securely in the connectors at
each end to prevent rotation or other strain.
In some units, especially the more sophisticated
Verify that there are no intermittent faults by
ones, it will be impossible to perform quantitative
flexing electrical cables near each end and look-
checks on all monitoring and alarm circuits. Refer to
ing for erratic operation or by using an ohmmeter.
the manufacturer’s service manual for suggestions
when the procedures described below cannot be carried 1.10 Fittings/Connectors. Examine all electrical ca-
out in a straightforward manner. ble connectors for general condition. Electrical
contact pins or surfaces should be straight,
1. Qualitative tests clean, and bright. If keyed connectors (e.g.,
1.1 Chassis/Housing. Examine the exterior of the pin-indexed gas connectors) are used, make sure
unit for cleanliness and general physical condi- that no pins are missing and that the keying is
tion. Be sure that plastic housings are intact, correct. Verify that tubing segments from dis-
that all hardware is present and tight, and that posable tubing sets fit securely in pinch valves.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Peritoneal Dialysis Units
1.13 Controls/Switches. Before changing any con- alarm by unplugging the device at any point
trols or alarm limits, check their positions. If during the PD cycle. If the unit has an alarm-si-
any settings appear inordinate (e.g., alarm lim- lence feature, check the method of reset (i.e.,
its at the ends of their range), consider the pos- manual or automatic) against the manufac-
sibility of inappropriate clinical use or incipient turer’s specifications. It may not be possible to
device failure. Record the settings of those con- check out all alarms at this time, since some may
trols that should be returned to their original require abnormal operating conditions that will
positions following the inspection. be simulated later in this procedure.
Examine all controls and switches for physical 1.21 Audible Signals. Operate the device to activate
condition, secure mounting, and correct motion. any audible signals. Confirm appropriate vol-
Check that control knobs have not slipped on ume, as well as the operation of a volume control,
their shafts. Where a control should operate if so equipped. If audible alarms have been si-
against fixed-limit stops, check for proper align- lenced or the volume set too low, alert clinical
ment, as well as positive stopping. Check mem- staff to the importance of keeping alarms at the
brane switches for membrane damage (e.g., from appropriate level.
fingernails, pens). During the course of the in-
spection, be sure to check that each control and 1.22 Labeling. Check that all necessary placards, la-
switch performs its proper function. bels, conversion charts, and instruction cards
are present and legible.
1.14 Heater. Examine the heater for physical condi-
tion (e.g., corrosion of its sheath, deteriorated 1.24 Pinch Valves. If pinch valves are present, check
insulation). them for mechanical integrity. Make sure they
move freely, are clean, and properly occlude the
1.15 Motor/Pump. Check the physical condition and tubing when activated. Check occlusion pres-
proper operation of these components, if present. sure as recommended by the manufacturer.
Clean and lubricate as required, and note this on Pinch valves on some devices may need to be
Lines 3.1 and 3.2 of the inspection form. (How- calibrated or checked with a calibration kit sup-
ever, do not check 3.1 and 3.2 until all necessary plied by the manufacturer. If so, obtain the kit
cleaning and lubrication are completed.) and follow the manufacturer’s recommended in-
terval for calibration or calibration checks.
1.17 Battery/Charger. Inspect the physical condition
of batteries and battery connectors, if readily 2. Quantitative tests
accessible. Check operation of battery-operated
power loss alarms, if so equipped. Operate the 2.1 Grounding Resistance. Using an ohmmeter,
unit on battery power for several minutes to electrical safety analyzer, or multimeter with
check that the battery is charged and can hold a good resolution of fractional ohms, measure and
charge. Check battery condition by activating the record the resistance between the grounding pin
battery test function or measuring the output of the power cord and exposed (unpainted and not
voltage; for lead-acid batteries, measure the spe- anodized) metal on the chassis. We recommend
cific gravity. Check the condition of the battery a maximum of 0.5 Ω. If the system is modular or
charger if present, and to the extent possible, composed of separate components, verify ground-
confirm that it does, in fact, charge the battery. ing of the mainframe and each module or compo-
Be sure that the battery is recharged or charging nent. If the device is double insulated, grounding
when the inspection is complete. When it is nec- resistance need not be measured; indicate “DI”
essary to replace a battery, label it with the date. instead of the ground resistance value.
1.18 Indicators/Displays. During the course of the 2.2 Leakage Current. Measure chassis leakage cur-
inspection, confirm the operation of all lights, rent to ground with the grounding conductor of
indicators, meters, gauges, and visual displays plug-connected equipment temporarily opened.
on the unit and charger (if so equipped). Be sure Operate the device in all normal modes, including
that all segments of a digital display function. on, standby, and off, and record the maximum
Record the reading of an hourmeter if present. leakage current. Set the thermostats so that the
heater operates while taking measurements.
1.20 Alarms. Induce alarm conditions to activate
audible and visual alarms. Check that any asso- Chassis leakage current to ground should not
ciated interlocks function. Test the power-failure exceed 300 µA.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
2.3 Fluid Temperature. Set up the PD unit accord- (expired dialysate or tap water). Set the infusion
ing to the manufacturer’s instructions, using the volume to 1 L and dwell and drain times to
2 L dialysate bag filled with expired dialysate or minimal values. After a dialysate warming pe-
tap water (at room temperature) and the tubing riod, the solution will flow from the dialysate
set. Connect the thermometer or temperature bag, through the tubing, and into the “patient”
measuring device to the end of the dialysate line bag. Using a stopwatch or watch with a second
using a T connector, and place the open end of hand, measure the dwell time and drain time
the T into an empty graduated cylinder. Set the (time from end of dwell to next fill). Cycle time
infusion volume at a volume typical of the unit’s should be within ±10% of set times.
clinical usage (e.g., 2 L for adult use, 500 mL or
1 L for pediatric use). After a dialysate warming 2.7 Ultrafiltration Monitor (if present). After com-
period (15 to 30 min), the patient fill line will pletion of the cycle-timing procedure described
open, and the dialysate will flow from the bag, above, allow all of the fluid to collect in the drain
through the tubing, and into the graduated cyl- bag. The ultrafiltration monitor should display
inder. Record the temperature of the dialysate a volume within 5% of the known volume of fluid
as it flows past the thermometer in the T connec- added to the “patient” bag at the beginning of the
tion. The temperature should be 32° to 37°C. cycle-timing procedure. Alternatively, ultrafil-
tration accuracy can be verified by confirming
2.4 Infusion Volume Accuracy. Measure the volume the accuracy of the infusion volume and drain
of fluid collected in the graduated cylinder dur- scales. Overall, ultrafiltration accuracy should
ing the dialysate temperature measurement de- be within 10%. Individual scale accuracies, if
scribed above. Be sure to wait until the infusion used for determining ultrafiltration, should be
cycle is completed before measuring the volume. within 5%.
Alternatively, infusion volume accuracy can 2.8 Fill Alarm. This alarm can be tested in the
be verified using calibrated weights rather than second cycle, following the cycle-timing proce-
fluid on some PD units. Scale accuracy verifica- dure described above. While the fluid is flowing
tion procedures may be described in the opera- from the dialysate bag into the “patient” bag,
tor’s or service manual. clamp the tubing between the two bags to oc-
clude the flow. (Note: Fill and drain alarms may
A 10% fill volume accuracy appears to be accept- work along with a timing mechanism — the
able for safe and effective treatment; however, a alarm may occur only if the proper volume of
maximum error of 5% is needed if fill and drain fluid fails to reach a specific point in a given
volumes are used to calculate ultrafiltration (UF). period of time. As a result, the alarm may not
occur until several minutes after the tubing is
2.5 Temperature Alarm. The high-temperature occluded.)
alarm can be tested using the same testing con-
figuration used for the temperature control test- 2.9 Drain Alarm. The drain alarm can similarly be
ing described above, but use warm tap water tested when the fluid is flowing from the “pa-
(about 40°C or consistent with manufacturer’s tient” bag to the drain bag. Clamp the tubing
specifications), instead of room-temperature dia- between the two bags to occlude the flow.
lysate or tap water. Verify that dialysate cannot
be delivered to the patient in a high-temperature 3. Preventive maintenance
alarm condition. A low-temperature alarm is 3.1 Clean the exterior and interior, if needed. Pay
usually not present because dialysate at room particular attention to solution deposits. Vac-
temperature is adequately warmed during the uum the air vents and cooling fans, if needed.
heating phase to prevent patient discomfort.
This has already been checked in Item 2.3. 3.2 Lubricate per the manufacturer’s instructions.
2.6 Cycle Timing. Set up the unit according to 3.3 Calibrate per the manufacturer’s instructions.
manufacturer’s instructions using a 2 L dia-
lysate bag filled with expired dialysate or water,
4. Acceptance tests
the tubing set, and the two drain bags, one Conduct major inspection tests for this procedure
simulating the patient’s peritoneal cavity and and the appropriate tests in the General Devices Pro-
the other the drain. To the “patient” bag, add a cedure/Checklist 438. In addition, perform the follow-
known volume (e.g., 500 mL) of additional fluid ing tests.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Peritoneal Dialysis Units
4.1 Leakage Current from Dialysate Line to lysate has not heated sufficiently. This feature
Ground. If the chassis leakage current meas- can be tested by the same testing configuration
ured in Item 2.2 exceeds 50 µA, measure the described in Item 2.3 but using cold (refriger-
leakage current from the patient dialysis line to ated) water instead of room-temperature water.
ground. Test with the unit in all normal operat-
ing modes and with the unit off. Before returning to use
If the device housing is not grounded, measure Set alarms loud enough to alert personnel in the
leakage currents from the patient dialysis line to area in which the device will be used.
the housing.
Attach a Caution tag in a prominent position so the
Leakage current from the patient dialysis line user is aware that control settings may have been
should not exceed 50 µA. changed.
4.2 Cold-Fluid Protection. Most units have a Recharge battery-powered devices or equip them
mechanism that prevents infusion if the dia- with fresh batteries if needed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 469-0595
Phototherapy Units
Used For:
Phototherapy Units, Visible Light, Hyperbilirubinemia [17-515]
Also Called: Bili-lights, phototherapy lamps (lights), blue lamps (lights)
Commonly Used In: Neonatal intensive care units, hospital nurseries, homes
Scope: Applies to phototherapy units with overhead lamps or fiberoptic pads and phototherapy lights integral
with incubators or radiant warmers
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Time Type Interval By Hospital Required
Major 12 months* months . hours
Minor NA months . hours
* For overhead lamps with fluorescent tubes, the spectral irradiance may need to be measured at more frequent
intervals, depending on the level of use and the types of tubes used. However, other tasks of this IPM procedure
typically need not be performed on a more frequent basis.
Overview Fiberoptic phototherapy systems apply therapeutic
light using a plastic pad. The light is delivered from a
Hyperbilirubinemia is characterized by elevated levels tungsten-halogen bulb through a fiberoptic cable and
of bilirubin (a pigment in the blood derived from hemo- is emitted from the sides and ends of the fibers inside
globin). The condition is typically associated with jaun- the pad. Filters are used to maximize light output
dice — a yellowish skin discoloration that affects within the blue spectrum. Some systems provide light
many newborns. Phototherapy units are used to re- intensity controls to adjust the irradiance levels of the
duce bilirubin levels in the blood. These units emit light sources.
visible light, which photodegrades bilirubin into ex-
cretable photoproducts. Blue light (420 to 480 nm) is Any ultraviolet (UV; 280 to 400 nm) or near-infrared
considered most effective. (IR; 780 to 1,400 nm) radiation that is emitted by these
light sources must be filtered because both UV and IR
Overhead phototherapy lamps can be one of two radiation, at high enough levels or for long exposure
types: a bank of fluorescent tubes or a tungsten-halo- periods, can damage the eyes (retina and cornea) and
gen spotlight. Fluorescent tubes that are typically the skin. Fluorescent tubes emit mostly UV; in units
used include (1) wide-spectrum white light (e.g., day- with fluorescent tubes, the UV is blocked by the Plexi-
light, cool white), (2) regular wide-spectrum blue light glas cover. Tungsten-halogen bulbs emit UV and IR;
(designated F20T12/B), or (3) narrow-spectrum blue in units with these bulbs, the radiation is blocked by
light (e.g., Special, or Super, Blue; F20T12/BB). Tung- UV/IR filters or heat-reflecting mirrors.
sten-halogen bulbs are filtered for maximum light
output within the blue spectrum. Light intensity can Radiometers are used to measure the light perform-
be controlled by changing the distance between the ance of phototherapy units in a clinical setting. These
patient and the light source. devices take a single measurement across a relatively
232562 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
469-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
wide band of wavelengths concentrated in the region operate the equipment, the significance of each control
considered most therapeutically effective. The readings and indicator, and the alarm capabilities. Also deter-
(displayed in units of µW/cm2/nm) are intended to pro- mine whether any special inspection or preventive
vide an effective irradiance measurement that users maintenance procedures or frequencies are recom-
can relate to the light’s ability to degrade bilirubin. No mended by the manufacturer.
standards currently specify phototherapy treatment
levels. However, a minimum average spectral irradi- 1. Qualitative tests
ance of 4 µW/cm2/nm in the range of 425 to 475 nm has 1.1 Chassis/Housing. Examine the exterior of the
been suggested. Most medical textbooks recommend unit for cleanliness and general physical condi-
average levels in the range of 6 to 12 µW/cm2/nm. tion. Be sure that plastic housings are intact,
that all hardware is present and tight, and that
Citations from Health Devices there are no signs of spilled liquids or other
Freestanding phototherapy units [Evaluation], 1981 serious abuse.
Apr-May; 10:133-51.
1.2 Mount/Fasteners. If the device is mounted on a
Fiberoptic phototherapy systems [Evaluation], 1995 stand or cart, examine the condition of the
Apr; 24:134-52. mount. If it is attached to a wall or rests on a
shelf, check the security of this attachment.
Test Equipment and Supplies 1.3 Casters/Brakes. If the device moves on casters,
Leakage current meter or electrical safety analyzer check their condition. Verify that they turn and
Ground resistance ohmmeter swivel, as appropriate, and look for accumula-
tions of lint and thread around the casters.
Radiometer that measures spectral irradiance
Check the operation of brakes and swivel locks,
across the wavelength band of 425 to 475 nm
if the unit is so equipped. Conductivity checks,
Note: A radiometer’s reading depends on the unique where appropriate, are usually done more effi-
spectral response characteristics of each model pho- ciently as part of a check of all equipment and
totherapy device and radiometer. Therefore, only irra- furniture in an area.
diance readings for a particular light
1.4 AC Plug/Receptacles. Examine the AC power
source/radiometer combination can be compared.
plug for damage. Attempt to wiggle the blades to
Readings from different manufacturers’ radiometers
check that they are secure. Shake the plug and
for the same light source cannot be compared. It is not
listen for rattles that could indicate loose screws.
necessary to use a phototherapy unit manufacturer’s
If any damage is suspected, open the plug and
radiometer.
inspect it.
Special precautions 1.5 Line Cord. Inspect the cord for signs of damage.
Plexiglas covers, for phototherapy units with fluo- If damaged, replace the entire cord or, if the
rescent tubes, must be put back in place after tube damage is near one end, cut out the defective
replacement. portion.
ECRI has received reports of inappropriate replace- 1.6 Strain Reliefs. Examine the strain reliefs at
ment of fluorescent phototherapy tubes with UV tubes. both ends of the line cord. Be sure that they hold
Although these UV light sources may emit some blue the cord securely. If the line cord is detachable
light and may have the same pin bases and dimensions (by the user), affix the cord to the unit so that it
as the correct tubes, they are not intended for pho- cannot be removed by the operator. (See Health
totherapy of hyperbilirubinemia and may expose in- Devices 1993 May-Jun; 22:301-3.)
fants to hazardous levels of UV radiation. 1.7 Circuit Breaker/Fuse. If the device has an ex-
Do not touch the glass of tungsten-halogen bulbs. ternal circuit breaker, check that it operates
Hold the bulb with a cloth during installation. freely. If the device is protected by an external
fuse, check its value and type against that
Procedure marked on the chassis and ensure that a spare
is provided.
Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and 1.8 Fiberoptic Pads/Cables. Inspect any fiberoptic
service manuals; be sure that you understand how to pads and cables associated with the phototherapy
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Phototherapy Units
unit for general condition. Check that there are 2. Quantitative tests
no unusual dark spots across the pad when the
light unit is turned on. Carefully examine insu- 2.1 Grounding Resistance. Using an ohmmeter,
lation of cables for broken fibers. electrical safety analyzer, or multimeter with
good resolution of fractional ohms, measure and
1.10 Fiberoptic Cable Connector. Verify that the fi- record the resistance between the grounding pin
beroptic cable is firmly gripped by its cable of the power cord and exposed (unpainted and
connector. not anodized) metal on the chassis. We recom-
mend a maximum of 0.5 Ω. If the system is
1.12 Filters/Heat-Reflecting Mirrors. In pho- modular or composed of separate components,
totherapy units with tungsten-halogen bulbs, verify grounding of the mainframe and each
check the condition of the IR/UV filter for any module or component. If the device is double
noticeable scratches or flaking. Clean with insulated, grounding resistance need not be
manufacturer-recommended solutions. In pho- measured; indicate “DI” instead of the ground
totherapy units with fluorescent tubes, check resistance value.
that the Plexiglas cover (UV filter) is clean and
in place. If the device has an accessory receptacle,
check its grounding to the main power cord.
1.13 Controls/Switches. Examine all controls and
2.2 Leakage Current. Measure chassis leakage cur-
switches for physical condition, secure mount- rent to ground with the grounding conductor of
ing, and correct motion. Check that control plug-connected equipment temporarily opened.
knobs have not slipped on their shafts. Where a
Operate the device in all normal modes, includ-
control should operate against fixed-limit stops, ing on, standby, and off; record the maximum
check for proper alignment, as well as positive leakage current. If the unit has heating and
stopping. During the course of the inspection, be
cooling modes, set the thermostats so that each
sure to check that each control and switch per- operates while taking measurements.
forms its proper function.
Measure chassis leakage current with all ac-
1.14 Heater. If the unit is integral with a radiant cessories normally powered from the same line
warmer, refer to the Radiant Warmers Proce- cord connected and turned on and off. This in-
dure/Checklist 419. cludes other equipment that is plugged into the
primary device’s accessory receptacles, as well
1.15 Fan. Check the physical condition and proper as equipment plugged into a multiple outlet strip
operation of the fan, if so equipped. Clean and (“Waber strip”) so that all are grounded through
lubricate as required, and note this on Line 3.1 a single line or extension cord.
and 3.2 of the inspection form.
Chassis leakage current to ground should be
1.18 Indicators/Displays. During the course of the 300 µA or less.
inspection, confirm the operation of all indica-
tors on the unit. Be sure that all segments of a 2.10 Spectral Irradiance. Measure spectral irradi-
digital display function. Record reading of an ance with a radiometer, and determine an aver-
hourmeter, if present. age of at least three measurements. Use the same
model radiometer and sensor head with the same
1.20 Alarms. Induce alarm conditions to activate phototherapy unit and the same method of meas-
audible and visual alarms. urement as used to obtain baseline readings dur-
ing acceptance testing (see Item 4.1). Compare
1.21 Audible Signals. Operate the device to activate the average irradiance with the average value
any audible signals. determined during acceptance inspection.
1.22 Labeling. Check that all necessary placards, Replace fluorescent tubes if light has dropped
labels, and instruction cards are present and 20% to 30% below the baseline value (the se-
legible. lected level should be no lower than 4
µW/cm2/nm) or after the manufacturer-specified
1.23 Accessories. Verify that user-operated radiome- number of operating hours. When the spectral
ters are returned for manufacturer calibration irradiance level is marginal, it may be desirable
at least annually. to determine that it is not due to low line voltage
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
(i.e., below 105 VAC). Replace fluorescent tubes units with fluorescent tubes, note the type of
having output below acceptable levels, as well as tube(s) and tube combinations that are used.
tungsten-halogen bulbs when they have burned Also, record the model of the radiometer and
out, and indicate this on Line 3.4 of the inspec- identification (control and/or serial number) of
tion form. the sensor head. To ensure consistent measure-
ments in future inspections, it is important to
3. Preventive maintenance describe the position of measurement in relation
3.1 Clean the exterior (interior, if appropriate). to the light source (a diagram may be useful) and
the method of averaging data. Otherwise, meas-
3.2 Lubricate the fan, if necessary. ure at a normal operating distance (e.g., 20 in)
3.4 Replace tube(s)/bulb, if necessary. from an overhead lamp, along a line that marks
the central axis. For fiberoptic phototherapy sys-
4. Acceptance tests tems, measure irradiance on the surface of a pad
at a central position.
Conduct major inspection tests for this procedure
and the appropriate tests in the General Devices Pro- Determine if the manufacturer recommends
cedure/Checklist 438. In addition, perform the follow- inspection and/or tube/bulb replacement at a
ing test: specified interval.
4.1 Baseline Spectral Irradiance. Measure spectral
irradiance with a radiometer and determine an Before returning to use
average of at least three measurements. Units
with variable intensity should be adjusted to the Ensure that all controls are set properly. If the unit
maximum setting. Measure and record line volt- is being used at home, ensure that all controls are set
age supplied to the phototherapy unit and, for correctly before it is returned to the patient.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 470-0595
Physical Therapy Ultrasound Units
Used For:
Ultrasound Units, Physical Therapy [11-248]
Ultrasound Units/Neuromuscular Stimulators, Physical Therapy [17-908]
Also Called: Therapeutic Ultrasound
Commonly Used In: Physical therapy departments and clinics
Scope: Tabletop, portable, and cart- or wall-mounted therapeutic ultrasound units and combination ultra-
sound/neuromuscular stimulator units
Risk Level: ECRI Recommended, Low; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
* Output power should be tested following any user report that a transducer has been dropped, has been
operated without proper coupling to a patient, or is generating heat. It is also generally necessary to calibrate
output power following transducer replacement or repair to the ultrasound unit.
Overview skin. Not using gel or using an inadequate amount will
cause heat at the transducer/skin interface instead of
Therapeutic ultrasound units convert electromagnetic the underlying tissues, possibly burning the patient.
energy to high-frequency (i.e., 1 or 3 megahertz [MHz])
sound waves that penetrate tissues to produce pain Most units allow selection of a continuous mode, in
relief through thermal and nonthermal physiologic which the output power is constant, or a pulsed mode,
reactions. This conversion of energy occurs in the in which the output is switched on and off; the pulse
transducer, or sound or treatment head, of the ma- rate is typically 60 to 120 pulses per second (pps),
chine. Ultrasound as a modality can be used inde- although some units operate at a higher or lower rate.
pendently or in conjunction with a neuromuscular Pulsed waves are further characterized by the duty
stimulator to enhance pain-relief mechanisms. cycle, the percentage of time that ultrasound waves are
present during a pulsed period. Typical duty cycles
A therapeutic ultrasound unit has two basic compo- range from 20% to 50%. Because the output power of
nents — a generator and a transducer. The electrical a pulsed waveform averaged over the on and off phase
output of the generator is applied through a flexible of the cycle is lower, it causes less heating than a
cable to a piezoelectric crystal in the transducer. The continuous output on the same setting.
electrical energy is converted into sound energy
through the reverse piezoelectric effect: as the voltage Since there is no direct indicator of internal tissue
alternates across it, the crystal expands and contracts, temperature, the operator depends on patient feed-
creating vibrations. This sound energy exits the back to adjust the intensity of the treatment and
transducer in a collimated beam pattern. A special prevent burns. The operator can, however, estimate
coupling gel is used to facilitate transmission of the the output strength by knowing the transducer’s effec-
ultrasound beam from the transducer to the patient’s tive radiating area (ERA), the sound wave frequency,
232563 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
470-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
and the length of treatment. Ultrasound units specify and service manuals; be sure that you understand how
output as power (watts) and/or as intensity (power to operate the equipment and know the significance of
divided by a transducer’s ERA in cm2 [watts/cm2]. The each control and indicator. Also determine whether
maximum output of most units does not exceed 20 any special inspection or preventive maintenance
watts. procedures or frequencies are recommended by the
manufacturer.
Some units have an automatic shutoff that discontin-
ues therapy and stops the unit’s treatment timer when Note: To prevent damage to the transducer, it must
there is insufficient coupling between the transducer and be connected to the load of the power meter/balance any
the patient; they can also have an audible and/or visible time that the ultrasound unit is operating during this
alarm to alert the user to the problem. Some units also procedure (e.g., for leakage current or timer accuracy
accommodate the use of two transducers at a time, either measurements).
to treat two separate areas on one patient or to treat two
patients at once. In addition, some vendors offer water- Reliable ultrasound power measurements require a
tight transducers for use in underwater therapy. significant amount of user technique to properly posi-
tion and couple the transducer to the test device. Most
In a neuromuscular electrical stimulator, an elec- test devices require degassed water (water with less
tronic generator transmits pulses of energy through than 5 ppm dissolved oxygen) for a coupling medium.
the sound head, which acts as the active electrode, and In hospitals, this requirement can frequently be met
into the tissue. Pulse waveforms are monophasic by using sterile distilled water prepared by most cen-
(either positive or negative) or biphasic; typically, a tral sterile supply/materials management depart-
biphasic waveform is used in conjunction with the ments (the water should be sealed in an airtight
ultrasound therapy. The pulse rate is variable; gener- container immediately after preparation). Water is
ally, 80-150 pps are used therapeutically. The pulse usually sufficiently degassed after boiling for 30 min-
amplitude is adjusted separately for each modality, utes and sealing the container. Boiling the water in a
allowing the maximum benefit from both modalities flask makes it easy to seal and cool in a refrigerator.
while maintaining patient comfort. (Some users find it convenient to store and transport
Neuromuscular stimulation produces some local degassed water in 2 L plastic soft drink bottles.) Gen-
thermal and chemical changes in the patient; however, tly pour the degassed water into the test cavity of the
it is most often used to create a muscle contraction. power meter/balance, avoiding turbulent flow.
When electrical stimulation is used in conjunction with
ultrasound, the active electrode can be manipulated to 1. Qualitative tests
produce a rhythmic contraction/release episode in the
1.1 Chassis/Housing. Examine the exterior of the
muscle or muscle group that is most affected by the
unit for cleanliness and general physical condi-
injury. The contraction/release acts as a pump and
tion. Be sure that plastic housings are intact,
promotes the removal of metabolic by-products, which
that all hardware is present and tight, and that
helps reduce spasm and pain.
there are no signs of spilled liquids or other
serious abuse.
Test apparatus and supplies
Leakage current meter or electrical safety analyzer 1.2 Mount/Fasteners. If the device is mounted on a
Ground resistance ohmmeter stand or cart, examine the condition of the
mount. If it is attached to a wall or rests on a
Stopwatch shelf, check the security of this attachment.
Ultrasound power balance or meter (1 to 30 watts, 5%)
1.3 Casters/Brakes. If the device moves on casters,
50 to 500 mL degassed water check their condition. Verify that they turn and
Manufacturer-specified test load (for units with swivel, as appropriate, and look for accumula-
neuromuscular stimulators) tions of lint and thread around the casters.
Check the operation of brakes and swivel locks,
Oscilloscope (for units with neuromuscular stimula-
if the unit is so equipped.
tors)
1.4 AC Plug/Receptacles. Examine the AC power
Procedure plug for damage. Attempt to wiggle the blades to
Before beginning an inspection, carefully read check that they are secure. Shake the plug and
this procedure and the manufacturer’s instruction listen for rattles that could indicate loose screws.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Physical Therapy Ultrasound Units
If any damage is suspected, open the plug and Check that control knobs have not slipped on
inspect it. their shafts. Where a control should operate
against fixed-limit stops, check for proper align-
1.5 Line Cord. Inspect the cord for signs of damage. ment, as well as positive stopping. During the
If damaged, replace the entire cord or, if the course of the inspection, be sure to check that
damage is near one end, cut out the defective each control and switch performs its proper func-
portion. Be sure to wire a new power cord or plug tion.
with the correct polarity.
1.18 Indicators/Displays. During the course of the
1.6 Strain Reliefs. Examine the strain reliefs at inspection, confirm the operation of all lamps,
both ends of the line cord. Be sure that they hold indicators, meters, gauges, and visual displays
the cord securely. If the line cord is detachable on the unit. Be sure that all segments of a digital
(by the user), we recommend that the cord be display function.
affixed to the unit so that it cannot be removed
by the operator. 1.19 User Calibration. Verify that the calibration
function operates, if so equipped.
1.7 Circuit Breaker/Fuse. If the device has an ex-
ternal circuit breaker, check that it operates 1.21 Audible Signals. Operate the device to activate
freely. If the device is protected by an external any audible signals. Confirm appropriate vol-
fuse, check its value and type against that ume, as well as the operation of a volume control,
marked on the chassis. if so equipped.
1.9 Cables. Inspect any cables (e.g., sensor, elec- 1.22 Labeling. Check that all necessary placards, la-
trode, remote control) and their strain reliefs for bels, conversion charts, and instruction cards
general condition. Carefully examine cables to are present and legible.
detect breaks in the insulation and to ensure that 1.23 Accessories. Confirm the presence and condition
they are gripped securely in the connectors at of accessories, such as ultrasound coupling gel
each end to prevent rotation or other strain. (check the expiration date), different size/fre-
Verify that there are no intermittent faults by quency transducers, and neuromuscular stimu-
flexing electrical cables near each end and look- lator electrodes and probes.
ing for erratic operation or by using an ohmmeter.
2. Quantitative tests
1.10 Fittings/Connectors. Examine all electrical ca-
ble connectors for general condition. Electrical 2.1 Grounding Resistance. Using an ohmmeter,
contact pins or surfaces should be straight, electrical safety analyzer, or multimeter with
clean, and bright. Verify that leads and elec- good resolution of fractional ohms, measure and
trodes are firmly gripped in their appropriate record the resistance between the grounding pin
connectors. If keyed connectors are used, make of the power cord and exposed (unpainted and
sure that no pins are missing and that the keying not anodized) metal on the chassis. We recom-
is correct. mend a maximum of 0.5 Ω. If the system is
modular or composed of separate components,
1.11 Transducers/Electrodes. Confirm that any nec- verify grounding of the mainframe and each
essary transducers and/or electrodes are on module or component. If the device is double-in-
hand and check their physical condition. sulated, grounding resistance need not be meas-
ured; indicate “DI” instead of the ground
1.13 Controls/Switches. Before changing any con-
resistance value.
trols or alarm limits, check their positions. If any
settings appear inordinate (e.g., a gain control at 2.2 Leakage Current. For units that are not double-
maximum, alarm limits at the ends of their insulated, measure chassis leakage current to
range), consider the possibility of inappropriate ground with the grounding conductor temporar-
clinical use or of incipient device failure. Record ily opened. Operate the device in all normal
the setting of those controls that should be re- modes, including on, standby, and off, and record
turned to their original positions following the the maximum leakage current. Chassis leakage
inspection. current to ground should be 300 µA or less.
Examine all controls and switches for physical 2.3 Timer. Connect the transducer to the power me-
condition, secure mounting, and correct motion. ter/balance. At a timer setting of 1 minute and at
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
maximum output, verify that output is switched tive load specified by the stimulator manufac-
off (i.e., the power meter/balance indicates no turer (commonly, a precision 1,000 Ω, ≥1⁄4-watt
output) in 1 min ±10 sec. (At settings above 5 min, resistor) and to an oscilloscope. At maximum,
timers should be accurate to within 10%.) midrange, and low stimulator output settings,
determine the voltage from the oscilloscope for
2.10 Ultrasound Power. Identify the power meter/
the corresponding waveforms. Compare the volt-
balance used for this test and its specified test
ages or derived currents (voltage ÷ test load
error in the “Notes” section of the inspection
resistance) to those set on and/or displayed by
form, and carefully follow all manufacturer di-
the stimulator at each setting. Refer to the
rections for its use. With the ultrasound unit
manufacturer’s accuracy specification, although
selected for continuous output, measure output
the measured output for most units can be ex-
power at maximum, midrange, and low settings
pected to be within 10%.
