You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Pembimbing Koas Bedah Periode 1 MaretDocument6 pagesPembimbing Koas Bedah Periode 1 MaretTri SulistiyawatiNo ratings yet
- By Kate Scarlata MPH, RDN, FODMAP & IBS Expert: FruitDocument1 pageBy Kate Scarlata MPH, RDN, FODMAP & IBS Expert: FruitTri SulistiyawatiNo ratings yet
- This Grocery List Was Developed by Kate Scarlata, MPH, RDN and Fody Food CoDocument1 pageThis Grocery List Was Developed by Kate Scarlata, MPH, RDN and Fody Food CoTri SulistiyawatiNo ratings yet
- RPF - Low FODMAP Guide - 2nd EdDocument17 pagesRPF - Low FODMAP Guide - 2nd EdTri Sulistiyawati100% (1)
- RPF FoodGuide Print v.2-smDocument4 pagesRPF FoodGuide Print v.2-smTri SulistiyawatiNo ratings yet
- The Open Dermatology JournalDocument6 pagesThe Open Dermatology JournalTri SulistiyawatiNo ratings yet
- The Open Dermatology Journal: 0.1MG/ML Tamoxifen Gel Improves Plaque Psoriasis. An Open StudyDocument5 pagesThe Open Dermatology Journal: 0.1MG/ML Tamoxifen Gel Improves Plaque Psoriasis. An Open StudyTri SulistiyawatiNo ratings yet
- The Open Dermatology JournalDocument7 pagesThe Open Dermatology JournalTri SulistiyawatiNo ratings yet
- The Headaches and Polymorphisms of The Methylenetetrahydrofolate ReductaseDocument5 pagesThe Headaches and Polymorphisms of The Methylenetetrahydrofolate ReductaseTri SulistiyawatiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Peritonsillar AbscessDocument2 pagesPeritonsillar AbscessKevin Leo Lucero AragonesNo ratings yet
- Lean Body DietDocument68 pagesLean Body DietManiraj PalanikaniNo ratings yet
- Epidemiology, Health Policy and PlanningDocument18 pagesEpidemiology, Health Policy and PlanningMorgen Pangaila100% (1)
- Effective Versus Successful Managerial Activities Fred Luthans andDocument20 pagesEffective Versus Successful Managerial Activities Fred Luthans andSsssNo ratings yet
- Elimination DisordersDocument30 pagesElimination DisordersFaridatul IsniyahNo ratings yet
- What Is Gastroparesis?Document8 pagesWhat Is Gastroparesis?Naseeb Khoury100% (1)
- Gordon's 11 Functional PatternDocument2 pagesGordon's 11 Functional PatternFatima JubailNo ratings yet
- Chart Notes-Megan JolmaDocument5 pagesChart Notes-Megan Jolmaapi-317575833No ratings yet
- Adime Note GDMDocument2 pagesAdime Note GDMapi-242547654100% (1)
- Auditing E-Commerce Platforms For Algorithmically Curated Vaccine MisinformationDocument27 pagesAuditing E-Commerce Platforms For Algorithmically Curated Vaccine MisinformationNafisa SadafNo ratings yet
- 10 Penyakit Terbanyak JKN 2016Document2 pages10 Penyakit Terbanyak JKN 2016RSUD dr. H. Soemarno Sosroatmodjo Kuala KapuasNo ratings yet
- Gsa Notes PDFDocument35 pagesGsa Notes PDFhasanNo ratings yet
- LIIFT4 WorkoutDocument1 pageLIIFT4 Workoutlinsims0% (1)
- Person-Centered Medication Study: HypertensionDocument3 pagesPerson-Centered Medication Study: HypertensionAshley Mapusao (imgorgash)No ratings yet
- National Guidelines For Lab Testing and Reporting On Resp Infectious Diseases Ghana - 2 PDFDocument18 pagesNational Guidelines For Lab Testing and Reporting On Resp Infectious Diseases Ghana - 2 PDFHenry OseiNo ratings yet
- Sem 8 Thesis Topic-Final Assignment 21Document1 pageSem 8 Thesis Topic-Final Assignment 21Romi MewadaNo ratings yet
- Empirical Validation of Operations Strategy FrameworkDocument15 pagesEmpirical Validation of Operations Strategy FrameworkSaayantan RoyNo ratings yet
- The AAS Personal StatementDocument3 pagesThe AAS Personal StatementRetno Suminar100% (3)
- Skills ChecklistDocument2 pagesSkills Checklistapi-300770497No ratings yet
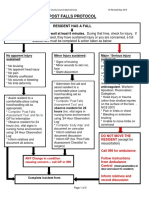
- 4-Hampshire Falls ProtocolDocument5 pages4-Hampshire Falls ProtocolsheenaNo ratings yet
- Communicable Diseases Kala Azar May 07Document4 pagesCommunicable Diseases Kala Azar May 07Niraj KumarNo ratings yet
- Liberty Referral PDFDocument1 pageLiberty Referral PDFTuba HabibNo ratings yet
- Alcohol ResearcDocument85 pagesAlcohol ResearcEmmanuel de LeonNo ratings yet
- Where The Money Is in 2021Document34 pagesWhere The Money Is in 2021FidelisNo ratings yet
- Bio Medical Waste Authorization Certificate: Haryana State Pollution Control BoardDocument3 pagesBio Medical Waste Authorization Certificate: Haryana State Pollution Control BoardManishNo ratings yet
- 57d28ad03fcf8 - Nama Peserta Training PV 2016 - PESERTA UTAMADocument8 pages57d28ad03fcf8 - Nama Peserta Training PV 2016 - PESERTA UTAMASaepul BahriNo ratings yet
- The Policy Cycle PDFDocument11 pagesThe Policy Cycle PDFLauditta AchyaNo ratings yet
- Bladder Training Stroke PDFDocument10 pagesBladder Training Stroke PDFLeony KhairunisaNo ratings yet
- Canmedaj01540 0049Document4 pagesCanmedaj01540 0049ImanNo ratings yet
- RPBRS-ICU For Covid - Mentari ICU Covid 2021 - 25-01-2022Document24 pagesRPBRS-ICU For Covid - Mentari ICU Covid 2021 - 25-01-2022abdillah muttaqien alqodryNo ratings yet