(e.g., 20, 10, and 5 watts). (If the unit has output
indicated and displayed only in units of intensity
[watts/cm2], it will be necessary to convert to 3. Preventive maintenance
watts by multiplying each intensity setting by 3.1 Clean the exterior and interior, if needed.
the value of the transducer’s area. For example,
at an intensity setting of 5 watts/cm2, a 4 cm2 3.3 Calibrate per the manufacturer’s instructions.
transducer should emit 20 watts.) Measured val-
ues should be within 20% at each setting (25% 4. Acceptance tests
would be acceptable, allowing for a test error of
5%). If the unit has more than one transducer Conduct major inspection tests for this procedure
and/or frequency, perform this test at both fre- and the appropriate tests in the General Devices Pro-
quencies for each transducer, recording the cedure/Checklist 438.
transducer serial number and the selected fre-
quency for each test. Before returning to use
2.11 Stimulator Voltage or Current. Connect the Make sure that power controls are set to zero output
leads of the neuromuscular stimulator to a resis- level.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 443-0595
Pneumatic Tourniquets
Used for:
Tourniquets, Pneumatic [14-074]
Also Called: Surgical tourniquets, automatic tourniquets, arterial tourniquets
Commonly Used In: Operating rooms
Scope: Applies to pneumatic tourniquets used during limb surgery
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview must remain inflated until the infused agent has been
sufficiently absorbed.
Pneumatic tourniquets are primarily used to occlude
blood flow and maintain a bloodless surgical field dur- Nerve damage, although rarely permanent, is the
ing limb surgery. Inflating the tourniquet cuff to a most common tourniquet-related injury. Injury is
suprasystolic pressure compresses the arteries and likely to result from extended application time and/or
arrests circulation. The fundamental objective of a excessive cuff pressure. Tourniquet literature sug-
pneumatic tourniquet is to reliably maintain the mini- gests that the application period be limited to 1 hr on
mum pressure necessary to stop blood flow in the limb. arms and 11⁄2 hr on legs.
These devices have four basic components: a cuff Sudden depressurization — such as would occur if
that is usually applied around the proximal portion of a connector came loose — or insufficient pressure from
a limb, a means for inflating the cuff bladder (e.g., a slow leak may also cause injury. If cuff pressure falls
compressed gas, hand or electric pump), an indicator below the patient’s systolic pressure during the first
for monitoring cuff pressure, and a means of regulating 20 min of IVRA, serious adverse reactions (e.g., cardio-
this pressure. Some tourniquet controllers also have vascular collapse, convulsions, coma) or death can
a timer or elapsed-time meter. result from the anesthetic entering the circulatory
system. Venous congestion or edema may also occur if
In addition to providing a bloodless surgical field, a cuff pressure falls between systolic and diastolic.
pneumatic tourniquet used during intravenous re-
gional anesthesia (IVRA) prevents infused local anes- Tourniquets inflated with oxygen or nitrous oxide
thetic (e.g., lidocaine) from flowing out of the limb until present a fire risk. Nevertheless, we continue to see
most of the infusion has been absorbed by limb tissues oxygen routinely used for this purpose, and some tour-
(about 20 min). This technique usually employs a niquet manufacturers sanction oxygen inflation in
dual-bladder cuff and a control valve for interfacing a their operator’s manuals and sell oxygen fittings. We
standard tourniquet controller with the dual-bladder emphasize that tourniquets should never be inflated
cuff. Because the various anesthetics used for IVRA with oxygen or nitrous oxide; rather, compressed air
are potentially toxic, at least one of the two bladders or nitrogen should be used.
017859 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
443-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Citations from Health Devices 1.4 AC Plug. Examine the AC power plug for dam-
age. Attempt to wiggle the blades to determine
Pneumatic tourniquets [Evaluation], 1984 Oct; 13:299. that they are secure. Shake the plug and listen
for rattles that could indicate loose screws. If
Maintaining pneumatic tourniquets: Who is responsi-
any damage is suspected, open the plug and
ble? 1984 Oct; 13:316.
inspect it.
Test apparatus and supplies 1.5 Line Cord. Inspect the cord for signs of damage.
Leakage current meter or electrical safety analyzer If damaged, replace the entire cord or, if the
(line-powered units only) damage is near one end, cut out the defective
portion. Be sure to wire a new power cord or plug
Ground resistance ohmmeter observing correct polarity.
Pressure gauges or meter to ≥1,000 mm Hg
1.6 Strain Reliefs. Examine the strain reliefs at
Hoses, T fittings, and adapters for connecting both ends of the line cord. Be sure that they hold
squeeze bulb and pressure gauge or meter the cord securely.
Cylindrical object to simulate an arm (1 lb coffee can 1.7 Circuit Breaker/Fuse. If the device has a
or a pipe with 3 to 4 in outer diameter) switch-type circuit breaker, check that it moves
Squeeze bulb with bleed valve freely. If the device is protected by an external
fuse, check its value and type against that
Stopwatch or watch with a second hand
marked on the chassis, and ensure that a spare
is provided.
Procedure
Before beginning an inspection, carefully read this 1.8 Tubes/Hoses. Check the condition of all tubing
procedure and the manufacturer’s instruction and and hoses. Be sure that they are not stretched,
service manuals; be sure that you understand how to cracked, kinked, or dirty. If the device has hose
operate the equipment, the significance of each control barbs, ensure that tubing/hoses fit tightly and are
and indicator, and the alarm capabilities. Also deter- not stretched at these sites. Because serious
mine whether any special inspection or preventive consequences can result from sudden cuff depres-
maintenance procedures or frequencies are recom- surization, replace any questionable hoses.
mended by the manufacturer. 1.10 Fittings/Connectors. Examine all fittings and
Although most units are gas powered and have few connectors for general condition. Gas fittings
(if any) alarms, we have included electrical safety and should lock tightly and should not leak. If keyed
electronic component functional tests for use on those connectors (e.g., pin-indexed gas connectors) are
units, where appropriate. used, make sure that no pins are missing and
that the keying is correct. Gas source connectors
1. Qualitative tests should not be compatible with oxygen or nitrous
oxide supplies.
1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condi- 1.13 Controls/Switches. Before moving any controls
tion. Be sure that plastic housings are intact, or alarm limits, check their positions. If any of
that all hardware is present and tight, and that them appear inordinate (e.g., a cuff pressure set
there are no signs of spilled liquids or other at maximum), consider the possibility of inappro-
serious abuse. priate clinical use or of incipient device failure.
1.2 Mount/Fasteners. If the device is mounted on a Examine all controls and switches for physical
stand or cart, examine the condition of the condition, secure mounting, and correct motion.
mount. Check that control knobs have not slipped on
their shafts. If a control should operate against
1.3 Casters/Brakes. If the device moves on casters, fixed-limit stops, check for proper alignment, as
check their condition. Look for accumulations of well as positive stopping. Check membrane
lint and thread around the casters, and be sure switches for membrane damage (e.g., from fin-
that they turn and swivel, as appropriate. Check gernails, pens). During the course of the inspec-
the operation of brakes and swivel locks, if the tion, be sure to check that each control and
unit is so equipped. switch performs its proper function.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Pneumatic Tourniquets
1.15 Motor/Pump. Check the proper operation of operate properly and hold securely. Velcro-type
these components (line-powered units only). fasteners should be clean, since excessive dirt or
lint may affect their ability to fasten securely.
1.17 Battery/Charger. Inspect the physical condi-
tion of batteries and battery connectors, if read- Test the cuffs for leaks by wrapping each
ily accessible. Check operation of around a cylindrical object and connecting it to
battery-operated power-loss alarms, if so pressure gauge or meter with a T fitting. Use a
equipped. Operate the unit on battery power for squeeze bulb to inflate the cuff to 300 mm Hg.
a minimum of 15 min to check that the battery Cuff pressure should remain unchanged after 1
is charged and can hold a charge. (The inspec- min. (This procedure may be performed simulta-
tion of controller stability [Item 2.4] or timer neously with Item 2.4 or 2.5.) Leak test both
[Item 2.5] may be carried out simultaneously on bladders of dual-bladder cuffs.
battery power to help confirm adequate battery
capacity.) Check battery condition by activating 1.24 Dual-Bladder Control Valve. Verify that tubing
the battery test function, if so equipped. Check and connectors are secure and in good condition.
the condition of the battery charger, and to the Check that fittings are secure and do not leak
extent possible, confirm that it does, in fact, and that tubing is not stretched, cracked,
charge the battery. Be sure that the battery is kinked, or dirty. Connect the control valve to the
recharged or charging when the inspection is tourniquet controller and a dual-bladder cuff.
complete. When it is necessary to replace a bat- Verify correct functioning of the control valve,
tery, label it with the date. including ability to sequentially have one cuff
(proximal) inflated, both cuffs inflated, and one
1.18 Indicators/Displays. During the course of the cuff (distal) inflated.
inspection, confirm the operation of all lights,
indicators, meters, gauges, and visual displays 2. Quantitative tests
on the unit and charger (if so equipped). Be sure
2.1 Grounding Resistance. Using an ohmmeter,
that all segments of a digital display function
electrical safety analyzer, or multimeter with
and that gauges read zero with no pressure ap-
good resolution of fractional ohms, measure and
plied.
record the resistance between the grounding pin
1.20 Alarms. Where possible, induce alarm condi- of the power cord and exposed (unpainted and
tions (e.g., kinked tube, cuff underpressure and not anodized) metal on the chassis. We recom-
overpressure) to activate audible and visual mend a maximum of 0.5 Ω.
alarms. Disconnect the cuff to simulate under-
2.2 Leakage Current. Measure chassis leakage cur-
pressurization, and squeeze the inflated cuff to
rent to ground with the grounding conductor of
produce an overpressure. If the unit has an
plug-connected equipment temporarily opened.
alarm-silence feature, check the method of reset
Check the unit while on and off, and record the
(i.e., manual or automatic) against the manufac-
maximum leakage current. Chassis leakage cur-
turer’s specifications.
rent to ground should not exceed 300 µA.
1.21 Audible Signals. Operate the device to activate
2.3 Maximum Cuff Pressure. Disconnect the cuff
any audible signals, including elapsed time indi-
from the tourniquet controller, and in its place
cators. Confirm appropriate volume, as well as
connect a T fitting attached to the pressure
the operation of a volume control, if so equipped.
gauge or meter and a squeeze bulb. Adjust the
If audible alarms have been silenced or the vol-
controller for maximum cuff pressure, then at-
ume set too low, alert clinical staff to the impor-
tempt to exceed this pressure with the squeeze
tance of keeping alarms at the appropriate level.
bulb. Verify that the maximum pressure does
1.22 Labeling. Check that all necessary placards, la- not exceed 550 mm Hg or is within 50 mm Hg of
bels, and instruction cards are present and leg- the manufacturer’s specified maximum pres-
ible. sure. While we recommend that maximum pres-
sure not exceed 550 mm Hg, many units are
1.23 Accessories. Confirm the presence and condition designed to allow higher pressures.
of all cuffs. Verify that fittings lock securely and
that the bladders and tubing are not stretched, 2.4 Controller Stability. When testing pressure in-
cracked, kinked, or dirty. The covers should be dicator accuracy (Item 2.10), observe each pres-
clean, and the fastening mechanisms should sure reading for 2 min to verify that the pressure
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
remains stable. Because experience indicates 3. Preventive maintenance
that the Kidde Model 400 may develop a valve
leak that permits excess reservoir pressure into 3.1 Clean the exterior, if needed.
the cuff, verify the stability of this controller. 3.2 Lubricate per manufacturer’s instructions.
Using the same setup as used in the previous
test, adjust the gauge or meter pressure to 400 3.3 Calibrate per manufacturer’s specifications.
mm Hg from 0 mm Hg. This pressure should
not vary more than 10 mm Hg after 15 min. 3.4 Replace tubing, hoses, cuffs, and batteries, if
needed.
2.5 Elapsed-Time Meter/Timer. Verify the accu-
racy of a timing mechanism, where present, us- 4. Acceptance tests
ing a stopwatch or watch with a second hand for
Conduct major inspection tests for this procedure
a period of 15 min. The error should not exceed
and the appropriate tests in the General Devices Pro-
2 min.
cedure/Checklist 438.
2.10 Cuff Pressure Indicator Accuracy. With the con-
troller still connected to the pressure gauge or Before returning to use
meter, verify indicator accuracy at settings of Return controls to their preinspection or normal
200 and 450 mm Hg. Observe each pressure pre-use settings. Either recharge batteries or equip
reading for 2 min. The cuff pressure indicator battery-powered devices with fresh batteries.
should be accurate to within 5%.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 471-0595
Portable Ventilators
Used For:
Ventilators, Portable [17-423]
Also Called: Respirators, home care ventilators
Commonly Used In: Home care and hospital or emergency vehicle transport
Scope: Applies to ventilators that are physically compact, totally powered by battery or AC line cord and
that have an internal chamber in which a piston driven by an internal motor pressurizes air that is delivered
to the breathing circuit; these ventilators may use external O2 source attachments for delivering supplemental
O2 therapy, external positive end-expiratory pressure (PEEP) valves, heated humidifiers, and external monitors
or remote alarms; does not apply to anesthesia units and critical care ventilators (see Procedure/Checklists
461 and 458, respectively)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 6 months* months . hours
Minor NA months . hours
* Inspection and preventive maintenance intervals should be scheduled according to the manufacturer’s
recommendations, which may be related to hours of use. However, units should have a major inspection at
least every six months. Pre-use checks should be performed by a respiratory therapist or respiratory equipment
technician.
Overview spontaneous breathing or by completely regulating a
prescribed breathing pattern for a patient who cannot
As technological advances continue to prolong life for breathe without assistance. Dependence on the
critically ill patients and make life possible for both amount and type of mechanical support varies accord-
children and adults with otherwise fatal conditions, a ing to the disorder and the presence of any pulmonary
large, rapidly growing patient population needs long- complications; therefore, ventilation needs may range
term ventilatory support. To meet these needs, some from occasional ventilator use to complete ventilator
hospitals have special care areas, such as intermediate dependency. Patients who require long-term mechani-
care or prolonged respiratory care units, where stable cal ventilation include adults and children who have
ventilator-dependent patients can remain indefinitely impaired or total loss of ventilatory function resulting
or be cared for until they are weaned from ventilatory from a variety of etiologies, such as neuromuscular
support, moved to another facility, or sent home. These diseases, restrictive and chronic obstructive lung dis-
patients do not need to be in an ICU and do not require eases, and spinal cord injuries, as well as children who
complex critical care ventilators and are instead were born with premature or neonatal lung disease.
placed on portable ventilators.
Mechanical ventilators are used to compensate for Portable ventilators are available with varying de-
deficiencies in normal breathing by aiding or augmenting grees of sophistication to meet the spectrum of needs
233036 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
471-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
of long-term ventilator users. For example, to control charged, the inspection can be carried out on battery
costs, some ventilators have limited capability for pa- power to help confirm adequate battery capacity.
tients with limited needs. Other ventilators have ad-
ditional features for pediatric use and for patients who Manufacturers’ recommended procedures for in-
may be more difficult to treat. Thus, portable ventila- spection and preventive maintenance of mechanical
tors offer some features that are usually available only ventilators vary in both methods and required accu-
on critical care ventilators (e.g., nonphysiologic breath- racy. In addition, ventilation modes, controls, and al-
ing patterns, such as inverse inspiratory:expiratory gorithms for calculated variables vary greatly
[I:E] ratio), while retaining simplicity of operation, according to manufacturer and model. This procedure
portability, and low cost. provides the basic framework for complete ventilator
inspection and preventive maintenance. Manufactur-
Citations from Health Devices ers’ recommended procedures should be added where
appropriate. References to specific pages of the manu-
Leaving ventilator-dependent patients unattended
facturer’s manual should be added to the checklist.
[Hazard], 1986 Apr; 15:102-3.
(The checklist includes blank spaces for the insertion
Remote alarms for ventilators and other life-support of these page references.)
equipment, 1986 Dec; 15:323-4.
IPM Task ManagerTM, the software component of the
Portable volume ventilators [Evaluation], 1988 Apr; Inspection and Preventive Maintenance System, en-
17:107-31. ables easy production of customized procedures and
checklists for specific ventilator models and clinical
Portable volume ventilators [Evaluation], 1992 Aug;
needs. Items performed by outside vendors can be
21:255-89.
excluded from the checklist; a separate checklist for
Disposal breathing circuits [Evaluation], 1993 Jul; use by outside vendors can be produced to ensure that
22:311-31. those items agreed upon are performed by the vendor.
Test apparatus and supplies 1. Qualitative tests
Lung simulator with expandable bellows
1.1 Chassis/Housing. Examine the exterior of the
Pressure gauge or meter with 2 cm H2O resolution
unit for cleanliness and general physical condi-
from -20 to +120 cm H2O
tion. Be sure that plastic housings are intact,
Syringe with a volume of at least 1.5 L or a volume that all hardware is present and tight, and that
monitor there are no signs of spilled liquids or other
Stopwatch serious abuse.
Ventilator tester (optional) 1.2 Mount/Fasteners. If the device is mounted on a
Various breathing circuit adapters, including a con- bracket or wheelchair tray, examine the condi-
nector that can occlude the breathing circuit’s exha- tion of the mount. If it rests on a shelf, check the
lation port security of this attachment. Check the mounting
security of all components (e.g., supplemental O2
Leakage current meter or electrical safety analyzer
equipment, heated humidifiers) or attached
Ground resistance ohmmeter monitors.
Additional items as required for a specific manufac-
1.4 AC Plug. Examine the AC power plug for dam-
turer’s procedures
age. Attempt to wiggle the blades to check that
they are secure. Shake the plug and listen for
Procedure rattles that could indicate loose screws. If any
Before beginning an inspection, carefully read this damage is suspected, open the plug and inspect
procedure and the manufacturer’s instruction and it.
service manuals; be sure that you understand how to
operate the equipment, the significance of each control 1.5 Line Cord. Inspect the cord for signs of damage.
and indicator, and the alarm capabilities. Also deter- If damaged, replace the entire cord or, if the
mine whether any special inspection or preventive damage is near one end, cut out the defective
maintenance procedures or frequencies are recom- portion. Be sure to wire a new power cord or plug
mended by the manufacturer. If the battery is fully with the correct polarity.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Portable Ventilators
1.6 Strain Reliefs. Examine the strain reliefs at Examine all controls and switches for physical
both ends of the line cord. Be sure that they hold condition, secure mounting, and correct motion.
the cord securely. If the line cord is detachable Check that control knobs have not slipped on
(by the user), affix the cord to the unit so that it their shafts. Where a control should operate
cannot be removed by the operator. (See Health against fixed-limit stops, check for proper align-
Devices [Hazard], 1993 May-Jun; 22:301-3.) ment, as well as positive stopping. Check mem-
brane switches for damage (e.g., from
1.7 Circuit Breaker/Fuse. If the device has a
fingernails, pens). During the course of the in-
switch-type circuit breaker, check that it moves
spection, be sure to check that each control and
freely. If the device is protected by an external
switch performs its proper function.
fuse, check its value and type against that
marked on the chassis and ensure that a spare 1.15 Fan/Motor. Check the physical condition and
is provided. proper operation of these components. Clean and
1.8 Tubes/Hoses. Check the condition of all tubing lubricate if required, according to the manufac-
and hoses. Be sure that they are not cracked, turer’s instructions, and note this on Lines 3.1
kinked, or dirty. and 3.2 of the form.
1.9 Cables. Inspect any cables (e.g., remote alarm 1.17 Power Sources/Internal Battery Charger. Inspect
cable) and their strain reliefs for general condi- the physical condition of the internal battery and
tion. Carefully examine cables to detect breaks battery connectors.
in the insulation and to ensure that they are
securely gripped in the connectors at each end, Verify that, the ventilator operates on AC
which will prevent rotation or other strain. power and that the AC power indicator is lit.
Where appropriate, verify that there are no in- Disconnect the device from AC power.
termittent faults by flexing cables near each end
and looking for erratic operation or by using an If an external battery is connected, verify that
ohmmeter. the ventilator switches to its external battery
and continues to operate without interruption.
1.10 Fittings/Connectors. Examine all gas fittings Verify that the external power and power
and connectors for general condition. Gas fit- switchover indicators light and that the audible
tings should be tight and should not leak. Con- alarm activates. Usually, this is a continuous
nectors to hospital central piped medical gas alarm that can be reset by pressing the alarm-
systems for delivering supplemental oxygen silence button. Disconnect the external battery.
should have the appropriate DISS or quick-con-
nect fitting to eliminate the need for adapters. Verify that if no external battery is connected
1.12 Filters. Check the condition of gas (e.g., air-in- or if the external battery is disconnected, the
let) filters. Check for corrosion residue indicative ventilator switches to its internal battery and
of liquid, gaseous, or solid particle contaminants continues to operate without interruption. Ver-
in the gas supply; advise appropriate personnel ify that the internal battery and power
if found. Clean or replace if appropriate, and switchover indicators light and that the audi-
indicate this on Lines 3.1 and 3.4 of the inspec- ble alarm activates. Usually, this is a continu-
tion form. ous alarm that can be reset by pressing the
alarm-silence button.
1.13 Controls/Switches. Before changing any con-
trols or alarm limits, check their positions. If any Operate the unit on internal battery power.
settings appear inordinate (e.g., alarm limits at Check battery condition by activating the bat-
the ends of their range), consider the possibility tery test function or measuring the output volt-
of inappropriate clinical use or of incipient device age. Verify that the battery is charged and can
failure. Investigate questionable control settings hold a charge and that the device operates for at
on a home care unit. Consult with the patient’s least 20 minutes.
physician to determine correct settings. The pa-
tient or caregiver should receive additional Reconnect the external battery, if available,
training, if required. Record the settings of those then plug the ventilator back to AC power, and
controls that should be returned to their original verify that the ventilator switches from internal
positions following the inspection. to external battery and then to AC power.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
Turn the ventilator off and verify that the 1.23 Accessories. Confirm the presence and condition
battery charging indicator is lit. A battery charg- of accessories, including the humidifier (see
ing control may need to be set on some models. Heated Humidifiers Procedure/Checklist 431)
and the nebulizer.
Be sure that the battery is recharged or
charging when the inspection is complete. When Verify that all external devices are connected
it is necessary to replace a battery, label it with into the breathing circuit or to the ventilator
the date. correctly.
Verify that all breathing circuit components
1.18 Indicators/Displays. During the course of the
(including filters) are compatible with the ventila-
inspection, confirm the operation of all lights,
tor according to the manufacturer’s recommenda-
indicators, meters, gauges, and visual displays
tions (see Health Devices 1988 Apr; 17:109). Check
on the unit. Be sure that all segments of a digital
that all breathing circuit components that were
display function. Record the reading of an hour
retained are assembled correctly.
meter, if present.
1.24 Modes. Set the ventilator to operate in control
1.20 Alarms/Interlocks. Induce the high- and low- mode. Verify that the ventilator can deliver
pressure alarms as described below and any breaths to the test lung. Set the ventilator to
other alarm conditions to activate audible and operate in the intermittent mandatory ventila-
visual alarms. Check that any associated inter- tion (IMV) mode, if so equipped, and verify that
locks function. If the unit has an alarm-silence the ventilator delivers breaths to the test lung.
feature, check the method of reset (i.e., manual
or automatic) against the manufacturer’s speci- Set the ventilator to operate in Assist/Control
fications. Verify that the remote alarm indicator mode (or Assist mode) and simulate spontaneous
functions properly. breaths by expanding the bellows of the test
lung. Verify that an assisted breath is delivered
Disconnect the breathing circuit at the tra- in response to a breathing effort when the
cheostomy tube connector to activate the low- breathing circuit exceeds the sensitivity setting.
pressure alarm. Verify that the low-pressure Adjust the sensitivity control to 1 cm H2O above
alarm activates audibly and visually and that the end-expiratory pressure, and verify that the
the alarm activates within the manufacturer’s ventilator autocycles.
specified time delay. Reattach the breathing cir-
Set the ventilator to operate in synchronized
cuit and verify that the indicator remains lit
IMV (SIMV) mode. Simulate several breathing
until manually reset.
efforts. Verify that a single assisted breath is
To activate the high-pressure alarm, adjust delivered followed by spontaneous unassisted
the high-pressure alarm limit to 5 cm H2O below breaths.
the peak inspiratory pressure (PIP). Verify that Set the ventilator to operate in pressure-cy-
the high-pressure alarm activates audibly and cled mode, if available, and set the high-pressure
visually and that the displayed pressure does not alarm limit 5 cm H2O below the peak airway
exceed the high-pressure alarm limit. Return the pressure. Verify that the ventilator cycles to
high-pressure alarm limit to its original setting exhalation when the breathing circuit pressure
and verify that the indicator remains lit until on the ventilator’s display reaches the high-pres-
manually reset. sure alarm limit.
1.21 Audible Signals. Operate the device to activate 2. Quantitative tests
any audible signals. Confirm appropriate vol-
ume, as well as the operation of a volume control, 2.1 Grounding Resistance. Using an ohmmeter,
if so equipped. If audible alarms have been si- electrical safety analyzer, or multimeter with
lenced or the volume set too low, alert clinical good resolution of fractional ohms, measure and
staff to the importance of keeping alarms at the record the resistance between the grounding pin
appropriate level. of the power cord and exposed (unpainted and
not anodized) metal on the chassis. We recom-
1.22 Labeling. Check that all necessary placards, la- mend a maximum of 0.5 Ω. If the system is
bels, and instruction cards are present and legible. modular or composed of separate components,
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Portable Ventilators
verify grounding of the mainframe and each Record the tidal volume measured by the
module or component. volume monitor at the outlet of the exhalation
valve or the PEEP valve, if used. (Volume can
2.2 Leakage Current. Measure chassis leakage cur- also be confirmed by calculating the delivered
rent to ground with the grounding conductor of tidal volume from the product of the test lung
plug-connected equipment temporarily opened. and breathing circuit compliance [C] and the
Operate the device in all normal modes, including PIP [V = C × PIP]. To determine the compliance,
on, standby, and off, and record the maximum deliver a set volume [same volume that the
leakage current. ventilator is set to deliver] to the breathing
circuit and test lung with a large syringe, and
Measure chassis leakage current with all ac-
record the resultant change in pressure at the
cessories normally powered from the same line
inlet of the test lung. The compliance is the
cord connected and turned on and off. This in-
delivered volume divided by the recorded pres-
cludes other equipment that is plugged into the
sure.) The measured volume should be within
primary device’s accessory receptacles, as well
10% of the set tidal volume.
as equipment plugged into a multiple outlet strip
(“Waber strip”) so that all are grounded through Press the sigh button, if available, to activate
a single line or extension cord. the sigh mode and verify that the sigh indicator
Chassis leakage current to ground should not illuminates. Record the delivered sigh volume
exceed 300 µA. and verify that it is within 10% of the volume
specified by the manufacturer for the set sigh
2.3 System Leakage. Refer to the manufacturer’s volume.
manual for ventilator settings. To check that
there are no leaks in the breathing circuit or in Record the number of breaths delivered dur-
the tubing within the ventilator, occlude the ing a 1-minute period. Verify that the measured
exhalation port and verify that the pressure does rate is within 1 breath/min of the set respiration
not fall more than 10 cm H2O below the PIP rate (may be ±2 breaths/min at high set rates).
between breaths. If the ventilator fails this test,
2.6 Pressure-Relief Mechanism. If the ventilator
detach the breathing circuit and repeat the test
has an adjustable pressure-relief valve, adjust
while covering the ventilator’s air outlet with a
the control to its maximum setting. Remove the
gloved hand.
test lung. Check for proper operation of the ven-
2.4 Pressure Display. Record the PIP from the ven- tilator’s internal pressure-relief mechanism by
tilator’s pressure display and from the pressure occluding the breathing circuit’s exhalation port
gauge or meter at the inlet of the test lung. The and measuring the resulting peak pressure on
ventilator display should be the within 10% or the pressure gauge. The pressure should not
±3 cm H2O (whichever is greater) of the pressure exceed the value specified by the manufacturer.
measured at the test lung. Verify that both pres- Remove the occlusion from the exhalation port
sure readings return to zero during exhalation. and reattach the test lung. Decrease the adjust-
able pressure-relief setting to its lowest setting
2.5 Control Settings. Check the operation and accu- during delivery of a machine breath and verify
racy of ventilation controls. Typically, these tests that the breathing circuit pressure lowers.
are performed by attaching the ventilator to a lung
simulator and comparing measured values to set-
3. Preventive maintenance
tings on the ventilator. The manufacturer should
recommend the appropriate ventilator settings
3.1 Clean the exterior, interior, and components, if
(e.g., tidal volume, rate, inspiratory time) to verify
needed.
proper operation and accuracy (generally within
10%). The procedures for checking the tidal volume 3.2 Lubricate the fan and/or motor, if required.
and respiration rate control are listed below. A
ventilator tester or some other method to record 3.3 Calibrate according to the manufacturer’s in-
the pressure and flow waveform is required to structions.
verify the accuracy of the other controls, which
may include inspiratory time, expiratory time, I:E 3.4 Replace components according to the manufac-
ratio, % O2 concentration, or flow. turer’s instructions.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
4. Acceptance tests normal pre-use positions. If the unit is being used at
home, ensure that controls are set correctly before it is
Conduct major inspection tests for this procedure returned to the patient.
and the appropriate tests in the General Devices Pro-
cedure/Checklist 438. Attach a Caution tag in a prominent position so that
the user will be aware that control settings may have
Before returning to use been changed.
Ensure that all controls are set properly. Set alarms
loud enough to alert personnel in the area in which the Recharge battery-powered devices or equip them
device will be used. Other controls should be in their with fresh batteries, if needed.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 435-0595
Pressure Transducers
Used For:
Transducers, Pressure [14-119]
Commonly Used In: Special care units, emergency rooms, operating rooms, cardiac catheterization
laboratories
Scope: Applies to reusable pressure transducers used for blood pressure and other physiologic pressure
monitoring; can be adapted for the purpose of verifying performance of disposable pressure transducers
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
* If users routinely use an external pressure source to verify the performance of each transducer/monitor pair
before use on a patient and if transducers are well maintained during use and processing, periodic inspection
may not be required or may be reduced to qualitative checks only.
Overview Alternative in-use calibration techniques, 1982 Nov;
12:24.
Pressure transducers are used in conjunction with
physiologic monitors to sense a pressure and convert it Disposable pressure transducers [Evaluation], 1984
into an electrical signal that is processed by the monitor Sep; 13:268.
and displayed on a digital or waveform display. Blood Electrical isolation of blood pressure channels [User
pressure transducers are generally used with a fluid- Experience NetworkTM], 1986 Dec; 15:331.
filled catheter to transmit the pressure from a point in
the circulatory system to the transducer located outside Disposable pressure transducers [Evaluation], 1988
the body. Catheter-tip transducers that are placed Mar; 17:75.
within the body and have electrical leads that leave the
Pre-use pressure transducer calibration procedure,
body through the catheter are also available.
1988 Sep; 17:278.
In addition to being used to monitor blood pressure, Disposable pressure transducers and multipressure
transducers are also used to monitor uterine and in- channel physiologic monitors [User Experience Net-
tracranial pressure. workTM], 1988 Nov; 17:357.
Citations from Health Devices Test apparatus and supplies
Physiological pressure transducers [Evaluation], 1979 Leakage current meter or electrical safety analyzer
Jul; 8:199. Ground resistance ohmmeter
Air embolism during calibration of invasive blood pres- Pressure gauge or meter (range to 300 mm Hg)
sure monitoring systems [Hazard], 1982 Nov; 12:22. Sphygmomanometer squeeze bulb
009091 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
435-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Y connector Proper calibration and use of test equipment will
increase the quality of testing.
Accurate pressure monitor
Mating connector for the transducer or small-di- 1. Qualitative tests
ameter probe to gain access to transducer connector 1.1 Chassis/Housing. Examine the exterior of the
terminals (acceptance testing only; may be part of transducer for cleanliness and general physical
an electrical safety analyzer) condition. Be sure that plastic housings are intact,
Container of 0.9% saline solution that necessary assembly hardware is present and
tight, and that there are no signs of spilled liquids
or other serious abuse. Examine — but do not
Special precautions touch — the surface of the sensing diaphragm for
The transducer diaphragm is extremely delicate nicks or dents. The transducer should be stored
and easily damaged. Do not touch the diaphragm or with a dome attached or in such a way that the
allow any tools to contact it. We recommend against transducer diaphragm is protected from damage.
the use of a mercury manometer for pressure measure-
1.2 Mount. If the transducer is mounted on a stand
ments because of the associated mercury contamina-
or IV pole, examine the condition of the mount.
tion risks.
1.9 Cables. Inspect the cable for cracks, cuts, or
Procedure pinching. Examine the strain reliefs at both
ends of the cable; be sure that they hold the cable
Before beginning an inspection, carefully read this securely.
procedure and the manufacturer’s instruction and
service manuals. Also determine whether any special 1.19 User Calibration. Connect the transducer to a
inspection or preventive maintenance procedures or monitor that has been inspected and is known to
frequencies are recommended by the manufacturer. be accurate. Perform any necessary zero and
calibration functions. The pressure reading with
We recommend assigning each transducer a sepa- no pressure applied should be within 2 mm Hg
rate equipment control number independent of the of zero (and will usually read exactly zero). If the
monitor, since any particular transducer may be used monitor has a calibration function, it should give
with more than one monitor. (Because it is difficult to a pressure reading within 5 mm Hg of the pres-
permanently tag a transducer, the serial number may sure specified by the monitor manufacturer.
be used instead of an assigned control number.)
1.23 Accessories. Confirm that monitoring kits are
Testing the accuracy of blood pressure monitors and available or that adequate stopcocks, tubing, con-
transducers presents a practical problem. Clinical nectors, and continuous flushing devices are avail-
requirements for blood pressure measurements call for able. Metal stopcocks and connectors provide a
an accuracy of 5% on arterial pressure ranges and conductive pathway to the saline in the catheter,
±2 mm Hg on venous or pulmonary pressure meas- which, in turn, could provide a conductive pathway
urements. Because the criteria apply to the measure- to the heart. Advise users to replace any metal
ment system, the individual components must have connectors and stopcocks with plastic ones.
greater accuracy. Thus, we recommend using a pres-
If the transducer is used with disposable
sure simulator to verify the accuracy of the pressure
domes, make sure that an adequate supply of
monitor to be used to test the transducer.
sterile domes is available. If the transducer has
For efficiency, first test all of the monitors in one a metal case and is not isolated, use disposable
area with a transducer simulator or one transducer diaphragm domes where blood pressure meas-
that is known to be accurate. Then, test all the urements are made (see Health Devices 1979 Jul;
transducers in that area using one monitor. Record 8:206).
the control number of the monitor used to test the
transducer. As long as the transducer/monitor combi- 2. Quantitative tests
nation is accurate to within 5% or ±2 mm Hg of a given 2.10 Pressure Accuracy. Connect the transducer to a
static pressure, the monitor and transducer can be monitor that has been inspected and is known to
considered acceptably accurate. Most pressure moni- be accurate. Connect the stem of the Y connector
tor and transducer problems result in complete failure to the transducer; connect the sphygmomanome-
of the unit or relatively large errors. ter squeeze bulb and the pressure gauge or meter
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Pressure Transducers
to the arms of the Y connector. Be sure to attach The diaphragm is very delicate. Do not con-
the transducer dome (especially a disposable dia- tact it directly with a probe. Some transducers
phragm dome) to the transducer according to the have metal cases that are in continuity with the
manufacturer’s recommendations. Carefully sensing diaphragm and can be easily contacted
zero the transducer. Test the transducer at 20, without danger of damaging the diaphragm.
100, and maximum (or 200) mm Hg. Use the Otherwise, it is necessary to make electrical
monitor’s mean arterial pressure range for the contact through saline solution. This is most
higher measurements and the venous range for conveniently done by suspending the transducer
the lower measurements. The transducer and so that the diaphragm is immersed in a noncon-
monitor combination should be accurate to ductive pan or cup of saline solution. The site
within ±2 mm Hg or 5%, whichever is greater, where the cable enters the transducer case should
for a given pressure. be kept out of the solution.
If the transducer is being tested as part of a The test setup is shown in Figure 1. Connect
monitor/transducer pair, replace this test with the saline solution to the grounded side of the
Items 2.10 and 2.11 in the Blood Pressure Moni- isolation test supply to minimize the hazard to
tors Procedure/Checklist 434. the inspector. CAUTION: To avoid electric
shock, do not touch any part of the transducer,
3. Preventive maintenance
transducer connector case, saline solution, or ex-
3.1 Clean the transducer case and cable, if neces- posed wires or probes. To simplify testing, a
sary, with a damp cloth. Do not attempt to clean connector may be made with all terminals and
the diaphragm other than by soaking and rinsing the connector shell shorted together and at-
according to the manufacturer’s instructions. tached to a single lead; this lead can then be
connected to the isolation test supply. Measure
4. Acceptance tests the current flow when 120 volts are applied to
Conduct major inspection tests for this procedure the lead of this adapter cable. Flow through an
and the appropriate tests in the General Devices Pro- isolated transducer should be less than 20 µA.
cedure/Checklist 438. In addition, perform the follow-
ing test.
Before returning to use
4.1 Isolation. Disposable diaphragm domes, if used,
provide electrical isolation and may eliminate the Submit the transducer for disinfection or steriliza-
need for checking transducer isolation. This test tion according to the hospital’s standard policy. (This
should be performed on isolated transducers is not usually required if disposable diaphragm domes
only. are used.)
Figure 1. Transducer isolation test
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 448-0595
Pulmonary Resuscitators, Gas-Powered
Used For:
Resuscitators, Pulmonary, Gas-Powered [13-366]
Also Called: Pulmonary resuscitators, oxygen-powered resuscitators, demand valves
Commonly Used In: Critical care areas, recovery rooms, emergency rooms, patient care areas, ambulances
Scope: Applies to manually cycled, pressure-limited gas-powered resuscitators; does not apply to manually
operated resuscitators (see Procedure/Checklist 422); also does not apply to pressure-cycled gas-powered
resuscitators, which are considered inappropriate for use during cardiopulmonary resuscitation (CPR) by the
American Heart Association (AHA) and the National Research Council (NRC) because these units can be
triggered into exhalation by regular chest compressions
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval* By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
*
These units should be routinely checked (see Items 1.1 and 1.25) following each use (after cleaning and
reassembly).
Overview this inspection procedure). Such units should be modi-
fied to meet AHA’s recommendations. Unless in-
Pulmonary resuscitators are relatively simple devices, structed otherwise by the manufacturer, return the
yet ECRI frequently receives reports of failures that units to be modified to the manufacturer during sched-
have led to unsuccessful resuscitations. The failures uled inspection and preventive maintenance periods.
we have investigated were caused by incorrect assem- Do not attempt to modify or repair gas-powered resus-
bly following cleaning or repair or by mechanical fail- citators unless instructed to do so by the manufacturer.
ure. Because these devices are frequently needed for When purchasing new gas-powered resuscitators, buy
lifesaving procedures, users have no time and may lack units that perform according to the criteria set forth in
the expertise to troubleshoot, repair, and reassemble this procedure.
units. Resuscitators must immediately function prop-
erly whenever they are needed. Citations from Health Devices
All earlier recommendations called for greater than Gas-powered resuscitators [Evaluation], 1978 Dec;
100 L/min outlet flow. However, the most recent AHA- 8:24-38.
recommended maximum flow criterion for gas-powered Gas-powered resuscitators [Hazard], 1988 Nov;
resuscitators is 40 L/min (JAMA 1986; 255[21]:2934). 17:352-4.
Many current gas-powered resuscitators and all gas-
powered resuscitators manufactured before 1985 will Gas-powered pulmonary resuscitators [Standards up-
exceed this criterion (keep this in mind when performing date], 1989 Oct; 18:362-3.
060258 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
448-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Test apparatus and supplies Safety System) threaded body fitting. Check that
the fitting threads are clean and free of burrs or
Pressure gauge or meter (0 to 60 cm H2O) metal particles. If the threaded fitting is at-
Lung simulator tached to an adapter, verify that the connection
50 psi oxygen source capable of providing at least is tight and that the adapter is clean and com-
100 L/min flow patible only with oxygen fittings.
100 L/min oxygen flowmeter with less than 10 cm 1.13 Controls. Examine any controls for physical
H2O back pressure (or gasometer or spirometer and condition and verify that each control performs
stopwatch or watch with a second hand) its proper function.
1.22 Labeling. Check that all necessary placards, la-
Procedure bels, conversion charts, and instruction cards
CAUTION: Inspect units only after appropriate are present and legible.
cleaning and disinfection.
1.23 Accessories. Check all accessories stored with
Before beginning an inspection, carefully read this the resuscitator. List the accessories that
procedure and the manufacturer’s instruction and should accompany each resuscitator, and check
service manuals; be sure that you understand how to them against the list at each inspection. Exam-
operate the equipment and the significance of each ine all accessories for cleanliness and mechani-
control and indicator. Also determine whether any cal integrity.
special inspection or preventive maintenance proce- Oxygen cylinders. If the resuscitator is stored
dures or frequencies are recommended by the manu- with an oxygen cylinder, check the amount of
facturer. Take appropriate precautions when working oxygen in the cylinder. Replace the cylinder
with pure oxygen (e.g., no open flames). when it is less than half full. A cylinder
wrench should be chained to the regulator and
1. Qualitative tests
yoke assembly.
1.1 Housing. Examine the exterior of the unit for Transparent face masks. An assortment of mask
cleanliness and general physical condition. Be sizes (e.g., adult, pediatric) should be stored
sure that plastic and metal housings are intact, with the resuscitator to allow its use with a
that necessary assembly hardware is present wide range of patients.
and fits tightly together, and that there are no
signs of spilled liquids, cracks, or other serious Use only transparent masks with resusci-
abuse. tators. If the hospital has opaque masks,
order transparent replacements, but do not
Examine the resuscitator’s components to remove opaque masks from use until the re-
verify that they are not from other similar model placement masks are in stock and the change
resuscitators. Even if components appear to be has been discussed with users. Inspect masks
similar, they may not function as the original and their connectors for signs of deterioration
components. For this reason, use only parts (e.g., embrittlement). Rein-flate collapsed in-
from the unit’s manufacturer. In addition, the flatable rims, and check for leaks or damage
hospital should stock only one model of manual by immersing the mask in water. Replace if
and gas-powered resuscitators to prevent inad- necessary.
vertent mixing of components.
1.24 Valve Assembly.
1.2 Mount. If the unit is attached to a wall or rests
on a shelf, check the security of the attachment. CAUTION: Before proceeding with this item,
The unit should be available for immediate use. be certain that you are familiar with the correct
valve assembly. Misassembly will likely cause the
1.8 Tubes/Hoses. Check the condition of all tubing resuscitator to fail, which may result in patient
and hoses, especially at connectors. Be sure that death. Verify valve operation (Item 1.25) after
they are not cracked, kinked, or dirty. reassembly.
1.10 Fittings/Connectors. Verify that gas-powered Ideally, the valve should require no disassem-
resuscitators are fitted with an oxygen supply bly for cleaning. However, some models must be
hose and have an appropriate connector for an partially disassembled. Therefore, disassemble
oxygen source, usually a DISS (Diameter Index the valve only to the extent recommended by the
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Pulmonary Resuscitators, Gas-Powered
manufacturer for effective cleaning. Keep parts volume of gas expelled over a given time period.
of a unit together and separate from other units The outlet flow with full depression of the resus-
by placing each disassembled unit in its own citator trigger should be 35 to 45 L/min. (The
mesh bag for machine cleaning and disinfection. AHA-recommended maximum flow rate is 40
After disinfecting, inspect the components for L/min; we allow ±5 L/min for measurement er-
signs of wear or damage. Confirm that the flap- ror.) If a unit fails this test, contact the manu-
per-valve device (present on some gas-powered facturer to determine if a flow-limit modification
resuscitators) that directs the gas flow is not torn is available.
or damaged. Carefully reassemble the valve, and
verify correct assembly. 2.5 Continuous Flow Rate. Using the flowmeter,
measure the flow of inhalator-type gas-powered
Valves that are disassembled for cleaning resuscitators that allow continuous oxygen flow
should also be disassembled during periodic in- to spontaneously breathing patients. On adjust-
spections to verify cleanliness, condition (as able units, check minimum, middle, and maxi-
above), and correct assembly. mum settings for accuracy (to ±20%).
1.25 Operation. Connect the resuscitator to a 50 psi 2.6 Demand Valve Function.
oxygen source capable of providing at least 100
L/min flow. A gas-powered resuscitator should CAUTION: Items 2.3 and 2.4 must be per-
fill a lung simulator of equivalent volume quickly formed before attempting the following test. Also,
and, upon releasing the trigger, should allow be certain that the unit has been properly cleaned
passive exhalation. If the resuscitator does not and disinfected.
fill quickly, verify that the gas source is not at When inspecting units incorporating demand
fault. Pressure regulators may not be capable of valves (a feature of some gas-powered resuscita-
providing adequate flow because of improper tors that supply a flow of oxygen in response to
calibration or varying tank pressures. Simi- the patient’s inspiratory effort in addition to
larly, a hospital oxygen wall outlet may provide manually triggered flow), inhale deeply from the
less than the necessary flow because of hidden mask or patient connector with the oxygen
line or outlet restrictions. turned on as well as turned off. With the oxygen
on, it should be possible to hear the flow through
2. Quantitative tests the demand valve upon inhalation. When inha-
2.3 Maximum Working Pressure. Connect the re- lation is complete, flow should cease and permit
suscitator outlet to a pressure gauge or meter. exhalation. When the oxygen is turned off (i.e.,
Fully depress the resuscitator’s trigger, and re- simulating an exhausted supply), it should be
cord the maximum pressure reading. (It may be possible to inhale room air through the valve. In
necessary to partially crimp the tubing between either case, minimal resistance should be felt
the resuscitator and a gauge to prevent pressure during inhalation.
oscillation.) Pressure should be 55 to 65 cm H2O.
If a unit fails to meet this criterion, return it to 3. Preventive maintenance
the manufacturer for repair. Some units tested Cleaning, disinfecting, and parts replacement are
with a low-compliance gauge attached directly to usually conducted by central service, the respiratory
the resuscitator may generate a pressure spike therapy department, or the user department after each
before pressure limiting occurs. Test these units use and thus should not be required during periodic
with a lung simulator (adult setting) to permit a inspections. Resuscitator operation should always be
more realistic delay time for pressure limiting to verified after processing.
occur.
4. Acceptance tests
2.4 Maximum Flow Rate. To determine the maxi-
mum flow rate, connect the resuscitator’s outlet Conduct major inspection tests for this procedure.
to a flowmeter with less than 10 cm H2O back
pressure at 100 L/min to the outlet (flowmeters Before returning to use
that produce higher back pressure will affect the Return inspected units to use in a clean, clear plastic
flow significantly). Alternatively, a gasometer or bag. Following major inspection in which contamina-
spirometer can be used along with a stopwatch tion may have occurred (e.g., Item 2.6), the unit should
or a watch with a second hand to measure the be submitted for processing just as after clinical use.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 422-0595
Pulmonary Resuscitators, Manual
Used For:
Resuscitators, Pulmonary, Manual, Reusable [17-591]
Also Called: Pulmonary resuscitators, manual resuscitators, bag resuscitators, bag-valve-mask units, Ambu
bags (Ambu is a registered trademark of Ambu of Denmark to be used only when referring to that device)
Commonly Used In: Critical care areas, recovery rooms, emergency rooms, patient care areas, ambulances
Scope: Applies to manually operated models; does not cover gas-powered resuscitators (use Pulmonary
Resuscitators, Gas-Powered Procedure/Checklist 448)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval* By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
*
These units should be routinely checked (see Items 1.1 and 1.25) following each use (after cleaning and
reassembly).
Overview Test apparatus and supplies
Pulmonary resuscitators are relatively simple devices, Pressure gauge or meter (0 to 60cm H2O)
yet ECRI frequently receives reports of failures that
Lung simulator
have led to unsuccessful resuscitations. The failures
we have investigated were caused by incorrect assem- Stopwatch or watch with a second hand
bly following cleaning or repair or by mechanical fail-
ure. Because these devices are frequently needed for 50 psi oxygen source with flowmeter for connection
lifesaving procedures, users have no time and may lack to resuscitator (for acceptance test only)
the expertise to troubleshoot, repair, and reassemble
units. Resuscitators must immediately function prop-
erly whenever they are needed.
Procedure
CAUTION: Inspect units only after appropriate
cleaning and disinfection.
Citations from Health Devices
Before beginning an inspection, carefully read this
Reprocessing and inspection of manual pulmonary re- procedure and the manufacturer’s instruction and serv-
suscitators [Hazard], 1987 Nov; 16:378-9. ice manuals; be sure that you understand how to oper-
ate the equipment and the significance of each control
Exhaled-air pulmonary resuscitators (EAPRs) and dis- and indicator. Also determine whether any special in-
posable manual pulmonary resuscitators (DMPRs) spection or preventive maintenance procedures or fre-
[Evaluation], 1989 Oct; 18:331-52. quencies are recommended by the manufacturer.
009082 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
422-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
1. Qualitative tests Use only transparent masks with resuscita-
tors. If the hospital has opaque masks, order
1.1 Housing/Bag. Examine the exterior of the unit transparent replacements, but do not remove
for cleanliness and general physical condition. opaque masks from use until the replacement
Be sure that plastic and metal housings are masks are in stock and the change has been
intact, that necessary assembly hardware is pre- discussed with users. Inspect masks and their
sent and fits tightly together, and that there are connectors for signs of deterioration (e.g., em-
no signs of spilled liquids or other serious abuse. brittlement). Reinflate collapsed inflatable rims,
and check for leaks or damage by immersing the
Inspect the resuscitator for overall physical mask in water. Replace if necessary.
condition. It should be clean and free of cracks or
other signs of damage. Carefully inspect resus- 1.24 Valve Assembly.
citator bags, especially while compressing them.
CAUTION: Before proceeding with this item,
There should be no tears, holes, or flaking; they
be certain you are familiar with the correct valve
should compress easily and not leak, reexpand
assembly. Misassembly will likely cause the re-
fully and quickly, and have no permanent set.
suscitator to fail, which may result in patient
Examine resuscitator components to verify death. Verify valve operation (Item 1.25) after
that there are no components from other similar reassembly.
model resuscitators. Even if components appear Disassemble the valve to the extent required
to be similar, they may not function like the for effective cleaning, and examine it for cleanli-
original components. For this reason, use only ness, condition, and correct assembly. Inspect
parts from the unit’s manufacturer. In addition, the components for signs of wear or damage.
the hospital should stock only one model each of Confirm that the valve device that directs the
manual and gas-powered resuscitators to pre- gas flow is not torn or damaged. Some resusci-
vent inadvertent mixing of components. tators have a separate valve assembly associated
Verify that the unit is placed in a sealed with their oxygen reservoir and/or air inlet. In-
plastic bag and that if the bag seal is broken, the spect this in the same manner. Reassemble the
unit is submitted for cleaning and reinspection. unit.
1.25 Operation. Compressing the bag should fill the
1.2 Mount. If the unit is attached to a wall or rests
lung simulator, and releasing the bag should
on a shelf, check the security of this attachment.
allow passive exhalation. By placing your hand
The unit should be available for immediate use.
in front of the exhalation port to feel the flow of
1.8 Tubes/Hoses. Check the condition of all tubing escaping gas, check that gas escapes from the
and hoses, especially at connectors. Be sure that exhalation port of the resuscitator and is not
they are not cracked, kinked, or dirty. retained in the compression bag. Test the inlet
valve by occluding the patient connector and
1.10 Fittings/Connectors. Examine all gas fittings squeezing the compression bag. No air should
and connectors for general condition. escape from the inlet valve.
1.22 Labeling. Check that all necessary placards, la- Operate the resuscitator connected to a lung
bels, conversion charts, and instruction cards simulator (with proper adult or pediatric set-
are present and legible. tings, if adjustable) to confirm proper opera-
tion of the resuscitator, particularly its valve
1.23 Accessories. Check all accessories stored with assembly.
the resuscitator. List the accessories that
should accompany each resuscitator, and check 2. Quantitative tests
them against the list at each inspection. Exam-
2.3 Cycling Rate. Connect the resuscitator to a lung
ine all accessories for cleanliness and mechani-
simulator of equivalent volume, and compress it
cal integrity.
fully with one hand as rapidly as possible for 1
Transparent face masks. An assortment of mask min while counting the number of cycles. Record
sizes (i.e., adult, infant) should be stored with the maximum cycling rate. A rate of less than
the resuscitator to allow its use with a wide 50/min for adult models or 70/min for infant
range of patients. models, while higher than that used during
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Pulmonary Resuscitators, Manual
resuscitation efforts, indicates deterioration of therapy department, or the user department after each
the compression bag or a malfunctioning inlet use and thus should not be required during periodic
valve. Check the valve for proper assembly, inspections. Resuscitator operation should always be
adequate cleaning, or any damage. After check- verified after processing.
ing the valve, retest the cycling rate. If still
unacceptable, replace the compression bag and 4. Acceptance tests
verify proper operation.
Occlude the oxygen inlet connector with your Conduct major inspection tests for this procedure.
finger, and verify that room air is admitted and In addition, perform the following test.
that there is no impediment to cycling rate or
4.1 Cycling rate with High O2 Flow. In addition to
ease of bag compression.
performing the tests in Item 2.3, verify that the
2.4 Maximum Pressure. Some units (e.g., Ambu, cycling rate is not affected by high oxygen flow
Hope) have pressure-relief mechanisms or pop- rates. Connect a source of oxygen to the oxygen
off valves. To determine the actual operating inlet (if provided), set the flowmeter to its maxi-
pressure of a pressure-relief mechanism, con- mum (flush) rate, and cycle the resuscitator into
nect the patient outlet of the nonrebreathing the lung simulator with various combinations of
valve to a pressure gauge or meter, and record small, medium, or large compressions and slow,
the maximum pressure that activates the relief average, or fast cycling rates. The nonrebreath-
mechanism as you fully compress the bag. ing valve should not jam, the maximum cycling
Check the reading against the manufacturer’s rate should not be significantly reduced, and
specifications. The mechanism should activate excess oxygen should be vented to the atmos-
at from 50 to 60 cm H2O for adult bags. (The phere. Carefully check models that have a valve
specification for some models may be as low as assembly associated with an oxygen reservoir
45 cm H2O.) bag.
3. Preventive maintenance
Before returning to use
Cleaning, disinfecting, and parts replacement are
usually conducted by central service, the respiratory Resubmit unit for normal cleaning and processing.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 451-0595
Pulse Oximeters
Used For:
Oximeters, Pulse [17-148]
Also Called: Oximeters, ear oximeters, finger oximeters, oxygen saturation monitors, O2 sat monitors
Commonly Used In: All patient care areas, including emergency vehicles; most commonly used in operating
rooms, recovery rooms, critical care units, NICUs
Scope: Applies to stand-alone pulse oximeters and to pulse oximeter modules built into patient monitoring
systems, anesthesia machines, or ventilators, as well as to devices that combine pulse oximeters with other
devices (e.g., capnometers) to serve as multiple-purpose respiration monitors (for capnometers and multiple
medical gas monitors; see Procedure/Checklist 450)
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview The two wavelengths of light (red and infrared) used
by the pulse oximeter are differentially absorbed by
Through continuous, noninvasive monitoring, pulse oxygenated hemoglobin (O2Hb) and deoxygenated he-
oximetry provides rapid indication of a patient’s moglobin (HHb). The absorption characteristics of
changing level of oxygenation, before significant hy- O2Hb and HHb differ markedly at the red wavelength
poxia occurs. Pulse oximeters are very easy to under- and are more similar at the infrared wavelength.
stand and use, and have reduced the frequency of Based on the relative absorption of the two wavelengths
arterial blood analysis, thereby eliminating many in the measurement site, the pulse oximeter deter-
costly procedures. mines the relative amount of oxygenated and deoxygen-
ated hemoglobin and displays the calculated spO2.
Pulse oximeters use the principle of differential
light absorption to determine the percent oxygen satu-
ration of hemoglobin in arterial blood (spO2; this value Pulse oximeters also display pulse rate and some
is referred to as saO2 when determined from an arterial indication of the amplitude or quality of the pulse
blood sample). Two different wavelengths of light are signal. This is usually in the form of a flashing LED
transmitted from a probe through a pulsating arterial or a bar-graph display, which changes with each pulse,
bed, usually in the fingertip or earlobe. Both dispos- or a plethysmogram waveform that corresponds to the
able (single use) and reusable probes are available; patient’s pulse waveform. The plethysmogram wave-
some attach to the ear, nose, or toe of adults and the form is typically generated from the signal received
hand or foot of infants. Probes that are based on (after processing) from the infrared LED. Pulse oxime-
reflectance (rather than transmittance) are also avail- ters also have alarms for high and low spO2 and pulse
able and typically attach to the forehead. rate and for probe disconnections.
084826 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
451-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Some pulse oximeter manufacturers sell pulse and indicator, and the alarm capabilities. Also deter-
waveform simulators for approximately $500 that at- mine whether any special inspection or preventive
tach to the unit to verify internal calibration. These maintenance procedures or frequencies are recom-
simulators input signals that correspond to one or mended by the manufacturer.
more specific spO2 and pulse rate values.
1. Qualitative tests
Other pulse oximeter test devices are available for
approximately $3,500 that simulate spO2 and pulse 1.1 Chassis/Housing. Examine the exterior of the
rate. These devices can be used to verify proper opera- unit for cleanliness and general physical condi-
tion and dynamic performance of various model pulse tion. Be sure that plastic housings are intact,
oximeters and probes. One simulator produces various that all hardware is present and tight, and that
spO2 and pulse rate values at several different signal there are no signs of spilled liquids or other
strengths, which are intended to simulate conditions serious abuse.
such as weak pulse or motion artifact. Pulse oximeters 1.2 Mount/Fasteners. If the device is mounted on a
and probes cannot be tested independently with this stand or cart, examine the condition of the
unit. Another simulator has independent inputs for the mount. If it is attached to a wall or rests on a
pulse oximeter and probe and is used to independently shelf, check the security of this attachment.
verify internal calibration of the oximeter and probe.
Signals are input to the pulse oximeter that correspond 1.4 AC Plug/Receptacles. Examine the AC power
to various spO2 and pulse rate values and waveforms. plug for damage. Attempt to wiggle the blades to
Parameters such as LED outputs are analyzed from the check that they are secure. Shake the plug and
probe. Simulators do not test the clinical accuracy of listen for rattles that could indicate loose screws.
pulse oximeters, since the signals generated by the If any damage is suspected, open the plug and
simulators are based on pulse oximeter specifications inspect it.
and are not true simulations of patient conditions.
If the device has electrical receptacles for ac-
Although simulators provide added convenience when
cessories, verify presence of line power; insert an
performing this inspection procedure, they are expen-
AC plug into each and check that it is held firmly.
sive and are not required for this procedure.
If accessories are plugged and unplugged often,
consider a full inspection of the receptacles.
Citations from Health Devices
Using an oxygen monitor with a pulse oximeter during 1.5 Line Cord. Inspect the cord for signs of damage.
anesthesia [User Experience NetworkTM], 1986 Sep- If damaged, replace the entire cord or, if the
Oct; 15:294-5. damage is near one end, cut out the defective
portion. Be sure to wire a new power cord or plug
Pulse oximeter interference from surgical lighting with the correct polarity. Also check the line
[Hazard], 1987 Feb; 16:50-1. cords of battery chargers.
Ambient light interference with pulse oximeters [User 1.6 Strain Reliefs. Examine the strain reliefs at
Experience NetworkTM], 1987 Sep-Oct; 16:346-7. both ends of the line cord. Be sure that they hold
the cord securely. If the line cord is detachable
Pulse oximeters [Evaluation], 1989 Jun; 18:184-230.
(by the user), we recommend that the cord be
affixed to the unit so that it cannot be removed
Test apparatus and supplies by the operator. (See Health Devices 1993 May-
Ground resistance ohmmeter Jun; 22:301-3.)
Leakage current meter or electrical safety analyzer
1.7 Circuit Breaker/Fuse. If the device has a
Pulse waveform simulator (if available from the switch-type circuit breaker, check that it moves
manufacturer) freely. If the device is protected by an external
spO2 and pulse rate simulator (optional) fuse, check its value and type against that
marked on the chassis and ensure that a spare
Procedure is provided.
Before beginning an inspection, carefully read this 1.9 Cables. Inspect any cables (e.g., probe) and their
procedure and the manufacturer’s instruction and strain reliefs for general condition. Carefully ex-
service manuals; be sure that you understand how to amine cables to detect breaks in the insulation and
operate the equipment, the significance of each control to ensure that they are gripped securely in the
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Pulse Oximeters
connectors at each end to prevent rotation or other 1.18 Indicators/Displays. During the course of the
strain. Verify that there are no intermittent faults inspection, confirm the operation of all lights,
by flexing cables near each end and looking for indicators, and visual displays on the unit and
erratic operation or by using an ohmmeter. charger, if so equipped. Be sure that all segments
of a digital display function properly. Observe a
1.10 Connectors. Examine all electrical cable connec- signal on a CRT display and check its quality
tors for general condition. Electrical contact pins or (e.g., distortion, focus, 60 Hz noise). Verify the
surfaces should be straight, clean, and bright. Ver- function of integral or accessory printers and the
ify that probe cable connectors are firmly gripped in quality of any output. Also verify that the unit
their appropriate connectors. If keyed connectors can be set to produce an audible tone with each
are used, make sure that the keying is correct. detected pulse, if so equipped.
1.11 Probes. If disposable probes are used, confirm Connect the pulse oximeter probe to your fin-
that an adequate supply is available. Check the ger or earlobe (whichever is appropriate) or to a
integrity of all reusable probes (see also Item simulator, and verify that a reasonable spO2 and
1.9). Confirm that any necessary electrodes pulse rate are displayed. The spO2 for a healthy
and/or transducers (e.g., for multigas monitors) adult should fall between 95% and 100%. If a
are on hand and check their physical condition. simulator is used, test at several spO2 and pulse
rate values, if available. The displayed pulse rate
1.13 Controls/Switches. Before changing any con-
should correspond to your manually palpated
trols or alarm limits, check their positions. If
pulse (within 10%). If a plethysmogram wave-
any settings appear inordinate (e.g., alarm lim-
form is displayed, confirm that the signal corre-
its at the ends of their range), consider the pos-
sponds to waveforms displayed in the operator’s
sibility of inappropriate clinical use or of
manual and that no excessive noise is present.
incipient device failure. Record the settings of
If a pulse waveform simulator is available, verify
those controls that should be returned to their
that the oximeter displays appropriate SpO2 and
original positions following the inspection.
pulse rates when attached to it.
Examine all controls and switches for physical 1.20 Alarms. Attach a probe to your finger or earlobe
condition, secure mounting, and correct motion. or to a simulator, and set pulse rate and spO2 alarm
Check that control knobs have not slipped on limits so that visual and audible alarms are acti-
their shafts. Where a control should operate vated. Verify that the alarm occurs within 1% spO2
against fixed-limit stops, check for proper align- or 1 beat per minute of the setting. If the unit has
ment, as well as positive stopping. Check mem- an alarm-silence feature, check the method of reset
brane switches for membrane damage (e.g., from (e.g., manual or automatic) against the manufac-
fingernails, pens). During the course of the in- turer’s specifications. Remove the probe from your
spection, be sure to check that each control and finger and verify that a probe disconnect or similar
switch performs its proper function. alarm occurs.
1.17 Battery/Charger. Inspect the physical condi- 1.21 Audible Signals. Operate the device to activate
tion of batteries and battery connectors, if read- any audible signals. Confirm appropriate vol-
ily accessible. Check operation of ume, as well as the operation of a volume control,
battery-operated power-loss alarms, if so if so equipped. If audible alarms have been si-
equipped. Operate the unit on battery power for lenced or the volume set too low, alert clinical
several minutes to check that the battery is staff to the importance of keeping alarms at the
charged and can hold a charge. (The inspection appropriate level.
can be carried out on battery power to help
confirm adequate battery capacity.) Check bat- 1.22 Labeling. Check that all necessary placards, la-
tery condition by activating the battery test func- bels, conversion charts, and instruction cards
tion or measuring the output voltage. Check the are present and legible.
condition of the battery charger and, to the ex-
tent possible, confirm that it does, in fact, charge 2. Quantitative tests
the battery. Be sure that the battery is re- 2.1 Grounding Resistance. Using an ohmmeter,
charged or charging when the inspection is com- electrical safety analyzer, or multimeter with
plete. When it is necessary to replace a battery, good resolution of fractional ohms, measure and
label it with the date. record the resistance between the grounding pin
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
of the power cord and exposed (unpainted and 3. Preventive maintenance
not anodized) metal on the chassis. We recom-
3.1 Clean the exterior, if needed.
mend a maximum of 0.5 Ω. If the system is
modular or composed of separate components, 4. Acceptance tests
verify grounding of the mainframe and each mod-
ule or component. If the device is double insulated, Conduct major inspection tests for this procedure
grounding resistance need not be measured; indi- and the appropriate tests in the General Devices Pro-
cate “DI” instead of the ground resistance value. cedure/Checklist 438.
If the device has an accessory receptacle, Before returning to use
check its grounding to the main power cord. Make sure that all controls are set properly. Set
2.2 Leakage Current. Measure chassis leakage cur- alarms loud enough to alert personnel in the area in
rent to ground with the grounding conductor of which the device will be used. Other controls should
plug-connected equipment temporarily opened. be in their normal pre-use positions.
Operate the device in all normal modes, includ- Attach a Caution tag in a prominent position to alert
ing on, standby, and off, and record the maxi-
the user that control settings may have been changed.
mum leakage current.
Recharge battery-powered devices or equip with
Chassis leakage current to ground should not
fresh batteries if needed.
exceed 300 µA.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 419-0595
Radiant Warmers
Used For:
Warmers, Radiant, Adult [13-249]
Warmers, Radiant, Infant [13-250]
Warmers, Radiant, Infant, Stationary [17-956]
Warmers, Radiant, Infant, Transport [13-251]
Also Called: Infant warmers, Krieselman (a registered trademark to be used only when referring to that
device) warming beds, warming lamps
Commonly Used In: Nurseries, delivery rooms, recovery rooms, PACUs
Scope: Applies to infant or adult, bassinet- or freestanding-type overhead warmers
Risk Level: ECRI Recommended, High for Infant Warmers, Medium for Adult Warmers; Hospital Assess-
ment, for Adult Warmers, for Infant Warmers
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview Radiant warmers are available in four configura-
tions: freestanding, integral bassinet, detachable, and
Radiant warmers are designed to provide thermal wall or ceiling mounted. Freestanding units are de-
support for patients while permitting free access to the signed for mobility and provide continuous thermal
patient for treatment and nursing care. support for infants in conventional bassinets or during
Radiant warmers are typically overhead heating diagnostic or therapeutic treatment. The integral bas-
units consisting of a lamp, a skin temperature sensor, sinet unit provides a total system for continuous ther-
an automatic (servo) control unit, and visual and audi- mal support of a sick infant and may also act as a
ble alarms. Some warmers are used exclusively in the short-term resuscitation platform in the delivery suite
manual (nonservo) mode and generally include a heat- or operating room. The detachable unit is essentially
ing unit, a timer to limit the heating time, and an a freestanding warmer that can be mounted on an
alarm to prompt reassessment of the patient’s status. optional bassinet. For mobility, warmers are mounted
Most radiant warmers with an automatic mode allow on casters, which may be equipped with brakes. Wall-
the operator to select the manual mode, as well. mounted units are situated directly over a bassinet,
table, or bed; some are jointed to allow horizontal
Typical heating elements are quartz tubes or incan- movement from a center position, as well as for
descent lamps, which are broadband energy sources retractability.
that generate a significant amount of radiant energy in
the far infrared (IR) wavelength region (longer than ECRI does not recommend use of manually operated
three microns, to avoid damaging a patient’s retina and units except for short, closely monitored periods be-
cornea). The radiant output of the heating unit is also cause of the increased danger of overheating or under-
limited to prevent thermal damage to the patient’s skin. heating the patient.
009084 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
419-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Other problems with radiant warmers include fail- 1. Qualitative tests
ures within the unit. Mechanical failure of the heater
support mechanism or the heating source can put the 1.1 Chassis/Housing/Bassinet. Examine the exte-
patient in contact with a hot surface or material that rior for overall condition. Check that the tem-
has fallen onto the mattress. Electronic circuit failure perature control unit is clean, that all labels and
can result from metal particles falling onto a circuit markings are legible, and that no adhesive tape
board, failure of a solder run to a metal chassis sup- or tape residue is present. Remove any adhesive
port, and contaminated solder flux. In addition, fires tape, paper, or other combustibles attached to
can result from flammable objects (e.g., oxygen hoses, any potentially hot surface.
drapes) placed close to a radiant heat source, arcing in
1.2 Mount. If the device is mounted on a stand or
a laminated plastic canopy, or heat aging of wire insu-
cart, examine the condition of the mount. If it is
lation. Eliminating these hazards requires good pre-
attached to a wall or rests on a shelf, check the
purchase evaluation and selection of equipment,
security of the attachment. If the heater canopy
proper user training, and periodic inspection and pre-
is designed to rotate, test the security at the
ventive maintenance.
farthest points of travel and check for positive
stopping at fixed-stop points.
Citations from Health Devices
1.3 Casters/Brakes. If the device moves on casters,
Infant radiant warmers [Evaluation], 1984 May;
check their condition. Look for accumulations of
13:119-44.
lint and thread around the casters, and be sure
Heat loss from infants, 1984 May; 13:130-1. that they turn and swivel, as appropriate. Check
the operation of brakes and swivel locks, if so
Manual and automatic (skin) temperature control, equipped. Conductivity checks, where appropri-
1984 May; 13:138-40. ate, are usually done more efficiently as part of
a check of all equipment and furniture in an area
Plastic thermal blankets [Hazard], 1984 Aug; 13:261-3.
(see Procedure/Form 441, Conductive Furniture
Temperature probe jacks on Ohmeda infant radiant and Floors).
warmers [User Experience NetworkTM], 1990 Dec;
1.4 AC Plug/Receptacles. Examine the AC power
19:456.
plug for damage. Attempt to wiggle the blades to
determine that they are secure. Shake the plug
Test apparatus and supplies and listen for rattles that could indicate loose
Ground resistance ohmmeter screws. If any damage is suspected, open the
Leakage current meter or electrical safety analyzer plug and inspect it.
Patient probe simulator, capable of simulating a If the device has electrical receptacles for ac-
range of temperatures as well as open- and short- cessories, insert an AC plug into each and check
circuited probe conditions (for testing units with that it is held firmly. If accessories are plugged
patient-temperature probes) and unplugged often, consider a full inspection
of the receptacle.
Calibration thermometer, accurate to at least
±0.3°C over the range of at least 30° to 45°C 1.5 Line Cord. Inspect the cord for signs of damage.
Controlled-temperature water bath or cups of water If damaged, replace the entire cord or, if the
damage is near one end, cut out the defective
Wire or twist ties portion. Be sure to wire a new power cord or plug
with the same polarity as the old one. Also, check
Procedure line cords of battery chargers.
Before beginning the inspection, carefully read this 1.6 Strain Reliefs. Examine the strain reliefs at
procedure and the manufacturer’s instruction and both ends of the line cord. Be sure that they hold
service manuals; be sure you understand how to oper- the cord securely.
ate the equipment, the significance of each control and
indicator, and the alarm capabilities. Also determine 1.7 Circuit Breaker/Fuses. If the device has a
whether any special inspection or preventive mainte- switch-type circuit breaker, check that it moves
nance procedures or frequencies are recommended by freely. If the device is protected by an external
the manufacturer. fuse, check its value and type against that
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Radiant Warmers
marked on the chassis, and ensure that a spare associated with asbestos in medical devices.)
is provided. Clean any residue or dirt from reflectors, lenses,
and heating element. Operate the warmer to
1.9 Cables. Inspect the cables (e.g., sensor, elec-
verify that all sections of the heater operate.
trode, remote control) and their strain reliefs for
general condition. Examine cables carefully to 1.17 Battery/Charger. Inspect the physical condi-
detect breaks in the insulation and to ensure tion of the batteries and battery connectors, if so
that they are gripped securely in the connectors equipped. Operate the unit on battery power for
of each end to prevent rotation or other strain. several minutes to check that the battery is
charged and can hold a charge. Check the re-
1.10 Fittings/Connectors. Examine all pneumatic
maining battery capacity by activating the bat-
fittings and connectors, as well as all electrical
tery test function or measuring the output
cable connectors, for general condition. Electri-
voltage. For lead-acid batteries, measure the
cal contact pins or surfaces should be straight,
specific gravity. Check the condition of the bat-
clean, and bright.
tery charger and, to the extent possible, confirm
1.11 Probes. Carefully examine the unit’s patient that it does, in fact, charge the battery.
probes. If the hospital has more than one model
The unit can be operated on battery power
of radiant warmer, be sure that probes are prop-
during performance testing to ensure adequate
erly identified for use with the appropriate unit.
battery capacity. However, be sure that an alter-
Interchanging probes may result in hazardous
nate unit is available while the unit under test
operation. Replace probes that are cracked or
is being recharged. When it is necessary to re-
deteriorating.
place a battery, label it with the date.
1.13 Controls/Switches. Before moving any controls
and alarm limits, check their positions. If any of 1.18 Indicators/Displays. During the course of the
them appear inordinate (e.g., alarm limits at the inspection, confirm the operation of all lights,
ends of their range), consider the possibility of indicators, gauges, and visual displays on the
inappropriate clinical use or incipient device fail- unit and charger, if so equipped. Be sure that all
ure. Record the settings of those controls that segments of a digital display function.
should be returned to their original positions 1.19 Self-Test. Verify operation of the self-test func-
following the inspection. tion, if so equipped.
Examine all controls and switches for physical 1.20 Alarms. Operate the device in such a way as to
condition, secure mounting, and correct motion. activate each audible and visual alarm. Check
Where a control should operate against fixed- that any associated interlocks function. If the
limit stops, check for proper alignment, as well device has an alarm-silence feature, check the
as positive stopping. Check membrane switches method of reset (e.g., manual, automatic)
for membrane damage (e.g., from fingernails or against the manufacturer’s specifications. If the
pens). During the course of the inspection, be unit has alarms for open- and short-circuited
sure to check that each control and switch per- patient probes, check their operation by insert-
forms its proper function. ing open- and short-circuited probe plugs. Also
1.14 Heating Element. If the heating element is a check for a disconnected-probe alarm, and verify
replaceable lamp, check that it is the correct type that it operates.
and wattage. Verify that filters or metallized 1.21 Audible Signals. Operate the device to activate
lenses in front of the heating element are not any audible signals. Confirm appropriate vol-
cracked or scratched. The heating element can- ume, as well as the operation of a volume control.
opy or housing, as well as all shields and protec-
tive devices, should be adequately secured. 1.22 Labeling. It is essential that radiant warmers
Check all plastic mounting components in the include adequate placards warning of possible
heating element and canopy for heat deforma- patient burns and other injury that can result
tion. Check for asbestos or loose fiberglass par- from misuse of the equipment. If no such plac-
ticles that can fall on the patient when the ard exists, make one and prominently attach it
heating element or its shield is tapped or jarred. on the warmer. We suggest the following word-
(If asbestos is detected, contact ECRI or the ing: WARNING: UNATTENDED OR IM-
manufacturer for information on health risks PROPER USE OF THE WARMER CAN
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
OVERHEAT OR BURN THE PATIENT OR RE- Measure chassis leakage current with all ac-
SULT IN SIGNIFICANT WATER LOSS. cessories normally powered from the same line
CHECK PATIENT TEMPERATURE AT cord connected and turned on and off. This in-
LEAST EVERY 15 MIN. cludes other equipment that is plugged into the
primary device’s accessory receptacles, as well
1.23 Accessories. Inspect examination lights and as equipment plugged into a multiple-outlet
phototherapy lamps for proper size, ease of posi- strip (“Waber strip”) so that all are grounded
tioning, and general condition. Check oxygen through a single line or extension cord.
cylinders for adequate supply and appropriate
fittings. Check flowmeters for proper operation. Chassis leakage current should not exceed
Inspect resuscitators and aspirators using a 300 µA.
separate procedure if they were not tested after
2.10 Temperature Accuracy. This test checks the ac-
their last use.
curacy of the patient probe and temperature
1.24 Bassinet/Mattress. Examine the bassinet’s side readout, as well as the heater control circuit on
panels for general condition and warping, and warmers with an automatic mode.
check that they can be easily raised and lowered. Connect the probe simulator to the warmer
Check that hinges are clean and that panel and set it for 34° or 35°C. If the warmer displays
latches hold the panels securely. Suspect defec- patient probe temperature, record the indicated
tive latches if adhesive tape is being used to reading and the simulated (actual) temperature
secure the panels. on Item 2.10 of the form. Raise the control set-
If the mattress position is adjustable, check point temperature gradually, and record the
the ease of motion and security of the locking value at which the heater activates (as indicated
mechanism. Examine the mattress for cleanli- either by a Heater On light or by slight deflection
ness. If the unit is to be used in the presence of of a heater power meter). Now, lower the set-
flammable anesthetics, check that a conductive point temperature, and record the temperature
mattress cover is being used. setting at which the heater turns off. (On units
with proportional control of the heater power,
2. Quantitative tests the heater will turn off at virtually the same
temperature at which it activated.)
2.1 Grounding Resistance. Using an ohmmeter,
Repeat this procedure at a simulated probe
electrical safety analyzer, or multimeter with
temperature of 36°C, and enter these data on the
good resolution of fractional ohms, measure and
form. Then set the simulator to 39°C, and check
record the resistance between the grounding pin
the accuracy of the display (do not check controller
of the power cord and exposed (unpainted and
operation at this temperature). We have found
not anodized) metal on the chassis. Verify that
that the patient probe temperature is generally
various sections of the unit (e.g., control unit,
within 0.3°C of the actual value, and the activation
heater, canopy, bassinet, stand) are all
and deactivation points of the automatic control
grounded. We recommend a maximum of 0.5 Ω.
are well within 0.5°C of the probe temperature.
If the device has an accessory outlet, check its
grounding to the main power cord. Because the simulator tests only the circuitry
and not the probe itself, probe operation and
2.2 Leakage Current. Measure chassis and patient
accuracy must still be tested for at least one
probe leakage currents in all modes of operation.
temperature. A convenient method is to dip all
Chargers of battery-powered units should be at-
probes simultaneously into one body-tempera-
tached and plugged into line power. If the frame
ture water bath, allow them to equilibrate, and
and chassis of the unit is not grounded through the
successively plug each into the same pretested
power cord, ground them with a clip lead. Record
temperature unit or module. All probes should
the highest value of leakage and the operating
give the same temperature reading. However,
mode with which it is associated. Check the unit
some variation is normal because the water tem-
in the automatic and manual heating modes and
perature varies slightly with location in the bath
with the heater on and off. Also measure leakage
and because the water gradually cools with time.
with all accessories that plug into accessory outlets
on the warmer (e.g., examining lamps, pho- If a patient probe simulator is not available,
totherapy lamps) on and off. test indicator accuracy and controller switching
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Radiant Warmers
using cups of water at about 34°, 36°, and 39°C. the automatic mode, and set the control tem-
Tie the probe to the calibration thermometer perature to 37°C. Add small quantities of hot
(with wire or twist ties), and insert them into the water to the cup to raise its temperature, stirring
cup to obtain the actual and indicated readings. the water in the cup frequently. Record the tem-
perature at which the high-temperature alarm
2.11 Alarm Accuracy. Check the high- and low-tem- comes on. Be careful not to add too much hot
perature alarms with the unit set to 37°C. If an water at once, or you will overshoot the alarm
appropriate temperature probe simulator is temperature.
available, set it to 37°C and verify that the alarm
is activated as the simulated temperature is If the unit has a low-temperature alarm and
increased or decreased beyond the alarm limits. patient-temperature display, determine the
alarm point by first heating the probe until there
If a probe simulator is not available, use one is no alarm, and then removing it from the influ-
of the following methods to check the high- and ence of the heater and noting the temperature at
low-temperature alarms of warmers with auto- which the alarm comes on.
matic control.
If the unit has a low-temperature alarm but no
If the unit displays patient probe tempera- patient-temperature display, follow a procedure
ture, operate the warmer in the automatic mode similar to that described for the high-tempera-
with the control point set at 37°C. Place the ture alarm limit, but add cold water to the cup.
connected patient probe on the bassinet mat-
tress or similar surface. After the heater has Compare the high- and low-temperature
been on for a minute or two, raise the probe and alarm thresholds against the manufacturer’s
hold it close to the heater. Record the tempera- specifications. The thresholds may be fixed or
ture reading at which the high-temperature may vary with the control setting. In either case,
alarm activates. This technique will work only the measured values should agree with the
because the heater has some degree of thermal manufacturer’s specifications, typically ≤0.5°C.
inertia and continues to put out heat even after
the control unit cuts off power to it. However, if 3. Preventive maintenance
the probe is not held close enough to the heater, 3.1 Clean the exterior, including vents and cooling
this inertia will not be sufficient to raise the fans. Clean residue or dirt from reflectors,
probe temperature to the alarm point. Should lenses, and heating element.
this happen, move the probe out of the range of
the heater, and wait for it to cool off. Once the 3.3 Calibrate if needed.
heater comes back on for a minute or two, hold 3.4 Replace the battery if needed.
the probe closer to it than before, and record the
temperature at which the high-temperature 4. Acceptance tests
alarm comes on.
Conduct major inspection tests for this procedure
If the unit under test has no patient-tempera- and the appropriate tests in the General Devices Pro-
ture display, prepare a cup of water at about cedure/Checklist 438.
37°C, measured with the calibration thermome-
ter, with room in the cup to add more water. Before returning to use
Insert the patient probe in the cup, close to the Inappropriate use of radiant warmers can cause
thermometer (tie them together with wire or patient burns. Any inordinate control settings or fail-
twist ties, if necessary). Rest the cup on the ures observed during inspection that may indicate
mattress or hold it away from the heat, which- incorrect use of the warmer should be discussed with
ever is more convenient. Operate the warmer in appropriate clinical personnel.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist No. 472-0595
Radiographic Units, General-Purpose
Used For:
Radiographic Units, General-Purpose [13-271]
Also Called: General radiographic room, rad room
Commonly Used In: Radiology departments, remote clinics, physicians’ offices
Scope: Applies to general-purpose radiographic systems and associated components with ceiling-suspended
or integrated x-ray tube supports
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview control (AEC) to automatically terminate the exposure
when a sufficient x-ray intensity has reached the film
General-purpose radiographic table systems are used cassette.
to perform routine diagnostic x-ray procedures. Some
systems can be enhanced with optional modular com- The x-ray generator is usually three phase, high
ponents for fluoroscopy and linear tomography. A gen- frequency, or constant potential, depending on the
eral-purpose radiographic system consists of a table, a manufacturer. The x-ray tube has either a stationary
Bucky film tray and grid, an x-ray tube with housing or rotating anode and is housed in either an integrated
and suspension, and an x-ray generator. tubestand or an overhead tube suspension. Beam re-
strictors (collimators) are used to regulate the shape
The table consists of a rectangular steel or metal and size of the x-ray beam to cover only the area of
alloy pedestal base or an open frame that supports a diagnostic interest.
tabletop constructed of carbon fiber or plastic or wood
laminate. Tableside and footplate controls allow the
table to be raised or lowered for transferring patients Test apparatus and supplies
or accommodating different imaging procedures. Table
Electrical multimeter
movement is usually power assisted. Some tables can
be tilted without moving the patient. Most tables can Noninvasive kVp meter (compatible with the x-ray
also be equipped with handgrips, headrests, compres- generator being inspected)
sion bands, footrests, and other accessories necessary
Noninvasive timer (may be included with the kVp
during certain radiographic procedures.
meter)
The Bucky film tray and grid are located under the
Ionization chamber with electrometer or a combina-
tabletop. The grid is used to reduce scatter radiation.
tion exposure meter
Bucky systems are usually fully automatic and can
accommodate film cassettes up to 35 × 43 cm (14″ × 17″) Five filters of 10 cm × 10 cm × 1 mm Type 1100
in size. Most systems also include automatic exposure aluminum
241480 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
472-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Collimator alignment template marked in centime- is crucial because it generates data on the baseline
ters or inches performance of the device.
Large (35 cm × 43 cm or 14″ × 17″), medium (25 cm
1. Qualitative tests
× 30 cm or 10″ × 12″), and small (20 cm × 24 cm or
8″× 10″) format x-ray cassette and film 1.1 Chassis/Housing. Examine the exterior of all
equipment items (e.g., table, tube support, x-ray
Ten pieces of 30 cm × 30 cm × 2.5 cm plexiglass (or
generator console and equipment cabinets, up-
another patient-simulating material for testing the
right cassette holders) for cleanliness and gen-
AEC)
eral physical condition. Be sure that all
Densitometer hardware is present and tight and that there are
Oscilloscope (calibration only) no signs of spilled liquids, deep scratches, dents,
or other serious abuse. Check the mechanical
High-voltage divider (calibration only) operation of all moving parts on all items, includ-
ing the x-ray tube, x-ray tube support, collima-
Special precautions tor, tabletop, vertical table movement if
Wear a lead apron and thyroid shield, and maintain applicable, and upright cassette holders. Ensure
the greatest possible reasonable distance from the that all movements are smooth and easy, with
x-ray source and all scattering material during all no binding or undue resistance.
x-ray exposures. It should not be necessary to place 1.3 Brakes. Check the brake or locking device for
hands or fingers in the x-ray beam; if this is unavoid- each movement of the x-ray tube, x-ray tube
able, wear lead gloves. support, collimator, tabletop, upright cassette
Do not remove the high-voltage cables from the holders, etc. Ensure that all locks function prop-
wells with the power on. Ensure that high-voltage erly and hold securely.
cables are completely discharged by repeatedly touch- 1.6 Strain Reliefs. Examine the strain reliefs at both
ing the conductor to ground as soon as it is removed ends of all cables subjected to movement and
from the well. stress. Be sure that they hold the cord securely.
Wear rubber gloves or other appropriate protection 1.7 Circuit Breaker/Fuse. If the device has an exter-
when exposed to blood or other body fluids. nal circuit breaker, check that it is accessible (not
Allow adequate time between repeated exposures to blocked by cabinets, covered with clipboards, or
prevent overheating of the x-ray tube. out of reach because of the presence of tables,
counters, etc.) and operates freely.
Procedure 1.9 Cables. Inspect any cables (e.g., collimator ca-
Before beginning an inspection, carefully read this bles, high-voltage cables, exposed interconnect
procedure and the manufacturer’s instruction and cables) and their strain reliefs for general condi-
service manuals; ensure that you understand how to tion. Carefully examine cables to detect breaks in
operate the equipment, the significance of each control the insulation and to ensure that they are gripped
and indicator, and the alarm capabilities. Also deter- securely in the connectors at each end to prevent
mine whether any special inspection or preventive rotation or other strain. For cables other than
maintenance procedures or frequencies are recom- high-voltage cables, verify that there are no in-
mended by the manufacturer. termittent faults by flexing electrical cables near
each end and looking for erratic operation. Use
This procedure is intended to ensure adequate sys- an ohmmeter if a problem is suspected. High-
tem performance and maintenance. It should not be voltage cables should be removed from the wells
construed as providing full compliance with the re- (at the x-ray tube ends), cleaned, coated with
quirements of all governmental regulations and ac- high-voltage compound, reinserted, and tight-
creditation standards of professional associations. ened securely. The high-voltage transformer end
Such regulations and standards may include testing should not require routine inspection if the wells
beyond that provided below and may also require docu- are vertical and high-voltage oil is used.
mentation by a certified medical physicist.
1.10 Fittings/Connectors. Examine all electrical cable
For acceptance testing, we strongly recommend con- connectors for general condition. Electrical contact
tracting with a medical physicist. Acceptance testing pins or surfaces should be straight, clean, and
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Radiographic Units, General-Purpose
bright. If keyed connectors are used, make sure that exposure). Confirm appropriate volume. If audi-
no pins are missing and that keying is correct. ble alarms have been silenced or the volume set
too low, adjust the alarm volume to the appropri-
1.12 Filters. Check the condition of any air filters pre- ate level.
sent in the systems. Clean or replace as needed.
1.22 Labeling. Check that all necessary certification
1.13 Controls/Switches. Before changing any con- labels, warning labels, technique charts, and
trols or alarm limits, check their positions. If any instruction cards are present and legible.
settings appear inordinate (e.g., high mA set-
ting), consider the possibility of inappropriate 1.23 Accessories. Confirm the presence and condition
clinical use or of incipient device failure. Record of accessories (e.g., clamp-on devices such as
the setting of those controls that should be re- handgrips for the tabletop).
turned to their original positions following the
inspection. Examine all controls and switches 1.24 Positive Beam Limitation. On units provided
(x-ray initiation, collimation, technique selection, with positive beam limitation (automatic colli-
etc.) for physical condition, secure mounting, and mation), ensure proper operation by making vis-
correct motion. Check that control knobs, if pre- ual checks of the light field with different-size
sent, have not slipped on their shafts. Where a cassettes in the Bucky and with the orientation
control should operate against fixed-limit stops, of the cassettes changed. The light field should
check for proper alignment, as well as positive be limited to the size and orientation of the
stopping. During the course of the inspection, be cassettes.
sure to check that each control and switch per-
forms its proper function. Ensure that the fluoro- 2. Quantitative tests
scopic and radiographic exposure switches do not 2.1 Grounding Resistance. Using an ohmmeter or
stick, that continuous pressure is required to multimeter with good resolution of fractional
continue exposure, and that release of pressure ohms, measure and record the resistance be-
immediately terminates exposure. Ensure the tween common ground and exposed metal on the
proper operation of the two-position exposure unit. We recommend a maxium resistance of 0.5
switch (i.e., ensure that the x-ray exposure is not Ω. Handswitches and footswitches that are pow-
released with the first trigger only). ered from low voltages need not be grounded.
1.18 Indicators/Displays. During the inspection, Although confirmation of grounding integrity
confirm the operation of all lamps, indicators, provides reasonable assurance of safety, NFPA
meters, gauges, and visual displays on the unit. 99 calls for voltage measurements for installed
Examples of indicators and displays are tech- devices in the patient vicinity.* Using a voltme-
nique settings, exposure time, x-ray on, and field ter, measure and record the voltage between a
size indicators on the collimator. Inspect the reference grounding point (e.g., the grounding
source-to-image distance (SID) indicator. If a pin of an electrical receptacle or some other
tape measure is present, ensure that it operates known ground) and exposed (i.e., unpainted and
smoothly and is accurate. not anodized) metal on the chassis. A voltage
reading below 500 mV is acceptable for general
1.20 Alarms. Induce conditions to activate audible and care areas in existing construction.
visual alarms (for example, x-ray on). Check that
any associated interlocks (e.g., x-ray exposure is 2.2 Leakage Current. Chassis leakage current of
inhibited if the x-ray tube is not aligned with the permanently wired equipment cannot be readily
image receptor) function. If the unit has an alarm measured after installation is completed. Per-
silence feature, check the method of reset (e.g., manently wired appliances in the patient vicin-
manual or automatic) against the manufacturer’s ity should be tested before installation, while the
specifications. It may not be possible to check out equipment is temporarily insulated from
all alarms at this time since some may require ground. The leakage current from frame to
abnormal operating conditions (e.g., long exposure ground of permanently wired appliances in-
times). Instruct users to document activation of stalled in general or critical patient care areas
these alarms to ensure that they are functional. should not exceed 5 mA with all grounds lifted.
*Patient vicinity is defined as a space within six feet beyond the
1.21 Audible Signals. Operate the device to activate perimeter of the patient support in its normal location and extending
any audible signals (for example, radiographic seven-and-a-half feet above the floor.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
2.3 Accuracy of kVp. Perform this test on all x-ray should have a coefficient of variation no larger
tubes. Use a noninvasive kVp meter that has than 10%. For long-term reproducibility, simply
previously been calibrated against a high-volt- record the current average mR/mAs value from
age divider on the type of generator being tested. the four measurements above, and compare this
Use the kVp meter in accordance with the manu- with the value recorded during the preceding
facturer’s recommendations. These may include inspection. It is critical that identical test condi-
the kind of filters to use and the distance at which tions be used for assessing reproducibility. For
the kVp meter has to be placed. Some meters example, the same chamber-to-source distance
require that the user specify the type of generator should be used, and the technique (kVp, mAs)
being tested and the amount of filtration present should be the same. Long-term reproducibility
in the primary x-ray beam. Make measurements should be within ±10% of the average.
at low, medium, and high settings (e.g., 60, 80,
100 kVp). After the appropriate corrections have 2.7 Half-Value Layer (HVL). This test must be per-
been applied to the measured kVp readings (e.g., formed on all x-ray tubes. Use an ionization cham-
for filtration), the difference between the meas- ber, electrometer, and Type 1100 aluminum filters
ured kVp and the preset kVp should not exceed for this test. Place the ionization chamber in the
±5% of the preset kVp. center of the x-ray beam at about 100 cm from the
focal spot. Collimate so that the x-ray field just
2.4 Timer Accuracy. Use a noninvasive timer to encompasses the ionization chamber. Set the unit
measure the accuracy of the time settings. Most to operate at 80 kVp. Select a midrange mAs value.
noninvasive kVp meters also display exposure These kVp and mAs values should be held constant
times. Once the unit has been appropriately set during the whole course of this test. Record the
up, dial up a midrange kVp setting (e.g., 80 kVp). initial exposure value (in mR) with nothing in the
The x-ray unit may display in mAs; if this is the primary beam (i.e., 0 mm of aluminum). Then
case, calculate the time by factoring out the mA. record the exposure reading with aluminum thick-
Conduct measurements at typical low, medium, nesses of 2 mm and 4 mm. The thickness of alumi-
and high settings. The difference between the num required to reduce the initial exposure
measured time and the preset time should not reading by half is the half-value layer of the beam.
exceed ±1 msec or ±5%, whichever is greater. The HVL is most accurately read by plotting the
measurements on semilog graphing paper. Plot
2.5 Linearity of mAs. This test must be performed the exposure values on the logarithmic scale
on all x-ray tubes. Use an ionization chamber against the thickness of aluminum on the linear
with an electrometer (or a combination exposure scale. At 80 kVp, the HVL should be a minimum
meter) to measure the exposure in mR for this of 2.3 mm of aluminum. The HVL measurement
test. The ionization chamber should be placed should be compared to measurements from pre-
centrally in the x-ray beam at a known standard vious inspections since a change in HVL may indi-
distance from the focal spot (e.g., 100 cm). Dial cate tube deterioration.
up a midrange kVp setting (e.g., 80 kVp). Make
radiographic exposures at this fixed kVp, and 2.8 Collimation. This test must be performed on all
record the exposure values (in mR) from the collimators and all receptor sizes. Place a me-
electrometer or exposure meter at a minimum of dium-format x-ray film (25 cm × 30 cm or 10″ ×
three mA settings that span the range commonly 12″) at an SID of 100 cm (40″). Ensure that the
used. Use an exposure time that is in the mid- x-ray film is perpendicular to the x-ray beam.
range for each mA value. Calculate the mR/mAs Ensure that the x-ray tube is in the detent for
at each setting and average the calculations. alignment with the receptor or aligned using a
Each individual mR/mAs value should be within centering light if there is no detent. Precisely
±10% of the average. center the collimator alignment tool on the cas-
sette. Turn on the collimator light, and collimate
2.6 Exposure Reproducibility. Use one of the to an area of 20 cm × 20 cm. Note the exact
above mR/mAs values as the one value to be readout of the exposure area size indicators.
used for evaluating short-term and long-term Ensure that the light beam is exactly centered
reproducibility of the x-ray tube and generator on the collimator alignment tool. Record the
combination. For the short-term test, make a exact boundaries of the illuminated area from
minimum of four exposures at the same mAs the collimator alignment tool. Make an x-ray
over a span of 15 minutes. The mR/mAs values exposure (for a film/screen speed of 400, a tech-
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Radiographic Units, General-Purpose
″ ″
Figure 1. Collimation test setup
nique of 55 kVp and 5 mAs should be sufficient), 2.9 AEC Object Thickness Compensation. This test is
and process the x-ray film. to be conducted on each available radiographic
image receptor holder (e.g., spot film, table Bucky,
Congruence of the light field to the x-ray field.
wall Bucky). Place 20 cm of 30 cm × 30 cm
Measure the distances of L1, L2, W1, and W2
plexiglass on the table, or support it up against the
on the processed film. The sum of W1 + W2 +
wall Bucky. (It is acceptable to use another patient-
L1 + L2 is the total misalignment between the
simulating material for AEC tests, such as alumi-
light field and the x-ray field. This sum must
num.) Ensure that the plexiglass covers the AEC
not exceed 2% of the SID; that is, at an SID of
detectors. Set the unit to operate at 80 kVp (or
100 cm, the misalignment should not exceed
some other setting commonly used to image a
2 cm (see Figure 1).
medium-size patient). Load a cassette of a size
Alignment of the x-ray source to the receptor. commonly used with the standard film used at the
Mark the exact center of the exposed area on facility, and place this into the receptor holder
the film by drawing diagonals from corner to being tested. Then make an AEC-controlled expo-
corner of the exposed area. Mark the exact sure. Process the film on a processor that has
center of the film by drawing diagonals from previously been verified as operating optimally.
corner to corner of the film. Measure the dis- Use a densitometer to measure the optical density
tance between the two centers; this must not of the radiograph in the center of the image. If the
be more than 2% of the SID — that is, at an optical density falls within the range chosen by the
SID of 100 cm, the centers should be mis- radiologists (typically 1.2 to 1.4 OD), repeat the
aligned no more than 2 cm. Also, ensure that test using identical setup conditions but with vary-
the exposed area is square to the film. ing amounts of plexiglass in the beam. At a mini-
mum, check the optical density at 15 cm and 25 cm
Field size indicators versus actual exposed area. of plexiglass. All films used in this test should come
Measure the length and width of the exposed from the same batch, and only one cassette is to be
area on the exposed film. Compare the actual used for all exposures. The optical density of all the
size of the exposed area with the readout of processed films should agree to within ±0.3 OD of
the exposure area size indicators noted earlier. the optical density at 20 cm.
The dimensions of the exposed area must be
within 2% of the SID — that is, 2 cm at an SID 2.10 AEC kVp Compensation. This test should also
of 100 cm. be conducted on each available radiographic
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
image receptor holder (spot film, table Bucky, 3.2 Lubricate per the manufacturer’s instructions.
and wall Bucky). Place 20 cm of plexiglass (or
3.3 Calibrate the system to ensure performance
some other patient-simulating material) on
within the manufacturer’s specifications, at in-
the table, or support it up against the wall
tervals recommended by the manufacturer or as
Bucky. Ensure that the AEC detectors are
indicated by inspection results. Adjust all
covered by the plexiglass. Use the most com-
brakes, locks, and bearings to ensure proper
mon size of films in the same cassette holder
performance.
for all checks in this test. Make a series of
AEC-controlled exposures of the 20 cm of 3.4 Replace air filters, if needed.
plexiglass at different kVp values. At a mini-
mum, use three kVp settings (e.g., 60, 80, 100 4. Acceptance tests
kVp). For each exposure, process the film on Acceptance testing is typically performed by a medi-
an optimally performing processor. Read the cal physicist.
optical density of the radiograph using a den-
sitometer. The optical density of the films at Before returning to use
all kVp settings checked should agree to
Ensure that all controls are set properly. Set alarms
within ±0.3 OD.
loud enough to alert personnel in the area in which the
device will be used. Other controls should be in their
3. Preventive maintenance
normal pre-use positions. Attach a Caution tag in a
3.1 Clean the exterior and interior. Take precau- prominent position so that the user will be aware that
tions when dealing with body fluids. control settings may have been changed.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist No. 473-0595
Radiographic/Fluoroscopic Units,
General-Purpose
Used For:
Radiographic/Fluoroscopic Table Systems [16-885]
Also Called: Fluoro room, R/F room
Commonly Used In: Radiology, urology
Scope: Applies to radiographic/fluoroscopic table systems with a spot-film tower, an overhead radiographic
x-ray tube, and associated components
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 6 months months . hours
Overview a number of film images to be exposed on a single
cassette. Digital photospot cameras are available from
Radiographic/fluoroscopic (R/F) table systems are used a number of manufacturers; they are used to convert
for diagnostic radiographic and fluoroscopic examina- x-ray images to digital format for immediate viewing
tions — for example, gastrointestinal studies, and storage.
myelography, and studies that require the use of con-
trast media. R/F systems can be purchased in a variety X-ray tubes generally are located under the table for
of configurations. A typical R/F system includes a fluoroscopy and over the table for radiography. The
table, a spot-film device (SFD), an undertable and/or overtable tube requires an overhead tube support,
over-table x-ray tube and housing, an x-ray generator, which allows the tube to be parked out of the way when
an image intensifier, and a Bucky film tray and grid. not in use. The x-ray tube has a rotating anode to more
effectively dissipate heat. Different types of x-ray gen-
The table base contains a motor drive unit for tilting erators are usually available for use with the system;
the tabletop and provides support for the tabletop, the three-phase, high-frequency, and constant-potential
undertable x-ray tube, the SFD, and the image intensi- generators are most commonly used.
fier. Table models are generally described according to
their degree of positive/negative tilting capability, such The image intensifier is used to convert radiation to
as +90/-90, +90/-45, or +90/-15. The tabletop is con- light, which it then amplifies. A television camera tube
structed of carbon fiber or a laminate material. Head- converts the light image to an electron pattern, then to
rests, footrests, handgrips, harnesses, and other an electric current that varies in proportion to the
accessories for certain imaging procedures are available. different light intensities of the original image. The
electrical information is then converted for viewing on
The SFD usually accepts a variety of cassette sizes a TV monitor. Image intensifiers are described in terms
and is capable of variable film formatting, which allows of their input phosphor diameter — for example, 9″ or
241481 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
473-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
12″. Different sizes are used, depending on the procedure sheet of 1.0 mm aluminum, with two sets of four
and field of view required. Some vendors offer dual, holes of the following sizes: 1/16″, 1/8″, 3/16″, and
triple, or quad mode image intensifiers. The image inten- 1/4″ (1.0, 3.0, 5.0, and 7.0 mm) (use of an alternative
sifier is mounted over the table in conventional table low-contrast phantom is acceptable, provided that
systems, and under the table in remote table systems. it can be reproducibly used for assessment of long-
term performance; use the criterion applicable to
The Bucky film tray and grid are located under the
the phantom selected)
tabletop. The grid is used to reduce scatter radiation.
Bucky systems are usually fully automatic and can Oscilloscope (calibration only)
accommodate film cassettes up to 35 cm × 43 cm (14″ High-voltage divider (calibration only)
× 17″) in size. Most systems also include automatic
exposure control (AEC) to automatically terminate the
exposure when a sufficient x-ray intensity has reached Special precautions
the film cassette. Wear a lead apron and thyroid shield and maintain
Function controls can be located on the SFD console, the greatest possible reasonable distance from the
at tableside, or in a remote location. Controls include x-ray source and all scattering material during all
x-ray exposure, cassette positioning and reloading, x-ray exposures. It should not be necessary to place
film format selection, rapid exposures, image intensi- hands or fingers in the x-ray beam; if this unavoidable,
fier mode selection, and table tilt. wear lead gloves.
Do not remove the high-voltage cables from the
Test apparatus and supplies wells with power on. Ensure that high-voltage cables
Electrical multimeter are completely discharged by repeatedly touching the
Noninvasive kVp meter (compatible with the x-ray conductor to ground as soon as they are removed from
generator being inspected) the well.
Noninvasive timer (may be included with the kVp Wear rubber gloves or other appropriate protection
meter) when exposed to blood or other body fluids.
Ionization chamber with electrometer or a combina-
Allow adequate time between repeated exposures to
tion exposure meter
prevent overheating of the x-ray tube.
Five filters of 10 cm × 10 cm × 1 mm Type 1100
aluminum Procedure
Collimator alignment template marked in centime-
ters or inches Before beginning an inspection, carefully read this
procedure and the manufacturer’s instruction and
Ruler with leaded 1 cm or 1/2″ marker service manuals; ensure that you understand how to
Ten pieces of 30 cm × 30 cm × 2.5 cm plexiglass (or operate the equipment, the significance of each control
another patient-simulating material for testing the and indicator, and the alarm capabilities. Also deter-
automatic exposure control) mine whether any special inspection or preventive
maintenance procedures or frequencies are recom-
Densitometer
mended by the manufacturer.
Large (35 cm × 43 cm or 14″ × 17″), medium (25 cm
× 30 cm or 10″ × 12″), and small (20 cm × 24 cm or This procedure is intended to ensure adequate sys-
8″ × 10″) format x-ray cassettes and films tem performance and maintenance. It should not be
construed as providing full compliance with the re-
Six pieces of 30 cm × 30 cm × 1 mm lead
quirements of all governmental regulations and ac-
A medium-size box approximately 12″ × 12″ × 12″ or creditation standards of professional associations.
plastic bucket approximately 12″ to 14″ high (this Such regulations and standards may include testing
will be used to support a film cassette and image beyond that provided below and may also require docu-
quality phantoms below the spot film tower) mentation by a certified medical physicist.
High-contrast resolution line-pair phantom to 5 lp/ For acceptance testing, we strongly recommend con-
mm minimum tracting with a medical physicist. Acceptance testing
Low-contrast phantom consisting of two 3/4″ (2 cm) is crucial because it generates data on baseline per-
aluminum plates, 7″ × 7″ (18 cm × 18 cm), and one formance of the device.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Radiographic/Fluoroscopic Units, General-Purpose
1. Qualitative tests 1.12 Filters. Check the condition of any air filters pre-
sent in the systems. Clean or replace if needed.
1.1 Chassis/Housing. Examine the exterior of all
1.13 Controls/Switches. Before changing any controls
equipment items (e.g., table, tube support, x-ray
or alarm limits, check their positions. If any set-
generator console and equipment cabinets, up-
tings appear inordinate (e.g., high mA setting),
right cassette holders) for cleanliness and general
consider the possibility of inappropriate clinical
physical condition. Be sure that all hardware is
use or of incipient device failure. Record the setting
present and tight and that there are no signs of
of those controls that should be returned to their
spilled liquids, deep scratches, dents, or other
original positions following the inspection.
serious abuse. Check the mechanical operation of
all moving parts on all items, including the x-ray Examine all controls and switches (i.e., x-ray
tube, x-ray tube support, collimator, tabletop, initiation, collimation, technique selection, etc.)
table tilt, spot-film tower, and upright cassette for physical condition, secure mounting, and cor-
holders. Ensure that all movements are smooth rect motion. Check that control knobs, if present,
and easy, with no binding or undue resistance. have not slipped on their shafts. Where a control
should operate against fixed-limit stops, check for
1.3 Brakes. Check the brake or locking device for proper alignment, as well as positive stopping. Be
each movement of the x-ray tube, x-ray tube sure to check that each control and switch per-
support, collimator, tabletop, spot-film tower, forms its proper function. Ensure that the fluoro-
upright cassette holders, etc. Ensure that all scopic and radiographic exposure switches do not
locks function properly and hold securely. stick, that continuous pressure is required to
continue exposure, and that release of pressure
1.6 Strain Reliefs. Examine the strain reliefs at both
immediately terminates exposure. Ensure the
ends of all cables subjected to movement and
proper operation of the two-position exposure
stress. Be sure that they hold the cord securely.
switch (i.e., that the x-ray exposure is not re-
1.7 Circuit Breaker/Fuse. If the device has an ex- leased with the first trigger only).
ternal circuit breaker, check that it is accessible 1.18 Indicators/Displays. Confirm the operation of all
(i.e., not blocked by cabinets, covered with clip- lamps, indicators, meters, gauges, and visual dis-
boards, out of reach behind tables, counters, etc.) plays on the unit. Examples of indicators and
and operates freely. displays are technique settings, exposure time,
x-ray on, field size indicators on the collimator,
1.9 Cables. Inspect any cables (e.g., collimator ca-
cassette size, and format selection on the spot-film
bles, high-voltage cables, exposed interconnect
tower. Inspect the source-to-image (SID) indicator
cables) and their strain reliefs for general condi-
for the overtable tube. If a tape measure is present,
tion. Carefully examine cables to detect breaks
ensure that it operates smoothly and is accurate.
in the insulation and to ensure that they are
gripped securely in the connectors at each end to 1.20 Alarms. Induce conditions to activate audible
prevent rotation or other strain. For cables other and visual alarms (e.g., five-minute fluoroscopic
than high-voltage cables, verify that there are no alarm, no cassette in Bucky). Check that any
intermittent faults by flexing the cables near associated interlocks (e.g., x-ray exposure is in-
each end and looking for erratic operation. Use hibited if x-ray tube is not aligned with image
an ohmmeter if a problem is suspected. High- receptor) function. If the unit has an alarm si-
voltage cables should be removed from the wells lence feature, check the method of reset (e.g.,
(at the x-ray tube end), cleaned, coated with manual, automatic) against the manufacturer’s
high-voltage compound, reinserted, and tight- specifications. It may not be possible to check out
ened securely. The high-voltage transformer end all alarms at this time, since some may require
should not require routine inspection if the wells abnormal operating conditions (e.g., long expo-
are vertical and high-voltage oil is used. sure times). Instruct users to document activa-
tion of these alarms to ensure that they are
1.10 Fittings/Connectors. Examine all electrical cable functional.
connectors for general condition. Electrical contact
pins or surfaces should be straight, clean, and 1.21 Audible Signals. Operate the device to activate
bright. If keyed connectors are used, make sure any audible signals (e.g., radiographic exposure).
that no pins are missing and that keying is correct. Confirm appropriate volume. If audible signals
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
have been silenced or the volume set too low, divider on the type of generator being tested. Use
adjust alarm volume to the appropriate level. the kVp meter in accordance with the manufac-
turer’s recommendations. These may include the
1.22 Labeling. Check that all necessary certification kind of filters to use and the distance at which
labels, warning labels, technique charts, and the kVp meter must be placed. Some meters
instruction cards are present and legible. require that the user specify the type of gener-
1.23 Accessories. Confirm the presence and condition ator being tested and the amount of filtration
of accessories (e.g., handgrips, footrests, straps). present in the primary x-ray beam. Make meas-
urements at low, medium, and high kVp settings
1.24 Positive Beam Limitation. On units provided (e.g., 60, 80, 100 kVp). After the appropriate
with positive beam limitation (automatic collima- corrections have been applied to the measured
tion), ensure proper operation by making visual kVp readings (e.g., for filtration), the difference
checks of the light field with different-sized cas- between the measured kVp and the preset kVp
settes in the Bucky and with the orientation of the should, as a general rule, not exceed ±5% of the
cassettes changed. The light field should be limited preset kVp.
to the size and orientation of the cassettes.
2.4 Timer Accuracy. Use a noninvasive timer to
2. Quantitative tests measure the accuracy of the time settings. Most
noninvasive kVp meters also display exposure
2.1 Grounding Resistance. Using an ohmmeter times. Once the unit has been appropriately set
with good resolution of fractional ohms, measure up, dial up a midrange kVp setting (e.g., 80 kVp).
and record the resistance between common The x-ray unit may display in mAs; if so, calcu-
ground and exposed metal on the unit. We rec- late the time by factoring out the mA. Conduct
ommend a maximum resistance of 0.5 Ω. Hand- measurements at typically used low, medium,
switches and footswitches powered from low and high settings. The difference between the
voltages need not be grounded. Although confir- measured time and the preset time should not
mation of grounding integrity provides reason- exceed ±1 ms or ±5%, whichever is greater.
able assurance of safety, NFPA 99 calls for
voltage measurements for installed devices in 2.5 Linearity of mAs. This test should be performed
the patient vicinity.* Using a voltmeter, measure on all x-ray tubes. Use an ionization chamber
and record the voltage between a reference with an electrometer (or a combination exposure
grounding point (e.g., the grounding pin of an meter) to measure the exposure in mR for this
electrical receptacle, some other known ground) test. The ionization chamber should be placed
and exposed (i.e., unpainted and not anodized) centrally in the x-ray beam at a known standard
metal on the chassis. A voltage reading below distance from the focal spot (e.g., 100 cm).
500 mV is acceptable for general care areas in
Dial up a midrange kVp setting (e.g., 80 kVp).
existing construction.
Make radiographic exposures at this fixed kVp,
2.2 Leakage Current. Chassis leakage current of and record the exposure values (in mR) from the
permanently wired equipment cannot be readily electrometer or exposure meter at a minimum of
measured after installation is completed. Per- three mA settings that span the range commonly
manently wired appliances in the patient vicin- used. Use an exposure time that is in the mid-
ity should be tested before installation, while the range for each mA value. Calculate the mR/mAs
equipment is temporarily insulated from at each setting, and average the calculations.
ground. The leakage current from frame to Each individual mR/mAs value should be within
ground of permanently wired appliances in- ±10% of the average.
stalled in general or critical patient care areas
2.6 Exposure Reproducibility. Use one of the above
should not exceed 5 mA with all grounds lifted.
mR/mAs values as the one value to be used for
2.3 Accuracy of kVp. Perform this test on all x-ray evaluating short-term and long-term reproduci-
tubes for both radiographic and fluoroscopic bility of the x-ray tube and generator combina-
modes. Use a noninvasive kVp meter that has tion. For the short-term test, make a minimum
previously been calibrated against a high-voltage of four exposures at the same mAs over a span of
15 minutes. The mR/mAs values should have a
* Patient vicinity is defined as a space within six feet of the perimeter
of the patient support in its normal location and extending seven coefficient of variation no larger than 10%. For
and one-half feet above the floor. long-term reproducibility, simply record the
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Radiographic/Fluoroscopic Units, General-Purpose
current average mR/mAs value from the four vious inspections, since a change in HVL may
measurements above and compare this with the indicate tube deterioration.
value recorded during the preceding inspection.
It is critical that identical test conditions be used 2.8 Collimation. This test must be performed on all
for assessing reproducibility. For example, the collimators and all receptor sizes.
same chamber-to-source distance should be used Radiographic X-ray Tubes (overhead tubes).
and the technique (kVp, mAs) should be the
same. Long-term reproducibility should be Place a medium-format x-ray film (25 cm × 30
within ±10% of the average. cm or 10″ × 12″) at an SID of 100 cm (40). Ensure
that the x-ray film is perpendicular to the x-ray
2.7 Half-Value Layer (HVL). Perform this test on all
beam. Ensure that the x-ray tube is in the detent
x-ray tubes. Use an ionization chamber, elec-
for alignment with the receptor or aligned using
trometer, and Type 1100 aluminum filters for
a centering light if there is no detent. Precisely
this test. Place the ionization chamber in the
center the collimator alignment tool on the cas-
center of the x-ray beam at about 100 cm from
sette. Turn on the collimator light, and collimate
the focal spot. Collimate so that the x-ray field
to an area of 20 cm × 20 cm. Note the exact
just encompasses the ionization chamber. Set
readout of the exposure area size indicators.
the unit to operate at 80 kVp. Select a midrange
Ensure that the light beam is exactly centered
mAs value. These kVp and mAs values should be
on the collimator alignment tool. Record the
held constant throughout this test. Record the
exact boundaries of the illuminated area from
initial exposure value (in mR) with nothing in
the collimator alignment tool. Make an x-ray
the primary beam (i.e., 0 mm of aluminum).
exposure (for a film/screen speed of 400, a tech-
Record the exposure reading with aluminum
nique of 55 kVp and 10 mAs should be sufficient),
thicknesses of 2 mm and 4 mm. The thickness of
and process the x-ray film.
aluminum required to reduce the initial expo-
sure reading by half is the HVL of the beam. The Congruence of the light field to the x-ray
HVL is most accurately read by plotting the field. Measure the distance L1, L2, W1, and
measurements on semilog graphing paper. Plot W2 on the processed film. The sum of W1 + W2
the exposure values on the logarithmic scale + L1 + L2 is the total misalignment between
against the thickness of aluminum on the linear the light field and the x-ray field. This sum
scale. At 80 kVp, the HVL should be a minimum must not exceed 2% of the SID; that is, at an
of 2.3 mm of aluminum. Compare the HVL SID of 100 cm, the misalignment should not
measurement with measurements from pre- exceed 2 cm. See Figure 1.
″ ″
Figure 1. Schematic showing misalignment of the light field with respect to the x-ray field
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
Alignment of the x-ray source to the receptor. To park position. Select a 4 on 1 format. While
evaluate the alignment of the x-ray source to performing fluoroscopy, using the appropriate
the film receptor, mark the exact center of the mode on the image intensifier, measure the
exposed area on the film by drawing diagonals visual field size (length and width). The fluoro
from corner to corner of the exposed area. image should be square, limited by the 4 on 1
Mark the exact center of the film by drawing mask. Make a spot-film exposure (for a
diagonals from corner to corner of the film. film/screen speed of 400, a technique of 55 kVp
Measure the distance between the two cen- and 10 mAs should be sufficient if photo tim-
ters; this must not be more than 2% of the SID. ing is not available or results in film that is
At an SID of 100 cm, the centers should be too dark). After the film has been processed,
misaligned no more than 2 cm. For this test, ensure that the dimensions of the x-ray beam
also ensure that the exposed area is square to measured on the film do not differ from the
the film. dimensions of the fluoroscopic image meas-
Field size indicators versus actual exposed area. ured with the lead ruler by more than 3% of
Measure the length and width of the exposed the SID to the spot film.
area on the exposed film. Compare the actual Alignment of source to receptor. Place a medium-
size of the exposed area to the readout of the format x-ray film (25 cm × 30 cm or 10″ × 12″)
exposure area size indicators noted earlier. in the spot-film tower, and place the film in the
The dimensions of the exposed area must be park position. Collimate to an area of approxi-
within 2% of the SID (that is, 2 cm at an SID mately 10 cm × 10 cm (an area small enough
of 100 cm). that you can visualize the entire edge of the
Fluoroscopic X-ray Tubes (undertable tubes). collimator blades). Ensure that the system is
in the mode of operation that will allow the
Collimation to the image intensifier during fluo-
collimator blades to remain as positioned un-
roscopy. Place the box or plastic bucket (up-
der fluoroscopy and that a 1 on 1 format is
side down) on the tabletop below the spot-film
selected. Make a spot-film exposure (for a
tower. Place a ruler with leaded 1 cm or 1/2″
film/screen speed of 400, a technique of 55 kVp
markers on top of the box, and lower the
and 10 mAs should be sufficient if photo timing
spot-film tower until the underside comes in
is not available or results in film that is too
contact with the ruler. While performing fluo-
dark), and process the film. Mark the exact
roscopy, using the largest available mode on the
center of the exposed area on the film by
image intensifier, measure the visual field size
drawing diagonals from corner to corner of the
(length and width). Next, raise the spot-film
exposed area. Mark the exact center of the
tower, remove the leaded ruler, and replace it
film by drawing diagonals from corner to cor-
with a large-format x-ray film (35 cm × 43 cm)
ner of the film. Measure the distance between
on the underside of the spot-film tower and
the centers; this must not be more than 2% of
make a fluoroscopic exposure, still using the
the SID. Also, ensure that the exposed area is
largest available mode on the image intensi-
square to the film.
fier. A fluoroscopic exposure of about 5 sec-
onds is likely to provide sufficient film 2.9 AEC Object Thickness Compensation. This test
darkening. After the film has been processed, is to be conducted on each available radiographic
ensure that the dimensions of the exposed image receptor holder (e.g., spot-film, table Bucky,
area measured on the film do not differ from wall Bucky). Place 20 cm of 30 cm × 30 cm
the dimensions of the fluoroscopic image plexiglass on the table or support it up against the
measured with the lead ruler by more than 3% wall Bucky. (It is acceptable to use another patient
of the SID. At an SID of 100 cm, the maximum simulating material for AEC tests, such as alumi-
deviation is 3 cm. num.) Ensure that the plexiglass covers the AEC
Collimation of x-ray field size to spot film. Place detectors. Set the unit to operate at 80 kVp (or
a ruler with leaded 1 cm or 1/2″ markers on some other setting commonly used to image a
top of the box or plastic bucket, and lower the medium-sized patient). Load a cassette of a size
spot-film tower until the underside comes in commonly used with the standard film used at the
contact with the ruler. Place a medium-for- facility, and place this into the receptor holder
mat x-ray film (25 cm × 30 cm or 10″ × 12″) in being tested. Then make an AEC-controlled expo-
the spot-film tower, and place the film in the sure. Process the film on a processor that has
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Radiographic/Fluoroscopic Units, General-Purpose
previously been verified as operating optimally. Determining the necessary amount of patient-
Use a densitometer to measure the optical den- simulating material will require some experi-
sity of the radiograph in the center of the image. mentation, but about 1.5 mm of copper is likely
If the optical density falls within the range cho- to work well. Once the type and amount of simu-
sen by the radiologists (typically 1.2 to 1.4 OD), lator material have been determined, use those
repeat the test using identical setup conditions for all inspections.
but with varying amounts of plexiglass in the
beam. At a minimum, check the optical density Run a fluoroscopic exposure, and record the
at 15 cm and 25 cm of plexiglass. All films used exposure rate. Check for consistency of the rate
in this test should come from the same batch, with exposures made during previous inspec-
and only one cassette is to be used for all expo- tions. The typical rate is 1 R/min (with a typical
sures. The optical density of all the processed range of 0.5 to 2.0 R/min). The rate will depend
films should agree to within ±0.3 OD of the greatly on the image quality demands of the
optical density at 20 cm. user. However, if comparisons to previous in-
spections indicate an increasing level, further
tests should be performed to explain the required
2.10 AEC kVp Compensation. This test should also
increase in radiation.
be conducted on each available radiographic
image receptor holder (e.g., spot-film, table 2.12 Maximum Fluoroscopic Exposure Rate. Main-
Bucky, wall Bucky). Place 20 cm of plexiglass (or tain the test setup used for Item 2.11. However,
some other patient simulating material) on the this time, replace the patient simulator material
table or support it up against the wall Bucky. with at least 6 mm of lead. See Figure 2.
Ensure that the AEC detectors are covered by
the plexiglass. Use the most common size of Ensure that the whole input face of the image
films in the same cassette holder for all checks intensifier is covered by the lead plate. Record the
in this test. Make a series of AEC-controlled exposure rate on the electrometer or exposure
exposures of the 20 cm of plexiglass at different meter during a fluoroscopic exposure, in the auto-
kVp values. At a minimum, use three kVp set- matic mode as well as in the manual mode, at the
tings (e.g., 60, 80, and 100 kVp). For each expo- highest technique. If the system also has a boost
sure, process the film on an optimally or high-level control mode, record the exposure
preforming processor. Read the optical density rate during a fluoroscopic exposure in this mode.
of the radiograph using a densitometer. The For units that have only manually selectable kVp,
optical density of the films at all kVp settings mA settings, the exposure rate at the highest
checked should agree to within ±0.3 OD. settings should not exceed 5 R/min. For units that
have automatic kVp, mA control, the exposure rate
should not exceed 10 R/min.
2.11 Standard Fluoroscopic Exposure Rate. In addi-
tion to verifying that the unit meets exposure There are no governmental regulations that
requirements, this test also verifies functioning limit exposure rates under boost mode for devices
of the ABS. Use an ionization chamber with an
electrometer (or a combination exposure meter)
capable of measuring exposure rate.
The chamber position depends on the type of
system being tested: For an undertable x-ray
tube with a spot-film tower, place the chamber 1
cm above the tabletop. Position a box, with a
cutout for the chamber, over the chamber. For an
overhead x-ray tube, such as a remote imaging
system, place the chamber 30 cm above tabletop,
and position the tube as close as possible to the
chamber. Then, for an undertable x-ray tube,
place sufficient patient simulator material on the
box such that the fluoroscopic kVp tracks to Figure 2. Test setup for measuring maximum fluoro-
around 70 kVp under ABS. For an overhead x-ray scopic exposure rate
tube, place the simulator material on the tabletop.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
Inspection and Preventive Maintenance System
in use now. But devices manufactured in 1996 FOV, the three smallest holes should be visible.
and after will be required to limit boost exposure It may be necessary to alter the brightness
rates to under 20 R/min. and contrast settings on the TV monitor to
optimize the display for the visualized object.
2.13 Image Quality.
High-Contrast Resolution. Raise the spot-film 3. Preventive maintenance
tower, and place the line-pair phantom on the 3.1 Clean the exterior (interior if needed).
bottom of the spot-film surface. It should be
placed at a 45° angle to the grid lines and 3.2 Lubricate per the manufacturer’s instructions.
raster lines of the TV system. Center the 3.3 Calibrate the system to ensure performance
line-pair phantom using fluoroscopy. Lower within the manufacturer’s specifications, at in-
the spot-film tower until it contacts the line- tervals recommended by the manufacturer
pair phantom. At low kVp (ABS with nothing and/or as indicated by inspection results. Adjust
other than the line-pair phantom in the field), all brakes, locks, and bearings to ensure proper
determine the maximum line-pair resolution performance.
for all available field sizes. Resolution in the
9-inch mode should be a minimum of 1.2 3.4 Replace air filters, if needed.
lp/mm. For the high-contrast resolution test,
it may be necessary to alter the brightness 4. Acceptance tests
and contrast settings on the TV monitor to Acceptance testing is typically performed by a medi-
optimize the display for the object being visu- cal physicist.
alized. Be sure to mark and return the set-
tings to the levels set for clinical use. Before returning to use
Low-Contrast Resolution. Place the low-con- Ensure that all controls are set properly. Set alarms
trast phantom on the grid. Ensure that the 1 loud enough to alert personnel in the area in which the
mm piece of aluminum is next to the grid. The device will be used. Other controls should be in their
thicker aluminum pieces should be on top of normal pre-use positions. Attach a Caution tag in a
the 1 mm thick plate. Initiate a fluoroscopic prominent position so that the user will be aware that
exposure under ABS control. On the 15 cm (6) control settings may have been changed.
Inspection and Preventive Maintenance System
8 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 452-0595
Smoke Evacuators
Used For:
Smoke Evacuation Systems, Surgical [16-262]
Also Called: Laser smoke evacuators
Commonly Used In: Operating rooms or ambulatory surgery rooms in which laser surgery is performed
Risk Level: ECRI Recommended, Low; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor 1 month months . hours
Overview assessment (see Item 2.3); users experienced with this
assessment may be able to identify when filter re-
A smoke evacuator is used during surgery to remove placement is required. The assessment will also be
the smoke that may result from laser or electrosurgical useful in investigating operator complaints.
interaction with tissue. Smoke evacuation provides a
clear view of the surgical site, in addition to removal Charcoal filters also have a finite lifetime and must
of potential mutagens. The smoke evacuator is basi- be replaced after a specified time period. Because most
cally a vacuum pump with a sophisticated filtration evacuators lack hour meters, filter use must be logged,
system, which may include a charcoal filter and one or or the time must be estimated from the hospital’s
more particulate filters to remove gaseous elements average use.
and particles in the smoke.
The components of the filtration system have a Filter inspection and replacement intervals should
finite life span and must be replaced. Many manufac- be determined by reviewing the manufacturer’s recom-
turers list the expected life of the filters in the opera- mendations and considering the typical frequency of
tor’s manual; however, these expectations are only use. Depending on the degree of difficulty, require-
approximations and can vary with evacuator use. The ment for tools, and availability of appropriate staff,
more an evacuator is used, the more frequently its filter inspection and replacement may be performed by
filter components must be replaced. OR or clinical engineering staff. In either case, respon-
sibility for testing and replacement must be clearly
As a particulate filter becomes loaded with parti- established. When a unit includes a pressure gauge, or
cles, its flow resistance increases, which results in the manufacturer supplies a test procedure, inspection
decreased effectiveness. Some evacuators have pres- should be performed by the OR staff before each use
sure gauges or test cycles to measure the pressure drop (or at the end of each day). Clinical engineering per-
across the filtration system. However, few evacuators sonnel should supplement this testing on a monthly
have an indicator that signals the need for filter re- basis to ensure that it is taking place. If no simple test
placement. For evacuators that lack an integral is available, filters should be replaced at regular inter-
mechanism for determining filter integrity, we recom- vals, according to the manufacturer’s recommenda-
mend that the hospital institute a standardized tions or as determined by the procedure outlined
084827 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
452-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
above. Indicating the next date for filter replacement 1.3 Casters/Brakes. If the device moves on casters,
on a label or inspection sticker will facilitate routine check their condition. Verify that they turn and
replacement. swivel, as appropriate, and look for accumula-
tions of lint and thread around the casters.
Citations from Health Devices Check the operation of brakes and swivel locks,
if the unit is so equipped.
General-purpose surgical laser smoke evacuation sys-
tems [Evaluation], 1990 Jan; 19:5-19. 1.4 AC Plug/Receptacles. Examine the AC power
plug for damage. Attempt to wiggle the blades to
Special precautions check that they are secure. Shake the plug and
Because the charcoal and particle filters contain listen for rattles that could indicate loose screws.
potentially infectious material, technicians should use If any damage is suspected, open the plug and
infection control procedures (e.g., wearing gloves and inspect it.
masks) during filter replacement. Used filters should
be treated as potentially infectious waste. (For more If the device has electrical receptacles for ac-
details on infection control, see the “IPM Safety” arti- cessories, verify the presence of line power, in-
cle in this binder.) sert an AC plug into each, and check that it is
held firmly. If accessories are plugged and un-
Test apparatus and supplies plugged often, consider a full inspection of the
receptacles.
Leakage current meter or electrical safety analyzer
Ground resistance ohmmeter 1.5 Line Cord. Inspect the cord for signs of damage.
If damaged, replace the entire cord or, if the
Vacuum gauge (0 to 50 mm Hg) or pressure meter damage is near one end, cut out the defective
with equivalent capabilities portion. Be sure to wire a new power cord or plug
Nozzle (e.g., an evacuation tip) for vacuum gauge or with the correct polarity.
pressure meter; always use the same type of tip for
inspections (results may change if the tip type is 1.6 Strain Reliefs. Examine the strain reliefs at
changed) both ends of the line cord. Be sure that they hold
the cord securely.
“T” piece and adapters or tubing for connecting
gauge (meter) and tip to evacuator 1.7 Circuit Breaker. If the device has a switch-type
circuit breaker, check that it moves freely. If the
Procedure device is protected by an external fuse, check its
Before beginning an inspection, carefully read this value and type against that marked on the chas-
procedure and the manufacturer’s instruction and sis and ensure that a spare is provided.
service manuals; be sure that you understand how to
operate the equipment, the significance of each control 1.8 Tubes/Hoses. Check the condition of all hoses.
and indicator, and the alarm capabilities. Also deter- Be sure that they are not cracked, kinked, or
mine whether any special inspection or preventive dirty.
maintenance procedures or frequencies are recom-
1.15 Pump. Check the physical condition and proper
mended by the manufacturer.
operation of the pump. Clean if needed and note
this on Line 3.1 of the inspection form. (However,
1. Qualitative tests
do not check this item until all necessary clean-
1.1 Chassis/Housing. Examine the exterior of the ing is completed.)
unit for cleanliness and general physical condi-
tion. Be sure that plastic housings are intact, 1.18 Indicators/Displays. During the course of the
that all hardware is present and tight, and that inspection, confirm the operation of all lights,
there are no signs of spilled liquids or other indicators, meters, gauges, and visual displays
serious abuse. on the unit. Record reading of an hour meter, if
present.
1.2 Mount/Fasteners. If the device is mounted on a
stand or cart, examine the condition of the 1.22 Labeling. Check that all necessary placards, la-
mount. If it is attached to a wall or rests on a bels, conversion charts, and instruction cards
shelf, check the security of this attachment. are present and legible.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Smoke Evacuators
1.23 Accessories. Confirm the presence and condition
of accessories (e.g., footswitch, aspirator tubing,
adapter, canister).
2. Quantitative tests
2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with
good resolution of fractional ohms, measure and
record the resistance between the grounding pin
of the power cord and exposed (unpainted and
Figure 1. Test setup for filter inspections.
not anodized) metal on the chassis. We recom-
mend a maximum of 0.5 Ω. If the system is With experience, it is possible to correlate
modular or composed of separate components, vacuum levels to the amount of use and to smoke
verify grounding of the mainframe and each evacuation performance during clinical use.
module or component. If the device is double Typically, a drop to 75% of the initial vacuum
insulated, grounding resistance need not be level should be considered significant.
measured; indicate “DI” instead of the ground
resistance value. This measurement and the functioning of in-
tegral monitors would be affected by a damaged
If the device has an accessory receptacle, (e.g., torn) filter. Such damage may cause an
check its grounding to the main power cord. abnormal or misleading reading.
2.2 Leakage Current. Measure chassis leakage cur- Replace filter(s) if needed and indicate this on
rent to ground with the grounding conductor of Line 3.4 of the inspection form. If, following
plug-connected equipment temporarily opened filter replacement, the gauge reading does not
with the device on and off. Maximum chassis leak- return to the expected value, consider the possi-
age current to ground should not exceed 300 µA. bility of other occlusions (e.g., additional filters
or canisters that require replacement) or pump
2.3 Filters. Check particle and charcoal filters accord-
deterioration.
ing to manufacturer recommendations. For units
without an integral mechanism (e.g., pressure 3. Preventive maintenance
gauge, filter test mode) for assessing the filter, use
the following test to roughly quantify performance 3.1 Clean exterior; clean interior if needed.
and provide a basis for comparison from one in- 3.4 Replace filters if needed.
spection to the next. (First perform the test on the
unit with new filters to obtain a benchmark for 4. Acceptance tests
future inspections.)
Conduct major inspection tests for this procedure
Remove accessory tubing from the evacuator. and the appropriate tests in the General Devices Pro-
Attach a standard nozzle, such as an evacuation cedure/Checklist 438.
tip, and a vacuum gauge or pressure meter to two
ports of a “T” adapter. Connect the third port to Before returning to use
the evacuator (see Figure 1). Set the unit to its Return controls to their preinspection or normal
highest flow setting and record the vacuum level. pre-use settings.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 424-0595
Sphygmomanometers
Used For:
Sphygmomanometers, Aneroid [16-156]
Sphygmomanometers, Mercury [16-158]
Also Called: Aneroid or mercury sphygmomanometers
Commonly Used In: All patient care areas
Scope: Applies to manual aneroid and mercury sphygmomanometers, including the manometer, cuff, squeeze
bulb, and associated tubing; does not apply to automated or invasive blood pressure monitoring devices (see
Procedure/Checklist 454 or 434, respectively)
Risk Level: ECRI Recommended, Low; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview the pressure of mercury (mm Hg) on the graduated
scale. Air displaced by the rising mercury column is
The blood pressure of a hospitalized patient is rou- vented at the top of the tube through a filter, which
tinely measured upon admittance, throughout the day, keeps the mercury from spilling out and filters the air.
and during and after surgery. Blood pressure is also
measured in the emergency room and outpatient
areas. In an aneroid sphygmomanometer, pressure extends
a bellows or flexes a diaphragm. Through a mechanical
A sphygmomanometer — the prefix “sphygmo” linkage, this movement rotates a pointer on a gradu-
means “relating to pulse” — consists of an inflatable ated dial gauge to the appropriate pressure reading.
compression bag enclosed in a relatively inelastic but
flexible covering called the cuff; a squeeze bulb with
valves for inflating and deflating the compression bag; The bulbs, valves, cuffs, compression bags, and tub-
a manometer (pressure-measuring device); and con- ing of mercury and aneroid blood pressure sets are
necting tubing. The manometer can be a mercury or similar and have similar maintenance requirements.
aneroid (nonliquid) type. The manometers have basic differences in operating
principles. The accuracy of a mercury manometer de-
A mercury sphygmomanometer includes a narrow, pends on dimensions that are fixed at the time of
vertical, constant-bore glass or plastic tube, connected manufacture; on the free flow of air above the mercury
at its bottom end to a large-diameter well containing column in the glass tube; on the cleanliness of the tube;
mercury. When the system is unpressurized, both the and on the amount of mercury in the system. Once an
well and the tube have the same mercury level, marked initial calibration has shown the bore of the glass tube
“0” on the tube’s graduated scale. Squeezing the bulb to be uniform and the graduated scale to be true, only
applies pressure to the inflatable bag and the mercury simple maintenance is needed to ensure lifetime accu-
well, forcing mercury up the tube to a height indicating racy of the instrument.
009086 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
424-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Aneroid gauges are dependent on deflection of a should remove all jewelry, especially gold or gold-
diaphragm within the meter. These units are prone to plated jewelry (mercury readily combines with gold)
error due to overpressurization, mechanical vibration, and should wear a mercury-vapor respirator and dis-
and shock received during normal use. Their reliability posable gloves. In high-use areas, workers should
is highly dependent on periodic inspection. Mercury wear disposable gowns and shoe coverings to minimize
sphygmomanometers are traditionally considered skin and clothing contamination, which can increase
more accurate and reliable in high-use hospital set- worker exposure and carry mercury to other areas of
tings, but newer, high-quality, wall-mounted aneroid the healthcare facility.
gauges are available that are more reliable than earlier
designs. We recommend against hospitals cleaning and proc-
essing their own mercury, since this increases mercury
Advise clinical personnel to have the units checked exposure risks. Dirty mercury should be stored in
following abuse (e.g., an accidental drop) that might have sealed, break-resistant containers until properly dis-
caused damage. This will minimize the risk of spilled posed of or delivered to a mercury refinery. (For more
mercury or inaccurate aneroid gauge readings. Replace- information on mercury contamination and control,
ment of mercury sphygmomanometers on a high-priority see the section on IPM Safety behind the Guidance Tab
basis is not cost-effective or justified if there are adequate of this binder.)
procedures for handling mercury. However, planned
elimination of mercury sphygmomanometers to reduce Procedure
the risk of mercury exposure is recommended.
Before beginning the inspection, carefully read this
procedure and the manufacturer’s instructions. Also
Citations from Health Devices determine whether any special inspection or preven-
Sphygmomanometers [Evaluation], 1971 Aug; 1:99-104. tive maintenance activities or frequencies are recom-
mended by the manufacturer.
Sphygmomanometers [Evaluation], 1975 Aug; 4:227-39.
Many sphygmomanometers lack serial numbers or
Test apparatus and supplies a convenient area to place a control-number tag. The
Pressure gauge or meter (not required for testing control number can be engraved on the back of the
mercury sphygmomanometers except for initial in- aneroid gauge or along the edge of a mercury manome-
spection or when glass tube is replaced) ter scale.
Y connector 1. Qualitative tests
Cylindrical object to simulate an arm (e.g., 1 lb
1.1 Chassis/Housing. Examine the exterior of the
coffee can or pipe with 3 to 4 in outside diameter)
unit for cleanliness and general physical condi-
Stopwatch or watch with a second hand tion. Be sure that plastic housings are intact,
Mercury column filler and mercury may be required that necessary assembly hardware is present
and tight, and that there are no signs of spilled
Special precautions liquids or other serious abuse. Examine mer-
cury column tubes for cracks. Remove damaged
CAUTION! Mercury and its vapors are toxic. All tubes from service, even if not currently leaking
workers who use, clean, or maintain mercury sphyg- or affecting performance, to avoid the possibility
momanometers should understand the properties of of mercury spills. Examine aneroid gauge hous-
mercury and its associated hazards and should be ings for dents and loose parts.
instructed in safe handling procedures. Specific poli-
cies and procedures must be established for mercury 1.2 Mount. If the device is mounted on a stand or
spill cleanup, and specific areas should be designated cart, examine the condition of the mount. If it is
for maintenance activities. attached to a wall or rests on a shelf, check the
security of this attachment.
The room used for sphygmomanometer calibration
and repair should be well-ventilated and reserved for 1.3 Casters/Brakes. If the device moves on casters,
the exclusive task of handling mercury; traffic through check their condition. Look for accumulations of
the area should be limited. There should be no smok- lint and thread around the casters, and be sure
ing, drinking, or eating in the room. The floor should that they turn and swivel, as appropriate. Check
not be carpeted, and a workbench should be equipped the operation of brakes and swivel locks, if the
with troughs to collect mercury spills. Personnel unit is so equipped. Conductivity checks, where
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Sphygmomanometers
appropriate, are usually done more efficiently as 1.24 Gauge/Column. Ensure that the pointer of an
part of a check of all equipment and furniture in aneroid gauge falls smoothly throughout its
an area. scale and does not stick or bind. In a mercury
manometer, the glass tube and mercury should
1.8 Tubes/Hoses/Bulb. Check the condition of all be clean. Check that the mercury column rises
tubing and hoses and the bulb. Be sure that they and moves smoothly. Mercury “dancing” or
are not cracked, kinked, or dirty. Replace loose “clinging” to the walls of the tube indicates a
or cracked tubing. dirty tube and filter. If the tube appears dirty,
remove it and clean it with an oversized pipe
1.10 Fittings/Connectors. Examine all fittings and cleaner. Before removing the glass tube for
connectors for general condition. cleaning, be sure that all the mercury is in the
reservoir either by tilting the unit or, on some
1.12 Filters. Check the condition of mercury column
units, by unlatching the locking mechanism. Re-
filters. Replace as needed and indicate on Line
place dirty mercury. CAUTION: Mercury is
3.4 of the inspection form.
toxic (see Special Precautions).
1.13 Bleed Valve. It should be possible to quickly and
accurately adjust the bleed valve to a rate of 2 to 2. Quantitative tests
3 mm Hg/sec. Pressurize the system and check 2.3 Pressure Leakage. Wrap the cuff around a simu-
the valve to see if it can be easily adjusted to this lated limb (coffee can or pipe, 3 to 4 in diameter).
bleed rate. A bleed valve with a damaged seat Close the bleed valve, and inflate the cuff to
will open too quickly, and it will be difficult to about the maximum scale indication. Read the
adjust the rate accurately. scale indicator after 1 min to determine the rate
of pressure loss in mm Hg/min. This rate should
1.18 Indicators/Displays. Meter and scale markings
not exceed 15 mm Hg/min. If it does, recheck all
should be clear and easy to read, and the cover
fittings, especially Luer taper fittings, and re-
glass on an aneroid gauge should be intact.
peat the test.
1.19 Zero Pressure Setting. With no pressure in the 2.10 Gauge Accuracy. Periodically check the accu-
cuff, the aneroid gauge or mercury level should racy of aneroid gauges. This test need not be
read zero (±1 mm Hg). If a mercury manometer done on mercury sphygmomanometers except
does not read zero, add or remove mercury care- during incoming inspection or when the glass
fully until it does. Discard aneroid gauges that tube has been replaced.
cannot be reset to read zero.
Connect the blood pressure set to a pressure
1.22 Labeling. Check that all necessary placards, la- gauge or meter using a Y connector, as shown
bels, conversion charts, and instruction cards in Figure 1. Inflate the system to 200 mm Hg
are present and legible.
1.23 Accessories.
Cuffs. Use of an improperly sized cuff can cause
significant measurement errors. Clinical per-
sonnel should be instructed never to substi-
tute an improper cuff for lack of one of proper
size. Record the cuff sizes that are either
stored with the manometer or are readily
available (e.g., at a nearby nursing station) on
the inspection form. These should correspond
to physical characteristics of the patients on
whom the instrument is likely to be used (e.g.,
smaller cuffs in a pediatric area). All cuffs
should be clean and in good condition with no
torn stitching. Look for signs of degradation
or cracking of the bladder. Check that Velcro
Figure 1. Test setup.
closures hold firmly.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
on the gauge or meter and record the reading of 3.2 Lubricate casters, swivel wall mount.
the unit under testing. It should not differ by
more than 3 mm Hg from the true pressure. 3.4 Replace mercury column filters and mercury, if
Aneroid gauges should be accurate in all posi- dirty.
tions in which they are likely to be held while
being read. Repeat the test for pressures of 120 4. Acceptance tests
and 60 mm Hg. Record pressures only when the
Conduct major inspection tests for this procedure.
system is at equilibrium (i.e., the pressure is not
varying).
Before returning to use
3. Preventive maintenance Ensure that no mercury has been spilled on the
3.1 Clean exterior and mercury tube, if needed. device and that the cuff is reconnected to the unit.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 459-0595
Suction Regulators
Used For:
Regulators, Suction, Low-Volume [13-329]
Regulators, Suction, Surgical [15-051]
Regulators, Suction, Thoracic [13-332]
Regulators, Suction, Tracheal [13-333]
Also Called: Vacuum regulators, suction controllers
Commonly Used In: Operating rooms, short-procedure or same-day surgery areas, emergency depart-
ments, critical care units, medical-surgical units
Scope: Applies to virtually all types of suction regulators used with central vacuum systems; does not apply
to aspirators (see Procedure/Checklist 433)
Risk Level: ECRI Recommended, High for Tracheal Suction Regulators, Medium for Surgical and Thoracic
Suction Regulators, and Low for Low-Volume Suction Regulators; Hospital Assessment, for
Low-Volume Suction Regulators, for Surgical Suction Regulators, for Tho-
racic Suction Regulators, and for Tracheal Suction Regulators
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
* Regulators in emergency departments, the OR, and some critical care units may require a six-month
inspection interval if they are the only source of tracheal suction. It may be efficient to inspect suction regulators
during the annual testing of the institution’s medical gas/vacuum system (Procedure/Inspection Form 440).
Overview diaphragm and dictates the pressure at which the
diaphragm will open or close the vacuum control valve.
Suction by means of a regulated central vacuum sys- The vacuum level of a suction regulator depends on
tem (and/or aspirator) is widely used in hospitals to its application, as follows: thoracic suction, 0 to 45 mm
remove secretions such as vomitus, mucus, or blood Hg; low-volume (gastric) suction, 0 to 150 mm Hg; and
during surgical procedures or to remove secretions in surgical, tracheal, and uterine suction, 0 to >300 mm
wound cavities following surgery. Clinical examples Hg. (The maximum vacuum of most central systems is
include surgical site suctioning, tracheal suctioning, >400 mm Hg.) Low-volume regulators typically oper-
wound drainage, gastric and uterine aspiration, and ate intermittently, cycling between atmosphere and
emergency airway clearance. 120 mm Hg, but some also have a continuous-flow
mode.
A suction regulator works on the same principle as
a compressed gas regulator: a diaphragm that is linked Regulators generally have a tiny bleed hole in the
to a control valve continuously senses the vacuum of patient port chamber that allows the suction system to
the suction channel. A spring works against the sensing respond to changing conditions. Because the bleed hole
084751 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
459-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
is typically only a fraction of a millimeter in diameter, service manuals; be sure that you understand how to
it can be clogged by dirt, lint, or other fine particles operate the equipment and the significance of each
suspended in the air; some regulators have a bleed hole control and indicator. Also determine whether any
filter. The bleed hole (and filter) should be examined special inspection or preventive maintenance proce-
whenever a regulator is opened for repair. dures or frequencies are recommended by the manu-
facturer.
Citations from Health Devices
It is vital to identify the type and/or application of
Filters in suction lines, 1982 Jan-Feb; 11:97-8.
the suction regulator to be inspected in order to define
Suction canisters [Evaluation], 1983 Apr; 12:127-49. the performance criteria for the inspection. In addi-
tion, the inspector must know if the regulator has a
General purpose wall vacuum regulators [Evaluation],
factory-set limit that is below the operating vacuum
1985 May; 14:191-209.
level of the system. (A minimum system vacuum of
Should vacuum pump effluent be treated? [User Expe- 300 mm Hg [12 in Hg] is required, but many systems
rience NetworkTM], 1994 Jul; 23:310. cycle between 400 and 600 mm Hg; tracheal suction
regulators may have an upper limit of 200 mm Hg.)
Use of filters on medical gas system outlets and vac- This information may be difficult to obtain because
uum system inlets [User Experience NetworkTM], some regulators bear only a model or catalog number.
1994 Dec; 23:494-5. Obtain device specifications from the manufacturer’s
literature, previous inspection forms, or clinical per-
Test apparatus and supplies sonnel. Once the type of regulator has been identified
Vacuum gauge, 0 to 760 mm Hg, ±3%, or pressure or when new units are purchased, enter this informa-
meter with equivalent capabilities tion on the equipment control or inventory record so
Flowmeter, 10 to 50 L/min, ±5% that it can be determined quickly in future applica-
tions.
Tubing and adapters for connecting vacuum gauge
or pressure meter and flowmeter (a T fitting is
needed) 1. Qualitative tests
Special precautions 1.1 Chassis/Housing. Examine the exterior of the
unit for cleanliness and general physical condi-
Never place your mouth on any part of the regulator tion. Be sure that housings are intact, that all
to blow or suck as a qualitative test of operation or to hardware is present and tight, and that there are
blow dirt out of a part. no signs of spilled liquids or other abuse.
Suction regulators should be used with an overflow
safety trap/filter, and most suction canisters are de- 1.8 Tubes/Hoses. Check the condition of all tubing
signed to prevent escape of suctioned material; still, and hoses. Be sure that they are not cracked,
contamination of the regulator can occur. Because kinked, or dirty. Replace if needed and indicate
contamination cannot be easily ascertained, the device this on Line 3.4 of the inspection form.
should be sterilized before it is opened. Follow the
1.10 Fittings/Connectors. Examine all fittings and
manufacturer’s instructions for sterilization; the regu- connectors for general condition and, where ap-
lator knob will usually need to be adjusted to maxi- plicable, for the presence of O-rings, gaskets,
mum suction setting. Check the regulator filter
etc.; verify that they are securely attached. Re-
condition following sterilization. (Note: Gas steriliza- place if needed and indicate this on Line 3.4 of
tion may not be effective if there is fluid inside the the inspection form. Examine the patient and
regulator.) If the regulator cannot be sterilized, wear
vacuum port connectors for liquids or residue
latex gloves, wrap cellophane or another nonperme- from dried aspirant. If keyed connectors (e.g.,
able barrier around the handles of all tools, and work pin-indexed gas connectors) are used, make sure
on a surface that can be easily disinfected. Dispose of
that no pins are missing and that the keying is
gloves and tool handle wrappings with infectious correct.
waste.
1.12 Filters. Check the condition of all filters, espe-
Procedure cially after the regulator has been sterilized.
Before beginning the inspection, carefully read this Replace if necessary and indicate this on Line 3.4
procedure and the manufacturer’s instruction and of the form.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Suction Regulators
1.13 Controls/Switches. Examine all controls and
switches for physical condition, secure mount- Suction Regulator Performance Values
These performance values represent best current opinion on clinical need
ing, and correct motion. Check that control and typical regulator capability, not optimal design criteria. Units unable to
knobs have not slipped on their shafts. Where a meet these criteria should be discussed with clinical staff and scheduled for
replacement or repair.
control should operate against fixed-limit stops,
Maximum Vacuum Maximum Flow
check for proper alignment, as well as positive
Type (mm Hg) (L/min)
stopping. Verify dynamic regulator operation by
Low Volume >40 NA
adjusting for maximum suction level, occluding Surgical >300 >30
the catheter line until the vacuum level peaks, Thoracic >40 >20
and then adjusting for 100 mm Hg. Check for Tracheal >300 >30
any leaks through the regulator by turning it off Uterine >300 >30
and observing the gauge with the patient port
occluded; if there are no leaks, the gauge needle piece of large-diameter tubing from the flowme-
will indicate a zero reading. ter to the device, with the correct size adapters
inserted at the regulator end. Any restrictions
1.18 Indicators/Displays. During the course of the (e.g., small-bore adapters) will tend to reduce the
inspection, confirm the operation of gauges and free airflow.
visual displays on the unit. Ensure that the
needle returns to zero when the regulator is 2.5 Maximum Vacuum. Connect the vacuum gauge
turned off. or pressure meter to the collection bottle or can-
ister patient connector with thick-walled tubing.
1.22 Labeling. Check that all necessary placards, la-
Adjust the regulator for maximum suction and
bels, conversion charts, and instruction cards
record this value. If the expected value (see the
are present and legible.
Suction Regulator Performance Values table
1.24 Overflow Protection. Confirm the presence and above) is not obtained, look for air leaks, espe-
condition of the overflow safety trap/filter as- cially in the collection bottle/canister and over-
sembly. In devices where overflow protection is flow safety trap caps and hoses.
provided by a hollow plastic ball, the ball will not
2.6 Vacuum Gauge Accuracy. Check the accuracy of
function reliably if it is dented or cracked or has
the vacuum gauge by comparing it to the test
dried aspirate solids adhering to it. (To verify
measurement device at low, medium, and high
operation of the overflow protection, water must
settings. Readings should be within 10% of full-
be aspirated into the protective device until it
scale deflection.
activates; such testing is not necessary for accep-
tance or routine inspections. If it is performed,
clear tubing should be used between the overflow
3. Preventive maintenance
protection device and the regulator; be prepared 3.1 Clean the exterior (do not immerse) and interior
to immediately turn off the regulator if the pro- of the suction regulator and overflow safety trap,
tective mechanism fails and fluid enters the if needed. Overflow protection mechanisms in
regulator’s input tubing.) reusable collection bottles and safety traps are
1.25 Intermittent Operation. If the regulator has an especially likely to require disassembly and
intermittent mode, verify that cyclical suction cleaning. Wear latex gloves when cleaning or
occurs (e.g., on 15 sec, off 8 sec) and that vacuum repairing a regulator. Verify patency of the
reaches the preselected level. bleed hole during repair.
3.2 Lubricate per manufacturer’s instructions.
2. Quantitative tests
2.4 Maximum Flow. Measure the maximum free 3.3 Calibrate gauge and timing of intermittent
airflow with the flowmeter and compare it with mode, if needed.
recommended values in the table. (This meas- 3.4 Replace filter(s), O-rings, gaskets, diaphragms,
urement need not be made in the intermittent if needed.
mode of operation.) Set the regulator for maxi-
mum suction. Perform the test with collection 4. Acceptance tests
bottle or canister in place, but without patient
catheters. Use either a direct coupling or a short Conduct major inspection tests for this procedure.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 425-0595
Temperature Monitors
Used For:
Temperature Monitors [12-672]
Thermometers, Electronic, Continuous [14-034]
Thermometers, Electronic, Intermittent [14-035]
Thermometers, Infrared, Ear [17-887]
Also Called: Electronic thermometers; infrared ear units are often referred to as “tympanic” thermometers,
although most units detect ear canal temperature and do not focus on the tympanic membrane
Commonly Used In: Operating rooms, nurseries, critical care units, emergency departments, patient care
rooms
Scope: Applies to line- or battery-powered thermometers
Risk Level: ECRI Recommended, Low; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview a special integrated circuit (typically, a matrix of small
thermocouples). Probe covers are part of the optical
Electronic thermometer designs range from a simple system and must be used for all readings because ear
temperature-sensing probe and readout to more com- wax buildup will produce inaccurate readings.
plex systems with alarms and calibration checks. An
electronic thermometer has a temperature probe that Some clinical applications and/or patient conditions
contains a sensing element (thermistor) whose resis- require continuous temperature monitoring (e.g., pa-
tance to the flow of electrical current varies with tem- tients under general anesthesia or suffering from any
perature. The resistance is measured by an electronic condition that depresses the body’s ability to regulate
circuit, and the corresponding temperature is dis- its own temperature, such as shock and septicemia).
played on an analog or digital meter. The circuits and Infants whose temperature-regulating mechanisms
display may be powered by line voltage, a rechargeable have not fully developed are often monitored. Body
battery, or a primary (nonrechargeable) battery. temperature should also be monitored during artificial
Many electronic thermometers use a cable with a heating or cooling. Monitors may stand alone or may
thermistor in the tip. A disposable cover is placed over be incorporated into multiparameter physiologic moni-
the tip or probe before each use. Cable/probe thermis- toring systems, infant incubators, and hypo/hyper-
tor unit temperature measuring sites include the thermia machines.
mouth, rectum, and axilla.
The vast majority of temperature measurements in
Infrared (IR) ear thermometers utilize an optical healthcare facilities are taken periodically along with
system to focus the IR radiation emitted by the ear other vital signs (e.g., once or twice during an eight-
canal or, in some cases, the tympanic membrane onto hour shift). Most electronic thermometers used for
009088 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
425-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
intermittent or discrete measurements are designed to whether any special inspection or preventive mainte-
reduce the time required to obtain a reading by pre- nance procedures or frequencies are recommended by
dicting patient temperature from the rate of tempera- the manufacturer.
ture rise after inserting the probe. For thermometers
with cable/probe thermistors, predictive mode meas- 1. Qualitative tests
urement time is typically within 15 to 60 sec. Some IR 1.1 Chassis/Housing. Examine the exterior of the
ear thermometers predict temperatures at alternative unit for cleanliness and general physical condi-
sites and produce a reading within 3 sec. tion. Be sure that plastic housings are intact,
Cable/probe thermistors are available with a vari- that all assembly hardware is present and tight,
ety of physical and electrical characteristics. Gener- and that there are no signs of spilled liquids or
ally, the electrical characteristics of all probes other serious abuse.
designed for a given instrument will be similar, but 1.2 Mount. If the device is mounted on a stand or
probe shapes may differ to facilitate temperature cart, examine the condition of the mount. If it is
measurements at various anatomic sites. Probes in- attached to a wall or rests on a shelf, check the
tended for use with different model units may not be security of this attachment.
interchangeable, even though both are designed for the
same anatomic site. 1.4 AC Plug. Examine the AC power plug for dam-
age. Attempt to wiggle the blades to determine
Citations from Health Devices that they are secure. Shake the plug and listen
for rattles that could indicate loose screws. If
Intermittent-use electronic thermometers [Evalu-
any damage is suspected, open the plug and
ation], 1982 Nov; 12:3-20.
inspect it.
Infrared ear thermometry [Guidance article], 1991
1.5 Line Cord. Inspect the cord for signs of damage.
Nov; 20:431-41.
If damaged, replace the entire cord, or if the
Test apparatus and supplies damage is near one end, cut out the defective
portion. Be sure to wire a new power cord or plug
Leakage current meter or electrical safety analyzer. with the correct polarity. Check line cords of
Ground resistance ohmmeter. battery chargers.
Reference thermometer, accurate within 0.1°C 1.6 Strain Reliefs. Examine the strain reliefs at
(0.2°F) over a range of at least 30° to 45°C (86° to both ends of the line cord. Be sure that they hold
113°F); an equivalent Fahrenheit thermometer can the cord securely.
be used if the units to be tested include Fahrenheit
scales. Precision mercury-in-glass thermometers 1.7 Circuit Breaker/Fuse. If the unit has a switch-
traceable to the National Institute of Science and type circuit breaker, check that it moves freely.
Technology (NIST) are available from chemical sup- If the unit is protected by an external fuse, check
ply houses. Alternatively, another electronic ther- its value and type against that marked on the
mometer of known accuracy may be used, but it may chassis, and ensure that a spare is provided.
require more frequent calibration.
1.9 Cables. Inspect cables (e.g., sensor) and their
Constant temperature water bath with a tempera- strain reliefs for general condition. Examine
ture range of 30° to 45°C. cables carefully to detect breaks in the insulation
Certified emmisivity black body or the thermometer and to ensure that they are gripped securely in
manufacturer’s dedicated calibration device (for IR the connectors of each end to prevent rotation or
ear thermometers). other strain.
Patient probe simulator (optional for cable/probe 1.10 Connectors. Examine all electrical connectors
thermistor thermometers). for general condition. Electrical contact pins or
surfaces should be straight, clean, and bright.
Procedure
1.11 Probes. Check that all probes are clean and not
Before beginning an inspection, carefully read this cracked, brittle, or otherwise damaged.
procedure and the manufacturer’s instruction and
service manuals; be sure that you understand how to 1.13 Controls/Switches. Before moving any controls
operate the equipment, the significance of each control and alarm limits, check their positions. If any of
and indicator, and the alarm capabilities. Also determine them appear inordinate (e.g., a zeroing control
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Temperature Monitors
or alarm limits at the ends of their range), con- the probe. It may not be possible to verify the
sider the possibility of inappropriate clinical use operation of all alarms at this time (e.g., high and
or of incipient device failure. Record the settings low temperature), but you should know all the
of those controls that should be returned to their alarm capabilities and remember to check them
original positions following the inspection. at the appropriate time.
Examine all controls and switches for physical 1.22 Labeling. Check that all necessary placards, la-
condition, secure mounting, and correct motion. bels, conversion charts, and instruction cards
Where a control should operate against fixed- are present and legible.
limit stops, check for proper alignment, as well
as positive stopping. Check membrane switches 1.23 Accessories. Probe covers should be stored with
for membrane damage (e.g., from fingernails, the unit. Notify clinical personnel if the covers are
pens). During the course of the inspection, be missing or are stored incorrectly (e.g., in a manner
sure to check that each control and switch per- that will not protect their cleanliness). A used
forms its proper function. cover should not be left on the probe after testing.
1.17 Battery/Charger. Inspect the physical condition 2. Quantitative tests
of batteries and battery connectors, if readily
accessible. Check operation of battery-operated 2.1 Grounding Resistance. Using an ohmmeter,
power-loss alarms, if so equipped. Operate the electrical safety analyzer, or multimeter with
unit on battery power for several minutes to good resolution of fractional ohms, measure and
check that the battery is charged and can hold a record the resistance between the grounding pin
charge. Check remaining battery capacity by of the power cord and exposed (unpainted and
activating the battery test function. Check the not anodized) metal on the chassis. We recom-
condition of the battery charger and, to the extent mend a maximum of 0.5 Ω. If the system is
possible, confirm that it does, in fact, charge the modular, verify grounding of the mainframe and
battery. When it is necessary to replace a battery, each module. If the device has an accessory out-
label it with the date. let, check its grounding to the main power cord.
1.18 Indicators/Displays. During the course of the 2.2 Leakage Current. Measure chassis and patient
inspection, confirm the operation of all lights, lead leakage current to ground with the ground-
indicators, meters, and visual displays on the ing conductor temporarily opened. Operate the
unit and charger, if so equipped. device in all normal modes, including on,
standby, and off. Leakage current should not
Check that all digits light in digital displays exceed 300 µA.
either by observing the changing temperature
readings as the probes warm during the water 2.10 Temperature Accuracy (cable/probe thermistor
bath accuracy test or by varying the probe simu- thermometers).
lator through its range. A display of “8” in the Predictive mode. Check approximate accuracy by
tens and units positions will check all elements taking an oral temperature. Compare the
of a segmented or dot display. Confirm that a “1” electronic thermometer reading with the
can be displayed in the hundreds position of a reading taken with a mercury thermometer
Fahrenheit display. on the same person at about the same time.
Expect discrepancies of several tenths of a
1.19 User Calibration. Confirm that the calibration
degree Celsius with this method. Larger er-
function operates. If the unit has an external
rors or inconsistent results may result from
calibration adjustment, verify that the control
improper user technique with either ther-
can be set to a point that brings the unit within
mometer. Improper technique may include
calibration and that this setting is not near the
failure to leave the mercury thermometer in
end of its range. A setting near the end of its
place long enough (3 to 8 min), incorrect place-
range may indicate that the unit requires bat-
ment of the probe and/or the glass thermome-
tery replacement or an internal adjustment.
ter, repeating an electronic thermometer
1.20 Alarms. Visual alarms should function prop- measurement before the probe has cooled suf-
erly. Confirm appropriate volume, as well as the ficiently, and repeating an electronic ther-
operation of a volume control. Check the probe- mometer measurement without replacing the
disconnect alarm, if so equipped, by unplugging probe cover.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
Thermometers that also allow operation in a body-temperature water bath, allow them to
steady-state mode facilitate assessment of the equilibrate, and successively plug each into
predictive mode and can be tested with a water the same pretested thermometer unit or mod-
bath. However, this steady-state test does not ule. All probes should give the same tempera-
check all of the predictive circuitry. See the ture reading. Some variation is normal
unit’s operating manual for specific instructions because the water temperature varies
for activating the steady-state mode and for slightly with location in the bath and the
specifications and directions for testing. water gradually cools with time.
Steady-state mode. Test the accuracy of the ther-
Steady-state thermometers should be ac-
mometer in a water bath of known tempera-
curate within 0.3°C (0.5°F) or within manu-
ture or with a patient probe simulator. Check
facturers’ specifications, with some allowance
accuracy at 35°C (95°F), 37°C (98.6°F), and
for possible errors in the measuring system.
39°C (102.2°F). Check thermometers in-
Correct reading inaccuracies according to the
tended for wide temperature range applica-
manufacturer’s recommended calibration
tions (e.g., hypothermia monitoring) at
procedure.
temperatures near the high and low extremes
of the range.
2.11 Temperature Accuracy (IR ear thermometers). It
If a patient probe simulator is not avail-
may be necessary to put the thermometer into a
able, use a thermostatically controlled con-
calibration or “unadjusted” mode. Test meas-
stant temperature water bath for accuracy
urements are made using a black body heated to
measurements. Alternatively, hot and cold
temperatures in the range of 35°C to 39°C. The
tap water can be mixed in an insulated cup or
black body must have an orifice that mates
beaker or a thermos flask to achieve the de-
snugly with the probe of the ear thermometer. If
sired test temperatures. Use a precision ther-
a black body float is used, place it in a water bath
mometer to measure the water temperature.
adjusted to 37°C. While agitating the bath suffi-
If a mercury-in-glass calibration thermome-
ciently to ensure thermal uniformity, measure
ter is used, submerge it to the recommended
the bath temperature by positioning the calibra-
depth to ensure a correct reading. Vary the
tion thermometer so that its tip is positioned
temperature by adding hot or cold water as
near the center of the bath without touching the
needed. Stir the water frequently and allow
sides or bottom; allow one minute for a reliable
sufficient time for the temperature probe and
reading and to ensure that the temperature has
the calibration thermometer to equilibrate at
equilibrated. Insert the probe of the thermome-
the water temperature before taking readings
ter into the black body so that it occludes the cone
and comparing them. Fluctuating or decreas-
of the float. IR thermometer readings should be
ing water bath temperature may cause errors
within 0.3°C of the bath temperature or other
if the response times of the electronic ther-
calibration device.
mometer being tested and the calibration
thermometer differ greatly or if the ther-
2.12 Temperature Alarms. This test checks the high-
mometer being tested is the type that reads
and low-temperature alarms of monitoring mod-
the maximum temperature during a meas-
ules. Set the low-temperature alarm below 35°C
urement. When inspecting multiple units,
and dip the probe in a 35°C water bath, or set the
use three vessels to establish the three test
simulator at the equivalent resistance. Slowly
temperatures at the same time to avoid the
increase the alarm setting until the alarm acti-
necessity of changing the temperature. Also,
vates. Record the final alarm setting and the
if conditions permit, save time by placing the
actual water bath temperature. They should be
probes of all the thermometers to be tested in
within 0.6°C.
the same bath simultaneously.
If a patient probe simulator is used, remem- Set the high-temperature alarm above 39°C,
ber that the simulator tests only the circuitry and place the probe in a 39°C water bath or use
and not the probe itself; therefore, probe op- the probe simulator. Slowly decrease the alarm
eration and accuracy must still be tested for at setting until the alarm activates. Record the
least one temperature. A convenient method alarm setting and the actual water bath tem-
is to dip all probes simultaneously into one perature. They should also be within 0.6°C.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Temperature Monitors
3. Preventive maintenance than 100 µA, then it is unnecessary to check
leakage current from the probe itself.
3.1 Clean the exterior of all units and the probe lens
of IR units, if needed. If the preceding method is inconvenient or if the
leakage current obtained exceeds 100 µA, measure
4. Acceptance tests patient probe leakage current by dipping the probe into
Conduct major inspection tests for this procedure a container of water. Do not immerse the probe above
and the appropriate tests in the General Devices Pro- the handle or allow the solution to enter any connec-
cedure/Checklist 438. In addition, perform the follow- tors. Leakage currents should not exceed 100 µA.
ing test. However, a reading above a few microamperes may
indicate deterioration of the probe covering and a need
4.1 Patient Probe Leakage Current. This test ap- to replace the probe.
plies only to units that can operate on line power
with probes that are not ground referenced.
Measure probe circuit leakage current directly
Before returning to use
from each probe electrical lead contact (using an Return alarms and other controls to their pre-in-
appropriate connector). If the leakage current to spection or normal pre-use setting. Recharge batteries
ground from each lead of the connector is less or equip with fresh batteries if needed.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Procedure/Checklist 427-0595
Traction Units
Used For:
Traction Units, Intermittent [14-106]
Traction Units, Intermittent, Mobile [14-108]
Also Called: Intermittent traction units, powered traction units
Commonly Used In: Physical therapy departments and clinics, orthopedic clinics
Scope: Applies to powered traction units used for cervical and lumbar traction; does not apply to static
traction devices consisting of pulleys and weights
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months months . hours
Minor NA months . hours
Overview against the bed dissipated all of the linear force before
it could widen the lumbar intervertebral spaces. Thus,
Traction units powered by hydraulics or an electric split beds were developed that allowed the lower half
motor apply traction to the cervical or lumbar spine of the bed to roll back and forth several inches on a
by means of harnesses attached to a patient’s head frame, eliminating the friction and permitting traction
or pelvic area. The traction force widens the inter- force to be transmitted directly to the lumbar region.
vertebral spaces, thus relieving nerve root compres-
sion by intervertebral disks and the associated pain Traction units usually have a timer to set treatment
and burning or tingling sensations in the neck, duration and automatically turn off the machine at the
shoulders, and arms (when the cervical spine is end of the treatment session; the units also have controls
involved) or in the back, buttocks, legs, and feet for adjusting cycling rate and the ratio of traction and
(when the lumbar spine is involved). relaxation. All units provide a method for adjusting the
traction force, which is usually calibrated in pounds.
Traction was traditionally provided with static
weights attached to a harness worn by a patient while Cervical traction units are typically wall mounted
immobilized in bed. Research has demonstrated that but can also be mounted overhead, on floor stands, or
considerably more force is required to widen interver- on standards associated with or integrated into special
tebral spaces than can be provided with such a system; chairs. Lumbar traction units may be integrated into
however, the required forces are too high to be toler- special beds or tables. Mobile, hydraulically powered
ated for long periods. Studies showed that intermit- units can be used with most beds or special tables.
tent or cycled traction provided sufficient, effective Universal models can be mounted overhead for cervi-
force but was relatively comfortable. Studies also cal traction or attached to a bed or special table for
proved that conventional traction applied with a pelvic either cervical or lumbar traction. The greatest safety
belt to the lumbar region of a patient lying in bed was problems are related to mounting security; ceiling- and
ineffective since friction of the lower half of the body wall-mounted units present the greatest hazard.
009089 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
427-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
Most of the hazards associated with powered units screws are used, verify that the stress is distrib-
involve mechanical safety. Machine components (e.g., uted to two or more studs. Molly bolts, plastic
cables, spreader bars, linkages, and scales that apply shield screws, wood screws, and direct mounting
and measure traction forces) have broken or separated on plaster or drywall are unacceptable.
from their mounts and fallen on patients. Improperly
secured mounts have caused entire machines to fall or Test the mounting integrity of vertically
topple, sometimes on patients. Foreign objects and mounted units by hanging a 100 lb weight from
clothing have been caught in moving parts, and fingers the patient cable or lever several inches above
have been pinched. the floor for 5 min, and examine mounts, fix-
tures, welds, and mounting surfaces for stress.
Test apparatus and supplies While this test is under way, continue with the
remainder of the visual inspection, but do not
Ground resistance ohmmeter
stand or sit under the unit.
Leakage current meter or electrical safety analyzer
1.3 Casters/Brakes. If the device moves on casters,
Weights (five 10 lb, one 50 lb), accurate to at least
check their condition. Check the operation of
5% and a connector for attaching them to the trac-
brakes and swivel locks, if the unit is so
tion unit
equipped.
100 lb spring scale or dynamometer, accurate to 5%
(for horizontally mounted units that cannot be re- 1.4 AC Plug. Examine the AC power plug for dam-
moved and mounted for testing in the vertical plane; age. Attempt to wiggle the blades to determine
optional for vertically mounted units) that they are secure. Shake the plug and listen
for rattles that could indicate loose screws. If
Stopwatch or watch with a second hand
any damage is suspected, open the plug and
Lubricants recommended by the manufacturer inspect it.
Procedure 1.5 Line Cord. Inspect the cord for signs of damage.
Before beginning an inspection, carefully read this If damage is present, replace the entire cord, or
procedure and the manufacturer’s instruction and if the damage is near one end, cut out the defec-
service manual; be sure you understand how to operate tive portion. Be sure to wire a new power cord
the equipment, the significance of each control and or plug with the correct polarity.
indicator, and the alarm capabilities. Also determine 1.6 Strain Reliefs. Examine the strain reliefs at
whether any special inspection or preventive mainte- both ends of the line cord. Be sure that they hold
nance procedures or frequencies are recommended by the cord securely.
the manufacturer.
1.7 Circuit Breaker/Fuse. If the device has a
1. Qualitative tests switch-type circuit breaker, check that it moves
1.1 Chassis/Housing. Examine the exterior of the freely. If the device is protected by an external
unit for cleanliness and general physical condi- fuse, check its value and type against that
tion. Be sure that plastic housings are intact, marked on the chassis, and ensure that a spare
that necessary assembly hardware is present fuse is provided.
and tight, and that there are no signs of spilled
1.13 Controls/Switches. Before moving any controls
liquids or other serious abuse. If required, clean
and alarm limits, check their positions. If any of
and lubricate (Items 3.1 and 3.2) at this time.
them appear inordinate, consider the possibility
1.2 Mount/Fasteners. Inspect the chassis and all of inappropriate clinical use or of incipient device
stress-bearing members. Carefully examine the failure. Record the settings of those controls
basic structure for evidence of undue stress, in- that should be returned to their original posi-
cluding metal fatigue; fractures; integrity of welds; tions following the inspection.
size, condition, and tightness of fasteners; condi-
Examine all controls and switches for physical
tion and characteristics of mounting substructure
condition, secure mounting, and correct motion.
(i.e., wall, backing board or plate, chair structure);
Where a control should operate against fixed-
and corrosion. Tighten loose fasteners.
limit stops, check for proper alignment, as well
Wall-mounted units should employ backing as positive stopping. Check membrane switches
plates to spread forces over a large area. If lag for membrane damage (e.g., from fingernails,
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Traction Units
pens). During the course of the inspection, be the grounding conductor temporarily opened.
sure to check that each control and switch per- Operate the unit in all normal modes, including
forms its proper function. on, standby, and off, and record the maximum
leakage current. Leakage current should not
1.15 Motor. Confirm physical condition and proper
exceed 300 µA.
operation. Perform lubrication, if required; note
this in Item 3.2 (but do not check until all neces- 2.3 Timer Accuracy. Check the timer accuracy with
sary lubrication has been completed). a stopwatch or a watch with a second hand. The
error should be less than 10%.
1.18 Indicators/Displays. During the course of the
inspection, confirm the operation of all lights, 2.10 Traction Control Accuracy. The machine should
indicators, meters, gauges, and visual displays deliver forces accurate to within 10% of the indi-
on the unit. Be sure that all segments of a digital cated value. Test vertically mounted traction
display function. units at 10, 50, and 100 lb by placing the appro-
priate weights on a chair under the unit and
1.20 Alarms. Test the activation of alarms, if so attaching them to a coupling device. Take into
equipped. account the weight of the weight carriers,
1.22 Labeling. Check that all necessary placards, la- spreader bar, and other parts that contribute to
bels, conversion charts, and instruction cards the total load. Set the machine’s force control to
are present and legible. the equivalent force in each case; set its controls
for hold (dwell) and rest times for 20 sec. The
1.23 Accessories. Carefully examine operating lev- machine should just lift each weight off the chair.
ers, cables, chains, ropes, and spreader bars used Many table-mounted traction units can be easily
to transfer the machine’s linear motion to the removed and clamped to the top of a door for
patient harness. Examine ropes for wear and testing in the vertical plane. Alternatively, they
fraying. Cables should be clean, free of corro- can be left in place and tested with a spring scale
sion, and without fishhooks or other evidence of or dynamometer. In either case, these units
broken strands, sharp bends, kinks, or unstrand- should also be tested at 10, 50, and 100 lb.
ing that would weaken the cable. Examine the Recalibrate the unit according to the manufac-
integrity of cable connections, whether splices, turer’s instructions, if necessary, and indicate
thimbles, press sleeves, or clevis or eye fittings. this on Line 3.3 of the inspection form.
Be sure that clevis or eye-fitting pins have cotter
pins or bolts with stop nuts to ensure security. 2.11 Intermittent Traction. Verify correct operation
Check S-hooks, chain links, and spreader bars when intermittent traction is selected, using the
for cracks, bends, and other evidence of weak- same test setup as in Item 2.10. The rope/cable
ness. Tighten, repair, or replace components as should slacken after 20 sec, setting the weight back
necessary. on the chair, or causing the spring scale/dyna-
mometer reading to fall to zero. After another
1.24 Patient Pendant Control. Examine the pendant period of 20 sec, the force should be resumed.
switch housing and its electrical cable and strain
relief for wear and damage. Check that the 3. Preventive maintenance
switch functions properly and that it overrides 3.1 Clean the exterior.
all other on/off switches and the treatment dura-
tion timer. 3.2 Lubricate the gearboxes, cams, and motor ac-
cording to the manufacturer’s instructions.
2. Quantitative tests
3.3 Calibrate, if necessary.
2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with 4. Acceptance tests
good resolution of fractional ohms, measure and
Conduct major inspection tests for this procedure
record the resistance between the grounding pin
and the appropriate tests in the General Devices Pro-
of the power cord and exposed (unpainted and
cedure/Checklist 438.
not anodized) metal on the chassis. We recom-
mend a maximum of 0.5 Ω. Before returning to use
2.2 Leakage Current. Measure chassis and patient Return controls to their preinspection or normal
pendant control leakage current to ground with pre-use settings.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Procedure/Checklist 453-0595
Transcutaneous O2/CO2 Monitors
Used For:
Carbon Dioxide Monitors, Transcutaneous [15-970]
Oxygen Monitors, Transcutaneous [12-592]
Commonly Used In: NICUs
Scope: Applies to devices that assess blood gas levels noninvasively from a skin-surface probe
Risk Level: ECRI Recommended, High; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months month . hours
Minor NA month . hours
Overview Citations from Health Devices
Transcutaneous carbon dioxide (tcpCO2) and oxygen Transcutaneous oxygen monitors [Evaluation], 1983
(tcpO2) monitors provide noninvasive methods for Jul-Aug; 12:213-51.
measuring the partial pressure of carbon dioxide and
oxygen at the skin surface. These measurements are
not always equal to the arterial partial pressure of Test apparatus and supplies
carbon dioxide (paCO2) and oxygen (paO2), but they
Leakage current meter or electrical safety analyzer
can be useful indicators of changes in these values.
Ground resistance ohmmeter
Transcutaneous monitoring is done primarily on
infants in the neonatal intensive care unit (NICU). Manufacturer’s recommended calibration equip-
Since these infants often experience respiratory dis- ment
tress, tcpO2 monitoring is critical for avoiding hypox-
Water bath or manufacturer’s patient simulator
emia (low paO2, which can lead to brain damage) and
hyperoxemia (high paO2, which can cause blindness).
Persistent hypercapnia (high paCO2) in the infant may Procedure
indicate potentially life-threatening pulmonary com-
plications. Hypocapnia (low paCO2) might be sympto- Before beginning an inspection, carefully read this
matic of infantile asthma or of a pulmonary embolism procedure and the manufacturer’s instruction and
limiting blood flow to the lungs; it might also result service manuals; be sure that you understand how to
from mechanical overventilation of the lungs, which operate the equipment, the significance of each control
creates an excessive minute respiratory volume (i.e., and indicator, and the alarm capabilities. Also deter-
the volume of new air moving into the lungs each mine whether any special inspection or preventive
minute). Prenatally, tcpO2 measurements can also maintenance procedures or frequencies are recom-
monitor maternal and fetal oxygenation. mended by the manufacturer.
084828 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
453-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
1. Qualitative tests 1.11 Probes. Confirm that any necessary probes are
on hand and check their physical condition.
1.1 Chassis/Housing. Examine the exterior of the
1.13 Controls/Switches. Before changing any con-
unit for cleanliness and general physical condi-
trols or alarm limits, check their positions. If
tion. Be sure that plastic housings are intact,
any settings appear inordinate (e.g., a gain con-
that all hardware is present and tight, and that
trol at maximum, alarm limits at the ends of
there are no signs of spilled liquids or other
their range), consider the possibility of inappro-
serious abuse.
priate clinical use or of incipient device failure.
1.2 Mount/Fasteners. If the device is mounted on a Record the settings of those controls that should
stand or cart, examine the condition of the be returned to their original positions following
mount. If it is attached to a wall or rests on a the inspection.
shelf, check the security of this attachment. Examine all controls and switches for physical
condition, secure mounting, and correct motion.
1.4 AC Plug. Examine the AC power plug for damage.
Check that control knobs have not slipped on
Attempt to wiggle the blades to check that they are
their shafts. Where a control should operate
secure. Shake the plug and listen for rattles that
against fixed-limit stops, check for proper align-
could indicate loose screws. If any damage is sus-
ment, as well as positive stopping. Check mem-
pected, open the plug and inspect it.
brane switches for membrane damage (e.g., from
1.5 Line Cord. Inspect the cord for signs of damage. fingernails, pens). During the course of the in-
If damaged, replace the entire cord, or, if the spection, be sure to check that each control and
damage is near one end, cut out the defective switch performs its proper function.
portion. Be sure to wire a new power cord or plug 1.17 Battery/Charger. Inspect the physical condi-
with the correct polarity. Also check line cords of tion of batteries and battery connectors if readily
battery chargers. accessible. Check operation of battery-operated
power-loss alarms, if so equipped. Operate the
1.6 Strain Reliefs. Examine the strain reliefs at
unit on battery power for several minutes to
both ends of the line cord. Be sure that they hold
check that the battery is charged and can hold a
the cord securely. If the line cord is detachable
charge. (The inspection can be carried out on
(by the user), we recommend that the cord be
battery power to help confirm adequate battery
affixed to the unit so that it cannot be removed
capacity.) Check battery condition by activating
by the operator. (See Health Devices 1993 May-
the battery test function or measuring the out-
Jun; 22:301-3.)
put voltage. Check the condition of the battery
1.7 Circuit Breaker/Fuse. If the device has a charger and, to the extent possible, confirm that
switch-type circuit breaker, check that it moves it does, in fact, charge the battery. Be sure that
freely. If the device is protected by an external the battery is recharged or charging when the
fuse, check its value and type against that inspection is complete. When it is necessary to
marked on the chassis and ensure that a spare replace a battery, label it with the date.
is provided. 1.18 Indicators/Displays. During the course of the
1.9 Cables. Inspect probes and their strain reliefs for inspection, confirm the operation of all lights,
general condition. Carefully examine cables to indicators, meters, gauges, and visual displays
detect breaks in the insulation and to ensure that on the unit and charger (if so equipped). Be sure
they are gripped securely in the connectors at that all segments of a digital display function.
each end to prevent rotation or other strain. Observe a signal on a CRT display, if present,
Verify that there are no intermittent faults by and check its quality (e.g., distortion, focus, 60
flexing electrical cables near each end and look- Hz noise).
ing for erratic operation or by using an ohmmeter. 1.19 User Calibration. Verify that the calibration
function operates.
1.10 Fittings/Connectors. Examine all electrical
connectors for general condition. Electrical con- 1.20 Alarms. Induce alarm conditions with each pro-
tact pins or surfaces should be straight, clean, cedure below, and verify that the unit operates
and bright. Verify that probe leads are firmly properly and activates an audible and visual
gripped in their appropriate connectors. alarm for each alarm limit that has been exceeded.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Transcutaneous O2/CO2 Monitors
If the unit has an alarm-silence feature, check the insulated, grounding resistance need not be
method of reset (i.e., manual or automatic) against measured; indicate “DI” instead of the ground
the manufacturer’s specifications. Verify that re- resistance value.
set silenced alarms reactivate within the manufac-
turer’s specified time. It may not be possible to 2.2 Leakage Current. Measure chassis leakage cur-
check out all alarms at this time, since some may rent to ground with the grounding conductor of
require abnormal operating conditions that will be plug-connected equipment temporarily opened.
simulated later in this procedure. Operate the device in all normal modes, includ-
ing heater on and off, standby, and off, and
Gas concentration alarms. Set the high- and record the maximum leakage current.
low-concentration alarm limits so that they
are exceeded when the probe is exposed to Chassis leakage current to ground should be
either ambient air or an exhaled breath. The 300 µA or less.
sensor may have to be exposed to a zero gas
(e.g., N2) to activate the low tcpO2 alarm. 2.3 Temperature Control. If a patient simulator is
Observe alarms. available from the manufacturer, secure the
probe to the simulator. If a simulator is not
Site-timer alarm. Verify that the site timer is
available, a water bath can be used to simulate
operational and activates an alarm.
the patient’s skin temperature. Select a com-
Other alarms. If the unit indicates any other monly used set-point temperature on the moni-
alarm condition, induce the alarm and verify tor. With the simulator temperature initially set
that the alarm condition is indicated by the at 30°C, verify that the heater indicator shows
unit. that the heater is on. Increase the temperature
of the simulator. When the simulator tempera-
1.21 Audible Signals. Operate the device to activate ture reaches the set-point temperature (within
any audible signals. Confirm appropriate vol- 0.1°C), the heater indicator should be off.
ume, as well as the operation of a volume control,
if so equipped. If audible alarms have been si- 2.4 Temperature Display Accuracy. The surface
lenced or the volume set too low, alert clinical temperature display should be within 0.1°C of
staff to the importance of keeping alarms at the the simulator temperature. Record the simula-
appropriate level. tor temperature and the displayed temperature
on the inspection form.
1.22 Labeling. Check that all necessary placards, la-
bels, conversion charts, and instruction cards 2.5 High-Temperature Alarm. Using the test de-
are present and legible. scribed in Item 2.3, continue to increase the
1.23 Accessories. Confirm the presence of probe ap- simulator temperature; the high-temperature
plication kits. alarm should activate when the simulator tem-
perature exceeds the set point by 0.5°C.
1.24 Chart Recorder. If the unit has a chart recorder,
confirm that it operates smoothly, that the paper 2.6 Low-Temperature Alarm. Detach the probe
feeds evenly and does not stray from side to side, from a simulator that has heated to the unit’s set
and that the trace is of good quality at all paper temperature, and verify that the low-tempera-
speeds. The trace should be dark and thin. ture alarm activates when the displayed tem-
perature is 0.5°C below the set temperature.
2. Quantitative tests
2.7 tcpO2 Display Accuracy. Expose the probe to
2.1 Grounding Resistance. Using an ohmmeter, calibration gas containing O2 and verify that the
electrical safety analyzer, or multimeter with display is within ±5 mm Hg or 10%, whichever is
good resolution of fractional ohms, measure and greater, of the actual concentration. If the dis-
record the resistance between the grounding pin play is inaccurate, calibrate the unit.
of the power cord and exposed (unpainted and
not anodized) metal on the chassis. We recom- 2.8 tcpCO2 Display Accuracy. Expose the probe to
mend a maximum of 0.5 Ω. If the system is calibration gas containing CO2 and verify that
modular or composed of separate components, the display is within ±5 mm Hg or 10%, which-
verify grounding of the mainframe and each ever is greater, of the actual concentration. If the
module or component. If the device is double display is inaccurate, calibrate the unit.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
3. Preventive maintenance 4. Acceptance tests
Conduct major inspection tests for this procedure
3.1 Clean the exterior, interior, chart recorder, and and the appropriate tests in the General Devices Pro-
rollers if needed and the probe if recommended. cedure/Checklist 438.
3.2 Lubricate the chart recorder paper drive per Before returning to use
manufacturer’s instructions. Make sure that all controls are set properly. Set
alarms loud enough to alert personnel in the area in
3.3 Calibrate according to the manufacturer’s rec- which the device will be used. Other controls should
ommended procedure. be in their normal pre-use positions.
3.4 Replace filter, printer paper, battery, and cali- Recharge battery-powered devices or equip with
bration gas tanks, if needed. fresh batteries, if needed.
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Procedure/Checklist 474-0595
Ultrasound Scanners
Used For:
Scanners, Ultrasonic, Abdominal [16-241]
Scanners, Ultrasonic, Cardiac [17-422]
Scanners, Ultrasonic, Dedicated Linear Array [16-747]
Scanners, Ultrasonic, General-Purpose [15-976]
Scanners, Ultrasonic, Intravascular [17-746]
Scanners, Ultrasonic, Mammographic [15-656]
Scanners, Ultrasonic, Obstetric/Gynecologic [15-657]
Scanners, Ultrasonic, Ophthalmic [11-389]
Scanners, Ultrasonic, Small-Parts [18-052]
Scanners, Ultrasonic, Vascular [15-957]
Also Called: Real-time scanners, 2-D scanners, duplex scanners, echocardiographs, cardiac ultrasound
imagers, vascular ultrasound imagers
Commonly Used In: Cardiology, diagnostic imaging, OB/GYN, ophthalmology, radiology, surgery, vascular lab
Scope: This procedure covers all diagnostic ultrasound scanners, including general-purpose and dedicated
systems; this procedure does not cover nonimaging diagnostic ultrasound systems such as Doppler blood-flow
detectors and Doppler fetal heart monitors
Risk Level: ECRI Recommended, Medium; Hospital Assessment,
ECRI-Recommended Interval Used
Type Interval By Hospital Time Required
Major 12 months* months . hours
Minor NA months . hours
* Scanners with a mechanically steered transducer should probably be inspected semiannually. It is also
necessary to perform Items 2.3 to 2.8/2.9 whenever a new or repaired transducer is to be used.
Overview vibrations that require a medium for transmission.
Because they exhibit the normal wave properties of
Ultrasound scanners provide 2-D images of soft tissue reflection, refraction, and diffraction, they can be pre-
for abdominal, obstetric/gynecologic, cardiac, small- dictably aimed, focused, and reflected. Echoes are pro-
parts, and vascular examinations. With specially de- duced whenever the beam encounters an interface of
signed probes, they can also be used for intravascular different acoustic impedances, such as the soft-tissue/
and intraoperative applications. bone interface. Large differences in tissue acoustic
impedance characteristics result in a high degree of
Ultrasound refers to sound waves emitted at fre- reflection.
quencies above the level of human hearing. For diag-
nostic imaging, frequencies ranging from 2 to 10 MHz A transducer, which consists of one or more piezo-
are typically used. Ultrasound waves are mechanical electric elements, is placed on the skin after an acoustic
238196 5200 Butler Pike, Plymouth Meeting, PA 19462-1298, USA
474-0595 Telephone +1 (610) 825-6000 ● Fax +1 (610) 834-1275 ● E-mail info@ecri.org
A NONPROFIT AGENCY
Inspection and Preventive Maintenance System
coupling gel is applied. The transducer converts an Test apparatus and supplies
electrical signal into ultrasonic energy that can be
transmitted into tissues. When this ultrasonic energy Multipurpose ultrasound phantom (see Specifica-
is reflected back from the tissues, the transducer re- tions for a Multipurpose Ultrasound Phantom)
converts it to an electrical signal. The scanner system
Doppler ultrasound phantom (required only for a
measures the intensity of the echoes, the time between
comprehensive evaluation of ultrasound scanners
them, and their direction. This information is then
that have Doppler capabilities; see Specifications
processed and used to generate a display in one of
for a Doppler Ultrasound Phantom)
several modes. A scan converter system displays the
image on a high-resolution TV monitor. During scan- Blood flow simulator (required if only the basic
ning, the converter assigns discrete shades of gray operation of ultrasound scanners with Doppler is
(gray scale) to the returning echo amplitude levels; the being checked; see Specifications for a Doppler Ul-
number of shades depends on how many bits of infor- trasound Phantom)
mation can be stored for each horizontal and vertical ECG simulator (required for cardiology ultrasound
point of image memory. Some scanners offer user-se- systems or general-purpose systems with cardiac
lectable preprocessing and postprocessing features options)
that permit the operator to optimize the image quality
by altering the texture and gray-scale emphasis within Leakage current meter or electrical safety analyzer
the image. Ground resistance ohmmeter
A data-entry keyboard permits information, such as
patient name, date, and type of study, to be entered Specifications for a multipurpose ultrasound
and displayed along with the scanned image. In some phantom
systems, an alphanumeric keyboard interacts with a
computer to permit manipulation of the displayed im- A multipurpose phantom is required to comprehen-
age or system operating parameters. In cardiac and sively evaluate the performance of diagnostic ultra-
vascular studies, the Doppler effect is used to deter- sound imaging systems. Some multipurpose phantoms
mine the direction and speed of blood flow. This prin- do not contain all of the recommended capabilities. To
ciple states that sound waves increase in frequency evaluate both general-purpose and small-parts scan-
when they echo from objects (in this case, red blood ners, it may be necessary to acquire more than one
cells) moving toward the transducer and decrease in phantom to perform all of the recommended tests.
frequency when they echo from objects moving away General testing capabilities of the phantom should
from it. This change in frequency, which is related to include:
the velocity of the moving red blood cells, is then
measured and used to determine blood flow velocity. Dead-zone or ring-down
Vertical and horizontal measurement calibration
Doppler color flow mapping (CFM) simultaneously
assesses the direction and relative velocity of blood flow Focal zone
at multiple points along multiple beam paths. The
Sensitivity
result is an image of the hemodynamics of the heart and
great vessels, which is useful for detecting stenoses and Axial and lateral resolution
valve defects. As conventional 2-D real-time techniques
Functional resolution
display the heart’s anatomic features in black and
white, color superimposed on this image visually de- Gray scale and displayed dynamic range
picts the direction and velocity of blood flow. CFM
complements and enhances the diagnostic value of con- The phantom should be designed with a combina-
ventional 2-D real-time images; it also provides more tion of monofilament line targets and tissue-mimick-
information about and enables better quantification of ing cylindrical targets of varying sizes and contrasts.
the direction and velocity of blood flow abnormalities. The monofilament line targets should have a diameter
of 0.1 mm to 0.5 mm to optimize the displayed image
at frequencies typically used on general-purpose scan-
Citations from Health Devices ners. Monofilament line targets with diameters of ap-
proximately 0.5 mm should be present to optimize the
Duplex ultrasound scanners [Evaluation], 1990 Nov; displayed image at the high ultrasound frequencies
19:379-422. typically used on small-parts scanners.
Inspection and Preventive Maintenance System
2 ©1995 ECRI. All Rights Reserved.
Ultrasound Scanners
For dead-zone or ring-down evaluation, at least 6 Specifications for a Doppler ultrasound
monofilament line targets should be present at depths phantom
ranging from 2 mm to 10 mm.
A calibrated Doppler flow phantom is required for a
For vertical distance measurement calibration, the comprehensive evaluation of ultrasound scanners that
monofilament line targets should have an interval incorporate continuous-wave, pulsed-wave, or color-
spacing of 1 cm at a depth of 1 cm to a total depth of at flow Doppler capabilities. Some Doppler phantoms are
least 18 cm. To evaluate small-parts scanners, an designed specifically for evaluating either peripheral
interval spacing of 0.5 cm is recommended. vascular or cardiac systems.
For horizontal distance measurement calibration, General testing capabilities of the phantom should
the monofilament line targets should have an interval include:
spacing of 1 or 2 cm. To evaluate small-parts scanners, Flow velocity
an interval spacing of 0.5 cm is recommended. Targets Location of flow
should be available at more than one depth for accu-
rate determination of horizontal distance measure- Directional discrimination
ment calibration. The phantom can be either the tissue-mimicking
type with one or more fluid-flow channels (containing
For axial and lateral resolution evaluation, multiple
a nondegradeable blood-mimicking solution with cali-
monofilament line targets are required with interval
brated reflecting targets) or the type that incorporates
spacings of 1 mm, 2 mm, 3 mm, 4 mm, and 5 mm or
a moving string target within a fluid-filled container.
less. To evaluate small-parts scanners, the smaller
The string phantom provides greater accuracy for flow
interval space should be 0.5 mm or less. Targets should
velocity calibration.
be available at more than one depth to properly evalu-
ate lateral resolution. For peripheral vascular system evaluation, the
target(s) within the phantom should move parallel
The phantom should contain multiple anechoic to the phantom’s scanning surface (perpendicular to
(nonechogenic) cylindrical target structures of varying the transducer’s beam path). For cardiac system
sizes from 2 mm to at least 6 mm. Anechoic target evaluation, the target(s) within the phantom should
structures with a 1 mm diameter are recommended move at an angle of approximately 45° to the phan-
when evaluating ultrasound scanners that are rou- tom’s scanning surface. Although not optimum,
tinely used for small parts. phantoms designed specifically for cardiac system
evaluation can be used to evaluate peripheral vascu-
The phantom should contain multiple gray-scale lar systems.
(echogenic) cylindrical targets, calibrated in decibels
(dB), to evaluate the displayed dynamic range and The phantom should provide user-variable velocity
gray-scale processing performance. of the moving target(s).
To check only basic Doppler operation, it is not
The phantom should be constructed of a tissue-mim-
necessary to use the calibrated Doppler phantoms
icking material with a recommended attenuation coef-
described above. A less-costly blood-flow simulator
ficient of 0.5 dB/cm/MHz or 0.7 dB/cm/MHz.
may be purchased, or one may be constructed using a
fluid pump and flexible tubing submerged within a
The velocity calibration of the tissue-mimicking ma-
fluid-filled container. In lieu of the nondegradeable
terial should be 1,540 meters per second.
blood-mimicking solution with calibrated reflecting
targets, any echogenic fluid, such as a detergent-water
The dimensions of the scanning surface should be
solution, may be used.
sufficiently large to permit evaluation of the longest
flat linear-array transducer.
Procedure
The phantom should be contained in a protective Before beginning an inspection, carefully read
housing. A built-in scanning well is recommended to this procedure and the manufacturer’s instruction
permit the use of water or a low-viscosity gel as the and service manuals; be sure that you understand
coupling agent. A deep scanning well, either built-in or how to operate the equipment and the significance of
removable, is recommended for proper evaluation of each control and indicator. Also determine whether
some endoscanning transducers. any special inspection or preventive maintenance
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 3
Inspection and Preventive Maintenance System
procedures or frequencies are recommended by the 1.8 Cables. Inspect any cables (e.g., transducer, elec-
manufacturer. This procedure should be documented trode, remote control) and their strain reliefs for
with the ultrasound scanners inspection form no. 474. general condition. Carefully examine cables to de-
tect breaks in the insulation and to ensure that
1. Qualitative tests they are gripped securely in the connectors at each
1.1 Chassis/Housing. Examine the exterior of the end to prevent rotation or other strain. Verify that
unit for cleanliness and general physical condition. there are no intermittent faults by flexing electri-
Be sure that plastic housings are intact, that all cal cables near each end and looking for erratic
hardware is present and tight, and that there are operation or by using an ohmmeter.
no signs of spilled liquids or other serious abuse. 1.9 Fittings/Connectors. Examine all electrical cable
1.2 Mount/Fasteners. If the device is mounted on a connectors for general condition. Electrical contact
stand or cart, examine the condition of the pins or surfaces should be straight, clean, and
mount. If it rests on a shelf, check the security of bright. Verify that leads and electrodes are firmly
this attachment. gripped in their appropriate connectors. If keyed
connectors are used, make sure that no pins are
1.3 Casters/Brakes. If the device moves on casters, missing and that the keying is correct.
check their condition. Verify that they turn and
swivel, as appropriate, and look for accumula- 1.10 Transducers. Check the surface areas of ultra-
tions of lint and thread around the casters. sound transducers for deterioration, cracks, or
Check the operation of brakes and swivel locks, dents in the membrane. Check the acoustic fluid
if the unit is so equipped. Conductivity checks, of mechanically steered transducers; refill with
where appropriate, are usually done more effi- the recommended fluid if air bubbles are present
ciently as part of a check of all equipment and and indicate this in section 3 of the inspection
furniture in an area. form.
1.4 AC Plug/Receptacles. Examine the AC power 1.11 Filters. Check the condition of all air vents and
plug for damage. Attempt to wiggle the blades to filters. Clean or replace filters, if appropriate, and
check that they are secure. Shake the plug and indicate this in section 3 of the inspection form.
listen for rattles that could indicate loose screws.
1.12 Controls/Switches. Before changing any controls,
If any damage is suspected, open the plug and
check their positions. If any settings appear inor-
inspect it.
dinate (e.g., a gain control at maximum), consider
If the device has electrical receptacles for acces- the possibility of inappropriate clinical use or of
sories, verify the presence of line power, and insert incipient device failure. Record the setting of those
an AC plug into each and check that it is held controls that should be returned to their original
firmly. If accessories are plugged and unplugged positions following the inspection.
often, consider a full inspection of the receptacles.
Examine all controls and switches for physical
1.5 Line Cord. Inspect the cord for signs of damage. condition, secure mounting, and correct motion.
If damaged, replace the entire cord or, if the Check that control knobs have not slipped on their
damage is near one end, cut out the defective shafts. Where a control should operate against
portion. Be sure to wire a new power cord or plug fixed-limit stops, check for proper alignment, as
with the correct polarity. well as positive stopping. During the course of the
inspection, be sure to check that each control and
1.6 Strain Reliefs. Examine the strain reliefs at switch performs its proper function.
both ends of the line cord. Be sure that they hold
the cord securely. If the line cord is detachable 1.13 Fans. Check the physical condition and proper
(by the user), affix the cord to the unit so that it operation of the system’s cooling fan(s), if present.
cannot be removed by the operator. (See Health Clean and lubricate the fan(s) if required, and note
Devices 1993 May-Jun; 22:301.) this in Items 3.1 and 3.2 of the inspection form.
1.7 Circuit Breaker/Fuse. If the device has a switch- 1.14 Indicators/Displays. During the course of the
type circuit breaker, check that it moves freely. If inspection, confirm the operation of all lamps,
the device is protected by an external fuse, check its indicators, meters, gauges, and visual displays
value and type against that marked on the chassis, on the unit. Be sure that all segments of a digital
and ensure that a spare is provided. display function. Observe an image on the CRT
Inspection and Preventive Maintenance System
4 ©1995 ECRI. All Rights Reserved.
Ultrasound Scanners
display, and check its quality (e.g., distortion, All portions of a simulated ECG waveform
focus, 60 Hz noise). Record the reading of an hour should be clearly visible, including the P wave
meter, if present. and QRS complex.
1.15 User Calibration. Verify that any calibration 60 Hz noise should not be present.
functions are operating. (Where a quantitative The accuracy of intervals between the timing
check is required, it will be included in Section marks displayed by the scanner should be con-
2, Quantitative Tests.) sistent with the timing of the ECG simulator.
1.16 Audible Signals. Operate the device to activate 1.20 Accessories. Confirm the presence and condition
any audible signals. Confirm appropriate vol- of accessories (e.g., electrodes and coupling gel).
ume, as well as the operation of a volume control, Verify that expiration dates have not been ex-
if so equipped. ceeded.
1.17 Labeling. Check that all necessary placards, la- 2. Quantitative tests
bels, conversion charts, and instruction cards
are present and legible. 2.1 Grounding Resistance. Using an ohmmeter,
electrical safety analyzer, or multimeter with
1.18 System Performance. Use the multipurpose ul- good resolution of fractional ohms, measure and
trasound phantom to evaluate the overall perform- record the resistance between the grounding pin
ance of the scanner. Use the test object’s multiple of the power cord and exposed (unpainted and not
gray-scale (echogenic) targets to evaluate the dis- anodized) metal on the chassis. We recommend a
played dynamic range and gray-scale processing maximum of 0.5 Ω. If the system is modular or
performance. Use the multiple anechoic (nonecho- composed of separate components, verify ground-
genic) cylindrical targets to observe the absence of ing of the mainframe and each module or compo-
echogenicity. The anechoic target should be clearly nent. If the device is double insulated, grounding
resolved. Higher-frequency transducers should resistance need not be measured; indicate “DI”
produce the clearest images of the smaller instead of the ground resistance value.
anechoic targets. Using normal gain and output
power settings, check for sensitivity/penetration If the device has an accessory receptacle,
relative to the frequency of the transducer being check its grounding to the main power cord.
used. (See the table below.) 2.2 Leakage Current. Measure chassis leakage cur-
rent to ground with the grounding conductor of
plug-connected equipment temporarily opened.
Typical sensitivity/penetration of a multipurpose
Operate the device in all normal modes, includ-
phantom
ing on, standby, and off, and record the maxi-
Transducer Frequency Penetration mum leakage current. (Many leakage current
1.9 MHz 20 cm meters cannot be used because of the high-cur-
2.3 MHz 18 cm
3.0 MHz 16 cm rent demands (e.g., greater than 10 amps) of the
3.5 MHz 15 cm larger, more complex ultrasound scanners.)
5.0 MHz 8 cm
7.5 MHz 5 cm Measure chassis leakage current to ground
10.0 MHz 3 cm with all accessories normally powered from the
same line cord connected and turned on and off.
Use a blood-flow simulator to check the basic This includes other equipment that is plugged
operation of the Doppler system, if installed. into the primary device’s accessory receptacles,
as well as equipment plugged into a multiple
1.19 ECG. Using an ECG simulator, verify normal outlet strip (“Waber strip”) so that all are
operation of ultrasound scanners configured for grounded through a single line or extension cord.
echocardiography, according to the following
Chassis leakage current to ground should not
criteria:
exceed 300 µA.
The baseline should have constant thickness; 2.3 Transducer Identification and Scanner Set-
it should be horizontal and not drift vertically. tings for Tests with the Multipurpose Ultra-
On systems equipped with a position control, sound Phantom. Before performing tests 2.4 to
check the range of movement. 2.8/2.9, record transducer identification and
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 5
Inspection and Preventive Maintenance System
instrument settings as noted in the table below 2.8 Horizontal Distance. Place the transducer over
for each transducer on the back of the ultrasound a horizontal distance calibration line target
scanners inspection form no. 474. Set the controls group. Use the scanner’s digital calipers and/or
for optimum penetration and image quality for marker grids to determine the accuracy of linear
each transducer to be tested. A picture or printout measurements perpendicular to the sound path.
should be made to document the image obtained On images produced by flat sequenced linear-ar-
with each transducer. Most equipment parame- ray transducers, check at 20 mm and 60 mm
ters will be displayed on these hard-copy record- measured distances, using any left to right loca-
ings. See Figure 1 for reference scanner images. tion. On images produced by sector transducers,
check at 20 mm and 60 mm measured distances,
Transducer Identification but at multiple left to right positions. If the
Type/Configuration transducer has adjustable transmit focus, perform
Serial No. measurements within the focal zone, if possible.
Frequency MHz
2.9 Doppler Calibration. If a calibrated Doppler ul-
Scanner Settings
trasound phantom is available, verify the accu-
Power dB
Gain dB racy of flow velocity, directional discrimination,
Dynamic Range dB and, if applicable, pulsed-Doppler gate position-
Preprocessing ing. Measurement parameters and display qual-
Postprocessing
Persistence ity should not vary between inspections with the
Transmit Focus cm same transducer configuration, scanner set-
Other: tings, and technique.
2.4 Dead Zone. Place the transducer over the dead 3. Preventive maintenance
zone line target group. Determine the minimum
3.1 Clean the scanner exterior, as well as the interior
distance (in mm) at which the scanner can re-
if needed. Use only manufacturer-approved solu-
solve individual structures.
tions on the scanning surfaces of transducers.
Clean the exterior and the interior of image record-
2.5 Axial Resolution. Place the transducer over one ing devices, including multi-image cameras, video
of the axial resolution line target groups. Deter- page printers, and videocassette recorders.
mine the minimum reflector separation (in mm)
along the axis of the transducer beam required 3.2 Lubricate moving parts, including wheels, cast-
to produce separate reflections. ers, and drawer slides.
3.3 Refill mechanically steered transducers with the
2.6 Lateral Resolution. Place the transducer over
recommended acoustic fluid if air bubbles are
each lateral resolution line target group. Deter-
present.
mine the minimum reflector separation (in mm)
perpendicular to the sound path needed to pro- 3.4 Clean air vents and or filters, if required.
duce discrete reflections. Because lateral resolu-
tion can vary with depth, multiple transducer 4. Acceptance tests
locations should be used. Record the lateral reso- Conduct major inspection tests for this procedure
lution for each depth checked. If the transducer and the appropriate tests in the General Devices
has adjustable transmit focus, verify its opera- Procedure/Checklist 438. In addition, perform the
tion and perform each lateral resolution meas- following test.
urement in the respective focal zone, if possible.
4.1 Record baseline image values determined in
2.7 Vertical Distance. Place the transducer over a items 2.4 to 2.8/2.9 for comparison with values
vertical distance calibration line target group. determined in subsequent inspections.
Use the scanner’s digital calipers and/or marker
grids to determine the accuracy of linear meas- Before returning to use
urements along the axis of the transducer beam Ensure that all controls are set properly. Controls
at 20 mm and 100 mm measured distances. should be in their normal pre-use positions.
Inspection and Preventive Maintenance System
6 ©1995 ECRI. All Rights Reserved.
Ultrasound Scanners
Scanning Surface Figure 1. Multipurpose Phantom line target groups
and corresponding scanner images (For Items 2.4 to
2.8)
A. Dead Zone: Nine line targets, positioned 2 mm thru
10 mm from the scanning surface.
B. Axial Resolution: Six line targets, positioned with 1 mm,
2 mm, 3 mm, 4 mm, and 5 mm separations.
C. Lateral Resolution: Six line targets, positioned with 1 mm,
2 mm, 3 mm, 4 mm, and 5 mm separations.
D. Vertical Distance: Eleven line targets, positioned with
10 mm separations.
E. Horizontal Distance: Seven line targets, positioned with
10 mm separations.
Image showing 4 mm dead zone, 1 mm axial resolution,
Image with all line target groups displayed. and 3 mm lateral resolution. See Items 2.4, 2.5, and 2.6.
Image showing normal vertical-distance calibration. See Image showing normal horizontal-distance calibration.
Item 2.7. See Item 2.8.
Inspection and Preventive Maintenance System
©1995 ECRI. All Rights Reserved. 7
You might also like
- Excel Lecture Notes3 PDFDocument45 pagesExcel Lecture Notes3 PDFSnehaKale100% (1)
- Medical Equipment MaintenanceDocument140 pagesMedical Equipment MaintenanceJehiel AlvarezNo ratings yet
- Medical Equipment PPM ChecklistDocument66 pagesMedical Equipment PPM ChecklistNana Yaw Owusu100% (1)
- Medical EquipmentDocument48 pagesMedical EquipmentKhalid Khassawneh100% (2)
- Maintenance of Oxygen FlowmeterDocument14 pagesMaintenance of Oxygen Flowmeterver_at_work100% (2)
- TD Isolette C2000 C2000eDocument212 pagesTD Isolette C2000 C2000eEco Aquiles100% (1)
- Checklist For BiomedDocument3 pagesChecklist For BiomedImtiaz Ahamed100% (1)
- Group 2I - Herman Miller Case AnalysisDocument7 pagesGroup 2I - Herman Miller Case AnalysisRishabh Kothari100% (1)
- For Calibration List - OrginalDocument62 pagesFor Calibration List - Orginaluttam khatriNo ratings yet
- Medical Equipment TroubleshootingDocument28 pagesMedical Equipment TroubleshootingNarendran Ravi83% (6)
- Ecg EkgDocument3 pagesEcg EkgrochimNo ratings yet
- Hospitals CSSDDocument72 pagesHospitals CSSDIwan HamzahNo ratings yet
- MED EquDocument9 pagesMED EquAmir100% (1)
- Erbe APC-300 ESU - Service ManualDocument87 pagesErbe APC-300 ESU - Service ManualDoru RazvanNo ratings yet
- Wood Plastic CompositesDocument12 pagesWood Plastic CompositesMadhusudhan SrinivasNo ratings yet
- Fairview Terminal PhaseII Expansion Project Report - Oct2012Document436 pagesFairview Terminal PhaseII Expansion Project Report - Oct2012NewsroomNo ratings yet
- Medical Equipment ManagementDocument334 pagesMedical Equipment Managementsavannah78100% (1)
- Management Review How To Rev1Document23 pagesManagement Review How To Rev1tony sNo ratings yet
- BME FMS PolicyDocument17 pagesBME FMS Policynaresh100% (1)
- Avocados in Love PatternDocument10 pagesAvocados in Love PatternTu Anh Nguyen100% (2)
- Anesthesia UnitsDocument75 pagesAnesthesia UnitsmohammedmadaniNo ratings yet
- Equipment Maintenance and UseDocument53 pagesEquipment Maintenance and UseRam Mohan S100% (1)
- Living From Truth A Manual For Masters of Long Enlightenment IntensivesDocument116 pagesLiving From Truth A Manual For Masters of Long Enlightenment IntensivesZeljko Zex Malinovic100% (1)
- Checklist For Bio-Medical Engineering in HospitalsDocument4 pagesChecklist For Bio-Medical Engineering in HospitalsSharia AttarNo ratings yet
- BMMP - Technical ManualDocument72 pagesBMMP - Technical ManualMurali Dathan100% (1)
- TR Biomedical Equipment Servicing NC IIDocument69 pagesTR Biomedical Equipment Servicing NC IIInternational Technology Center Inc100% (1)
- Attachment A-Medical Equipment Management Standards and RegulationsDocument54 pagesAttachment A-Medical Equipment Management Standards and RegulationsMichael100% (2)
- Module 3 Docket SystemDocument26 pagesModule 3 Docket SystemGinoong Kim GalvezNo ratings yet
- Medical Equipment Managment Manual DUKEDocument54 pagesMedical Equipment Managment Manual DUKELucila Figueroa Gallo100% (1)
- 258189r2 s9-Vpap-TX Clinical-Guide Glo EngDocument37 pages258189r2 s9-Vpap-TX Clinical-Guide Glo EngjamesmhebertNo ratings yet
- Maintenance Infusion Pump PDFDocument2 pagesMaintenance Infusion Pump PDFroydityanaziNo ratings yet
- Philips Heartstart MRX Defibrillator - Maintenance GuideDocument16 pagesPhilips Heartstart MRX Defibrillator - Maintenance GuideSergio Pérez100% (1)
- Pulmonetic LTV Ventilator - Service Manual OCR PDFDocument302 pagesPulmonetic LTV Ventilator - Service Manual OCR PDFSoluciones EspecializadasNo ratings yet
- Biomedical Department PlanDocument4 pagesBiomedical Department Planomar farooq33% (3)
- Doh Assessment ToolDocument96 pagesDoh Assessment TooleychceeNo ratings yet
- Heraeus Megafuge 8, Thermo Scientific SL8 Centrifuge - Service ManualDocument62 pagesHeraeus Megafuge 8, Thermo Scientific SL8 Centrifuge - Service Manualdescarteso50% (2)
- Planning Medical Device Management SRS PlaningDocument11 pagesPlanning Medical Device Management SRS PlaningRajesh KumarNo ratings yet
- 10 Protocol For Training On Medical Devices PDFDocument8 pages10 Protocol For Training On Medical Devices PDFChala DabalaNo ratings yet
- Cek List BiomedicDocument159 pagesCek List BiomedicIboedIstina100% (1)
- Calibration of Medical EquipmentDocument5 pagesCalibration of Medical EquipmentVer BautistaNo ratings yet
- CompreDocument53 pagesCompreGEr JrvillaruEl0% (3)
- Siaretron4000 960501 UE Rev1Document268 pagesSiaretron4000 960501 UE Rev1thsen100% (3)
- FMS 006-Medical Equipment Management ProgramDocument4 pagesFMS 006-Medical Equipment Management ProgramMohamed AttiaNo ratings yet
- MoH-JICA Medical Equipment Management Guidelines PDFDocument188 pagesMoH-JICA Medical Equipment Management Guidelines PDFNg'andu Kayunna DavidNo ratings yet
- Error Code Quick Guide Autoclave RunyesDocument4 pagesError Code Quick Guide Autoclave RunyesSinda MazouniNo ratings yet
- Maintain and Repair Simple Biomedical EquipmentsDocument83 pagesMaintain and Repair Simple Biomedical Equipmentsbereketab demmelash100% (1)
- HyBase 6100 - HyExtent-3 Operation Manual - 2.0 - (EN) PDFDocument52 pagesHyBase 6100 - HyExtent-3 Operation Manual - 2.0 - (EN) PDFstefany ramirez100% (2)
- Medical Equipment Maintenance Program Overview PDFDocument113 pagesMedical Equipment Maintenance Program Overview PDFFais Hamid100% (2)
- HCTGuide 4Document245 pagesHCTGuide 4mc11cmNo ratings yet
- Biomedical PPM PLANDocument3 pagesBiomedical PPM PLANEhsan alwafaa100% (2)
- Procedure For Service and Maintenance - AOCDocument3 pagesProcedure For Service and Maintenance - AOCMohamed EzzatNo ratings yet
- Biomedical Enggineering SOPDocument22 pagesBiomedical Enggineering SOPPranali MhatreNo ratings yet
- Proper Tagging of Medical Equipment 36072Document4 pagesProper Tagging of Medical Equipment 36072Salim AloneNo ratings yet
- Medical Equipment Management PlanDocument4 pagesMedical Equipment Management PlanShallaine MarieNo ratings yet
- 5 Protocol For Planned Preventive Maintenance PDFDocument7 pages5 Protocol For Planned Preventive Maintenance PDFChala Dabala100% (1)
- BME-04 Calibration of Biomedical EquipmentDocument2 pagesBME-04 Calibration of Biomedical EquipmentPAPPU RANJITH KUMARNo ratings yet
- Filmora KeyDocument3 pagesFilmora KeyMis50% (2)
- Biomedical Medical Equipment Key Performance Indicators (Kpi /QPS)Document4 pagesBiomedical Medical Equipment Key Performance Indicators (Kpi /QPS)Natasha Bhasin100% (8)
- Hospital Equipments PrecurmentDocument10 pagesHospital Equipments PrecurmentRashid UmerNo ratings yet
- Medical Devices - SOP 3 - Acceptance of Medical DevicesDocument6 pagesMedical Devices - SOP 3 - Acceptance of Medical DevicesCaalaa Dabalaa LamuuNo ratings yet
- Operation Manual: Impedance Audiometer AT235hDocument102 pagesOperation Manual: Impedance Audiometer AT235hmendezoswaldoNo ratings yet
- Biomedical MEDICAL EQUIPMENT INVENTORYDocument3 pagesBiomedical MEDICAL EQUIPMENT INVENTORYEhsan alwafaaNo ratings yet
- Preventive Maintenance Checklist DopplerDocument1 pagePreventive Maintenance Checklist DopplerHertia rusliNo ratings yet
- BME-05 Annual Maintenance ContractDocument1 pageBME-05 Annual Maintenance ContractPAPPU RANJITH KUMARNo ratings yet
- Allied Health-Ahp300-ManualDocument53 pagesAllied Health-Ahp300-Manualmaria jose rodriguez lopezNo ratings yet
- ALLI - AHP300 Ops Manual HJHJDocument54 pagesALLI - AHP300 Ops Manual HJHJThích chơi Liên QuânNo ratings yet
- Anesthesia Machine1Document9 pagesAnesthesia Machine1shoibyNo ratings yet
- تقديمDocument27 pagesتقديمas739562978No ratings yet
- CASELLA APEX2 - PRO - Air Sampling Solutions Handbook HB4071-03 ENGLISHDocument54 pagesCASELLA APEX2 - PRO - Air Sampling Solutions Handbook HB4071-03 ENGLISHekberg.joseNo ratings yet
- Impedanciometro Aplivox Otowave 102 - MsDocument29 pagesImpedanciometro Aplivox Otowave 102 - MsAnonymous dGFqrw5vONo ratings yet
- Resume Template & Cover Letter Bu YoDocument28 pagesResume Template & Cover Letter Bu YoatinnajahkamalasariNo ratings yet
- Writing A Parable (Grade 8)Document16 pagesWriting A Parable (Grade 8)JON-VIC FIGUEROANo ratings yet
- List of Staff - As On 25052021Document12 pagesList of Staff - As On 25052021Vismaya VineethNo ratings yet
- Makeup Artist Characteristics and QualitiesDocument5 pagesMakeup Artist Characteristics and QualitiesRizzia Lyneth SargentoNo ratings yet
- #6 Clinical - Examination 251-300Document50 pages#6 Clinical - Examination 251-300z zzNo ratings yet
- Prla 2 Set 1 Story - Friends For LifeDocument4 pagesPrla 2 Set 1 Story - Friends For Lifehilmann.ariffinnNo ratings yet
- Announcement PIR Kudus 2019Document2 pagesAnnouncement PIR Kudus 2019leiliaNo ratings yet
- 10 Multicast Zone Routing Protocol For Mobile Ad Hoc NetworksDocument6 pages10 Multicast Zone Routing Protocol For Mobile Ad Hoc NetworksakshusvgNo ratings yet
- Enable Root Access openSUSEDocument4 pagesEnable Root Access openSUSEAgung PambudiNo ratings yet
- Help For The W3C Markup Validation ServiceDocument10 pagesHelp For The W3C Markup Validation ServicetsbgyywaedmqNo ratings yet
- Lesson 1Document35 pagesLesson 1Irish GandolaNo ratings yet
- Mathematics Lesson 4 - 4 Digits Addition Worded With 0Document9 pagesMathematics Lesson 4 - 4 Digits Addition Worded With 0api-381088463No ratings yet
- All Progressive Circle Wise & Cadar Wise Summery Status 01-03-2024Document25 pagesAll Progressive Circle Wise & Cadar Wise Summery Status 01-03-2024vivekNo ratings yet
- Mitsubishi Forklift Edr13n 24v Esr18n 24v Esr20n 24v Ess15n 24v Ess20n 24v Operation Maintenance Manual enDocument23 pagesMitsubishi Forklift Edr13n 24v Esr18n 24v Esr20n 24v Ess15n 24v Ess20n 24v Operation Maintenance Manual enmichellejackson130187gcq100% (125)
- Grundfos - SL1 50 65 22 2 50D CDocument13 pagesGrundfos - SL1 50 65 22 2 50D CThilina Lakmal Edirisingha100% (1)
- Vulvovaginal InfectionDocument66 pagesVulvovaginal InfectionRadhika BambhaniaNo ratings yet
- 500kVA Dyn5Document1 page500kVA Dyn5edwardNo ratings yet
- Difference Between ISO-IEC 17025 and ISO 10012Document3 pagesDifference Between ISO-IEC 17025 and ISO 10012carlosalejo100% (1)
- Clinical Understanding of The Sign "Blue Sclera" in Some CasesDocument4 pagesClinical Understanding of The Sign "Blue Sclera" in Some CasesDr. Bikash BiswasNo ratings yet
- 2 EEE - EPM412 Load CCs 2Document30 pages2 EEE - EPM412 Load CCs 2Mohamed CHINANo ratings yet